On 15 April 2013 a two-car Matangi passenger train was operating the service from Wellington to Melling Station. As the train was slowing on the approach to Melling Station it encountered slippery track conditions, and despite the efforts of the train driver the train collided with the stop block just past the station platform. The train was damaged and three passengers received first aid, with one sustaining minor injuries. The force of the collision lifted the concrete stop block out of the ground. On 27 May 2014 a second train collided with the Melling Station stop block. The NZ Transport Agency notified the Commission of the second accident. As the lines of inquiry for the two accidents were similar, the Commission combined the two inquiries with a view to publishing one combined report.
Executive summary

- On 15 April 2013 a two-car Matangi passenger train was operating the service from Wellington to Melling Station. As the train was slowing on the approach to Melling Station it encountered slippery track conditions, and despite the efforts of the train driver the train collided with the stop block just past the station platform. The train was damaged and three passengers received first aid, with one sustaining minor injuries. The force of the collision lifted the concrete stop block out of the ground.
- Just over one year later, on 27 May 2014, the same thing happened when another two-car Matangi passenger train collided with the stop block. This time the train came to rest on top of the stop block. The concrete block split and the terminal pole for the overhead power line, mounted directly behind the stop block, was severed at ground level. The overhead contact wire drooped and momentarily touched the roof of the train, causing the electrical circuit breaker to trip for the area. The train was extensively damaged and two passengers received minor injuries.
- The Transport Accident Investigation Commission (Commission) found that for both accidents dew forming on the railway track following a period of dry weather made the track slippery (referred to as low adhesion). Both trains were being driven normally but the drivers were caught unaware by the slippery track conditions.
- The Commission also found that the training that drivers received for transitioning from the Ganz Mavag train type to the Matangi train type did not provide them with sufficient information in respect of the design and correct operation of the train brake and wheel-slide protection systems.
- The computer-controlled train braking system is sophisticated and is fitted with two independent wheel-slide protection systems to manage braking in slippery conditions. Post-accident testing revealed that the braking systems had not been optimised for slippery track conditions when the trains were first commissioned into service.
- The Commission identified a safety issue whereby the current National Rail System Standards did not require new train types to have their train brake systems tested under slippery track conditions against an appropriate standard.
- The Commission also identified safety issues with the assessment of risk for trains entering terminating stations. The normal allowable train speeds left little margin for error in the event of something going wrong, and the stop block was an older type and was less effective at absorbing impact forces than its modern equivalent. Also, the pole supporting the overhead electrical traction line was directly in the path of an overrunning train.
- It was of concern to the Commission that the driver of the train in the second accident was found to have cannabis in his system, although it does not believe that it was a contributory factor.
- The Commission made four urgent recommendations to KiwiRail to address issues to do with risk, and two further recommendations to the NZ Transport Agency to ensure that low-adhesion braking requirements were defined in rail standards and that the brake systems on the new Auckland electric trains were optimised for low-adhesion conditions.
- Actions were taken to address four of the recommendations, which were then closed before this report was published. The agencies involved have also made progress in addressing the remaining recommendations, and taken safety actions to address other safety issues identified in this report. Detail of the safety actions taken are included in sections six and seven of this report. In summary, they are:
- The train brakes were tested and optimised for slippery track conditions
- The line speed into Melling Station was reduced and the line speed at other terminal stations was reviewed and changed as appropriate
- The stop block at Melling was replaced with a shock absorbing buffer stop
- The traction power pole at Melling was relocated away from the track centreline
- Matangi drivers received further training on the Matangi brake systems
- Overhead traction power reset procedures were changed
- A low adhesion working group was formed for the Wellington area
- The procurement of a driver training simulator for Matangi trains was initiated
- The driving console in the Matangi trains was modified to alert the driver whenever the train was experiencing wheelslide activity.
- Key lessons arising from this inquiry were:
- Slippery track conditions are a foreseeable risk and train braking systems must be designed, tested and optimised to provide adequate braking performance under those conditions.
- Train drivers must be adequately trained to be fully conversant with the characteristics of their train braking systems, and to drive their trains within the trains’ capabilities.
- When a new train type is being commissioned and first entered into service, train operators should seek feedback from the drivers on train performance in order to identify and remedy promptly any potential performance issues.
Factual information Pārongo pono
Background
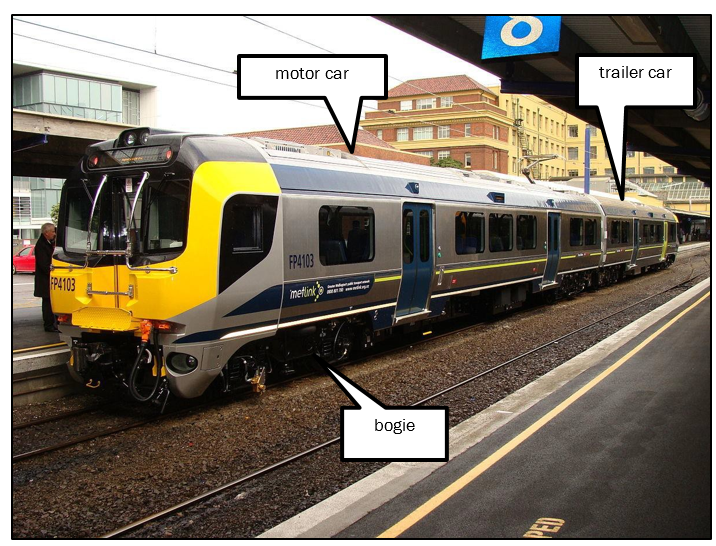
- The Matangi train is a two-car electrical multiple unit comprising a motor car coupled to a trailer car. Each car has two bogies, with two axles on each bogie. The wheels are fixed to the connecting axle and rotate as a unit. The cars are a matched set but may be coupled to other sets to make a longer train.
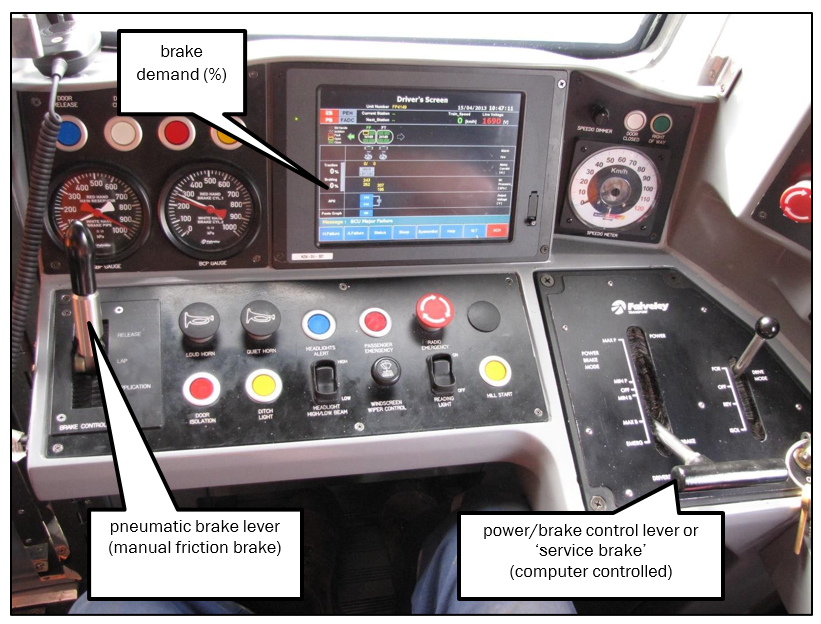
- The driver normally controls the train using a single power/brake lever by moving it forward for acceleration and back for braking. The selected power or brake setting is displayed on the driver’s control screen. A full-service train brake is when the power/brake position is moved to the 100% brake position. The computer-controlled brake system (see Figure 7) decides which type of brake system to use and the proportion of brake force to share between the motor car and the trailer car.
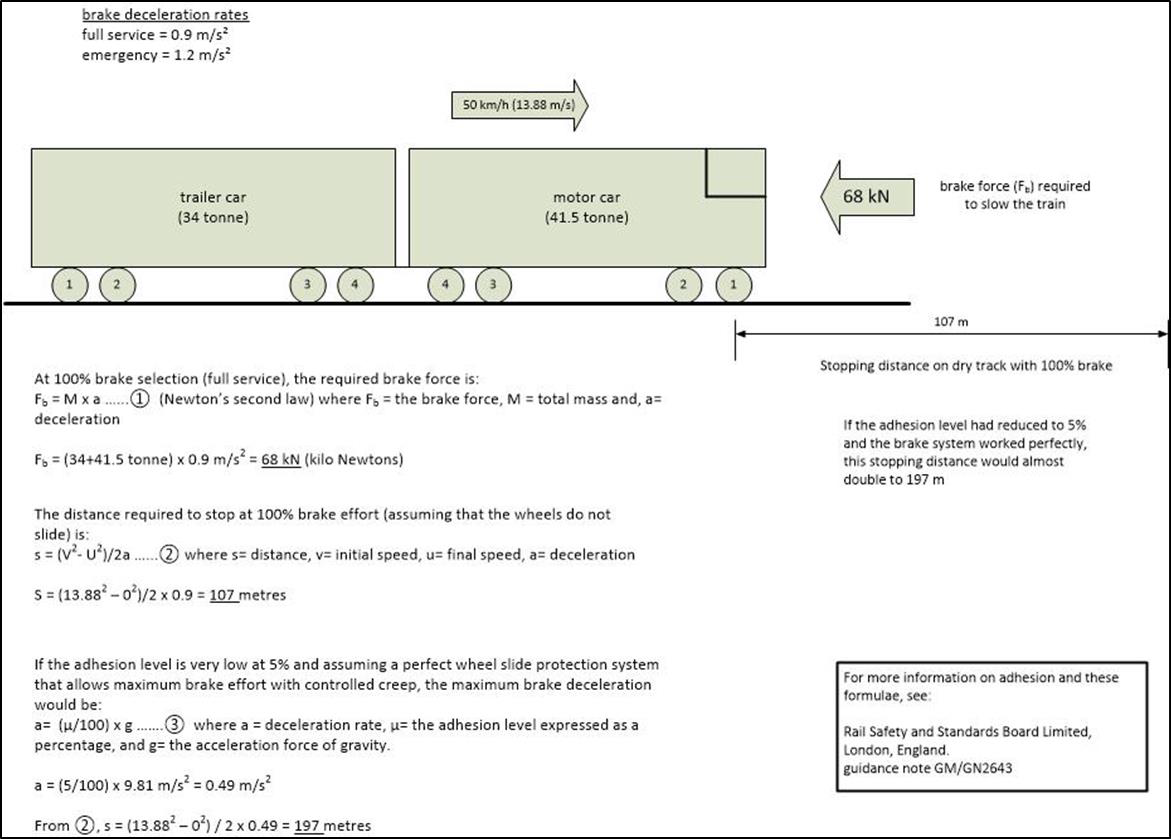
- The brake system is designed to achieve a full service (100%) brake deceleration rate of 0.9 metres per second per second (m/s2) and an emergency brake deceleration rate of 1.2 m/s2 in normal conditions. It achieves normal service braking with a combination of friction and dynamic brake systems, but for emergency stops it only uses friction brakes.
Friction brakes
- Friction brakes use air pressure to force a brake pad against a rotating surface to slow its rotational speed. Both cars are fitted with friction brakes, the motor car with wheel tread type and the trailer car with disc type. Tread brakes force a brake pad against the rolling surface of the wheel (the wheel tread (the wheel tread is the part of a rail wheel that runs on top of the rail). Disc brakes are attached to the axle and the brake pads are clamped to either side of the disc by a brake caliper. The friction brakes act independently on each car of the two-car set.
Dynamic brakes
- The motor car is also fitted with dynamic brakes, which use the magnetic fields generated in the electric traction motors to slow the wheels. This creates a braking torque that is available only when the train is in motion. The Matangi dynamic brakes act independently on each of the two motor car bogies.
- Dynamic brakes have an advantage over friction brakes in that they result in less wear to brake components. The limitation of dynamic braking is that the train has to be moving within an acceptable speed window for it to be effective and available.
Pneumatic brakes
- A separate, manually operated pneumatic brake lever is provided for drivers to operate the friction brakes. This also acts as a backup if the computer-controlled brake system should fail. The pneumatic brake acts equally on all axles of the train.
Emergency brake
- If a driver needs to stop urgently, the power/brake lever can be moved farther back beyond the 100% position into the emergency position. This triggers the emergency brake control loop, which disables the dynamic brake and applies friction brakes to both cars in the set. The emergency brake can be initiated by several different methods and is designed to decelerate the train at a higher rate and stop in a shorter distance than it would with 100% brake.
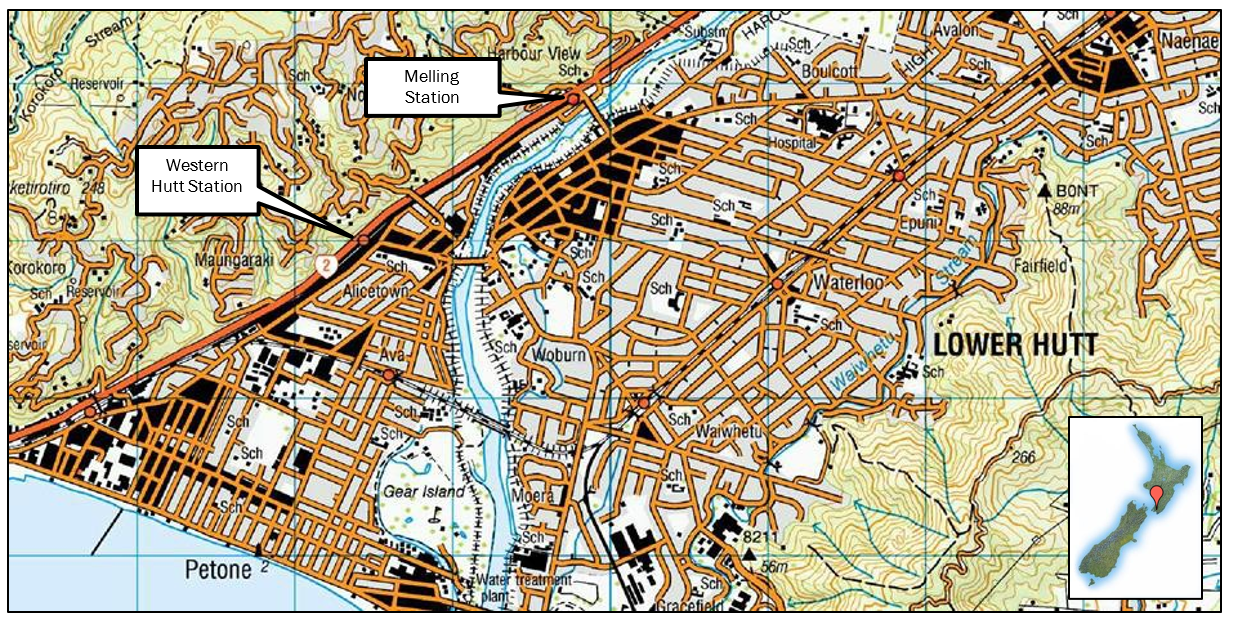
Melling Station
- Melling Station is a terminal station at the end of the Melling Line. The maximum line speed was 70 kilometres per hour (km/h) and the operator’s procedures require that when a train passes the start of the platform it is travelling slower than 50 km/h. The end of the line had a concrete stop block to prevent trains over-running.
Narrative
Melling 1 accident
- On 15 April 2013 a two-car Matangi train was operating the service from Wellington to Melling Station. The weather was fine but dew had formed in the area, including on the rails. The train was due to arrive at Melling Station at 0746 with a driver, train manager and nine passengers on board. As the train approached Melling Station, the driver began to apply the brake but the train did not slow as quickly as he expected.
- When the driver realised that his train was not decelerating at the rate he required, he increased to full service brake, quickly followed by full pneumatic brake, and finally emergency brake. However, the train continued past the station platform and collided with the stop block.
- The stop block was a partially buried concrete structure (see Figure 3). The collision forced the stop block out of the ground and the train rebounded back but remained on the rails (see Figure 4).


- Three passengers were treated at the site. One sustained minor injuries and went to hospital for further examination.
Melling 2 accident
- Just over one year later, on 27 May 2014, a two-car Matangi train operating from Wellington to Melling also collided with the stop block at Melling Station. The train had departed from Western Hutt Station shortly after 0808 with the driver, a train manager and 10 passengers on board and was due to arrive at Melling Station at 0809. The driver was on his second trip to Melling that morning with the same train when the accident occurred.
- About 500 metres (m) from the stop block with minimum braking applied, the driver realised that the train was not slowing as expected. He increased to full service brake then to emergency, and then he applied full pneumatic brake. Realising that his train would collide with the stop block, he pressed the emergency brake button. He then opened the door to his driving cab and called out to warn the passengers to brace themselves, then braced himself for the collision.
- The train collided with the concrete stop block that had been reinstalled after Melling 1 (see Figure 5 and Figure 6).

- The train came to rest on top of the stop block. The concrete block split and the terminal pole for the overhead power line, mounted directly behind the stop block, was severed at ground level. The overhead contact wire drooped and momentarily touched the roof of the train.

- When the live contact wire touched the train, it tripped the circuit breaker in the local electrical substation. The KiwiRail traction controller on duty at the time in the Wellington National Train Control Centre noted that the circuit breaker had tripped. The train controller called the Melling 2 driver on the radio but did not get a response, so the train controller and the traction controller agreed they would reset the circuit breaker remotely.
- A KiwiRail employee, who had been waiting to board the train as a passenger, recognised the potential electrical hazard to the public and prevented people on the platform touching the train until the overhead wire had been made safe.
- The train manager attended to the passengers, checked for injuries and performed first aid as required. The driver went to the rear cab to use the radio to call train control. He reported the accident, requested that the overhead power supply be made safe, and asked for emergency services to attend.
- Emergency services attended the scene and secured the train from public access. Ambulance staff entered the train through the emergency door at the rear to attend to one passenger with minor injuries and another in shock. The passenger doors remained closed for 22 minutes after the accident, until the train was deemed safe for passengers to exit.
The drivers
- At the time of the Melling 1 accident in 2013, the driver had 11 years’ driving experience with the operator. He had converted from the Ganz Mavag type train to drive the newer Matangi type train in 2011 and had been driving them regularly since. He was tested under the operator’s standard policy for the presence of drugs and alcohol and found to be clear.
- At the time of the Melling 2 accident in 2014 that driver had 11.5 years’ driving experience with the operator. He had been driving the Matangi trains since they were introduced in 2011. After the accident the driver was tested under the operator’s standard policy for the presence of drugs and alcohol. He had a positive result for THC acid (THC acid = 11-nor-delta-9-tetrahydrocannabinol-9-carboxylic acid (or TCH-COOH) in his urine (further information on the effects of cannabis is provided in Appendix 5).
Computer-controlled brake system
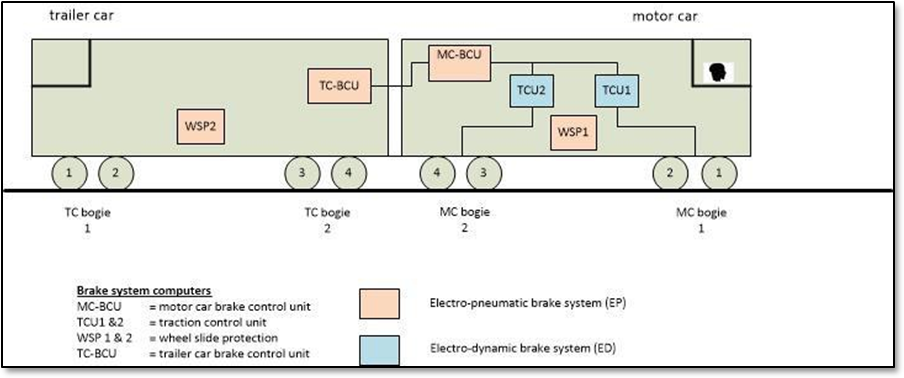
- The Matangi brakes are controlled by computers (control units). The control units read a driver’s brake demand signal and each activates an appropriate brake force depending on the speed and weight of the train at the time (see Figure 7). The control units each respond independently to the demand signal by calculating the required brake force. The control units then check how much brake force can be achieved using dynamic brakes and back off an equivalent friction brake force to ensure that dynamic is the preferred brake force.
- As the train slows down, there is a point where dynamic braking cannot generate enough brake force. At around 14 km/h the friction brakes are blended in and dynamic brakes faded out.
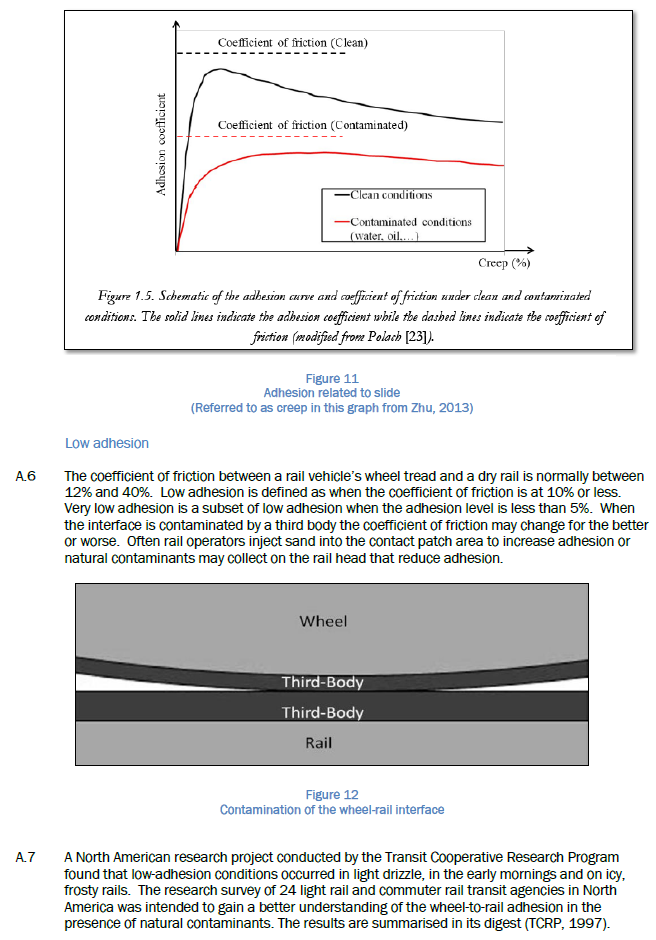
Rail adhesion
- Adhesion, in rail terminology, refers to the degree of grip, or friction, between a train wheel tread and the top surface of the rail head. Adhesion is the same as the friction coefficient but expressed as a percentage. The normal range for adhesion on rail is between 12% and 40% (see Appendix 4 for more information on adhesion).
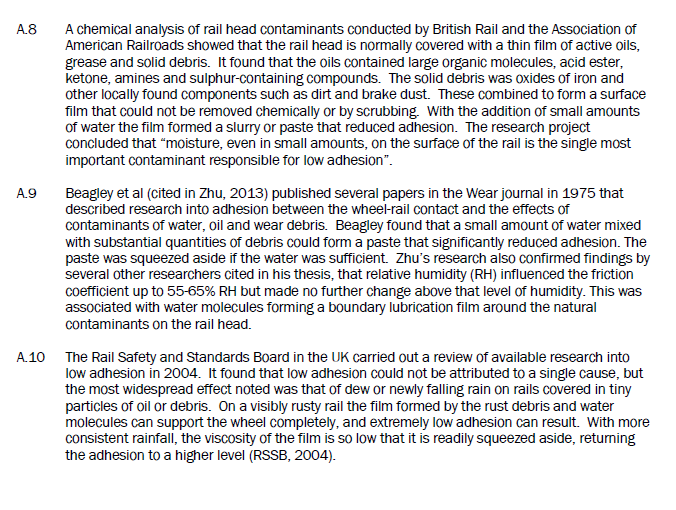
- Any brake application to a wheel will slow its rotating speed, which is transferred through the contact patch (the contact patch is the rolling contact area between a train wheel tread and the top surface of the rail head) between the wheel and the rail as a decelerating brake force. If the brake force is greater than the maximum adhesion force possible in the conditions, the wheel will begin to slide (wheel slide is a condition where the rotational speed of a wheel is less than that corresponding to the actual linear speed of the train). The effects of low adhesion upon a train are that the wheels may slide under braking and stopping distances will be longer.
- The Matangi procurement specification required the brake system designer to nominate the minimum adhesion level that its equipment would need to achieve the specified deceleration rates. The nominated levels were 9.6% adhesion for full service braking and 14.2% adhesion for emergency braking.
- Low adhesion as described in this report is when the adhesion is 10% or less. A subset of this condition is that when the adhesion is under 5% it can be termed very low adhesion. Low adhesion is an operational risk for train operators, while the very low adhesion condition is an important consideration for equipment designers. Any change to the interface between the rail and the wheel, such as the presence of water, leaves or grease, may affect the adhesion.
- The most common cause of low adhesion is when a light layer of moisture forms or collects on the top of the rail. This may be caused by morning dew, light rain or mist. When the moisture combines with other contaminants normally found on a rail, such as dirt, rust, brake dust or solid particles of air pollutants, it can form a slurry that acts as a lubricant. In heavy rain this slurry tends to wash off the rail top and thus low adhesion becomes less of a problem.
Wheel-slide protection system
- If a wheel starts to slide while a train is braking, its ability to apply an effective braking force through the contact patch is reduced. However, a small amount of controlled wheel slide can optimise the brake force. A wheel-slide protection (wheel-slide protection is a control system that limits any applied brake force during times of reduced adhesion to utilise the maximum available adhesion and to prevent the wheels locking up. It is analogous to anti-lock braking on a motor car) system allows a braked train wheel to rotate up to 20% slower than the train speed to achieve the most effective braking force in low-adhesion conditions. However, the actual train speed is not usually measured by these systems. Instead, it relies on a software-derived value analogous to the train speed called the ‘reference speed’. The system will override the brake force applied by the driver to keep the wheel speed within the 20% band below the reference speed. The Matangi has two types of wheel-slide protection system.
- One wheel-slide protection system is a software application within another controller. It resides in the two traction control units (see Figure 7) and is effective only when dynamic braking is in use. The other wheel-slide protection system is a dedicated, stand-alone, computerised control unit that only works with the pneumatic friction brakes. A system of this type is fitted to both the motor and the trailer cars. It continuously monitors for wheel slide and operates whenever wheel slide is detected while the friction brakes are in use. This wheel-slide protection system is disabled when the train speed drops below 5 km/h.
Similar accidents
England
- In 2005 the Rail Accident Investigation Branch in England investigated a series of low-adhesion-related events that occurred in 2004 and 2005 (RAIB, 2005). The investigation identified two key points that were relevant to New Zealand. One was that operators used past events to predict low adhesion rather than just monitoring current conditions or risk. The second point was that the train operating companies did not understand the characteristics of their new trains. That lack of understanding led to inadequate briefing of drivers and suboptimal performance of the wheel-slide protection systems.
- The report also highlighted: a lack of industry knowledge on the cause of low adhesion; a lack of test procedures to optimise the performance of whole-train braking systems with wheel-slide protection; and that further research was required to find the optimum set-up parameters for wheel-slide protection systems.
Melbourne, Australia
- In Melbourne a series of incidents occurred in 2009 in which trains failed to brake effectively and overran platforms. The Office of the Chief Investigator Transport Safety investigated (OCITS, 2009) and found several contributory factors. The listed contributory factors were:
- moisture on the rail caused low-adhesion conditions
- the Nexas trains’ braking system response to a wheel-slide event
- the Nexas trains did not have tread brakes, which could have otherwise helped to clean the wheel tread surface and improved braking
- the train’s very good dry-track braking performance may have raised drivers’ expectations in low-adhesion conditions
- drivers did not have a sufficient depth of understanding of how the Nexas braking system worked or specific guidance on operational procedures when encountering low adhesion
- the network risk management of low-adhesion conditions was inadequate at the time
- low-adhesion braking performance requirements were not adequately defined in the procurement specifications nor verified in acceptance tests.
Queensland, Australia
- In 2013 a Queensland Rail passenger train failed to stop at a platform and collided with the end-of-line buffer stop. The train rode up over the buffer stop and onto the platform, where it flattened the mast for the overhead power line and came to rest inside the station building. The train had encountered low-adhesion conditions and the driver’s actions were not contributory. The Australian Transport Safety Bureau’s report into the accident listed the main contributing factor as the operator’s inadequate management of low-adhesion risk (ATSB, 2013).
Analysis Tātaritanga
Introduction
- Operating trains in conditions of low rail adhesion is a predictable risk applicable to any rail system. The causes of low adhesion may vary from one country, region or town to the next, but the effect is the same: braking in low-adhesion conditions will increase the distance required to stop a train.
- We know that low rail-adhesion conditions existed in both of the Melling accidents because wheel-slide protection activities were recorded by the train data loggers. However, the exact locations of any low-adhesion area(s), the extent of each area or areas, and the actual levels of low adhesion present at the time were not able to be determined.
- There was nothing in the condition of the train wheels or the profile of the rail that would have adversely affected the wheel-to-rail contact patch
- The driver of the Melling 2 train tested positive for the presence of cannabis metabolites in his urine. The investigation was unable to establish whether his performance on the day was impaired by the effects of cannabis. However, the use of performance-impairing substances by train drivers is a significant safety issue.
- As the following analysis shows, a factor contributing to each accident was that the train braking system did not perform as well as it could have in the low-adhesion conditions.
- A key safety issue was that the National Rail System Standards (NRSS) did not require the Matangi braking system to be tested under slippery track conditions against an appropriate standard. Consequently the train brake system had not been optimised for low-adhesion conditions.
- The analysis discusses what happened in each case leading up to the collision.
- Consideration is also given to: the performance of the train braking system; driver training in respect of the differences between the Ganz Mavag and Matangi braking systems; and the management of risk to trains operating into terminating stations, which had not kept pace with industry changes.
Interpretation of evidence
Melling 1
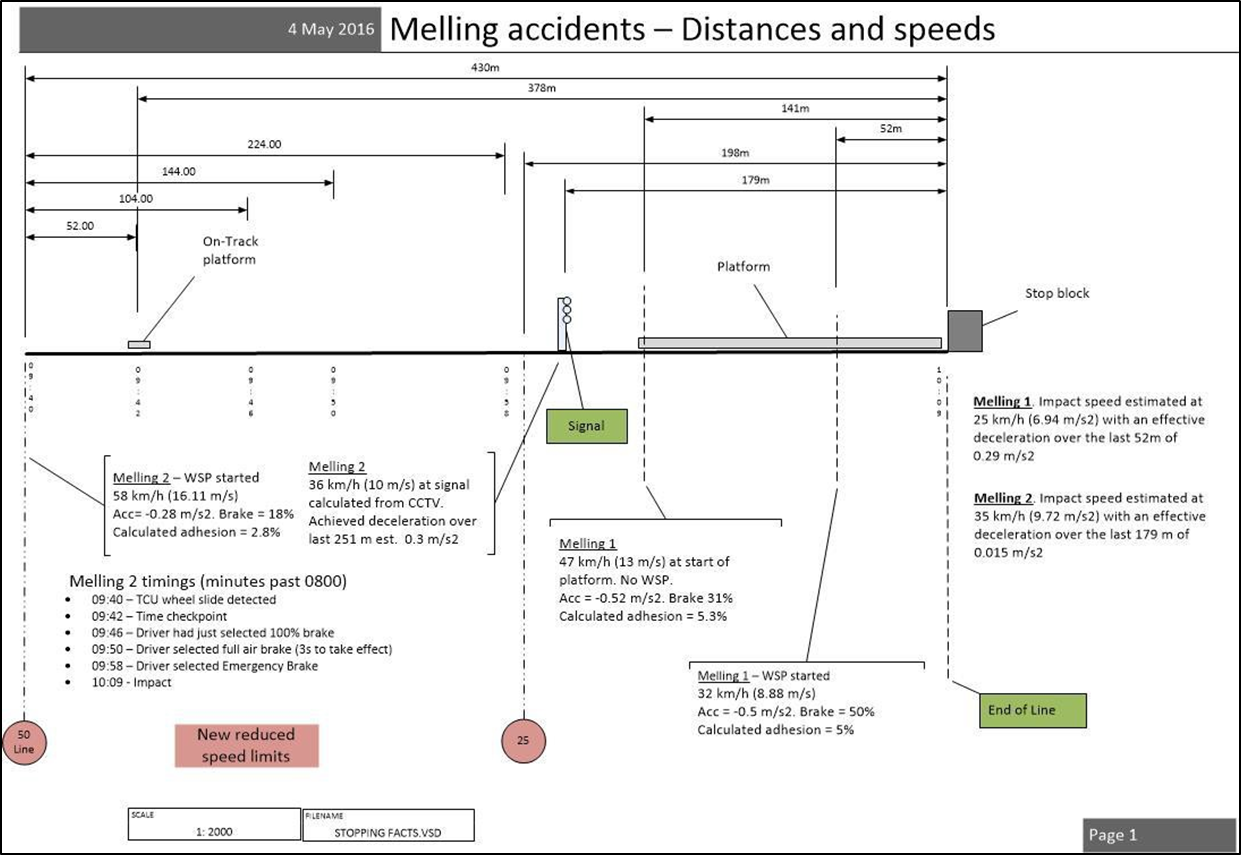
- The driver of the Melling 1 train had braked smoothly down to 47 km/h by the time his train reached the start of the platform. This was below the maximum speed of 50 km/h. When he increased the brake demand from 31% to 50% the wheels lost adhesion and began to slide. The dynamic brakes in the motor car were the only brakes in use at the time and the traction control units attempted to control the wheel slide. The train was about 52 m from the stop block and it would travel that distance in about six seconds.
- The driver applied full service brake, then full pneumatic brake (applying full pneumatic brake is effectively applying emergency brake), followed by the emergency brake. The computer-controlled brake system responded by disabling the dynamic brakes. Then it increased the friction brake force on both the motor car and the trailer. As the friction brake force increased, the wheels continued to slide. The applied brake force was limited by the wheel-slide protection system while it attempted to optimise the train braking force. The train braking system was unable to apply an effective brake force in the time available. The train collided with the stop block at 0754 at an estimated speed of 25 km/h.
- The speeds and brake actions are presented graphically in Appendix 1.
Melling 2
- The Melling 2 driver started decelerating his train 1.2 kilometres from the Melling Station stop block by selecting ‘off’ with the power/brake control lever. He increased the brake to 23% then reduced it to 18% when the train was about 525 m from the stop block. At 430 m out from the stop block, the wheels started to slide. The train was travelling at 58 km/h and the computer-controlled braking system was using dynamic brakes only. The traction control units were unable to control the wheel slide within three seconds, so the computer-controlled brake system disabled the dynamic brakes and increased the friction brake force in the motor car.
- The driver had also realised that the train was not slowing at the rate he expected, so he increased brake demand to 50%, and then to 100%. The computer-controlled brake system responded by increasing the friction brake force in the trailer car to about 75%, which caused the trailer car wheels to slide also. Four seconds later the driver applied full pneumatic brake, followed by emergency brake.
- After the dynamic brakes were disabled, the wheel-slide protection units fluctuated the friction brake force in both cars in an attempt to control the slide until the train hit the stop block at an estimated speed of 35 km/h. The wheel-slide protection systems were unable to regain an effective rate of deceleration over the last 430 m (see Appendix 1 for distances and speeds).
- The driver of the Melling 2 train tested positive for cannabis, which is of concern. The Commission has included substance use on its ‘watch list’ and encourages regulators and operators to put measures in place to prevent substance impairment by persons in safety-critical roles. It was not possible to determine whether the driver was impaired at the time of the accident.
- Although cannabis impairment reduces with time since exposure it affects people differently and is known to impair the executive cognitive function of information processing. Other executive functions affected are planning, decision-making, risk taking, and working memory. All of these functions are crucial for a train driver to operate safely (see Appendix 5 for more details).
Conditions common to both accidents
- Both drivers were handling their trains in a normal way. They approached Melling Station within the speed limit for the line and they were on target to reduce the train speed to less than 50 km/h by the time they reached the start of the platform.
- Both drivers said that they had been alert and focused upon the task and not distracted. They had had light duty schedules with adequate periods of rest in the days leading up to their respective accidents. Cell phone records proved that the drivers were not engaged in text or voice communications at the time. Therefore, fatigue and distraction were very unlikely to have been factors in either accident.
- The train event recorders showed that the train wheel-slide protection system activated in both accidents, meaning that low adhesion was a common factor.
- Both trains were repaired sufficiently for the brakes to be tested on the track. Repairs were limited to facilitate a safe test run but all brake equipment and brake-controller software were kept as they originally were during the accidents. Test runs were conducted by KiwiRail engineers on dry track around the Wellington rail network, with a Commission observer on board. Several brake test runs from a steady speed to a full stop were also conducted using various combinations of brake selection, pneumatic brake and emergency brake.
- These test runs proved that the train brakes were working on both trains at the time of the accidents, and that each train conformed to the NRSS standard for stopping distances on dry track.
- The Commission engaged MetService to analyse data on the weather conditions preceding both accidents. They concluded that in both cases dew was likely to have formed on the track and that the weather conditions preceding each accident had been dry for several days. These were the ideal circumstances for low-adhesion conditions to exist.
- Several dry days preceding the accidents would have allowed a layer of natural deposits to form on the top of the rail, which was then followed by the formation of dew. The resulting mixture would have created a low-adhesion layer between the rail and the train wheels.
Management of infrastructure risk at terminating stations
The line speed limit
- The maximum line speed for approaching Melling Station was 70 km/h. Drivers were taught to aim to have their train speeds at below 50 km/h by the time the trains reached the beginning of the platform. The line speed is set depending on the geometry of the track. From a risk perspective, Melling is a terminating station, meaning the consequences of overrunning the platform are much higher than at non-terminating stations. The same applies to the target speed for when the train reaches the start of the platform. Any train malfunction, low track adhesion or underperformance of the train braking system risks the train colliding with the stop block.
- The Commission recommended that KiwiRail reassess the speed limit for trains approaching Melling Station, and that it also reassess the speed limit for trains approaching other terminating stations on the rail network. KiwiRail has since accepted these recommendations and addressed the safety issue.
The stop block
- The concrete stop block had been installed in 1954. It lacked the impact-absorbing qualities of more modern stop blocks. The less effective they are, the greater the damage to the train and its occupants, as both these collisions demonstrated. The Commission recommended that KiwiRail replace the concrete stop block with a more appropriate shock-absorbing system similar to the type being installed in Auckland at the time. KiwiRail accepted this recommendation and replaced the stop block.
The overhead power
- There were two issues with the overhead traction power system. Firstly, the terminal pole was hit by the Melling 2 train because it was directly in the path of the train when it collided with and overran the stop block. The force of the collision severed the pole, causing the live overhead wire to droop and contact the train.
- The Commission recommended that KiwiRail relocate the terminal pole out of line with a direct overrun. This has since been completed with a new cantilevered pole mounted off to one side of the rail centreline and the safety recommendation has been closed.
- When the contact wire drooped and touched the train, it tripped the electrical protection system, which led to the second issue. The traction controller at the Wellington National Train Control Centre reset the power before the driver was able to warn train control of the accident. The Commission raised with KiwiRail the risk of promptly resetting the overhead power without first establishing the reason for the system tripping.
- After two further incidents KiwiRail submitted to the Commission in December 2014 that it had accepted its concerns about promptly resetting the overhead power after a protection trip. KiwiRail then issued an internal memo to change its operating procedures. Based on this action the Commission did not issue a safety recommendation.
Train brake performance
Brake performance expectations
- Appendix 2 demonstrates the best theoretical stopping distance for a Matangi train in low-adhesion conditions. It assumes that the wheel-slide protection systems operate perfectly to control the wheel creep and allow the maximum brake effort to be applied in the conditions. The calculation shows that a train with a typical passenger load for Melling could decelerate at 0.49 m/s2 to stop in 197 m from 50 km/h using full service brake in low-adhesion conditions (at 5%).
- In the Melling 2 accident (see details in Appendix 1) the train managed to decelerate at 0.3 m/s2 over the first 251 m, reducing to 0.015 m/s2 over the remaining 179 m, and only slow by 23 km/h but not stop in the total distance of 430 m. This comparison between theoretical and actual brake performance indicated that either the adhesion was much less than 5% or there was a performance issue with the train brakes in low-adhesion conditions, or that there was a combination of both factors.
- The train commissioning tests conducted by the manufacturer established that the train braking system performed to the GWRC procurement specification. These tests included extensive test runs with various combinations of brake application and some with simulated low-adhesion conditions. The overall requirement was that the train complied with NRSS/6 – Engineering Interoperability Standard, Version 1 (NRSS/6) to stop within 460 m from a speed of 100 km/h in all normal climatic conditions. Testing proved that the train met the NRSS/6 stopping distance requirements.
- The commissioning test specification did not require the train braking and wheel-slide protection systems to be tested in controlled low-adhesion conditions in accordance with an internationally recognised standard (for example, UIC 541-05), nor was it required by any other authority.
- To investigate the performance of the brake system, GWRC agreed to conduct a series of brake tests in low-adhesion conditions and measure the performance of the Matangi brake system.
Low-adhesion brake test programme
-
The tests proved that in low-adhesion conditions the current configuration of the computer-controlled brake system did not perform as well as it could have. Several opportunities for improving the train brake performance were identified and trialled. These included:
- reducing the initial amount of available dynamic brake effort
- reducing subsequent available dynamic brake effort after each wheel-slide control attempt
- improving the trailer car friction brake behaviour during wheel slide with dynamic brakes
- optimising the wheel-slide control in the motor car
- improving the handover between dynamic and friction brake controllers
-
improving the interaction of automatic brakes with the manual pneumatic brakes.
The system was reconfigured and further trials were conducted.
- As a result of the test programme, GWRC initiated corrective actions to improve the low-adhesion brake performance and approved software changes. The first software upgrade was rolled out across the Matangi fleet in 2015.
- The test programme raised a further concern that the wheel-slide protection system for the friction brakes was not performing in accordance with the UIC 541-05 standard (UIC is the Ünion Internationale Des Chemins De Fer (International Union of Railways). GWRC arranged for the brake manufacturer to conduct a more rigorous test of the wheel-slide protection units in a test facility in Italy. This resulted in a further software upgrade to improve the performance of the friction brake wheel-slide protection system in low-adhesion conditions. This software upgrade was rolled out across the fleet in mid-2016.
- Following the testing programme and the software changes to the train brake system, the Matangi train brake performance in low-adhesion conditions was noticeably improved.
- However, there are too many variables, unknowns and possible scenarios to draw any definitive conclusions on whether the trains would have stopped before the stop blocks if these improvements had been made when the trains were commissioned. For example:
- the dew suspected of causing the low adhesion evaporated soon after the events, so the extent and level of low adhesion could not be measured
- the method of measuring low adhesion is subject to variability and the result may differ from the actual adhesion experienced by a train
- the control inputs from the drivers could vary depending upon circumstances at the time, such as: their choice of speed and brake selections; their knowledge about how the brakes worked; and the response they had each experienced with the brakes during the accidents.
New Zealand standards for train brakes
- It is concerning that the brake performance of a new and modern commuter train was only made to comply with the basic requirements of NRSS/6. The standard is silent on: low-adhesion brake performance; wheel-slide prevention systems; full train brake performance across different braking systems; and reference to appropriate international standards.
- Although the selected train brake equipment had the capability to perform well in low-adhesion conditions, the brake performance specifications did not require it to be verified. Therefore, the system was not set up for optimum performance. The current trend in Europe is to test train brakes to local standards (for example in UK; BS EN 15595:2009 and RSSB GM/GN2695), with a complete train as a fully integrated brake system. These standards include the verification of wheel-slide protection systems in controlled low-adhesion conditions and the optimal integration of dynamic and friction brakes.
- The NRSS was originally intended to provide an interoperability framework for rail participants to meet when wishing to operate on the rail network. It is still the only formal set of rail standards available in New Zealand.
- In 2010 the Commission issued three safety recommendations to the Secretary for Transport to address safety issues relating to the status of the NRSS. As a result of the Melling accidents the Commission issued a new recommendation to the NZ Transport Agency in 2015 to review the NRSS to ensure that low-adhesion braking requirements were incorporated into the standards and that they were applicable to all trains intended to operate on the National Rail System. The Commission now has a total of seven open safety recommendations targeting changes to the NRSS. Three are to the Secretary of Transport and four to the NZ Transport Agency.
- The NZ Transport Agency is currently addressing these recommendations by undertaking an independent review to establish an appropriate rail regulatory framework for the future. In light of this review the Commission makes no new recommendations on this safety issue.
Driver training
-
The Matangi driver conversion training suggested that drivers consider the computer-controlled brake system as a ‘black box’ that performed better than the braking system in the older Ganz-Mavag trains. This suggestion was reinforced to the drivers when they experienced the Matangi train’s effective brakes on dry track.
-
Critical information describing how the computer-controlled brake system operated was not provided in the conversion course material or in the Train Crew Manual. Several drivers were interviewed about their understanding of how the computer-controlled braking system worked. It became evident that the conversion training had not adequately informed drivers about the differences between the two braking systems, particularly in low-adhesion conditions, and how the brake effort is shared between the motor car and trailer.
- A key difference was the Matangi’s preference for using dynamic brakes. This reduced the number of braked wheels to just those wheels on the motor car and consequently it required a higher level of adhesion to deliver that brake force. The effect was that the Matangi would experience wheel slide more often than the Ganz-Mavag in low-adhesion conditions. (See Appendix 3 for more details.)
- Another key difference between these two train brake systems was how brake effort was shared between the motor car and trailer. The Matangi computer-controlled brake system applied all brake effort from the motor car before using the trailer car brakes. The Ganz-Mavag stepped the brake effort sequentially in thirds. The first step would apply one-third brake force from the motor car, the next step would add one-third to the trailer, the next would increase the motor car to two-thirds and so on until full service brake had been reached on each car.
- In a four-year period, drivers encountered various braking problems with the newly commissioned trains, including dynamic brakes tripping out and their being unable to stop the trains at target points. The problems sometimes resulted in platform overruns, which were subsequently reported to the regulator and the operator but little progress was made in resolving them. This led to drivers losing confidence in the braking system and to experiment with alternative braking techniques or work-around actions.
- The operator did not have a best practice of braking in an emergency, so had left it to the drivers’ discretion. A benefit of the brake test programme was drivers actually experiencing wheel-slide protection activity while braking on a safe and controlled low-adhesion test track. The operator was subsequently able to define a best-practice braking technique for low-adhesion conditions and retrain its drivers accordingly.
Subsequent events and preventive measures
- On 10 June 2015 at 1039, a third Matangi train (Matangi train FP/FT 4218) had a braking problem at Melling in low-adhesion conditions. The Commission made enquiries into the incident and reviewed the train data logger record. The train had been upgraded with the new brake control software and the driver was aware of the new, best-practice, low-adhesion braking technique.
- The train started to slide near the ‘on-tracking boards’ at the start of the straight into Melling Station, but the driver recognised the wheel-slide protection activity and applied emergency brakes. The train was reported to have come to a stop from 35 km/h in 205 m, which represents a deceleration rate of approximately 0.23 m/s2. The point where it stopped was before the platform, so the driver then crept the train forward to the desired target stop point, where it was stopped normally.
-
GWRC arranged for the wheel-slide activity to be presented to the driver’s screen of the train management system. This will help drivers to recognise when low-adhesion conditions exist and to implement their defensive driving techniques.
- GWRC took the initiative to organise a ‘Low-adhesion working group’ in the Wellington area. The group has members from all aspects of the rail industry, including the train operator, network manager and infrastructure owner. The working group’s purpose is to share information about low-adhesion conditions and collaboratively take action to reduce its effect on operations in the Wellington rail network.
- In October 2016 GWRC started the purchasing process for a Matangi train simulator to assist with future driver training. Depending on the fidelity of the simulator controls, it could provide a means to better prepare drivers for handling low-adhesion conditions.
Appendix 1. Distances and speeds
Appendix 2. Brake calculations
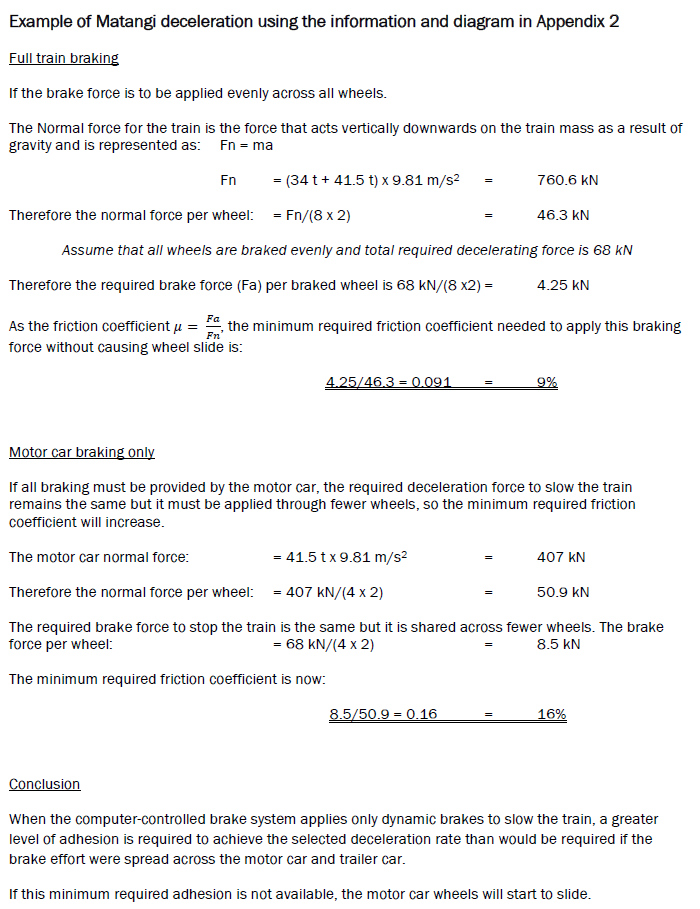
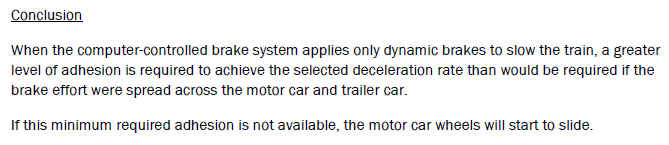
Appendix 3. Required coefficient of friction
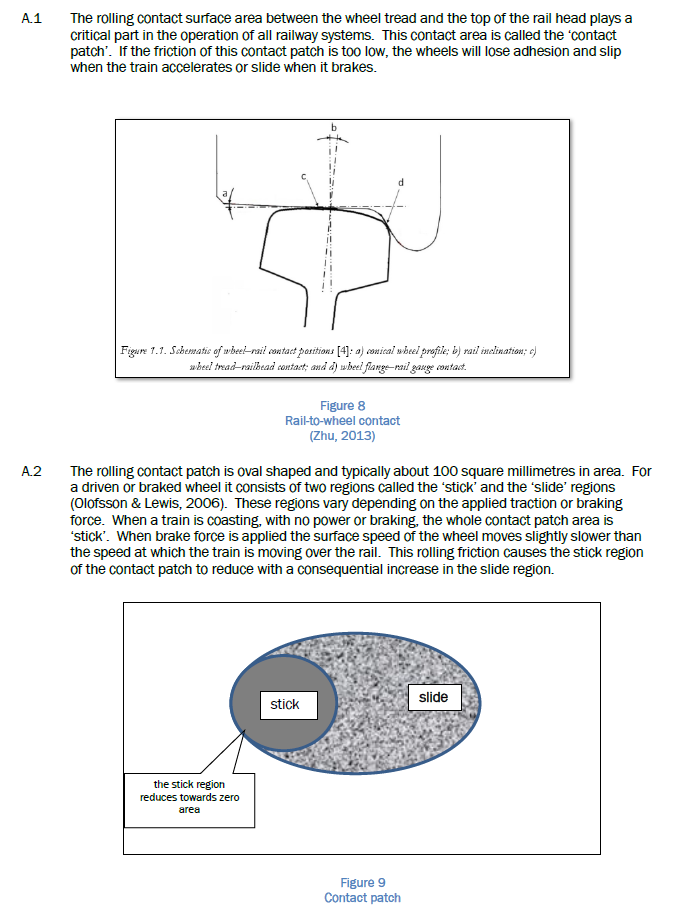
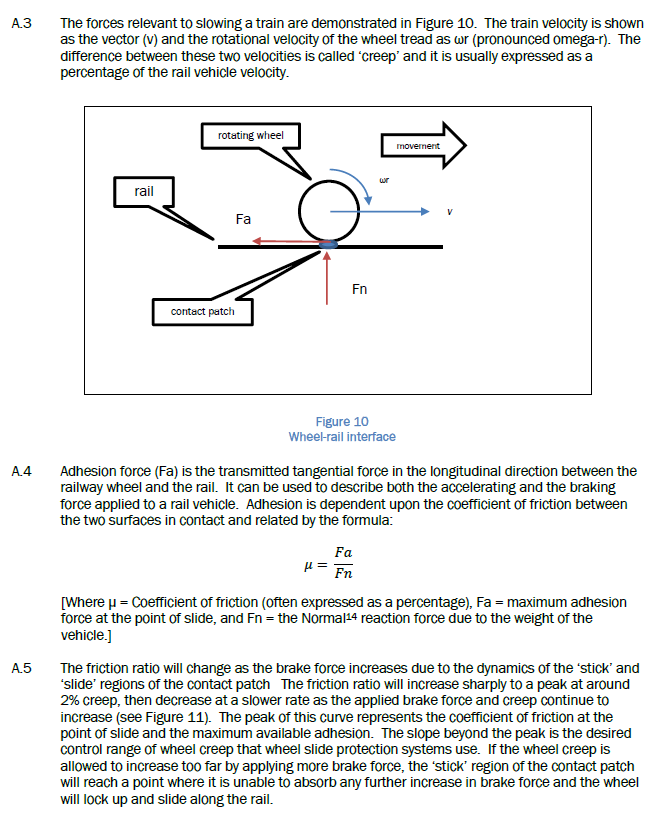
Appendix 4. Research on rail adhesion
![]()
Appendix 5. Research on cannabis impairment
![]()