Grounding of a pilot vessel in restricted visibility near Bluff highlights how routine navigation habits and the use of electronic tools play a critical role in maritime safety.
Executive summary Tuhinga whakarāpopoto

What happened
- On 26 December 2024, the pilot vessel Takitimu II was travelling outbound from South Port, Bluff, with three people on board: the master, the deckhand and one passenger. The passenger was a South Port pilot who was scheduled to board an inbound vessel and bring it into port.
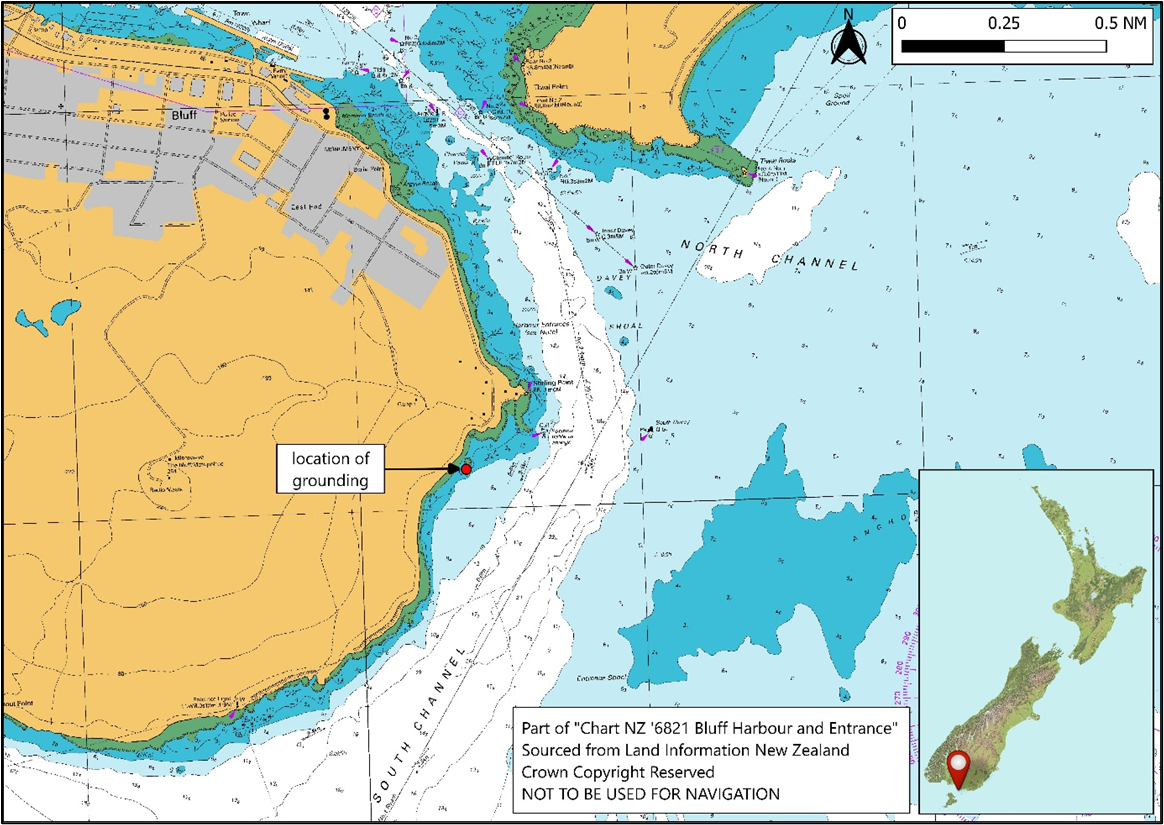
- After leaving the harbour and passing Stirling Point, the master turned Takitimu II too far to starboard and, at a speed of around 18 to 20 knots (kt), Takitimu II ran aground on rocks.
- Later that morning, a Coastguard vessel towed Takitimu II off the rocks.
- The master and the deckhand suffered minor injuries. Takitimu II sustained moderate damage to its hull and underwater fixtures while aground.
Why it happened
- The master’s situational awareness was significantly reduced while navigating the vessel, primarily by eye, in restricted visibility (any condition in which visibility is restricted by fog, mist, falling snow, heavy rainstorms, sandstorms or any other similar causes).
- The visibility was sufficient for the master to locate and identify the buoys and beacons marking the harbour entrance and the main channel. However, patchy fog affected the master’s perception of their usual visual references.
- The vessel had sufficient electronic navigation instruments to support navigation in restricted visibility. At the time of the accident, these instruments were switched on, but the master was not using them to verify the vessel’s position and progress.
- South Port’s training and familiarisation scheme for pilot-vessel masters did not contain procedures to ensure the continuing proficiency of pilot-vessel masters.
- Any condition in which visibility is restricted by fog, mist, falling snow, heavy rainstorms, sandstorms or any other similar causes
What we can learn
- Electronic navigation instruments can enhance a navigator’s understanding of the vessel’s position and surroundings and how the vessel is progressing relative to the environment. It is especially appropriate to use electronic navigation instruments while navigating in restricted visibility, when a navigator’s access to visual information about their surroundings is limited.
- Periodic verification of proficiency can help a maritime operator identify whether appropriate navigation methods are practised on board its vessels. It also provides an opportunity to identify when masters and crews need additional support.
Who may benefit
- Port companies, marine service providers, maritime operators and maritime training providers may all benefit from the findings in this report.
Factual information Pārongo pono
Narrative
- Takitimu II was a pilot and personnel transfer vessel owned and operated by South Port New Zealand Limited Te Pūkorokoro o Murihiku (South Port).
- On 26 December 2024, Takitimu II was scheduled to depart at 0430 (times in this report are in New Zealand Daylight Time (Coordinated Universal Time + 13 hours) and are expressed in the 24-hour format) to transfer a South Port pilot onto a vessel inbound to Bluff.
- The master woke at around 0400 and left for work shortly afterwards. At about 0417, the vessel’s automatic identification system (AIS) was started, and the onboard CCTV system recorded the master and the deckhand already on board.
- The master started the pre-departure checks by inspecting the engine room and checking the engine oil and water levels. Once the master was satisfied with the engine room checks, they went to the wheelhouse and switched on the electronic instruments.
- By 0420, the master had completed the pre-departure checks and recorded them on a checklist that was maintained on a tablet device.
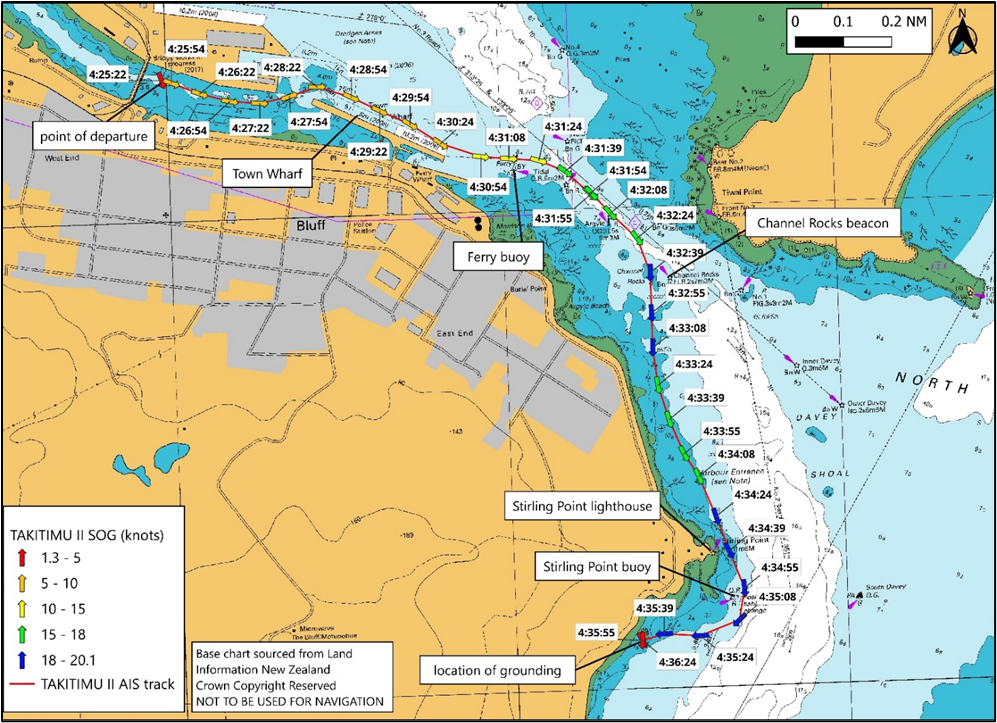
- At about 0425, the pilot boarded and shortly afterwards the vessel left the berth. The master estimated that the visibility was about 100 metres (m) because of fog (the suspension of very small water droplets in the air, reducing the visibility at ground level to less than 0.5 nautical miles (926 m)), so they steered the vessel along the Town Wharf (see Figure 3) and headed towards Ferry buoy once it became visible.
- At 0431, Takitimu II passed north of the Ferry buoy and the master turned the vessel into the main channel. They followed the starboard side of the channel and increased speed to about 15–18 kt (speed over the ground, sourced from AIS recordings).
- Because of the restricted visibility, the deckhand stood in the forward part of the wheelhouse to “stand a watch” (a common and recommended practice in the maritime industry, in which an additional lookout is posted during periods of restricted visibility. Their role is to support the master or officer of the watch by scanning the surroundings for other vessels, navigational marks and any potential navigational hazards, and reporting anything sighted).
labelled by the Transport Accident Investigation Commission)
- At 0432, the master steered the vessel out of the main channel and passed west of the Channel Rocks beacon (see Figure 3). The master increased speed to about 18–20 kt but realised that the vessel was closer to shore than usual, so altered course to seaward. They progressed along the coast slightly inside the five-metre depth contour, towards Stirling Point (see Figure 4).
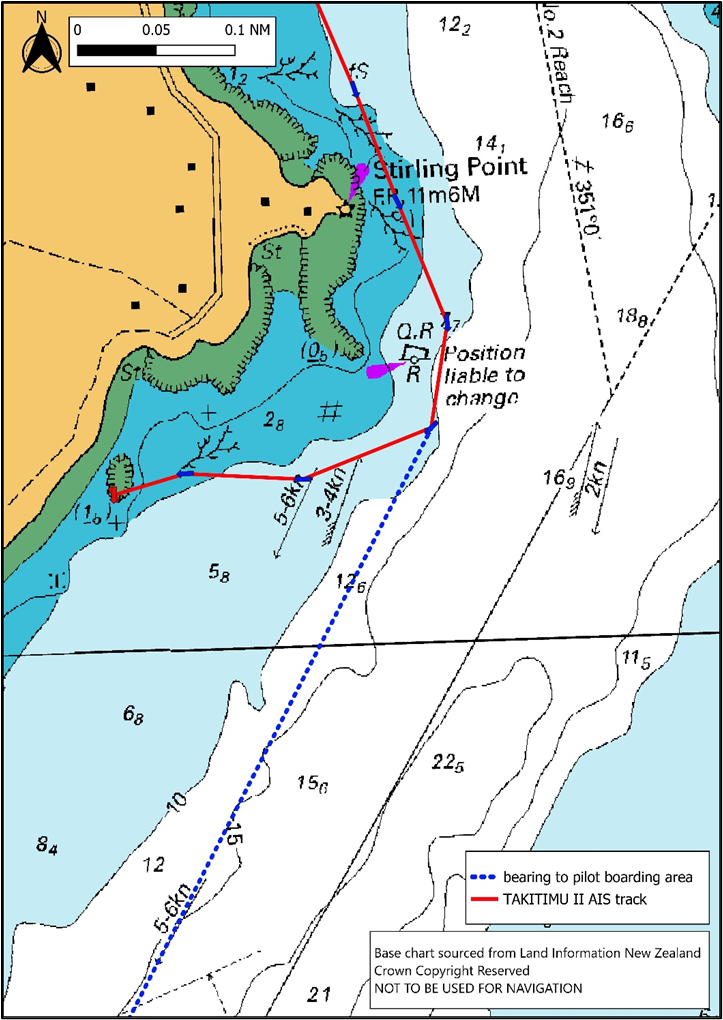
- At about 0435, Takitimu II passed east of the Stirling Point buoy and then altered course to starboard to continue towards the pilot boarding area (see Figure 5). The master was looking for the silhouette of Bluff Hill as their next visual reference to steer by. Shortly after the alteration of course to starboard, the deckhand noticed that the chart plotter and radar screens showed the vessel heading towards the land. The deckhand said to the master that they should be more to port. The master then looked down to check the screens and realised that the vessel was not where it should have been. A few seconds later, the vessel ran aground with both engines still running.
- Initially the master attempted to back off by putting both engines astern, but realised that would be ineffective when they saw rocks on both sides of the vessel and astern.
the charted pilot boarding area
- South Port’s tugs were already manned and preparing to assist with the arrival of the inbound vessel. The pilot called one of the tugs by radio (on very-high-frequency (VHF) radio channel 12) and informed them that Takitimu II was aground and in need of assistance. The pilot also asked the tugmaster to inform management of the accident and request assistance from the South Port workboat and the Coastguard.
- The deckhand checked the underdeck spaces for damage and at this stage there was no water ingress. However, Takitimu II was exposed to the rise and fall of the swell for over an hour while aground on the rocks, causing the loss of the starboard rudder and significant damage to the starboard propeller. Both engines were still operational, but the master shut down the starboard engine after a change in the sound from the starboard propeller.
- The South Port tug Te Matua was the first vessel to arrive on scene but could not safely approach Takitimu II. The South Port workboat arrived next, followed shortly afterwards by the Coastguard vessel. At about 0603, the Coastguard vessel towed Takitimu II off the rocks.
- The master had intended to navigate Takitimu II back into the harbour and to the shiplift under its own power. However, once they were afloat and clear of the rocks, it became apparent that the steering was not functioning and only the port engine was running. So, they were towed into port by Te Matua. At this stage, the deckhand noticed water ingress in the engine room and the aft locker. Before the vessel was lifted out of the water, portable pumps were employed to dewater these spaces.
Personnel information
- The master had been working in the maritime industry for over 40 years. They started working as crew on the Bluff pilot vessels in the early 1990s and obtained their Commercial Launch Master qualification in 1996.
- The deckhand had experience working on a variety of vessels in the area. They had obtained coastal and near-coastal master qualifications in New Zealand and Australia. Additionally, they held a marine engineering qualification. They had worked for South Port for about one year.
Vessel information
- Takitimu II was built in 2006 by Gough Brothers, Invercargill. The primary hull material was aluminium. Propulsion was by shaft and propeller, driven by twin 600 horsepower (hp) (447 kilowatt (kW)) Detroit Diesel engines, which equates to approximately 1198 hp (894 kW) combined. The vessel’s maximum operating limit was the Foveaux Strait inshore limit (inside a straight line starting at Wakaputa Point, from there 198° for 22.9 miles to the shore of Codfish Island / Whenua Hou, from there around the eastern shore of Codfish Island / Whenua Hou to position 46° 46.8’S, 167° 38.5’ E” on the south-eastern shore of Codfish Island / Whenua Hou, from there 090° to the shore of Stewart Island, and a line from Waipapa Point, South Island running 215° for 34.7 miles then 270° for 15.7 miles passing through White Rock to the shore on Stewart Island at 47° 08’S, 167° 59’E) as defined by Maritime Rules Part 20 – Operating Limits.
- Takitimu II was fitted with a radar, a Global Positioning System (GPS)-fed chart plotter and echo sounder. These were connected to two Raymarine multifunction displays.
Meteorological information
-
The MetService Te Ratonga Tirorangi forecast for the Foveaux area, issued at 0310 on Thursday 26 December 2024, stated the following:
Southwest 10 knots, rising to 20 knots for a time in the morning and afternoon.
Sea becoming moderate for a time.
Long period southwest swell 1 metre.
Possible morning fog in the east.
- The tide was ebbing towards a predicted low water of 1.2 m at 0545. The accident occurred during hours of darkness, with the time of sunrise estimated at about 0552.
Recorded data
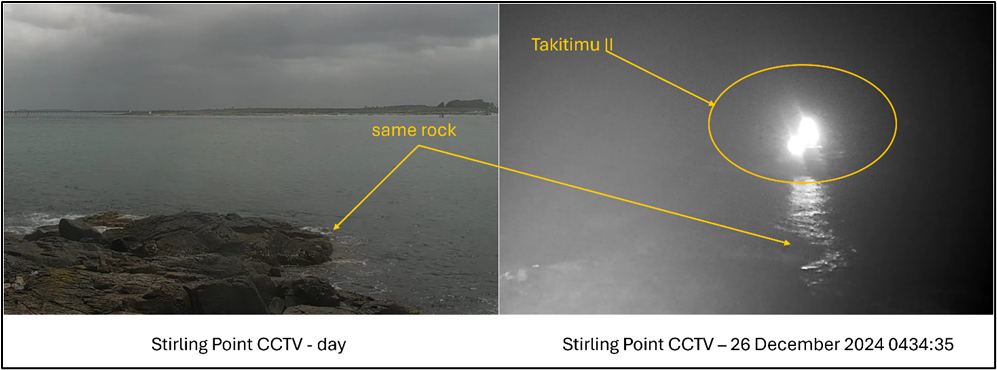
- Recordings of the vessel’s AIS transmissions were obtained from South Port and from another provider. This data was analysed by Commission investigators alongside video recordings from CCTV cameras on board the vessel.
Damage to the vessel
- Takitimu II was lifted out of the water using the shiplift at South Port.

- The damage and repair report, provided by South Port to the Commission, recorded the following damage:
- cracking, deformation and tearing of both propellers (see Figure 7)
- cracking, deformation and tearing of the rudder blades and rudder stocks (see Figure 7)
- cracking, deformation and tearing of the tail shaft, shaft bracket and shaft bearing coupling
- cracking, deformation and tearing of the hull structure, internal framing and independent fuel tank supports.

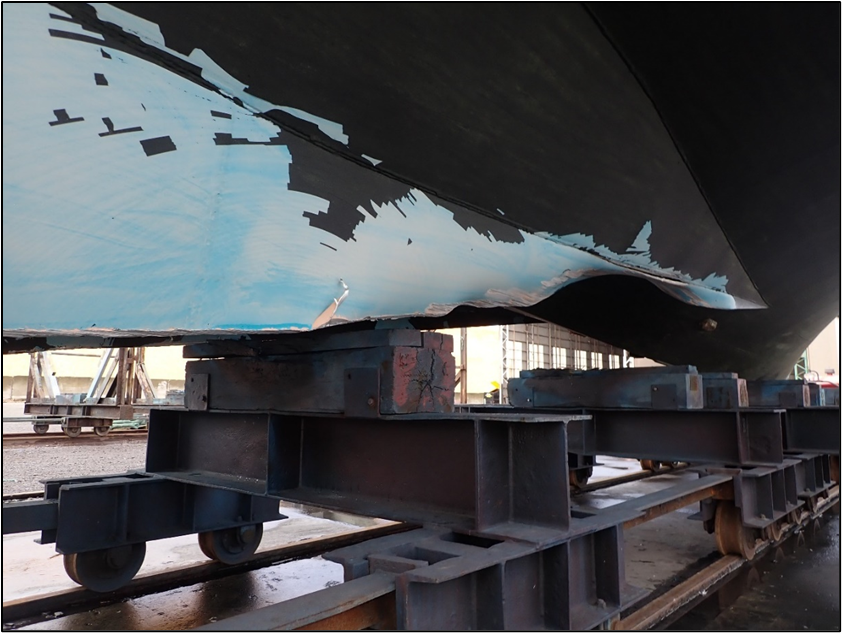
- Paint scrapes on the hull (see Figure 8 and Figure 9) indicated that the vessel struck the rocks with forward momentum, whereas the damage to the rudders and propellers was more consistent with damage from the vessel moving in the seas and swell whilst stranded on the rocks.

Medical information
- The master and the deckhand both had current Maritime New Zealand (MNZ) medical certificates.
- There was no evidence that the accident was the result of a medical event or pre-existing condition.
Tests and research
- South Port conducted drug and alcohol testing for the master and the deckhand. Both returned negative (clear) results.
Previous inquiries
- On 5 October 2023, the pilot vessel Corsair ran aground (Australian Transport Safety Bureau, 2025) on Point Lonsdale Reef at the entrance to Port Phillip, Victoria, Australia. The Australian Transport Safety Bureau found that the coxswain of the Corsair misinterpreted the navigational lights marking the entrance to Port Phillip and navigated to the west of their intended course. The return to Port Phillip following offshore pilot transfer was a routine activity and the coxswain had transited the entrance many times. Their perceptions were probably influenced by expectation and confirmation bias. The coxswain relied on their visual observations of navigational aids and did not make effective use of available onboard navigation equipment to monitor the vessel’s safe return through the entrance to Port Phillip. The navigational equipment on Corsair had additional (unused) features that could have further assisted navigation through Port Phillip Heads.
Organisational information
- South Port provides pilotage, towage, berthage and full marine services to international, coastal and southern fishing fleet vessels. Pilots board inbound vessels 1.5–2 NM south of Bluff Entrance light.
Analysis Tātaritanga
Introduction
- Throughout maritime history, restricted visibility has been regarded as particularly hazardous to navigation. The advent of electronic navigation systems has allowed vessel and port operators to broaden their safe-operating parameters to include restricted-visibility conditions that would have once stopped operations altogether.
- When Takitimu II left South Port on 26 December 2024, the master was aware that fog was forecast and present. This was not considered to be in any way problematic as the master was very experienced and the vessel well equipped.
- The master navigated Takitimu II primarily by visual references, which were more appropriate for good-visibility conditions. When the master checked the vessel’s position after the deckhand raised their concerns, it was too late to avoid running aground.
- As part of its inquiry, the Commission determined that this accident was not the result of a mechanical failure, distraction or medical condition or event.
- The following section analyses the circumstances surrounding the event to identify those factors that increased the likelihood of the event occurring or increased the severity of its outcome. It also examines any safety issues that have the potential to adversely affect future operations.
Navigating in restricted visibility
- The master and the deckhand were expecting fog because it had been forecast. As Takitimu II departed its berth, the master was navigating by visual methods and steering by hand. The master estimated that the visibility was about 100 m when they left the berth. They were able to identify the channel markers and other lights of the harbour, and they were able to determine their progress and position in relation to the channel buoys and beacons. However, once they passed Stirling Point there were fewer navigational marks to support their situational awareness. To steer by night, the master normally oriented themself using the silhouette of Bluff Hill. On the morning of the accident, despite being able to see Stirling Point light and Stirling Point buoy, the master could not see the silhouette of Bluff Hill and they did not seek alternative cross references to inform their navigation of the vessel.
- Section 19 of the Maritime Transport Act 1994 outlines the duties of masters, including being responsible for the safe operation of the vessel on a voyage, the safety and wellbeing of all passengers and crew, and the safety of cargo carried. The decisions rest with the master on how to safely operate the vessel in the forecast and encountered conditions. Such decisions can be informed by their training and qualification, experience, attitude and ability. The master informed the Commission that their preference was to navigate by visual methods, and they did not often practise other navigation methods to support their perception of the vessel’s movement through its immediate environment. It was normal practice for South Port’s pilot-vessel masters to turn the vessel out of the channel at Channel Rocks beacon and navigate closer to the shore. The water along this route was less affected by the sea and tidal conditions. However, on this occasion, the master continued to navigate visually at a speed that did not allow sufficient time and sea room to assess the situation when they became uncertain of the vessel’s position.
- The navigation instruments on board Takitimu II were sufficient for the safe execution of pilot-transfer operations in the visibility conditions at the time. There are many basic navigation techniques – both visual and electronic – that may have helped prevent this accident if they had been employed.
- Unless there is a speed limit mandated by local authorities, or stipulated by the vessel’s managers, the master will determine the speed at which the vessel proceeds.
- Determining a safe and appropriate speed is subjective and influenced by numerous factors. Maritime rules for collision prevention (Maritime Rules Part 22 – Collision Prevention) define a safe speed as one that allows for timely identification of risk of collision, leading to proper and effective collision-avoidance action, and for the vessel to be stopped in a distance appropriate to the prevailing circumstances and conditions. Through the collision-prevention lens, all masters must consider, amongst other factors, the state of the visibility, the manoeuvrability of the vessel and the proximity of navigational hazards in determining a safe speed.
- Because Takitimu II was travelling at about 18–20 kt, once the master turned too far to starboard there was very little opportunity to identify the error and correct it before running aground. The master may have had more time to verify the vessel’s position and correct their course towards navigable water if they had been proceeding at a slower speed. Immediately before the accident, the master was uncertain of their interpretation of their surroundings and was searching for their next visual cue, Bluff Hill, which could have been obscured by the visibility conditions at the time. Operating at a slower speed gives a master more time to verify their position by cross checking visual cues with electronic navigation methods, which are less vulnerable to restricted visibility than the human eye.
- A common operational risk associated with repetitive tasks is that sometimes a person can find a comfortable way to do a job that is appropriate for most of the conditions that they will encounter. However, if they do not practise for conditions outside their comfort zone, they may find themselves under additional pressure when they must recall these techniques in earnest.
- It is important for maritime operators to verify periodically that masters are practising appropriate navigation methods on their vessels, to mitigate this risk and provide support where required.
Oversight of ongoing proficiency
Safety issue: At the time of the accident, South Port’s Maritime Transport Operator Plan did not require an assessment of the ongoing proficiency of pilot-vessel masters. This omission meant that there was no formal verification that navigation practices on board the pilot vessel continued to meet industry best practice.
- The master of Takitimu II was very experienced and had started working on the Bluff pilot vessels before South Port became an operator under MNZ’s Maritime Operator Safety System (MOSS) (Maritime Rules Part 19 – Maritime transport operator certification and responsibilities, under which defined maritime operators must develop an MTOP, were signed into law by the Minister of Transport in October 2013 and entered into force on 1 April 2014. Operators had to comply by July 2014). South Port did not have records of the master’s onboard training and familiarisation because the master’s position as a pilot-vessel master predated the safety management system.
- South Port developed and introduced its Maritime Transport Operator Plan (MTOP), which described the qualities expected from their launch masters (launch masters included pilot-vessel masters and those employed to work on other launch-type vessels operated by South Port). These qualities included competence, ability and reliability. However, the plan did not include periodic checks to identify whether masters need additional training and support to ensure their ongoing proficiency. Periodic verification of onboard practices and proficiency were required for South Port’s pilots and tug masters, but not for the pilot-vessel masters.
- The primary operations conducted by a pilot vessel are:
- to take a pilot out to the pilot boarding area and provide a moving platform from which to safely transfer the pilot onto an inbound ship
- crew transfers
- to provide a moving platform to transfer a pilot from an outbound ship and return them to port
- to assist with vessel manoeuvres in port.
- South Port’s marine services were managed under a high-trust model that acknowledged the competence and experience of its maritime staff. However, this remote oversight did not provide opportunities to identify whether pilot-vessel masters and crew required more specific instruction or additional training and support. Navigation practices employed in restricted visibility were at the master’s discretion, but the MTOP had no standing orders or similar instructions to inform the master’s decisions. It is generally accepted as good practice to use all available means to determine a vessel’s position, monitor its progress and cross check the veracity of one method with the other.
- During their interview, the master confirmed that they had received a brief induction about the use of the radar and the chart plotter when the equipment was installed on Takitimu II. Any further practice of electronic navigation techniques was at the master’s discretion. It was not evident that South Port had requested its pilot-vessel masters to practise electronic navigation techniques before they were needed in earnest.
- The master usually navigated by eye with the vessel’s two Raymarine multi-screens (see Figure 10) displaying the GPS-fed chart plotter and the CCTV. Because of the restricted visibility conditions on the accident trip, the master set the Raymarine screens to display the GPS-fed chart plotter and the radar. However, they continued to navigate visually as navigation marks came into sight and did not regularly reference the chart plotter or radar until it was too late to avoid the rocks.

- Following this accident, South Port revised its pilot-vessel training scheme. The new scheme documents the operational standards that South Port expects from its pilot-vessel masters and crews and includes a six-monthly proficiency assessment. In the Commission’s view, this safety action has addressed the safety issue. Therefore, the Commission has not made a recommendation.