The Interislander ferry Aratere grounded after an inadvertent turn toward shore while on autopilot. The crew were unable to regain steering control. Key factors were change management of safety-critical upgrade to the steering system, operational differences not fully identified and inadequate sea trials and training. Ineffective audit reduced management oversight of bridge practices that may have reduced error detection.
Executive summary Tuhinga whakarāpopoto

What happened
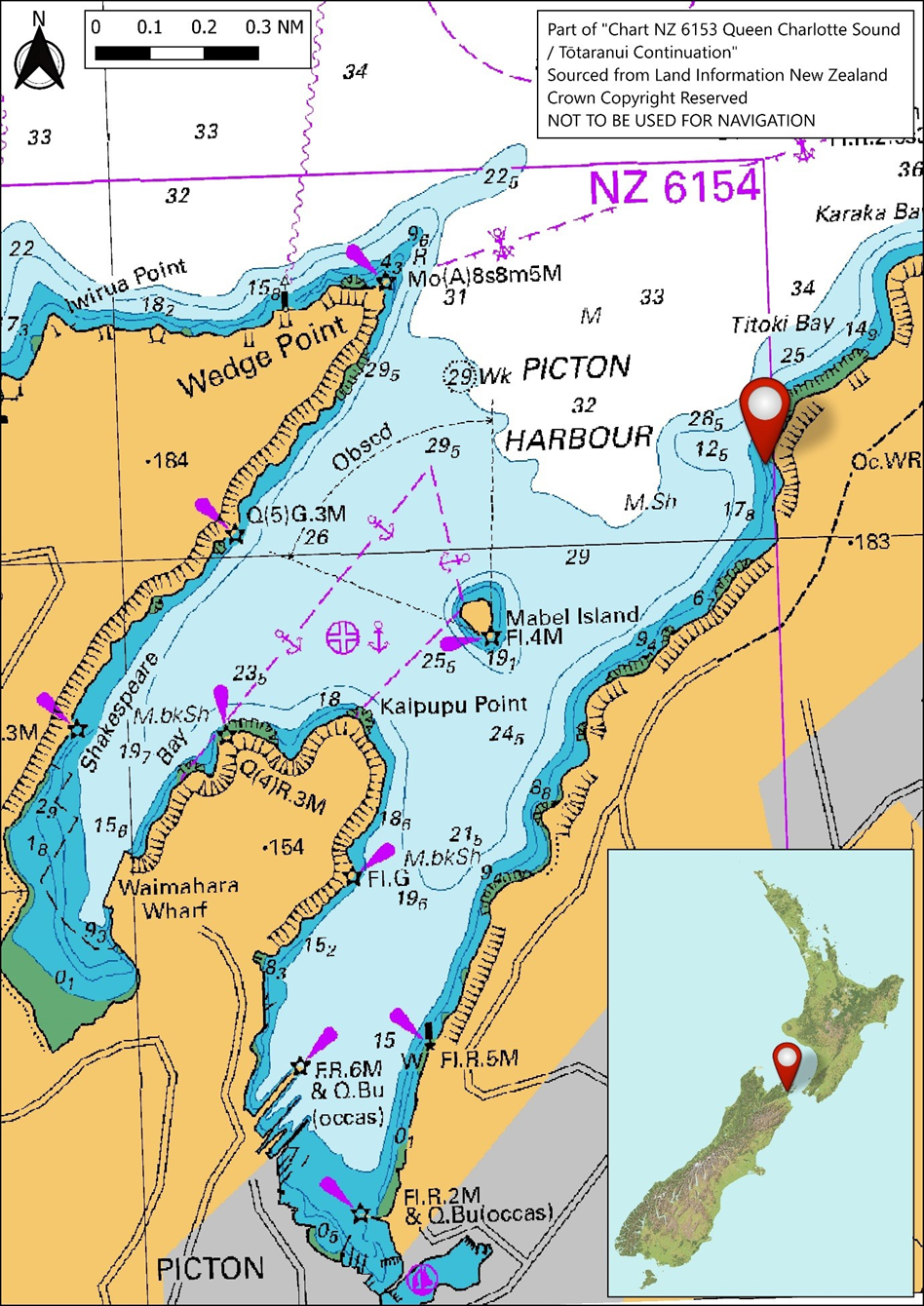
- On 21 June 2024, shortly after the Aratere (operated by Interislander) left Picton bound for Wellington, the pilot engaged the autopilot to control the rudders of the ship. A few minutes later the pilot pressed the ‘execute’ button on the autopilot, expecting the autopilot would perform a programmed three degree (°) turn to starboard, as per the passage plan.
- The ship had already passed that course alteration position, and the autopilot had locked on to the next course alteration position where the programmed turn was a 34° turn to starboard. As a result, upon pressing the execute button, the autopilot initiated the starboard turn, causing the ship to veer out of the channel towards the shore.
- When the bridge team realised that the ship’s turn to starboard was much greater than expected, they immediately attempted to transfer control of the rudders back to manual steering but were unable to do so.
- The crew attempted to stop the ship using astern thrust on the main propulsion system. The ship ran aground while slowing down.
Why it happened
- Spare parts were becoming difficult to source for the Aratere’s original steering control system and manufacturer support was declining. Interislander had chosen to replace the system with another which was considered like-for-like. The ship had been sailing between Wellington and Picton for three weeks following the replacement.
- Inadequate implementation of Aratere’s safe navigation procedures, including bridge resource management, meant the risk mitigations inherent to those procedures were ineffective. For example, there was no robust shared mental model of the planned passage and use of bridge equipment, bridge team member roles lacked clarity, communication lacked a closed loop structure, and steering commands were not adequately monitored. The master was also distracted to some degree by training duties. As a result, the inadvertent turn to starboard was able to occur.
- The safety management system included an audit and assessment programme to provide assurance that the safe navigation procedures were implemented, but the audit system itself was not enforced. Hence, Interislander management did not have adequate visibility on the status of its safe navigation procedures in practice and implementation lapses could go unnoticed and unaddressed.
- Once the crew members realised the error, they were unable to take manual control of the rudders because they were not familiar with critical procedures for the newly installed steering control system that differed from the old system.
- In particular, a feature of the steering control system was that control of the rudders could not transfer between consoles (for example from the autopilot to manual steering) unless their respective rudder commands were aligned within 2°. Control of the rudders could be forced from track pilot (the track pilot module is a module within an integrated bridge navigation system that includes an electronic chart display and information system, radar, position-indicating systems and sensors (for example, ship speed, rates of turn and water depth)) to the central helmsperson steering console, even without alignment, if the ‘take command’ button was pressed for 5 seconds (s). The crew members were not trained on either of these features.
- The recent upgrade to the steering control system had introduced safety-critical changes to rudder control procedures that were not identified, nor addressed via training. There was no appointed project manager with overall responsibility from the project’s initiation through to the ship's safe return to service. As a result, the management of change was overlooked and no structured evaluation of differences between the new and old systems was conducted.
What we can learn
- Any changes to safety-critical equipment, such as steering control systems, should include thorough risk analysis to identify any functional differences or potential changes to procedures, including specific training requirements for users.
- The benefits of safe navigation procedures can be lost if the procedures are not consistently and fully implemented on all passages.
- Quality assurance programmes, such as audits and assessments, are an important part of ensuring safety-critical procedures are consistently and fully implemented.
- The success of safety-critical projects is dependent on a clear scope of responsibility and accountability for the project manager, and a strong management of change process, from the project’s initiation through to a ship's safe return to service.
Who may benefit
- Ship operators, ship crew, those who operate safety management systems, auditors and regulators, maritime industry bodies, maritime training institutes, and any entities that introduce changes to safety-critical equipment may benefit from the findings and recommendations in this report.
Factual information Pārongo pono
Background
- The Aratere is part of the Interislander fleet, which is owned and operated by KiwiRail Holdings Limited. The Aratere, had been in service for about 26 years at the time of the accident. Interislander identified that the control system for the steering machinery (the electro-hydraulic system and rudders; the steering control system) required replacement because spare parts were becoming difficult to source and manufacturer support was declining.
- The purpose of the steering control system was to relay the rudder commands from the navigators on the bridge to the electro-hydraulic steering motors located in the steering room at the stern. This then turned the twin rudders to match the commands from the bridge. The steering control system was also integrated with the vessel’s electronic chart display and information system (ECDIS) (Electronic Chart Display and Information System is a system that integrates navigational information to assist the crew in maintaining situational awareness and navigational safety) when in all track pilot modes.
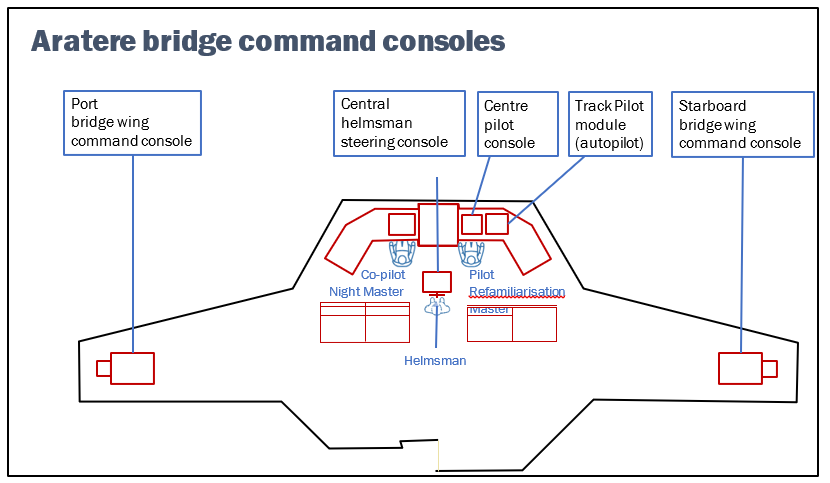
- On the bridge, steering could be controlled from any one of five command consoles (see Figure 3):
- the port (the left-hand side of the ship looking forward) bridge wing console
- the starboard (the right-hand side of the ship looking forward) bridge wing console
- the centre pilot console
- the central helmsperson (a person who steers a ship) steering console (which contained the wheel)
- the track pilot module (a module within an integrated bridge navigation system that includes an electronic chart display and information system, radar, position-indicating systems and sensors (for example, ship speed, rates of turn and water depth; incorporating the autopilot).
- Control of the rudders could be transferred to any one of the five command consoles.
- In September 2023, Interislander had opted to replace the Aratere’s steering control system with a system produced by Kongsberg (a major supplier of industrial sensors, robotics and digital systems).
- This involved replacing the controls at each of the command consoles, except for the autopilot. The autopilot was part of the original track pilot integrated bridge navigation system, made by a different manufacturer. The new Kongsberg steering control system was integrated with the track pilot.
- The steering control system had been installed and commissioned during a ‘wet docking’ (an extended period out of service to conduct maintenance not requiring the ship to be dry-docked) period in Wellington between 11 and 30 May 2024.
- The Aratere’s safe navigation procedures within its safety management system (SMS) prescribed two critical bridge team roles while navigating in pilotage waters: the pilot and the co-pilot. Only the master or officer of the watch (OOW) (the deck officer assigned to watch keeping and navigation on a ship’s bridge) could be assigned as pilot. The full descriptions of bridge duties for pilot and co-pilot are shown in Appendix 1, and some pertinent points are presented here.
- The pilot had the con (‘having the con’ means conducting the navigational command of the ship) of the ship, initiated all manoeuvres, and had responsibility for the successful execution of the passage plan.
- The co-pilot had significant and broad responsibilities, including (but not limited to) monitoring the ship’s position against the passage plan, following up on all manoeuvres and navigation made by the pilot, reviewing all actions taken by the pilot and maintaining awareness of all planned actions, being in charge of operational checklists, and communicating with parties external to the bridge (for example, by VHF radio, or with the engine room).
Narrative
- After re-entering service following the installation and commission of the new steering control system, Aratere completed 83 inter-island crossings in the subsequent three weeks. Unrelated to the steering control system, the Aratere’s starboard propeller shaft was running on reduced power because of an issue with the gearbox.
- On 21 June 2024, at 2110 (times are in New Zealand Standard Time (coordinated universal time (UTC) +12 hours) and expressed in 24-hour format) the Aratere completed loading at Picton in preparation for the passage to Wellington with 48 people and freight on board. Two masters (day master and night master) were on board to share the workload. The night master was in command for the departure from Picton while the day master was resting.
- An additional experienced master (the relieving master - a qualified master who temporarily takes command of a vessel when the regular master is absent) was also on board for refamiliarisation training with the ship, having not sailed on Aratere for some time. Following the refamiliarisation training, they were to relieve the master. Normally the night master would have been the pilot and the OOW would have been the co-pilot. For this departure from Picton, the night master was acting as co-pilot and supervising the relieving master who was acting as pilot.
- The OOW was on the bridge assisting as required. There were also two deck ratings (skilled seafarers who provide support with navigation, maintenance, security and other shipboard operations) on the bridge, one acting as lookout and the other as helmsperson.
- Aratere left the berth at 2119. The relieving master was operating the engine controls from the port bridge wing, supervised by the night master. The helmsperson was steering the ship using the central wheel.
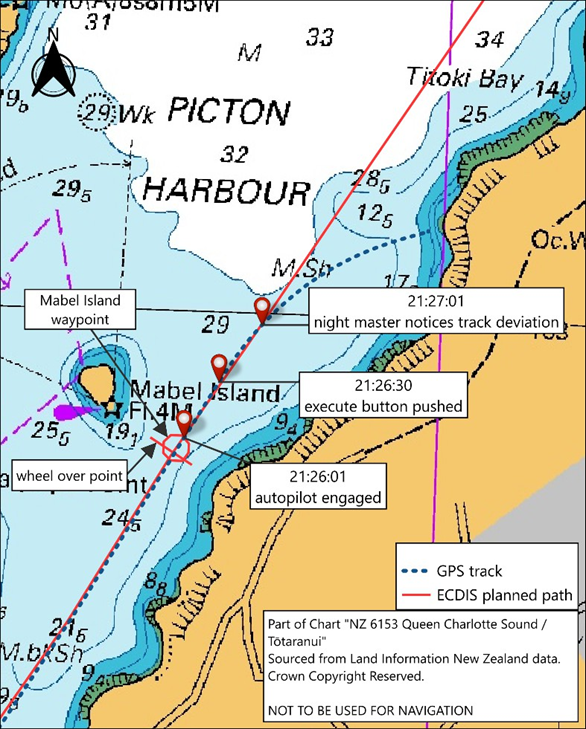
- Once clear of the berth, the relieving master asked the helmsperson to steer 030 degrees (°) true to head for the first waypoint (a coordinate or location along a route, usually where the course changes or a voyage starts or ends) off Mabel Island. Soon after that, they adjusted the course to 028° as Aratere was slightly too starboard of the track. The night master transferred control of the engines to the centre pilot console.
- The course between the Mabel Island waypoint and the Snout waypoint (programmed into the electronic chart display and information system (ECDIS) as Picton Point) (the next waypoint) was 033° true. This was a small alteration of 3° to starboard (see Figure 4).

- The night master normally waited until the ship was clear of Mabel Island before engaging the autopilot. When Aratere was about abeam (at right angles to the ship’s heading) of Mabel Island, the night master and relieving master discussed whether to use ‘heading mode’ (the ship will steer the acquired heading) or ‘course mode’ (the ship will steer the acquired heading, but will automatically detect any sideways deviation arising from current and wind, and will adjust the heading to achieve the acquired course) for the autopilot. The autopilot was engaged on the ship’s current heading of 028° in course mode, after which the helmsperson was released from the wheel to stand by on the bridge.
- From that point onwards the direction of the ship was controlled by the autopilot through the track pilot module.
- The planned track for the passage to Wellington had been programmed into the track pilot as a series of waypoints joined by the track/course lines. The transition from one course to the next at each waypoint was programmed as an arc with a set radius. A wheel-over point (the point at which a turn is initiated and the rudders are rotated) was displayed before each waypoint (see Figure 4).
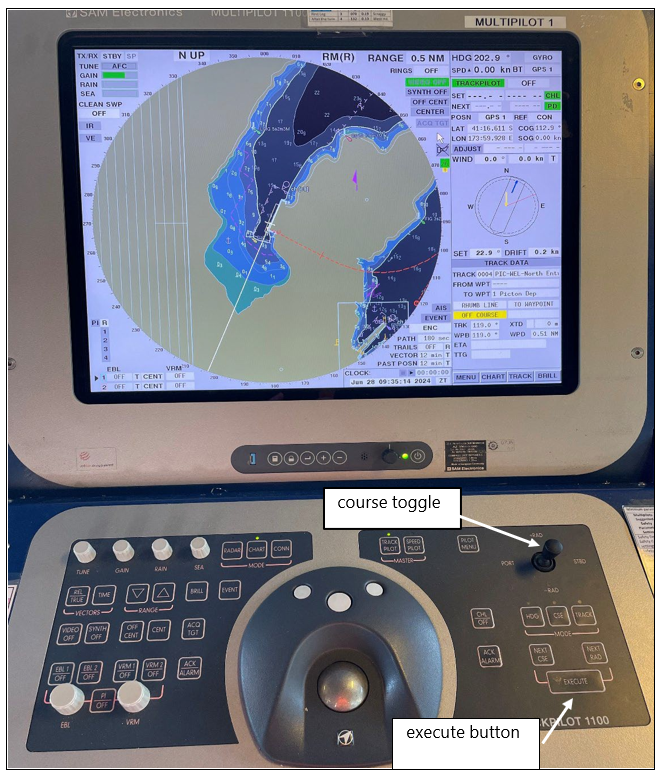
- When in course or track mode (the ship will automatically follow the planned track programmed into the autopilot), the track pilot receives additional information from the ECDIS, such as wheel-over point. However, in course mode the track pilot will not automatically begin the turn. The pilot must push the ‘execute’ button. The track pilot will then apply the required rudder to take the ship around the programmed arc onto the next course. The pilot can make manual adjustments to the course using the course toggle control (see Figure 5).
- Once the ship has passed a waypoint, the track pilot will automatically lock onto the radius turn for the next waypoint and the next course after achieving the turn.
- The autopilot was engaged at 2126:01 when the ship was on a heading of 028° (see Figure 6). The relieving master pushed the execute button at about 2126:30 (as detailed by the after-accident technical report provided by the equipment service technician. The Voyage Date Recorder recorded when the command was actioned and the rudder angle changed). However, Aratere had passed the Mabel Island waypoint 36 s earlier, and the track pilot had already automatically locked on to the next substantial turn around the Snout waypoint (see Figure 7).
- The track pilot applied 9°of initial starboard rudder and began to make a controlled turn as if the ship were making the turn around the Snout waypoint.
- After 31 s, the night master realised from the ECDIS that Aratere was deviating to starboard of the track towards the shore. The night master immediately instructed the helmsperson to take over steering on the wheel, located on the central helmsperson steering console, and to put the rudder ‘hard over to port’.
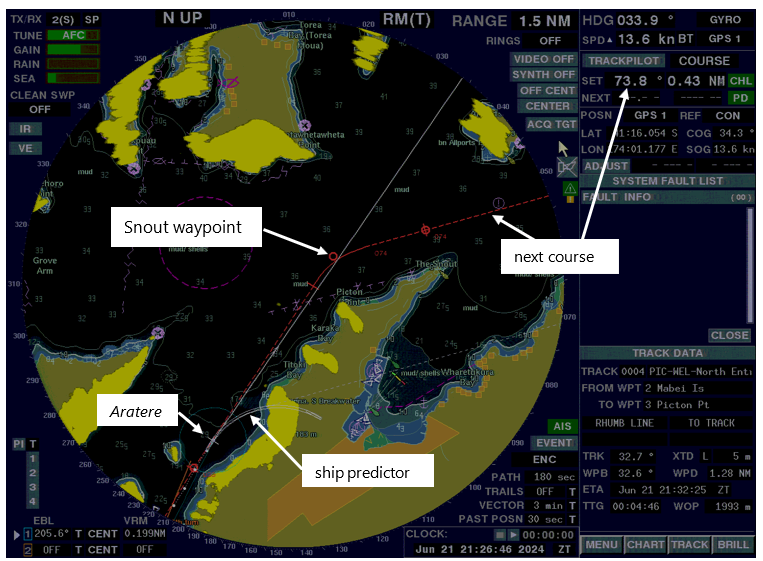
- Figure 7 shows a marked-up screenshot of Aratere’s ECDIS near the time the night master became aware that Aratere was deviating from the planned track. The set course was displayed as 73.8° with a radius turn of 0.43 nautical miles (NM), which was the next turn and course around the Snout waypoint. The ship predictor is a feature that shows the pilot where the ship will be in the immediate future, based on current speed and rate of turn.
- The helmsperson pressed the ‘takeover’ button on the central helmsperson steering console (the action of the helmsperson pressing the button rather than a qualified officer was performed because the takeover button was located in the helmsperson position) in an attempt to transfer control from the autopilot to hand steering, and then turned the wheel hard to port. However, the transfer of steering command from the track pilot module to the wheel position did not occur and Aratere continued its turn to starboard, still controlled by the autopilot.
- The OOW rushed to the central helmsperson steering console and pushed the takeover button, but with the same result. The autopilot had applied starboard rudder, but the helmsperson had the wheel set to amidships (a command to align the rudders with the fore and aft centreline of a ship), meaning the rudder commands between the two command consoles were not aligned.
- The night master also attempted to take control of the rudders at the centre pilot console, but without success.
- At 2127:43, recognising that the helmsperson did not have control of the steering and seeing that Aratere was already heading towards the shore, the night master put both engine combinators (the lever that controls the speed and direction of the ship’s propulsion systems) at full astern (moving aft or towards the rear of the ship) (41 s after noticing Aratere veering to starboard). Aratere was moving at 13 knots (kt) over the ground at that time.
- It took 21 s for the port propeller and 38 s for the starboard propeller to begin turning astern, at 2128:04 and 2128:21 respectively (the starboard propeller shaft was running on reduced power because of a gearbox issue).
- Records show that at 2128:06 the alternative non-follow-up mode of steering (an alternative mode of steering to the follow-up mode, in which the rudder will continue to move in the direction in which the lever is placed until the lever is released, after which the rudder will stay in that position until the lever is moved again) was engaged; this mode used the independent tillers on the centre pilot console. The port rudder moved hard to port (32°) and the starboard rudder moved 13° to port.
- During this sequence, the night master instructed the OOW to start the ship’s bow thrusters (a propulsion unit mounted in an athwartships (from one side of the ship to another) tunnel near the bow that is used to thrust the bow to port or starboard when manoeuvring) to assist in manoeuvring the ship. The bow thrusters were put into ‘standby’ mode, but due to the startup time only one of the thrusters was providing thrust at the time of the grounding.
- At 2128:34 Aratere crossed the 10-metre (m) sounding (water depth of 10 m on the chart where the ship would have been clear of the seabed) at about 8 kt. At 2128:46 the speed had dropped to about 1 kt. By 2128:50 the ship had stopped and was aground on a heading of 76.5° (the ship decelerated because of the actions taken by the crew, and also the subsequent friction of the ship on the seabed as it ran aground. The precise time the ship touched the seabed is not determined).
- The watertight integrity of the Aratere’s hull was not compromised, but the grounding dented the hull plating of the bulbous bow, and the internal structure sustained damage that required remedial repair before the ship’s return to service. There were no injuries.
Emergency response
- The Picton Harbourmaster was notified of the accident by a local pilot, soon after the grounding had occurred. The harbourmaster began mobilising a response team to assemble at the Marlborough District Council’s Nautical and Coastal office in Picton.
- At about 2156, approximately 27 minutes (min) after the vessel had stopped, Interislander notified the Rescue Coordination Centre New Zealand (RCCNZ) that the Aratere had run aground. They noted there was no water ingress and they were waiting for tugs to assist the ship back to berth in Picton. At about the same time, a crew member dialled 111 notifying New Zealand Police, and a response was initiated.
- By 2315, the master confirmed that there was no immediate threat to life, and the ship was stable. All 48 people on board were well and in good spirits
- At 2332, RCCNZ and Police agreed that the operation would continue to be led by Police with support from RCCNZ, where required.
- Meanwhile Maritime New Zealand (Maritime NZ) activated the Maritime Incident Response Team (MIRT) and appointed a national incident controller.
- By 2351, the decision was made that the safest option was to leave the passengers and crew on board and attempt to refloat the ship at the next high tide, during daylight hours, as the ship was in a relatively stable condition.
- As a result, Police and RCCNZ de-escalated their operations as there was no immediate threat to life that would require a search and rescue operation.
- In the following two days, various authorities were involved in overseeing Aratere being refloated using two Picton-based harbour tugs.
Crew information
- The night master first gained their Master’s Certificate of Competency (CoC) in 1995 and was most recently revalidated in September 2020. They joined Interislander in 2009 and first sailed as master on the Aratere in 2018.
- The relieving master first joined the Cook Strait inter-island ferry service (Between Wellington in the North Island and Picton in the South Island), that eventually became KiwiRail’s Interislander, in 1970. They were first issued a Master’s CoC in 1995 and began sailing as master of the Aratere in about 2003. After approximately five years working overseas, they returned to Interislander in 2016 to the role of superintendent. They had most recently completed a refamiliarisation of the Aratere as master in about 2020, and revalidated their CoC in March 2023.
- The second mate OOW was issued a Watchkeeper Deck CoC in January 2021, and had worked at Interislander since April 2023.
- The crew on the bridge were all aware the steering control system had been replaced.
- The officers on the bridge were all trained in bridge resource management (BRM).

Ship information
- Aratere was purpose built in 1998 to operate on the Cook Strait inter-island ferry service. The ship was owned by KiwiRail and operated by its subsidiary under the trading name Interislander. The Aratere was retired from service on 18 August 2025.
- The Aratere was certified to carry a total of 720 people and could carry both rail and vehicular cargo.
- The Aratere’s propulsion system was diesel–electric. The system included six diesel-driven generators that powered electric propulsion motors to drive two fixed-pitch propellors via two propellor shafts.
- The Aratere’s steering was provided by two rudders powered by an electro-hydraulic system. The steering control system included the control panels on the bridge and the cabling down to the steering flat (the compartment at the aft end of a ship that houses the steering gear and associated equipment used to operate the rudder). That system was replaced during wet docking before the accident. The new steering control system was the Kongsberg K-Steering 600 KM SG, which was designed for ships with single or twin rudders and could be integrated with autopilot and dynamic positioning systems (dynamic positioning systems are computer-controlled systems used on ships to maintain their position using propellors and thrusters instead of anchors).
- Once the Aratere had returned to service after the new steering control system was installed, the crew reported numerous alarms sounding during normal operations. These were reported to shoreside management who were working on the issue. This is discussed in section 3 of the report.
-
The Aratere’s steering control system (both old and new) controlled the rudder by either ‘follow-up’ or ‘non-follow-up’ steering control modes:
Follow-up steering control: The crew set a desired rudder angle (e.g. 5° port) using the wheel or control, and the rudder moved to that angle and stopped.
While in follow-up mode, the new steering control system had two methods for transferring control between the command consoles:
1. align the rudder commands on both consoles, then press the ‘take command’ button on the console, taking control; or
2. press and hold the ‘take command’ button on the central helmsperson steering consol for five seconds to force transfer of control from track pilot to the central helmsperson steering console, regardless of alignment.
Non-follow-up steering control: The steering command was a direction (e.g. port); the rudder continued moving in that direction while the control was held, stopping when the control was either released or the rudder reached its limit.
- The Aratere’s steering control system included two non-follow-up tillers (the tillers were hand-sized levers) on the centre pilot console, one for each rudder. The tillers were connected directly to the steering system and when activated would override other steering commands. They were an alternative steering control which met the requirements of the maritime rules to establish immediate manual control of the steering in emergency situations.
- Although neither Interislander nor the crew were aware of the forced control transfer feature until after the accident, post-accident testing by the crew showed that it did not work as expected when transferring control to the bridge wings (the forced control transfer feature did work as expected when transferring control to the central helmsperson steering console, as was attempted during the accident).
Previous occurrences
- The Commission found that there were two primary safety issues that contributed to the grounding. The first related to insufficient implementation of safe navigation procedures, including bridge resource management, because of a lack of quality assurance of those procedures via audits and assessments. The second related to inadequate project management of a project to replace a safety-critical system, which resulted in a lack of systematic management of change.
- The Commission has previously made recommendations on safety issues similar to those described in this report; two of those recommendations were to KiwiRail and related to Interislander.
Safe navigation practices and quality assurance
- Maritime inquiry MO-2011-202 (Transport Accident Investigation Commission, 2016a): A failure in implementation of BRM contributed to the Monte Stello running aground at the entrance to Tory Channel. The Commission recommended that the chief executive of KiwiRail ensure that the BRM policy and procedures outlined in its SMS remain relevant and effective for all crews on all ships in the fleet, all of the time. (see Recommendation 010/16).
- Maritime inquiry MO-2011-204 (Transport Accident Investigation Commission, 2014): Failure to follow safe navigation procedures, including BRM, contributed to the grounding of the Rena. The Commission recommended that the Rena’s manager, CIEL Shipmanagement S.A., evaluate the effectiveness of its SMS to ensure that the issues identified with that system as applied on board the Rena do not affect other ships within its fleet (see Recommendation 010/14).
- Maritime inquiry MO-2014-203 (Transport Accident Investigation Commission, 2016c): Weak auditing was linked to non-compliance with safety procedures. The Commission recommended that the operator of the Captain M. J. Souza review its internal auditing procedures to ensure that auditors make realistic assessments based on actual practices observed on board; and seek verification that documented procedures are being followed by the crew and are appropriate for the task. Audit findings should be recorded together with any safety actions taken as a result of the audit (see Recommendation 020/16).
- Maritime inquiry MO-2018-203 (Transport Accident Investigation Commission, 2019): A failure in BRM contributed to the Leda Maersk running aground. The Commission recommended to the chief executive of Maersk Line A/S that they review the implementation of the company’s SMS across its fleet with respect to navigation and pilotage, and take the necessary steps to ensure a high standard is achieved by all crews on all its ships (see Recommendation 005/19).
- Maritime inquiry MO-2024-203 (Transport Accident Investigation Commission, 2025b): Poor passage planning and unsafe navigation practices contributed to the grounding of the Chokyo Maru. The Commission recommended that Yugen Kaisha Chokyu take steps to ensure the effectiveness of its safety management practices with respect to voyage planning and navigation, and take steps to ensure the safe navigation of ships in its fleet (see Recommendation 027/25).
Project management/change management
- Maritime inquiry MO-2013-203 (Transport Accident Investigation Commission, 2016b): After major alterations, one of the passenger and freight ferry Aratere’s propellers fell off while on passage. The Commission recommended that the chief executive of KiwiRail ensure that when KiwiRail makes significant modifications to ships, appropriate oversight is in place. Oversight includes keeping comprehensive records to demonstrate that components are safe and reliable and comply with the appropriate standards (see Recommendation 014/15).
- Maritime inquiry MO-2015-201 (Transport Accident Investigation Commission, 2017): Insufficient oversight during changes to safety-critical systems contributed to the Kea collision with a wharf. The Commission recommended that Maritime NZ issue guidance and advice to operators and surveyors about the need to take a risk-based approach when determining the level of surveyor oversight required for changes to critical systems, regardless of whether or not the changes are considered major modifications (see Recommendation 026/17).
- Rail inquiry RO-2017-102 (Transport Accident Investigation Commission, 2018): Inadequate management of change to the signals system led to unsafe system configuration. The Commission recommended that the chief executive of KiwiRail review KiwiRail’s change management processes for modifying existing, and building new, safety-critical systems. KiwiRail should ensure that these change management processes include a full failure-mode-effect analysis and functional testing is performed before the new or modified systems are put into service (see Recommendation 010/18).
- Maritime inquiry MO-2023-205 (Transport Accident Investigation Commission, 2025a): Inadequate quality assurance and management of change led to the rudder falling off the Archilles Bulker. The Commission recommended that Maritime NZ investigate and submit papers as appropriate to the IMO (through the appropriate subcommittee) to promote standards that ensure sufficient quality assurance for rudder systems throughout the processes of installation, alterations, major repairs and maintenance. (see Recommendation 044/25).
Regulatory structure
- The IMO is the United Nations’ agency responsible for regulating global maritime safety. Two key IMO conventions are the Safety of Life at Sea (SOLAS) Convention and the Standards of Training, Certification and Watchkeeping for Seafarers (STCW) Convention.
- The objective of the SOLAS Convention is to specify minimum safety standards for the construction, equipment and operation of ships. The objective of the STCW Convention is to set the minimum global standards for the training and qualifications of seafarers.
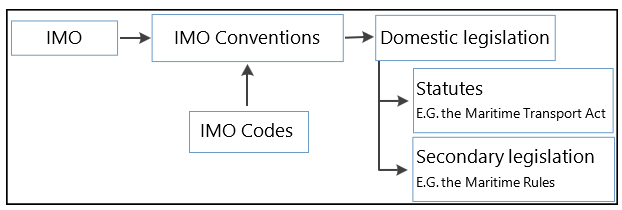
- Signatory countries are obliged to give effect to the SOLAS Convention and STCW Convention through their domestic legislation (see Figure 8).
- A flag State is the country in which a ship is registered (the Aratere’s flag State was New Zealand). It is responsible for implementing and enforcing all instruments to which it is party on its ships. The flag State audits and issues certification to its ships.
- The Maritime Transport Act 1994 provides the Minister of Transport with powers to implement IMO instruments by incorporating the requirements contained in those instruments into maritime rules. In practice, this is facilitated by Maritime NZ.
SOLAS Convention
- The SOLAS Convention is incorporated into New Zealand domestic law through the promulgation of maritime rules.
-
The relevant maritime rules are:
Maritime Rule Part 23.13 Testing of steering gear (this incorporates SOLAS Chapter V, Regulation 26.4.5)
(2) The owner and the master of a ship to which this rule applies must ensure that simple operating instructions with a block diagram showing the change-over procedures for remote steering gear control systems and steering gear power units are permanently displayed on the navigating bridge and in the steering gear compartment.
(3) The master of a ship to which this rule applies must ensure that all ships' officers concerned with the operation or maintenance of steering gear are familiar with the operation of the steering systems fitted on the ship and with the procedures for changing from one system to another.
(4) The master of a ship to which this rule applies must ensure that in, addition to the routine checks and tests prescribed in rule 23.13(1), emergency steering drills take place at intervals of not more than 3 months to practise emergency steering procedures. These drills must include -
(a) direct control from within the steering gear compartment; and
(b) the communications procedure with the navigating bridge; and
(c) where applicable, the operation of alternative power supplies
Maritime Rule Part 23.13A Use of heading and/or track control systems (this incorporates SOLAS Chapter V, Regulation 24)
(1) The master of a passenger ship that is both a New Zealand ship and a SOLAS ship must ensure that, when heading and/or track control systems are in use, it is possible to establish manual control of the ship’s steering immediately in conditions of -
(a) high traffic density; or
(b) restricted visibility; or
(c) all other hazardous navigational situations.
(2) The master must ensure that a qualified helmsperson is available to the officer in charge of the navigational watch to take over steering control where the conditions listed in subrule (1)(a), (b), or (c) are present.
(3) The master must ensure that the change over from automatic to manual steering and from manual steering to automatic steering is made -
(a) by the officer in charge of the navigational watch; or
(b) under the supervision of the officer in charge of the navigational watch.
International Safety Management Code
- At the time of the accident, the International Safety Management Code (ISM Code) was a mandatory code included in SOLAS Chapter IX. The ISM Code required ships’ operators to implement an SMS to ensure safe practices. Pertinent sections of the ISM Code are reproduced below:
-
ISM Code Part A, section 7 Shipboard operations:
The Company should establish procedures, plans and instructions, including checklists as appropriate, for key shipboard operations concerning the safety of the personnel, ship and protection of the environment. The various tasks should be defined and assigned to qualified personnel.
-
ISM Code Part A, section 6 Resources and personnel:
6.5 The Company should establish and maintain procedures for identifying any training which may be required in support of the safety management system and ensure that such training is provided for all personnel concerned.
-
ISM Code Part A, section 12 Company verification review and evaluation:
12.1 The Company should carry out internal safety audits on board and ashore at intervals not exceeding twelve months to verify whether safety and pollution-prevention activities comply with the safety management system. In exceptional circumstances, this interval may be exceeded by not more than three months.
12.2 The Company should periodically verify whether all those undertaking delegated ISM-related tasks are acting in conformity with the Company’s responsibilities under the Code.
12.3 The Company should periodically evaluate the effectiveness of the safety management system in accordance with procedures established by the Company.
- In New Zealand, Maritime Rule Part 21 references the ISM Code and sets out how it is applied. New Zealand was the flag State and in 2021 Maritime NZ issued a Document of Compliance for Interislander’s SMS.
- Maritime NZ audited the Safety Management Certificate in 2023 and issued Aratere’s renewed Safety Management Certificate in 2024.
STCW Convention
- The STCW Code is an annex to the STCW Convention. The Code provides the detailed technical standards and guidance to ensure that seafarers are properly trained and qualified to a consistent standard around the world, to provide for safe shipping operations. The pertinent sections of the STCW Code are:
-
STCW Code, Section A-VIII/2.8.5:
.5 watchkeeping personnel shall understand functions and operation of installations/equipment, and be familiar with handling them
-
STCW Code, Tables A-II/1 and 2:
Knowledge of steering control systems, operational procedures and change-over from manual to automatic control and vice versa. Adjustment of controls for optimum performance.
- Both of these provisions from the STCW Code are incorporated by reference through Maritime Rules 32.98, 32.100, 32.102, 32.104 and 32.106.
Interislander’s safety management system
-
Interislander’s safe navigation policy required that the master refer to various documents, including (but not limited to):
2.85.1 International Chamber of Shipping’s Bridge procedures guide (Bridge Procedures Guide), which includes sections on BRM, company policies and duties of the OOW.
2.85.2 The Nautical Institute’s Bridge Team Management: A practical guide (Bridge Team Management), which includes sections on bridge team management, leadership, communication and decision-making, and teamwork. It emphasises the importance of collaboration among bridge team members, fostering a culture of mutual support and shared responsibility.
2.85.3 The principles of BRM, as described in Bridge Procedures Guide and Bridge Team Management, were included and prescribed within Interislander’s SMS.
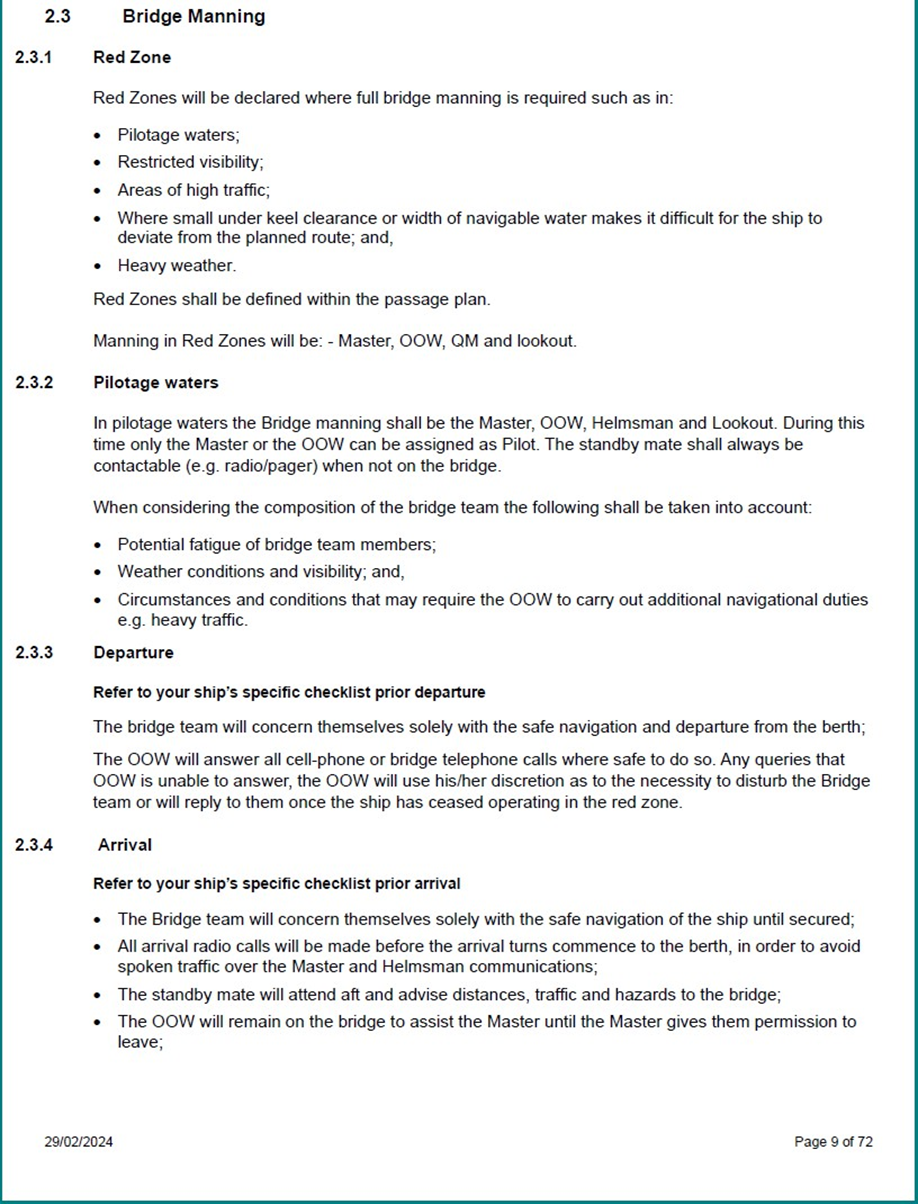
- Pertinent sections of the SMS relating to bridge procedures are given in Appendices 1 and 2.
Appendix 1. SMS procedures manual – bridge manning
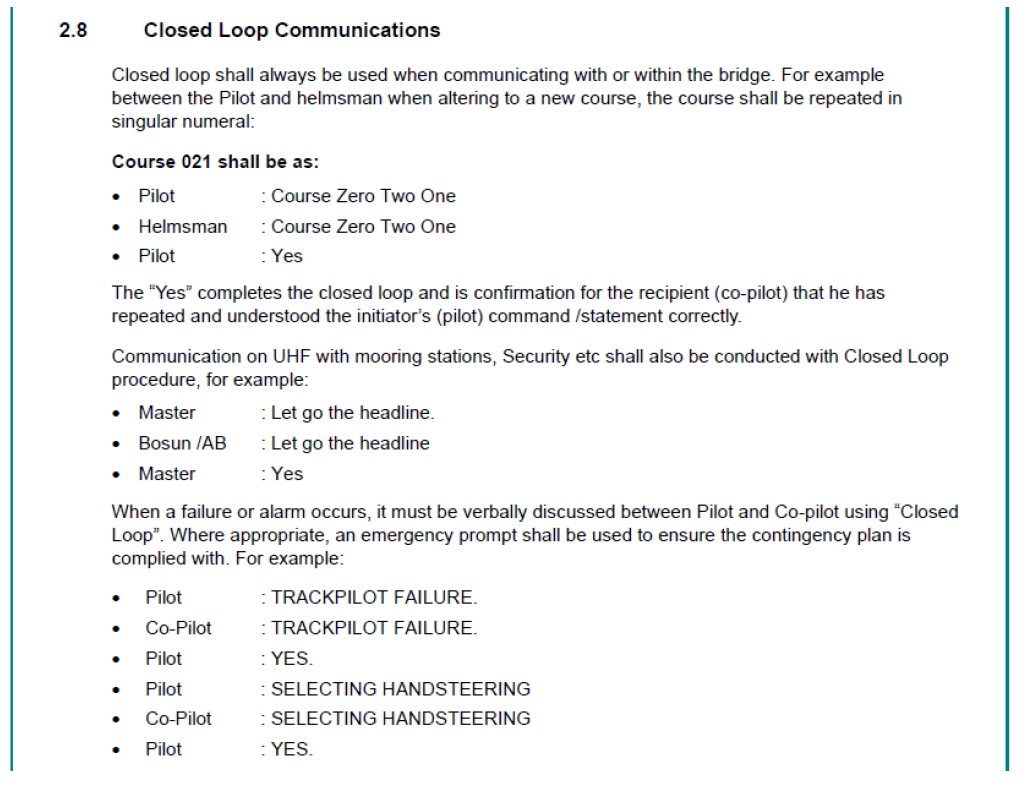
Appendix 2. SMS procedures manual – closed loop communications