A freight train hauling 36 wagons derailed soon after leaving Glenbrook for Mount Maunganui. Nobody was hurt, but there was extensive damage to the track, wagons and steel freight, and the line was closed for 3.5 days. The Commission found that brakes had failed because operating staff didn’t configure them correctly. Key learnings include the need for operating staff to follow established procedure and stay alert when working shifts.
Executive summary Tuhinga whakarāpopoto

- A KiwiRail freight train consisting of three locomotives hauling 36 wagons departed Glenbrook bound for Mount Maunganui at 0430 on 9 January 2013.
- When the train departed the brakes were working only on the three locomotives, and not the wagons (the train brake) due to the train braking system not being configured properly in the non-driving end of the lead locomotive. Also, the coupling between the sixth and seventh wagons in the train had not been secured properly.
- The train parted between the sixth and seventh wagons while descending a grade from Glenbrook. Within a matter of seconds, the rear portion of the train ran into the forward portion, causing the derailment.
- The track infrastructure and 28 wagons carrying steel product were extensively damaged. The line was closed for three and a half days while repairs were completed.
- The Transport Accident Investigation Commission (Commission) found that the train was able to depart with a wrongly configured brake control system due to there being no mechanical interlock preventing it moving.
- The Commission also found that the fact that the train brakes were not working when the train departed Glenbrook should have been detected, but was not, because the required brake test had not been performed after a third locomotive was added to the train.
- The Commission has made no recommendations because of the safety actions taken by KiwiRail Holdings Limited following the derailment and the trend of decreasing mainline derailments during the period of this investigation.
- Key lessons identified from this inquiry are:
- train drivers and train examiners need to comply with basic operating rules to ensure that trains have fully functioning and continuous air brake systems at all times
- it is important that all operating staff communicate properly and effectively and ensure that proper procedures are followed. Should there be any departure from the plan or any unusual or unexplained event occur, it must be communicated effectively
- shift workers need to remain alert to any situation that could affect their cognitive performance, and that of their work colleagues.
Factual information Pārongo pono
Locomotive and train coupling arrangements
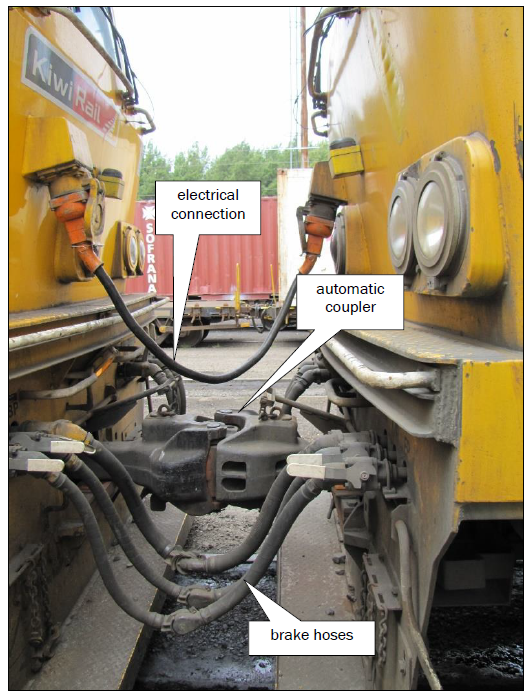
- There are three components used to join locomotives and wagons to form a train (see Figure 1). The components are:
- electrical connection – this arrangement allows for one train driver to operate multiple locomotives. Electrical connections are used between locomotives only
- coupler – this arrangement is the physical connection between locomotives and between locomotives and wagons. Couplers can be either automatic or standard mechanisms
- brake hoses – these allow compressed air to transfer from locomotives to the coupled freight wagons on a train. A train driver operates a valve in the locomotive cab to decrease air pressure to apply brakes on every coupled locomotive and wagon. Conversely the train driver operates the valve to increase air pressure to release the brakes on every coupled locomotive and wagon on a train.
The intermittent electrical connection
- Between 1630 and 1650 on 8 January 2013, KiwiRail’s locomotive servicing staff at Auckland coupled two diesel locomotives together and recorded details of the air brake and electrical connection tests that were carried out.
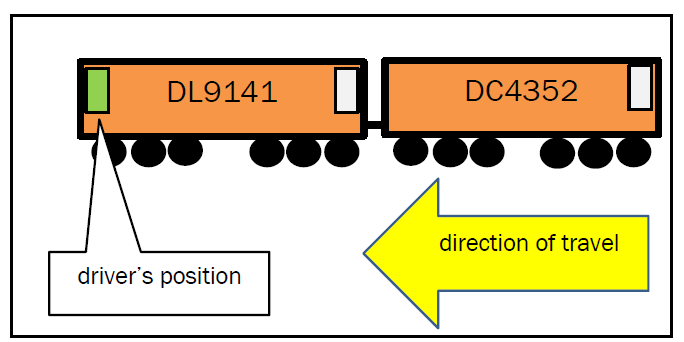
- At 1630 on the same day a KiwiRail train driver (driver A) started work to drive the two locomotives from Auckland to Mission Bush, a distance of 50.5 kilometres (km). The locomotives left Auckland at 1718 (see Figure 2).
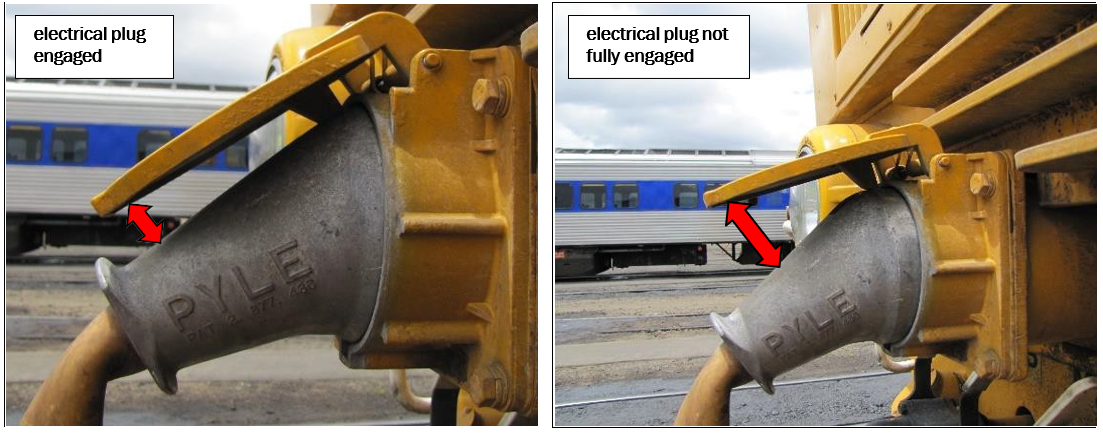
- At 1723 the Tranzlog (the brand name of the standard event recorder technology installed on KiwiRail’s locomotives) event recorders on the locomotives detected an intermittent loss of connectivity in the electrical connection. The electrical plug on the second locomotive was later found not fully engaged (see Figure 3). This resulted in the two locomotives not working together during the journey to Mission Bush. Driver A was not aware of the issue.
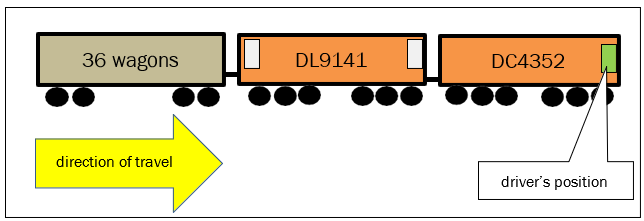
- The two locomotives arrived at Mission Bush at 1832 and were coupled to a rake of loaded wagons to form freight Train 345 (the train) destined for Mount Maunganui. The train weighed 1,845 tonnes, which was within the haulage capacity of the two locomotives. Driver A transferred control of the train to the new lead locomotive (see Figure 4).
- Air compressors on the locomotives charged the brake cylinders to full pressure on the wagons throughout the train after the brake hoses had been connected between the second locomotive and the first wagon.
- Driver A, with assistance from a ground-based KiwiRail train examiner, conducted a detailed test of the train’s brakes in compliance with KiwiRail’s rules after maximum air pressure had been reached. The procedure was called a terminal brake test and required the driver to release air pressure from the brake cylinders, thereby applying the wagon brakes, then recharge air pressure to the brake cylinders to release the brakes. The train examiner was also required to check that the couplers throughout the train were correctly secured.
- The driver completed two basic tests during this time, which showed that the locomotive’s brakes were working correctly and, despite the intermittent electrical plug connection, that both locomotives were working together.
- The train was moved in readiness for departure from Mission Bush. Shunting staff employed by the steel mill informed the train examiner that they considered the two locomotives were not working together during this movement. The train examiner had become busy with other tasks and forgot to pass on this information to driver A.
- Meanwhile, driver A had reached his own conclusion that his locomotive was not performing satisfactorily. Although he had walked past the area between the two locomotives on several occasions while at Mission Bush, he had not seen that the electrical plug was not fully engaged on DC4352. The two locomotives were disconnected from the train and reoriented using a triangular track layout provided for this purpose and that negated the need to break the couplers between the two locomotives (see Figure 5).
- The two locomotives were recoupled, and the brake hoses were reconnected to the train by the train examiner. The train driver and the train examiner conducted a shortened test on the train’s brakes in compliance with KiwiRail’s rules. The procedure, called an intermediate brake test, ensured that the train’s brakes remained functioning correctly. The test was successful.
- The train left Mission Bush at 2145 and took three and a half hours to travel the 5.7 km to Glenbrook, where driver A stopped the train. Driver A thought that the slow speed was due to a fault in the lead locomotive. Driver A had full braking control over both locomotives and the 36 wagons during this period.
- The separate data streams from the Tranzlog event recorders on the locomotives showed that the lead locomotive was hauling the train without any power coming from the second locomotive, as it would have done if the electrical plug connection had been fully engaged. The train weight exceeded the lead locomotive’s pulling capacity. Driver A had full control of the locomotives’ and wagons’ brakes during this time.
- At 0118 on 9 January 2013, driver A declared to train control that the train was disabled and needed additional locomotive power before the journey to Mount Maunganui could resume.
- Another train driver tasked, who later in the day would be tasked with driving the three non-derailed locomotives away from the derailment site, saw that the electrical connection was not fully engaged on the third locomotive. He said that he was able to fully engage and lock the electrical plug into its socket.
- Servicing staff later reported that a detailed examination of the control systems on DL9141 did not reveal any defects. The locomotive was returned to train operations without any repairs being necessary.
Setting the brake controls
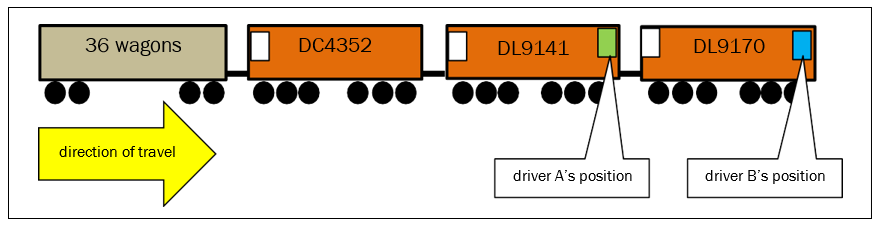
- Train control arranged for an assisting (third) locomotive from Auckland. It left Auckland with a Hamilton-based driver (driver B) at 0320 and travelled to Glenbrook, where it arrived at 0422.
-
The third locomotive was coupled and the brake hoses were connected. The train examiner had remained on duty and had driven by road from Mission Bush to Glenbrook to assist with the recovery of the disabled train.
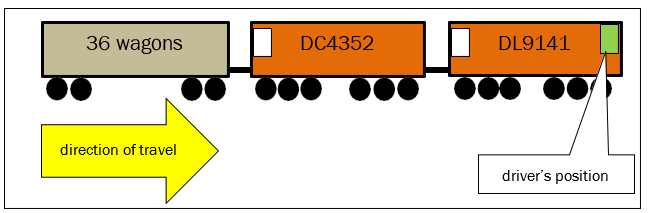
- The third locomotive now became the lead for the train (see Figure 6), but control had to be transferred to the driver’s cab at the other end of the locomotive. An electrical connection cable was plugged in between the two DL locomotives. These two locomotives now provided sufficient tractive power to enable the train to recommence its journey to Mount Maunganui.
- Driver B was now in charge of the train, and he transferred control to the other end of the lead locomotive. He did not neutralise the two brake handles before he left the cab, leaving the handles in the positions shown in Figure 7A. The train would not move when driver B applied power to the train.
- Driver B returned to the vacated cab and correctly neutralised the black handle for the locomotive brakes, but omitted to neutralise the red handle for the train brakes (see Figure 7B).
- In order to transfer control to the other driving cab correctly, Driver B should have placed both handles to the positions as shown in Figure 7C.

- The incorrect brake set-up meant that driver B had braking control on the three locomotives only, but no braking control on the 36 wagons. An intermediate brake test required to be conducted from the lead locomotive in compliance with KiwiRail’s rules was not carried out. The intermediate test would have identified that there was no braking control on the wagons.
- There was no loss of air pressure to the wagon’s brakes during this time, and the brake cylinders remained fully charged and kept the brakes in the release position.
- At 0435 driver B applied power and travelled a short distance on a slight rising gradient to a level crossing, where the train examiner dismounted from the lead locomotive to be near his parked motor vehicle. Driver B noticed that the train was not slowing as quickly as he expected because only the locomotive brakes were working. The train examiner dismounted while the train was still moving.
The derailment
- At 0437:02 driver B accelerated the train away from the level crossing. At 0440 the speed of the train reached 63 km/h on a descending gradient. The driver applied the train’s brakes to slow the train for an upcoming 40 km/h temporary speed restriction without success. Driver B made several applications of the locomotives’ brakes, but the speed of the train increased to 76 km/h over the speed-restricted section of track.
- At 0440:45 the Tranzlog recorded a sudden drop in air pressure in the train’s brakes. The wagons had surged forward on the descending gradient, causing the coupling hook to lift up and the brake hoses to separate between the sixth and seventh wagons (see Figure 8).
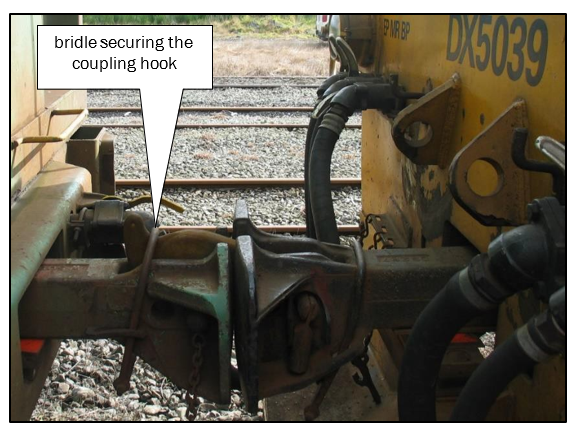
- The bridle and coupling hook were later found to be intact on the separated sixth and seventh wagons. It could not be established whether the bridle had been correctly secured between the two wagons before the train left Mission Bush or whether it had lifted off while the train was travelling between Mission Bush and the location of the derailment. It was normal practice for the train examiner to check that all bridles were in place before a train departed.
- The two detached sections of the train travelled independently for a short distance.
- At 0440:48 the rear section caught up and collided with the front section of the train. The Tranzlogs showed that the locomotives were travelling at 65 km/h and calculations showed that the rear section was travelling at 76 km/h at that instant. The collision, known as a ‘run-in’, caused three wagons to derail simultaneously in the vicinity of the 9.35 km mark, resulting in track damage that caused a further 28 wagons to derail.
Rail personnel
Driver A
- Driver A was based in Auckland and his licence to drive trains was current. He had been driving trains for 28 years. He was familiar with the Mission Bush Branch line and the DL class of locomotive.
- Driver A had resumed work on 8 January 2013 after the Christmas and New Year holiday period.
- Driver A had been assessed and passed competency for KiwiRail’s non-technical skills practices, alertness management and intermediate brake test procedures in 2012.
- KiwiRail did not conduct a post-accident drug and alcohol test on driver A in accordance with its own policy, which stipulated that it would test any member of staff directly involved in an incident.
Driver B
- Driver B was based in Hamilton and his licence to drive trains was current. He had been driving trains for 39 years. He was familiar with the Mission Bush Branch line and the DL class of locomotive.
- Driver B’s work hours during the preceding three weeks had been normal. He had been rostered off duty for five days between 4 and 8 January 2013, but he had been called out to drive overnight trains on two occasions. Driver B said that he had suffered from restless sleep in the two nights immediately leading up to the night of the derailment because of the prevailing hot and humid weather conditions.
- Driver B had been assessed and passed competency for KiwiRail’s non-technical skills practices and alertness management during 2002. His most recent intermediate brake test procedure assessment for competency had taken place during 1999.
- Driver B underwent a post-accident drug and alcohol test, which detected no performance-impairing substances.
Train examiner
- The train examiner was based in Mission Bush and his licence to operate was current. He was familiar with train operating practices at Mission Bush and KiwiRail’s brake examination rules. The train examiner’s work hours were normal.
- The train examiner had been assessed and passed competency for KiwiRail’s intermediate brake test procedures in 2012, but he had not been trained in or assessed for KiwiRail’s non-technical skills practices and alertness management practices.
- KiwiRail did not conduct a post-accident drug and alcohol test on the train examiner in accordance with its own policy, which stipulated that it would test any member of staff directly involved in an incident.
Analysis
Introduction
- Mainline derailments have the potential to cause serious harm to people, and damage to locomotives, wagons, rail infrastructure and the freight being conveyed. They therefore have significant implications for transport safety. This derailment occurred close to occupied farm dwellings, and the extended recovery period disrupted production at the steel mill the Mission Bush Branch line served.
- The actual derailment occurred after the train had separated when, seconds later, the rear portion of 30 wagons ran into the front six wagons and three locomotives. Evidence showed that the front portion of the train had slowed more quickly than the heavier rear portion of the train, very likely because of the heavy weight of the 30 wagons and the three locomotives being already under braking.
- The impact of the collision forced three wagons to derail simultaneously. Driver A had not been able to apply the train’s brakes, but the retained air pressure in the wagons’ brake cylinders resulted in the wagon brakes automatically applying on both portions of the train when the hoses separated between the sixth and seventh wagons.
- The separation between the sixth and seventh wagons and was very likely caused by an incomplete coupling connection that had gone undetected during the terminal brake test undertaken at Mission Bush before the train departed. The incomplete coupling allowed the hook to spring up when the couplings suddenly compressed as the train descended the gradient from Glenbrook.
- The investigation did not uncover any mechanical faults with the wagons, any freight loading issues, or any track geometry issues that could have contributed to the derailment. None of the three locomotives had any mechanical faults that made it unserviceable, except for the underlying brake handle issue on the DL locomotives. Subsequent tests carried out on the same three locomotives showed that the brakes on the wagons would not have functioned with the identical brake control configuration as set when the train left Glenbrook.
- The following analysis discusses the factors leading to the derailment, and safety issues relating to non-compliance with train operating practices.
The train drivers’ and train examiner’s actions
- Both train drivers and the train examiner were qualified for their roles. With the exception of driver B, they had recently demonstrated compliance with the intermediate brake test procedures.
- Driver B’s most recent assessment for intermediate brake tests had been undertaken in July 1999. He was therefore 12 years overdue for his intermediate brake test assessment. This, together with two other instances where driver A and the train examiner were overdue for their biannual theory assessments, has since been addressed by KiwiRail.
- KiwiRail implemented an improved assessment management system for its staff members during July 2014. The system now provides all levels of KiwiRail management with a transparent overview of dates by which any outstanding assessments must be completed.
- During the investigation the Commission identified the following procedural lapses by the locomotive servicing staff, the train drivers and the train examiner:
- the electrical connection was not fitted correctly by the servicing staff prior to the two locomotives leaving Auckland and was not subsequently identified or checked by driver A
- the incomplete coupling between the sixth and seventh wagons was not detected during the terminal brake test prior to the train leaving Mission Bush
- the brake handles in the rear cab of the lead locomotive were left in an incorrect configuration.
- The Commission reviewed KiwiRail’s procedures and instructions for these tasks and identified a number of improvements, which KiwiRail subsequently made.
The incomplete electrical plug connection
Safety issue – The incomplete electrical plug connection went undetected by several rail staff. Independently, both locomotives were performing correctly, but the incomplete electrical connection meant they were not operating together.
- The incomplete electrical connection resulted in the two locomotives only intermittently operating together. It was this poor locomotive performance that ultimately led to the train being unnecessarily declared as disabled at Glenbrook. This was the first in a chain of events that led to the derailment.
- Had driver A checked the electrical connection before leaving Mission Bush, it could have been rectified by simply pushing home the plug on the second locomotive until the lug on the top flap locked into the depression at the top of the plug (refer Figure 3).
- There is no automatic alert to inform a train driver when an electrical connection is not fully engaged. Train drivers use their experience to monitor the performance of multiple locomotives hauling trains.
- The ammeters (an ammeter is a dial fitted on a locomotive’s dashboard to display the amount of current being produced by the electrical generator) in the driving cab would have shown driver A that driving amps were being generated for the traction motors within the normal operating range for both locomotives. This would have been an indication to the train driver that both were fully functional and that there was potentially a problem with the electrical connection between the two locomotives.
- The servicing staff and the train driver were qualified for their roles and all had experience in fitting and checking electrical connections between locomotives. KiwiRail reviewed its locomotive servicing procedures and used this derailment to highlight the need for train drivers to include visual examinations of electrical connections when dealing with any similar locomotive performance issues. Consequently, the Commission has not made any recommendations to KiwiRail to address this issue.
Incorrect brake handle set-up
Safety issue – Driver B was able to set the brake handles incorrectly because there was no interlock (a mechanical or electrical feature that ensures that the operation of two linked mechanisms, brake handles in this instance, cannot be independently operated at the same time) capability between the two driving cabs of the DL-class locomotives. The incorrect brake set-up resulted in driver B not having brake control over the coupled wagons.
- The DL-class locomotive was the first double-cab diesel locomotive to operate in New Zealand that had brake handles permanently fitted to both cabs. It required train drivers to set the locomotive and train brake handles correctly before vacating a cab and relocating to the cab at the other end.
- In comparison, the earlier-generation double-cab diesel and electric locomotives, and the current fleet of double-cab EF-class electric locomotives, required some or all of the brake handles to be physically transferred by the drivers when changing ends. This meant that train drivers had to isolate the brakes in a cab being vacated in order to remove the appropriate handles. The handles were then carried to the other cab, where they were inserted to allow the brakes to be controlled from that end of the locomotive. This manual process provided a reliable interlock, preventing an incorrect brake handle set-up as seen in this instance.
- KiwiRail investigated several options before choosing the Tranzlog event recorder system to provide an interlock capability to prevent a similar incident. The Tranzlog system was chosen to perform this interlock because the positions of the brake handles were already being monitored by the system. This option was successfully tested during 2014/2015 and rolled out on all the DL-class locomotives. In view of this work, the Commission has not made a recommendation to KiwiRail to address this issue.
- Additionally, KiwiRail has committed to providing a similar Tranzlog-based interlock capability on all its other mainline diesel locomotives. This work will supplement the existing manual interlock and was underway at the time of the compilation of this report.
Non-technical skills
Safety issue – When the three staff members came together to couple the third locomotive to the disabled train at Glenbrook, no challenge and confirm actions were taken to complete a fundamental brake test procedure, which was designed to ensure that the trains’ air brakes were functioning correctly.
- Non-technical skills (previously known as crew resource management) are a set of practices designed to create a safe working environment, encourage teamwork, improve situational awareness and understand technical proficiency.
- Staff using non-technical skills will communicate more effectively, be more aware of their situation, use all of its available resources and work better with one another. Communication skills and practices form a significant component of what has become known as non-technical skills in other transport modes.
- The issue of non-technical skills was raised in seven rail occurrence reports published by the Commission between 2003 and 2008. Recommendations were made to KiwiRail to establish non-technical skills as a core operating practice to help reduce accidents and incidents within the rail industry.
- The Commission had issued its most recent recommendation on non-technical skills to the NZ Transport Agency during 2012. The recommendation required that the practice of non-technical skills be recognised in the National Rail System Standards. The recommendation remained open at the time of compiling this report.
- In this instance, the non-technical skill lapses were that:
- the comments by mill shunting staff regarding the two locomotives not working together were not communicated
- the required intermediate brake test was not carried out when the third locomotive was attached to the train at Glenbrook.
- The train examiner forgot to pass on the information to the train driver after the mill shunting staff had identified that the locomotives did not seem to be working together. The mill shunting staff were alert to the problem, and had the train examiner informed driver A of what he had been told, the driver may have been prompted to examine the electrical connection and could have found that it was not properly connected.
- If driver A had corrected the electrical connection, the train would have had sufficient locomotive power without the addition of the third locomotive.
- KiwiRail’s air brake rules stated that an intermediate brake test was required when a locomotive was added to a train. The straightforward test involved the train examiner positioning himself alongside any wagon on the train to observe the movement of the piston in the brake cylinder when driver B applied and released the train’s brakes from the lead locomotive.
- In this case the train examiner would have observed that the wagon’s brakes were not working. This would have prompted driver B to re-examine his brake handle set-up. The train would not then have departed with a non-operational train brake. Although driver B was responsible for ensuring compliance with this task, either driver A or the train examiner should have advised driver B that the intermediate test was required.
- As a result, there was no braking control on the loaded wagons that weighed a total of 1,845 tonnes. Driver B was unable to reduce the speed of the train and comply with the 40 km/h restriction shortly after leaving the level crossing at Glenbrook.
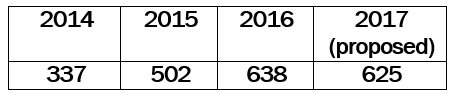
- On 26 October 2016 KiwiRail provided the Commission with an updated implementation plan to develop non-technical skills within its workforce. The plan stated that non-technical skills must be embedded and promoted in the workforce in order to build a strong safety culture. The plan showed that between 2014 and 2016 the following number of KiwiRail staff had participated in training programmes that included the principles of non-technical-skills:
- On 14 December 2016 KiwiRail provided the Commission with a further update on its planned implementation of its non-technical skills policy in the management of its core business operations and practices. KiwiRail said that current thinking internationally on the management of non-technical skills within rail and other modal transport industries has shifted. The new policy requires non-technical skills principles to be embedded in all technical and non-technical training, safety assessments/observations/audits and assurance activities within an organisation’s safety management and crew management systems.
- KiwiRail has referred to extensive material produced by the Rail Safety and Standards Board Limited and Network Rail in the United Kingdom. KiwiRail said that this approach was a big step forward because it had to have organisational alignment across all of its business groups and not be restricted to above rail, as was the case when non-technical skills practices were first delivered during the mid-1990s.
- KiwiRail said that other work done in the risk management of SPADs (signals passed at danger) had seen the development and implementation of a stabilised approach, risk-triggered commentary driving and engineering supervisory controls within its safety management systems. These actions were designed to support train driver cognition, trap human error before an accident and enable recovery to a safe condition.
- These plans show that KiwiRail is continuing to address non-technical skills awareness and therefore the Commission will not be making a further recommendation on this matter. Meanwhile, the Commission’s recommendation 002/12 made to the NZ Transport Agency in 2012 remains open.
- On 3 April 2017 the NZ Transport Agency said that it was continuing to work with KiwiRail on this issue. The agency added that it had issued a safety improvement plan notice during December 2016 in accordance with section 36 of the Railways Act 2005, requiring KiwiRail to prepare a safety improvement plan to address the implementation of non-technical skills in its rail operations.
The train drivers’ and train examiner’s performance
Safety issue – There were several procedural lapses by three experienced rail staff members between the coupling of the two locomotives at Auckland and the train examiner’s dismounting from the train 12 hours later.
- The Commission has considered whether fatigue was a contributory factor in respect of both drivers and the train examiner not carrying out the intermediate brake test.
- Driver A was working his second day after a period of leave and the train examiner had been off duty for the preceding weekend. They had started work the previous evening at 1630 and 1745 respectively and said they had been feeling tired when it came to coupling the third locomotive to the train at Glenbrook.
- However, based on driver A’s and the train examiner’s hours of work and their comments, it was very unlikely that either of these two members was suffering from fatigue.
- On the other hand, driver B reported suffering restless sleep during the three days leading up to the derailment. Although he reported feeling well when he started work at midnight on 8 January 2013, he overlooked the setting of the brake handles only four and a half hours later.
- Driver B said that he had not rested well and his sleep had been light and restless. It was highly likely that he was suffering from a level of sleepiness and was tired before starting the night shift. It was unlikely that he had reached a level of fatigue based on his hours of work leading up to the derailment and from his comments.
- The procedural lapses occurred during the period when circadian rhythm is at its lowest (the time in the natural body clock when performance is at its lowest and the drive for sleep is at its highest). Not checking the correct setting of the brake handles and not calling for an intermediate brake test occurred at precisely 0430, the time when cognitive performance is typically at its lowest.
- Research by sleep/wake experts (La Sapienza university and the Aeroporto Pratica di Mare of Rome) has shown that the period between 0300 and 0500, and specifically 0430, is when a person’s body reaches its lowest temperature, which in turn leads to reduced cognitive performance. Recognising that two procedural lapses occurred during this critical period, it may help to explain some of the shortcomings, particularly the need for driver B to call for an intermediate brake test.
- The Commission published six rail occurrence reports into freight train derailments and collisions during a two-year period between September 2000 and July 2002. Two of the themes identified in the reports were:
- train driver roster management
- recognising the difficulties of train drivers attaining good-quality sleep during summer months.
- The Commission published, and repeated, four recommendations in those six reports to Tranz Rail (the penultimate predecessor to KiwiRail) to address these issues. The four recommendations were subsequently closed out after the Sleep/Wake Research Centre in Wellington developed a best-practice policy for rostering train drivers.
- On 1 December 2013 KiwiRail and the Rail and Maritime Transport Union issued a document titled ‘Summer SPAD Awareness’. The document identified that the summer months (December–February) were among the worst for SPADs and other safety-related incidents.
- The purpose of the document was to raise awareness of the increased risks brought on during the summer months and offer advice to staff members on how to reduce the likelihood of incidents. One topic addressed was fatigue and shift work. The document identified that fatigue was exaggerated by the longer daylight hours and hotter temperatures reducing the ability for shift workers to obtain adequate rest, and the ability to get good sleep during the day.
- Between October and December 2016, KiwiRail engaged with its train operating staff and provided an update to its summertime fatigue management programme, addressing the increased risk of incidents occurring during this period. The programme covered matters such as entering shifts prepared, situational awareness and the ‘stop, think, act, review’ process. Based on the evidence supplied, the Commission has not made any further recommendations.
Safety issues and remedial action Ngā take haumanu me ngā mahi whakatika
General
-
The Commission classifies safety actions by two types:
(a) safety actions taken by the regulator or an operator to address safety issues identified by the Commission during an inquiry that would otherwise result in the Commission issuing a recommendation
(b) safety actions taken by the regulator or an operator to address other safety issues that would not normally result in the Commission issuing a recommendation.
Safety actions addressing safety issues identified during an inquiry
- On 18 January 2013 KiwiRail issued a Safety Briefing titled ‘Incorrect Brake Set-Up’. The briefing explained the consequences if either the independent or the train brake handles were incorrectly set up on a freight train with any DL-class locomotive in the lead position.
- On 5 May 2015 KiwiRail issued a Safety Briefing titled ‘Radio Test, Servicing and Brake Set-Up Card (Loco 387)’. The briefing detailed an update made to the Loco 387 form that required servicing staff to sign off as a check that the brake handles had been correctly set when locomotives were coupled together for multiple operation on a train.
- On 15 June 2015 KiwiRail issued a special bulletin titled ‘Incorrect Brake Set-Up Protection Trial – DL9129’. The bulletin explained that the Tranzlog system had been updated to provide incorrect-brake-set-up protection. The trial period was scheduled for a six-week period.
- On 9 May 2016 KiwiRail issued a subsequent special bulletin titled ‘DL locomotives – Tranzlog Upgrade’. The bulletin explained that following the successful trials on DL9129, the Tranzlog system upgrade would be rolled out to the remaining 39 DL-class locomotives.
- On 12 August 2016 KiwiRail advised that all operational DL-class locomotives had had the Tranzlog upgrades completed. A small number of non-operational locomotives that were currently having asbestos removed at its workshop facility in the Hutt Valley near Wellington would have the Tranzlogs upgraded when the repairs were completed.
- On 12 August 2016 KiwiRail advised that the couplers in 34% of the fleet of freight wagons used to transport export steel had been converted from standard to automatic couplers to mitigate against coupler partings on moving trains (see Figure 9).

- On 5 October 2016 KiwiRail advised that it was reviewing the Tranzlog upgrade designed to detect an incorrect brake set-up on the DL-class locomotives with a view to installing the upgrade in its remaining single-cab diesel locomotive fleet.
Safety actions addressing other safety issues
- On 3 April 2017 the NZ Transport Agency said that KiwiRail had improved its competency management system since the date of the incident. The system had been the subject of post-safety assessment remedial actions arising from the 2015 NZ Transport Agency assessment. The NZ Transport Agency continues to monitor KiwiRail’s usage of the system through the agency’s safety assessment system.