TAIC calling for improvements in ship safety management systems (Singapore) and mooring winch installation. On container ship Rio De La Plata, a rope handler suffered serious injuries to hand and face when they were trapped between incoming rope and winch. Issues with the ship’s safety system; equipment installation not optimised for safety; and loss of situational awareness. www.taic.org.nz/mo-2020-204
Executive summary Tuhinga whakarāpopoto

What happened
- On the morning of 14 November 2020, the container ship Rio De La Plata was preparing for departure from the Port of Timaru after completing cargo operations. Three crew members had just commenced unmooring operations at the forward mooring deck when one of them got caught in a rope that was being retrieved. The rope dragged the crew member into the mooring winch, resulting in serious injuries to their hand and face.
Why it happened
- It is likely that the crew member, completely engaged in communicating with the winch operator and handling the rope, had reduced situational awareness of their own safety. As a result, they stepped too close to the mooring winch and became trapped between the rope and the winch drum (see figure 8).
- The person in charge of the forward mooring party was also operating the winch. This very likely increased the risk of an accident because they no longer had a clear view of the entire operation and their ability to monitor the actions of others was reduced.
- The crew had not identified the need to change the unmooring plan to address new risks created by a reduction in crewing available on the forward mooring deck.
- The forward mooring party had not sufficiently planned the unmooring operations to mitigate the risk of crew members operating in blind spots, which increased the risk to crew working in close proximity to the mooring winch and in the blind spot of the winch operator.
- The safe job analysis undertaken by the crew deviated several times from the intent of the safety management system because there were several control measures that were lacking or did not sufficiently mitigate the risks identified.
- The transverse bars running across the mooring winch should have been removed after the winch was installed on the forward deck because it reduced the clearance available between the storage drum and deck and increased the risk of the rope getting stuck at the bar.
What we can learn
- Unmooring operations are just as dangerous as mooring operations and crew must ensure that there are always sufficient personnel available to carry out the operation safely.
- Equipment on board ships must be installed and operated as intended by the manufacturer. Any deviation from the manufacturer’s recommendation can increase the risk of serious injury.
- It is important that the person in a supervisory role remains an observer and does not take part in the actual work or handling operation.
- Risk assessments are only effective if realistic control measures are put in place to mitigate the hazards that have been identified. The control measures then need to be implemented correctly to reduce the risk to as low as possible.
Who may benefit
- The ship’s crew and the crews from other vessels in the fleet, the vessel owners and operators, maritime training facilities and shore-based emergency response agencies may all benefit from the findings in this report.
- The ship’s crew and the crews from other vessels and vessel owners and operators operating similar winches on their vessels.
- Winch manufacturers, ship builders and vessel inspectors.
Factual information Pārongo pono
Narrative
- On 4 November 2020, the Rio De La Plata completed its voyage from Sydney, Australia to Tauranga, New Zealand.
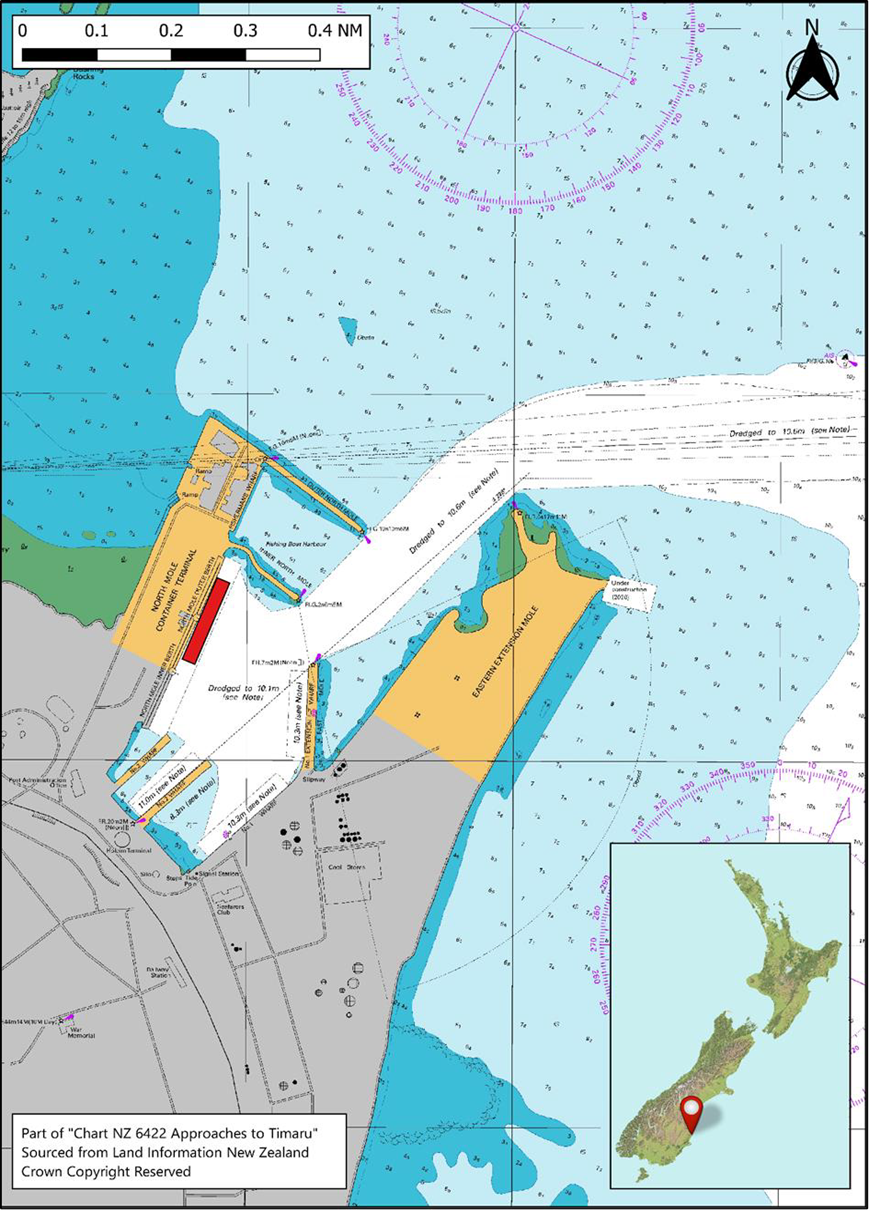
- From Tauranga the vessel visited Napier and Lyttelton before arriving in Timaru on the evening of 11 November 2020.
- At 0025 on 12 November 2020, the vessel was made fast (secured to the port facility) at the Northern Mole berth (a place for a ship to be secured in a port facility) in Timaru. The ship’s mooring configuration for its stay in Timaru consisted of four headlines (mooring lines leading ashore from the fore end of a ship in a forward direction) and three stern lines (mooring lines leading ashore from the aft end of a ship), two forward spring (mooring lines leading in a nearly fore and aft direction to prevent longitudinal movement of the ship while in berth) lines and two aft spring lines.
- At 0118 on 12 November 2020, the vessel commenced cargo operations of loading and unloading containers. The port used two mobile cranes to work the cargo until 0930 on 13 November 2020 when one crane broke down and was removed from service. Cargo operations continued using the remaining crane.
- At 0900 on 14 November 2020, the vessel completed cargo operations and recorded its last lift. At this time the engine room was given notice to prepare the engines for a scheduled departure at 1030 hours.
- At 1010 on 14 November 2020, standby (crew called to be ready for duty) stations was called by the master and the crew started preparing the vessel for departure.
- At about 1013, the pilot boarded the vessel. At 1025, the accommodation ladder was secured and the crew dispersed to their respective mooring stations.
- For this departure, the bridge team consisted of the master, chief officer, an able-bodied seaman and the pilot. At the aft mooring deck, the team consisted of the third officer and two able-bodied seaman. At the forward mooring deck, the team consisted of an able-bodied seaman (AB) and two ordinary seamen, OS1 and OS2 (the latter the injured person). The third officer was in charge of the aft mooring team and the AB was in charge of the forward mooring team.
- When the vessel carried a deck cadet, they assisted the forward mooring team, increasing the available crewing from three members to four. This was the case until about four weeks before the accident when the deck cadet signed off (paid off or departed from the vessel, usually to go home) from the vessel.
- At about 1028, the tugs were reported as secured on the starboard bow and at the stern. The master then gave the order to start unmooring.
Events at the forward mooring deck
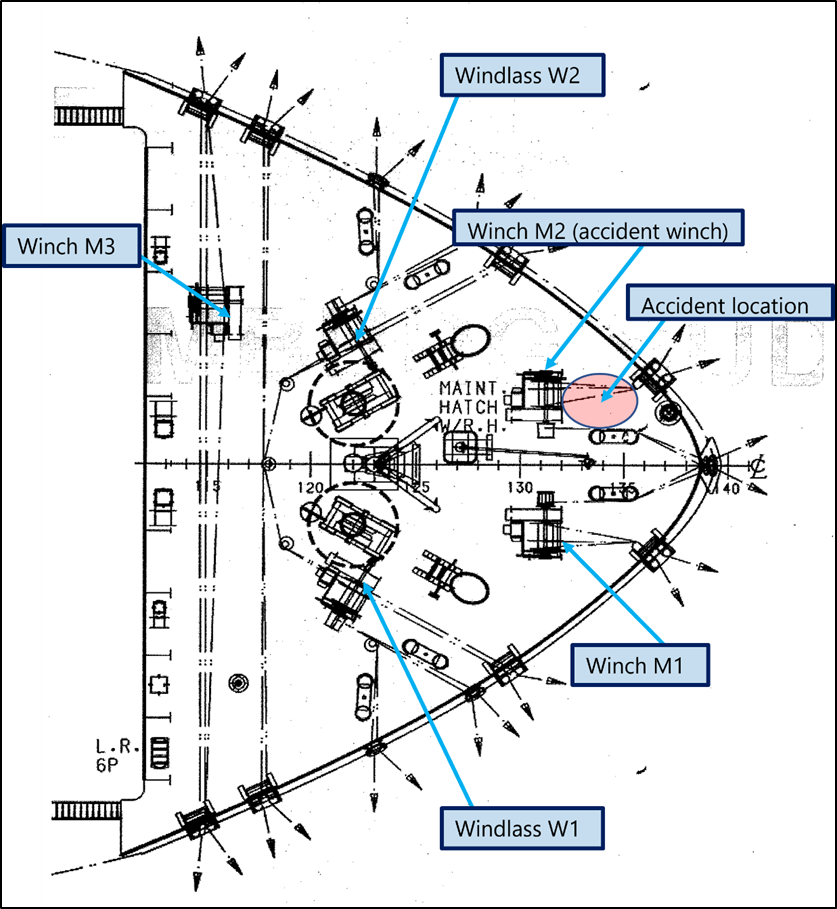
- The forward mooring deck (where the accident occurred) was equipped with three mooring winches and two windlasses. Figure 3 shows a drawing of the forward mooring deck layout.
- The deck equipment was operated from remote control stations located on either side of the forward mooring deck. The remote control stations were located away from the mooring winch, towards the aft end of the deck (see figure 4).
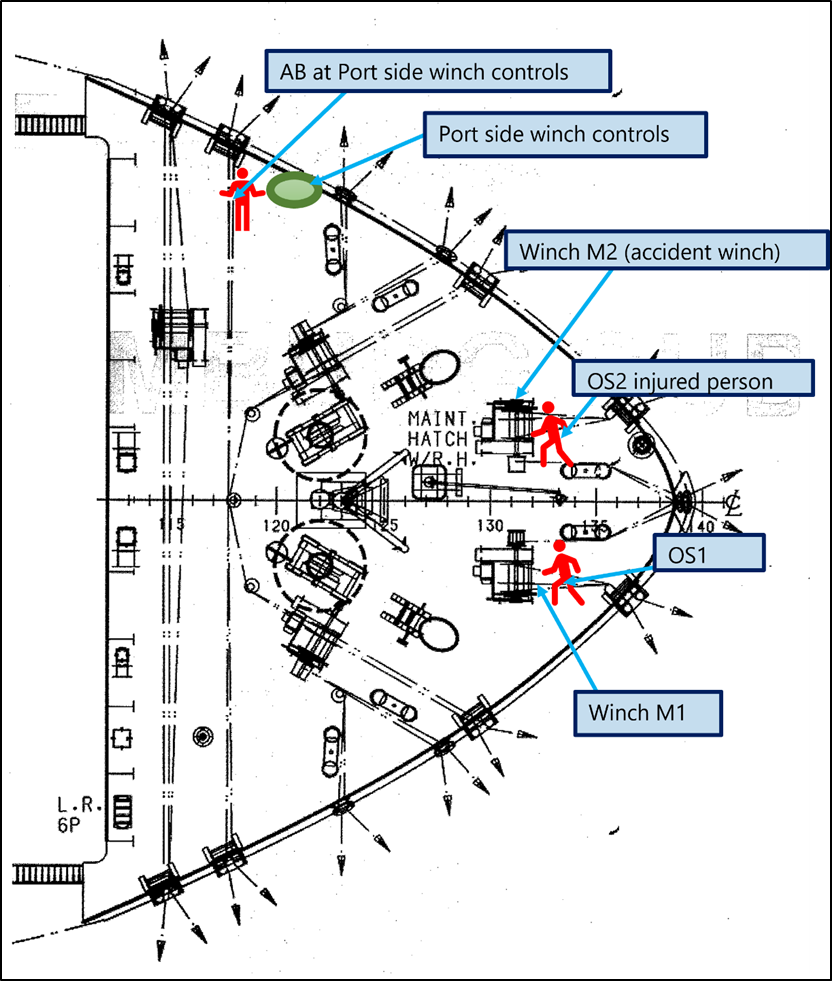
- The AB seaman positioned himself at the port side remote control station and took control of the mooring winches, while OS1 and OS2 (injured person) took up their positions near winch M1 and winch M2, respectively. From this position the AB did not have a direct line of sight of the two OS’s when they worked close to the winches.

- At about 1029, three of the four headlines were lowered to the water by the AB and two were cast off by the harbour linesmen.
- OS1 signalled to the AB to start operating the winches and retrieve the two ropes that were cast off. The winch M1 and the winch M2 were operated to pick up both the ropes simultaneously.
- OS1 and OS2 watched the ropes coming in and manually guided them, making sure they were correctly stowed on their respective drums. The AB stopped the winch when both the ropes were clear of the water line and then instructed OS1 and OS2 to start retrieving the other two ropes.
- Just before commencing the retrieval of the next two ropes, OS2 attempted to adjust the mooring rope on the winch drum and hand signalled to the AB to operate winch M2 at a slow speed. This was so the mooring ropes could be adjusted as they were wound onto the drum, to ensure correct storage.
- At about 1031, OS2 at winch M2 signalled ‘STOP’ by raising his hand and fell to the deck. OS1 at winch M1 who was facing the other way heard a scream and turned around to see OS2 lying on the deck with injuries to their face. The AB at the winch controls stopped the operation immediately and went to investigate.
Events after the accident
- At about 1035, immediately after seeing the injured crew member lying on the deck, the AB reported to the master that there had been an accident at the forward mooring deck.
- Shortly afterwards the pilot, who was on the bridge, called for the port ambulance. The master asked the second officer, who was off-duty, to report to the bridge and sent the chief officer forward to take charge of the medical response.
- The chief officer arrived at the forward stations with a first aid team and stretcher.
- At about 1050, OS2 was stretchered to the accommodation ladder where they were met by a shore-based medical team. The medical team assessed the casualty and called for more experienced paramedics.
- The medical team asked the ship’s staff to shift OS2 to the quay. The ship’s crew assessed that it was difficult and dangerous to carry a stretcher down the accommodation ladder. At about 1120, OS2 was transferred to another stretcher and lowered to the quay with the help of the ship’s monorail crane. By this time a second ambulance with paramedics had arrived by the shipside. OS2 was placed in the ambulance and transferred to Timaru Public Hospital.
- At about 1140, the vessel departed from the harbour and proceeded to a safe anchorage outside Timaru Port Limits awaiting instructions from the Timaru Port and the agents.
- Later that evening OS2 was shifted to Christchurch Hospital.
Personnel information
- The master joined the Rio De La Plata at Singapore on 25 August 2020. The master had started as a cadet in 1990 and had over 30 years of maritime experience. After graduating in 1999, the master’s first command was gained in 2004. The master has worked with Maersk since 2000.
- The chief officer joined the Rio De La Plata at Singapore on 26 August 2020. The chief officer had joined Maersk in January 2011 and had worked as a chief officer from January 2013.
- The AB operating the winch controls had joined the vessel on 13 October 2020 at Singapore. The AB was experienced, having worked as an AB and bosun for 10 years.
- The ordinary seaman (OS1) tending the rope at winch M1 had joined the vessel on 25 August 2020 at Singapore and had been in the rank for four years.
- The ordinary seaman (OS2) tending the ropes at winch M2 had joined the vessel on 25 August 2020 at Singapore, but this was his first time working as an OS. OS2 had previously worked as a deck cadet for 12 months with another company.
Vessel information
- The Rio De La Plata was a container ship registered in Singapore and operated by Maersk A/S. The vessel was built in South Korea in 2008 and was one of three vessels of the Rio class built by Daewoo Shipbuilding and Marine Engineering.
- The Rio De La Plata had an overall length of 286.45 metres, a breadth of 40.06 metres and a maximum draught of 13.5 metres. It was powered by a Sulzer 8RTA96C direct reversing diesel engine driving a single fixed-pitch propeller. The vessel had one 2720HP bow thruster and a 2040HP stern thruster.
- At the time of the accident, the vessel carried a multinational crew of 20, of which three deck officers and six deck crew were available for unmooring operations.
Forward mooring station and mooring winch
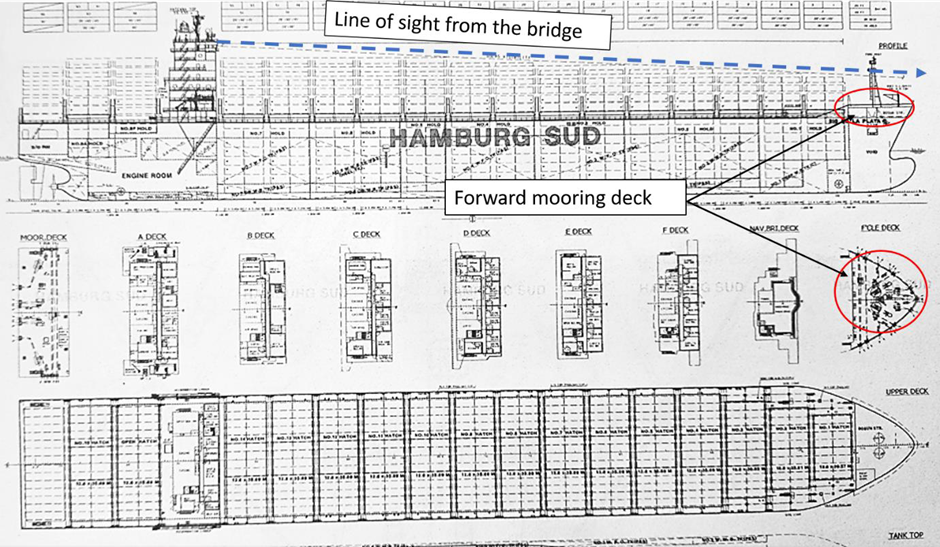
- The bridge, by virtue of the vessel’s design, had no view of the forward mooring deck as shown in figure 6.
- The forward mooring deck was located one deck above the vessel’s main deck. Figure 5 shows a view of the mooring deck from the port side winch controls and figure 7 shows the port side control station.

- At the time of the accident, the AB operating the winch was positioned at the port control station. From this position, there was no direct line of sight between the AB and the two OS’s working and handling the ropes forward of winch M1 and winch M2 (see figure 4 and figure 5). The forward mooring team therefore relied on verbal and/or hand signals to communicate. This issue is further discussed in the analysis section of the report.
Mooring winch
- The split drum mooring winches fitted on the forward mooring deck of the Rio De La Plata were manufactured by Hatlapa Uetersener Maschnenfarik Ltd. The company has since been taken over by MacGregor Germany GmbH & Co. KG.
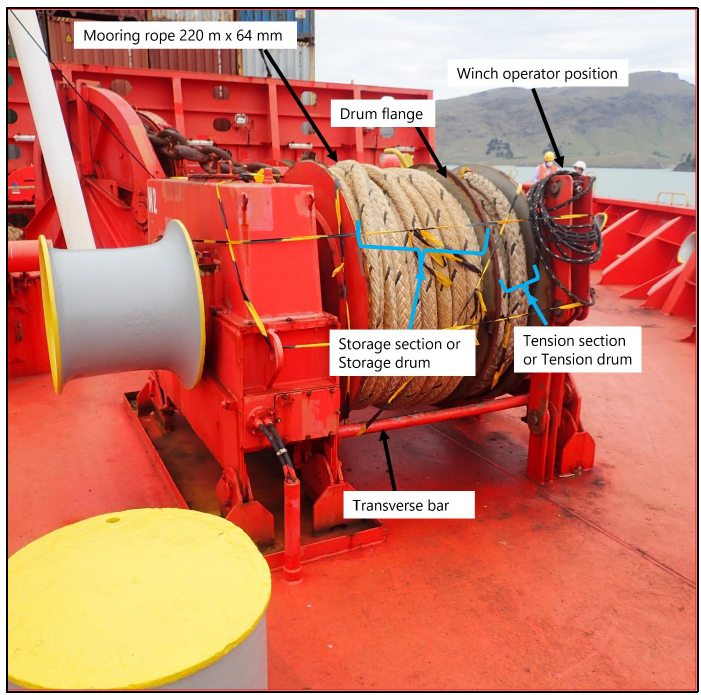
- The mooring winch design included two transverse bars running across the winch, one in the front and the other at the back. At the time of the accident OS2 was adjusting the rope on the storage drum to prevent it getting jammed between the drum and the transverse bar. Figure 8 shows a photo of the M2 mooring winch identifying the various sections of the drum and the location of the transverse bars.
Mooring rope
- The mooring winches were designed to accommodate a synthetic rope of 200 metres length and 64 millimetres in diameter, with a minimum breaking load (MBL) of 797.7 kN (approximately 80 tonnes).
- The mooring rope on board the vessel was manufactured from a mix of 50% polyester and 50% polysteel. Each rope was 64 millimetres in diameter and had an MBL of 108 tonnes. The mooring ropes on board the Rio De La Plata had been supplied in a 220 metre length, 20 metres longer than the maximum length of rope designed to be accommodated on the winch drum.
- The ropes were last inspected on 29 September 2020 and found to be in good condition.
Safety management system
- The safety management system is the company’s on board safety document that details the policies, procedures and guidelines that the ship’s crew must comply with to meet the obligations set out in the International Maritime Organization’s ISM (International Safety Management code). code. Compliance with the code is mandatory for vessels such as the Rio De La Plata.
- To comply with the code, the flag state must audit and approve the company’s safety management system. Once a company has been successfully audited, a document of compliance (DOC) is issued. Companies are subjected to auditing every year. Also, all vessels in their fleet are audited to verify the implementation of the safety management system and compliance with the ISM code.
- Once a vessel is audited a safety management certificate will be issued by the flag state. It is valid for five years and subject to verification of compliance with the code between year two and three of the certificate’s validity and at renewal every five years.
- The code also requires the company to conduct an internal audit every 12 months to ensure that the requirements of their safety management system are effectively implemented on board their vessels.
Rio De La Plata’s safety management system
- The following section describes the relevant parts of the company’s safety management system that refer to mooring activities and are therefore significant to this accident.
- The safety management system’s instructions on mooring operations ‘Mooring Operations, Document ID: P318’ comprised six sections:
- Personnel and responsibilities
- Mooring procedures
- Tugboats
- Mooring deck areas
- Adverse weather and environment
- References.
- Under the section ’Personnel and responsibilities’, the master was required to appoint ‘responsible persons’ to lead mooring operations at the forward and aft stations. The master was also required to ensure that a sufficient number of crew members were available to safely conduct the mooring operation.
- Under ‘Mooring procedures’ a ‘responsible person’ for mooring operations was required to:
- have read and understood the ‘safe job analysis’ for mooring/unmooring operations
- know the risks in mooring/unmooring operations
- brief the crew and conduct a ‘toolbox’ meeting before mooring/unmooring operations commenced
- reduce the risks as much as possible before and during the operation
- use clear and precise instructions or signals
- supervise the transfer of the mooring rope to the winch drum
- ensure that other team members handle ropes only after being directed by the responsible person.
Safe job analysis
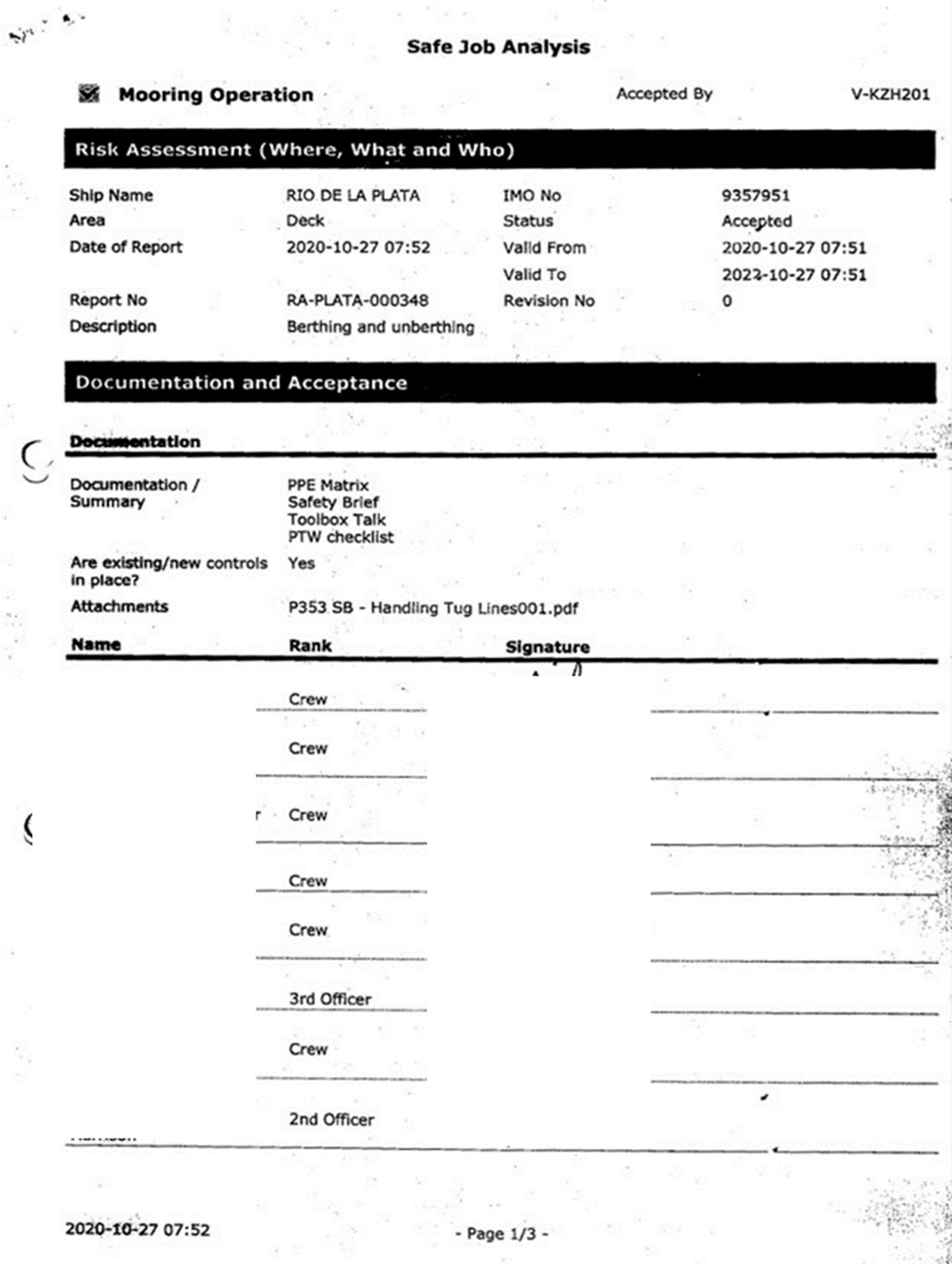
- The safety management system required the crew to conduct a safe job analysis for mooring and unmooring operations. The safe job analysis was a risk assessment for all mooring operations on the vessel, which was last conducted on 27 October 2020 and was valid till 27 October 2022.
- The safe job analysis was divided into the following scenarios:
- Choice of mooring/unmooring station team
- Completion of mooring/unmooring
- Approaching stations
- Preparing for stations
- Actual mooring/unmooring.
- For each scenario, the crew considered associated hazards, existing controls and any new controls that were required. The ‘Choice of mooring/unmooring station team’ scenario and the ‘Actual mooring/unmooring’ scenario are relevant to this accident. See Appendix 1 for a copy of the safe job analysis carried out on 27 October 2020.
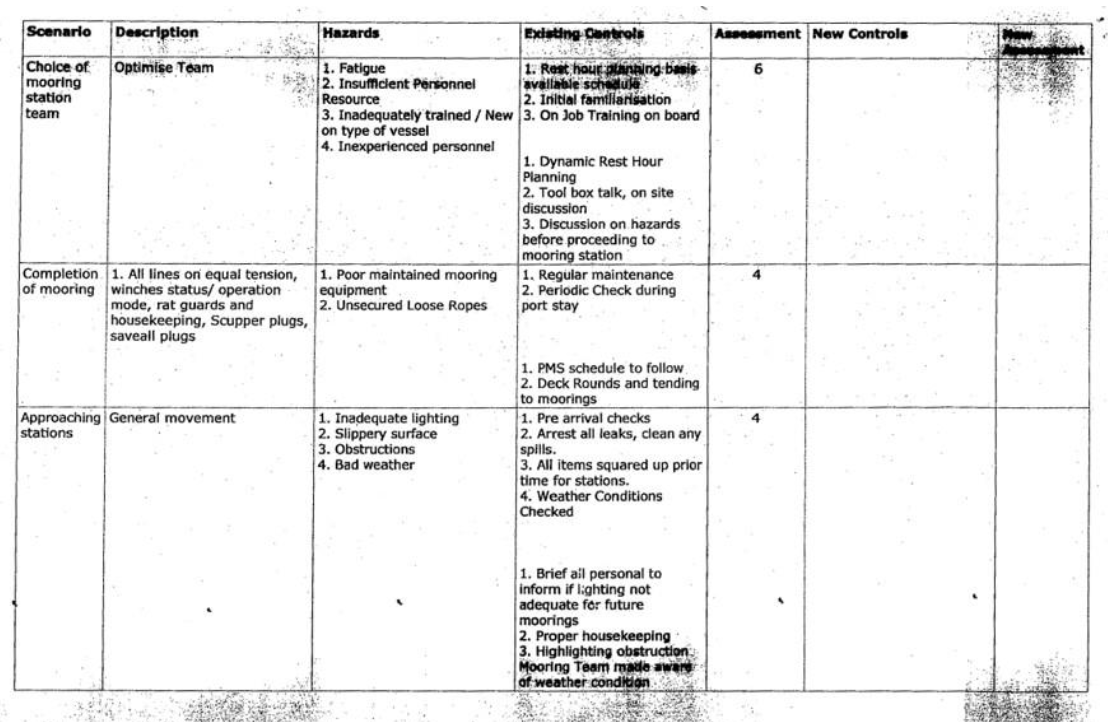
Scenario ‘Choice of mooring station team’
- Three hazards were examined for this scenario: fatigue, insufficient personnel resource, and inadequately trained and inexperienced personnel.
- The control in place to mitigate fatigue was dynamic rest hour planning, and lack of training and inexperience were mitigated through an initial safety familiarisation that the crew received when they joined the vessel and via training they received on the job. Further controls included a toolbox meeting and discussion of hazards before commencing mooring/unmooring operations. There was no clear mitigation put in place to address the risk of insufficient personnel resource.
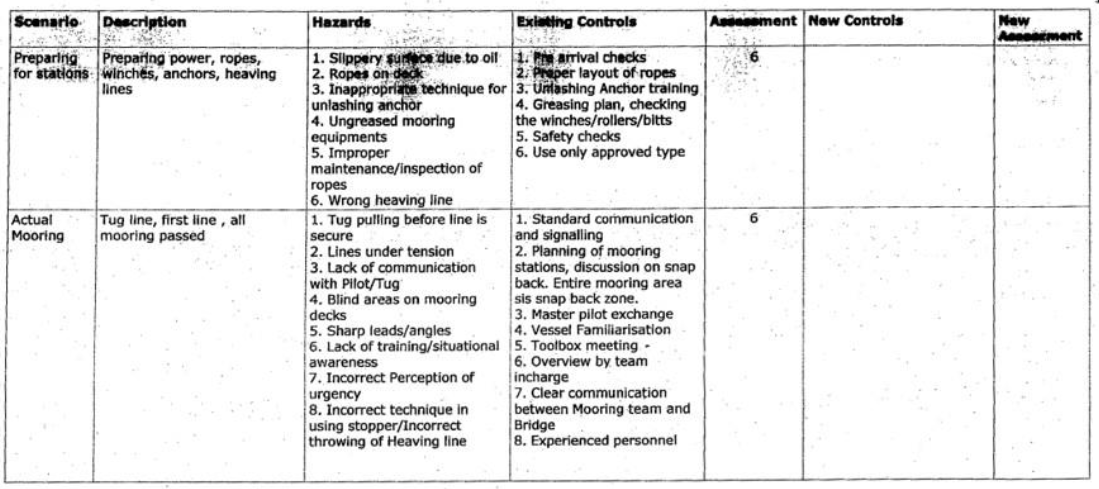
Scenario ’Actual mooring/unmooring’
- Eight hazards were examined for this scenario, and they included blind areas on mooring decks and ‘lack of training/situational awareness’, both relevant to this accident and discussed further in the analysis section of the report. The controls in place to mitigate these hazards were vessel familiarisation and an overview by the person in charge, respectively, along with a toolbox meeting before commencing mooring operations.
Meteorological and ephemeral information
- The weather conditions at the time of the accident were good that morning, with clear skies and good visibility. Prevailing winds were south-westerly force 2 (as indicated on the Beaufort scale, which is mean wind speed of 5 knots or 2.4 metres per second (m/s)), with slight seas and low swells. The barometric pressure recorded was 1009 millibars and the temperature was 17ºC.
Other relevant information
- Communication between the members of the forward mooring team was challenging because of equipment blocking the line of sight and noise levels due to the bow thrusters and the winches being operated at the time.
- The forward team communicated among themselves verbally when possible or by using hand signals.
Analysis Tātaritanga
Introduction
- Mooring is a complex and dangerous operation that can have serious consequences, including fatalities if things go wrong. The risks associated with mooring and unmooring operations are well known in the industry, and there are several guidelines issued by the International Maritime Organization and others to address these risks. However, the focus is often placed on the risks associated with mooring ropes being overloaded and breaking and the identification of safe zones at mooring stations. Unmooring operations, such as those carried out at the time of the accident, are equally dangerous and need to be carefully assessed to mitigate any unsafe situations before they become serious.
- The following section analyses the circumstances surrounding the event to identify those factors that increased the likelihood of the event occurring or the severity of its outcome. It also examines any safety issues that have the potential to adversely affect safe operations in the future.
- The issue of fatigue was assessed and not found to be contributory to this accident.
What likely happened
- When the master instructed to let go the ropes, the forward mooring team lowered the ropes and the shore linesmen cast them off. The forward team picked up two ropes at a time by operating mooring winch M1 and M2 simultaneously. The AB was positioned at the winch controls on the port side and (near mooring winches M1 and M2, respectively) OS1 and OS2 were watching and guiding the ropes onto the storage drums.
- When the ropes were clear of the waterline both OS1 and OS2 proceeded to make final adjustments to stow them correctly on the drums of the respective winches. To complete this task, OS2 had bent down and was manually guiding the rope onto the drum. While bending down to complete this task, OS2 was out of the line of sight of the winch operator who was positioned at the control station on the aft port side of the forward deck.
- OS2 communicated with the winch operator, by raising their right hand and making hand signals over the top of the drum, while still bent down to physically adjust the rope. OS2 was doing two jobs at the same time, while out of sight from the winch operator.
- It is likely that OS2, while completely engaged in communicating and handling the rope, had reduced situational awareness of their own safety and stepped too close to the winch drum. This made it possible for their left hand to get trapped between the rope and the winch, resulting in them being dragged into the storage drum.
- OS2 was wearing two sets of gloves that day – a tight-fitting inner glove and a loose-fitting ‘astro flex blue’ rubber glove on top. The left-hand loose-fitting astro flex blue outer glove was found stuck between turns of stowed rope on the winch drum. It is possible that OS2 may have escaped from more severe injuries as they were able to free themselves from the outer loose-fitting glove.
The operational limitation of the mooring winch
Safety Issue: The mooring winch had not been operated as recommended by the equipment manufacturer, and this increased the risk of injury to the crew operating the winch.
- At the time of the accident the Rio De La Plata was using a mooring rope that was outside of the manufacturer’s design criteria. The length of rope was 20 metres longer than the maximum design length (of 200 metres), but more importantly, the rope was not stowed correctly on the drum and this increased the risk to the crew working the ropes onto the mooring winch.
- The mooring winch has two sections, a tension section (tension drum) and a storage section (storage drum). The storage section is designed to accommodate 158 metres of mooring rope in six layers and the remaining 42 metres is designed to be stowed on the tension section
- The two transverse bars that run across the winch were very likely there since the winches were installed on the Rio De La Plata in 2008. The manufacturer stated that these transverse bars were installed as a support for the transport and alignment of the winch during installation.
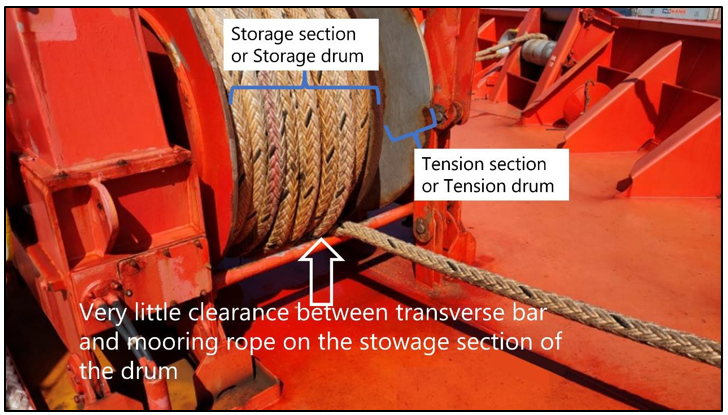
- Immediately prior to the accident, 200 metres of the 220 metre rope was stowed on the storage drum, about 42 metres more than the design limit. This significantly reduced the clearance between the transverse bar and the rope and very likely increased the risk of the mooring rope getting caught at the bar (see figure 9). The transverse bars are required during installation of the winch but serve no safety or operational function thereafter. Removing the transverse bars significantly increases the available clearance and improves the overall safety of the mooring operation as seen in figure 10.

- During the operation of mooring, as the rope is being retrieved, it can be difficult to always ensure that the rope is stored precisely and correctly as it should be on the drum, so there needs to be a margin for error. The additional 20 metres of rope and the presence of the transverse bar together reduced this margin of error by significantly reducing the clearance.
- The Commission has made a recommendation to the manufacturer of the mooring winch to ensure that other operators using the same type of winch are aware of the risks associated with leaving the transverse bar in place after the winch has been installed.
- OS1 and OS2 were tasked to watch the ropes being retrieved, and if the ropes were not stowing correctly, to make the required adjustments to reduce the overhang and prevent it getting caught at the bar. At the time of the accident OS2 was physically adjusting the rope so that it would stow correctly.
- It is very likely that the transverse bar (not required) and the rope too long and incorrectly stowed on the drum created an unsafe working environment where OS1 and OS2 had to physically adjust the rope to ensure it would stow correctly, and this increased the risk of them getting trapped in the process and sustaining serious injury.
Risk assessment for unmooring operations
Safety Issue: The risk assessment for mooring and unmooring operations on board the Rio De La Plata had not complied with the company’s safety management system.
- The mooring operation instructions in the safety management system (see paragraphs 2.48 to 2.52) specified that persons responsible for mooring operations read and understand the safe job analysis. Although not explicitly stated, it was reasonable to expect all crew members taking part in mooring and unmooring operations to be familiar with the risk assessment and the mitigation measures that were in place.
- The Commission reviewed the ship’s safe job analysis for mooring and unmooring operations and found that several risks identified during the assessment had not been properly mitigated. These risks are discussed below.
Blind spot
- The AB operating the winch was positioned at the port side control station located away from the mooring winches and had no visibility of the two OS’s handling the ropes working on the forward side of the winch. The AB was unable to see their actions and, as a consequence, he could not recognise or alert them immediately if they were in a dangerous position.
- The risk of blind areas on the mooring deck was identified during the safe job analysis, but there was no detailed evaluation of the consequences of this risk. The mitigation for blind areas was ‘vessel familiarisation’, but this alone was unlikely to reduce the risk to the OS’s handling the ropes, working unmonitored and without anyone to supervise their actions.
- The resulting situation was that a relatively inexperienced OS2, who was working in the blind area forward of the winch, had to maintain a high level of situational awareness while physically adjusting the rope and signalling to the winch operator with one hand raised above the winch drum.
- The forward mooring team, which was previously a four-member team, had reduced to three members after the deck cadet signed off from the vessel about four weeks before the accident. The risk assessment had identified a lack of sufficient personnel to conduct mooring/unmooring operations as a hazard. This risk remained unaddressed at the time of the accident and likely compounded the issue of working in blind areas of the deck.
- The presence of a fourth person who could stand back and monitor the actions of those handling the ropes, and communicate directly with the winch operator, would have very likely reduced the risk of an accident occurring.
Toolbox meeting
- Another hazard examined during the safe job analysis was a lack of training and inexperience (see paragraph 2.55). This was relevant to OS2, as it was their first time working as an OS. They had only 12 months of previous sea-going experience as a deck cadet in another company and had been on the job for about two-and-a-half months when the accident occurred.
- The mitigation measure to address any ‘lack of training and/or inexperience’ was through an initial safety familiarisation that the crew received when they joined the vessel and via the training they received on the job. All deck crew had completed this familiarisation after they had joined the vessel. The safe job analysis was completed by the deck officers and the deck crew on 27 October 2020. Further controls included a toolbox meeting and discussion of hazards before commencing mooring and unmooring operations.
- It is unclear if the AB conducted a toolbox meeting as intended in the safe job analysis. The AB simply discussed personal protective equipment (PPE) requirements with OS1 as they made their way to the forward mooring deck. It is also unclear if OS2 was present at the time, as there was some evidence to suggest they were securing the accommodation ladder and arrived at the mooring station later. In any case, no discussion of the hazards or any dynamic risk assessment for the unmooring operation in Timaru took place.
- Toolbox meetings are an opportunity for the person in charge to go through the risks and mitigation strategies identified during the safe job analysis, adapt them to the specific operation they are undertaking on the day, and reinforce the mitigation measures to the team before commencing this high-risk activity.
- If the person in charge had conducted a proper toolbox meeting, it is likely they would have identified that the winch operator’s ability to communicate with the team was severely compromised because they were positioned at a blind spot away from the crew handling the ropes.
- Further, a proper toolbox meeting may have identified other mitigation measures, such as changing the unmooring plan to handle one rope at a time (as opposed to two) to compensate for the lack of a fourth person. This would free up a team member to take on a monitoring role and be the communication conduit between the winch operator and the rope handler.
Responsible person
- An AB was the ‘responsible person’ (also known as supervisor) in charge of the forward mooring team. As the responsible person their primary role was to monitor the entire unmooring operation, supervise their team members and identify any problems before they became serious.
- However, the responsible person was also the winch operator, operating the winch from a remote control station located in an area where they had no direct line of sight of their team members.
- Winch operators need to pay careful attention to the control equipment they are operating and also ensure they are following the instructions of the rope handlers as they pick up and store the rope on the winch drum. This is a resource intensive activity and requires the full attention of the operator. It is very unlikely that the AB would have been able to safely carry out the role of supervisor and winch operator at the same time.
- Supervisors need to make sure that mooring and unmooring operations both on board and over the side are always monitored. They need to have a clear overview of the entire area, good visibility of their teammates and act as the point of contact for the bridge and shore-based personnel, which requires their full attention.
- A responsible person’s single most important role is to ensure the safety of their team, which is only possible if they remain an observer and are not physically taking part in handling lines or equipment.
Implementation and auditing of the safety management system
- The safety management system, its policies, procedures and guidelines, are all based on the outcome of risk assessments of the various operations that are undertaken on board. A key aim of the safety management system is to provide a safe working environment for the crew by establishing control measures that either eliminate all identified risks or reduce them to as low as reasonably practicable.
- If a vessel is compliant with the requirements of the ISM code, it is issued a safety management certificate by the flag state. The certificate is valid for five years, and at each renewal the flag state or their representative will audit the safety management system to ensure that it is being appropriately implemented on board.
- A current safety management certificate does not necessarily imply that the vessel is free of accidents or near misses. However, there is an expectation that the auditing authority issuing the certificate (the flag state) has confidence that the safety management system is sufficiently effective to detect and limit risks in the operation.
- The safe job analysis undertaken by the crew for mooring operations deviated several times from the intent of the safety management system because there were many control measures that were lacking or did not sufficiently mitigate the risks identified. This suggests that more can be done to improve the efficiency of the internal audits conducted by the company, as well as the external audits conducted by the flag state or their representative. The Commission has made a recommendation to the vessel’s flag state to address this issue.
Recommendations Ngā tūtohutanga
General
- The Commission issues recommendations to address safety issues found in its investigations. Recommendations may be addressed to organisations or people and can relate to safety issues found within an organisation or within the wider transport system that have the potential to contribute to future transport accidents and incidents.
- In the interests of transport safety, it is important that recommendations are implemented without delay to help prevent similar accidents or incidents occurring in the future.
New recommendations
-
On 27 April 2022, the Commission recommended that the Maritime and Port Authority of Singapore investigate and, if necessary, review their audit processes to see if they can be further developed to identify weaknesses in the safety management system and their practical implementation on board vessels under their flag. (006/22)
On 16 May 2022, Maritime and Port Authority or Singapore replied: We wish to acknowledge receipt of your email and its content.
MPA is aware of the incident and had initiated its preliminary inquiry in accordance with the Merchant Shipping Act of Singapore. This inquiry is conducted independently from the Transport Safety Investigation Bureau’s (Ministry of Transport) Marine Safety Investigation (MSI), whose aim is for lessons learned and the prevention of recurrence, without apportioning blame or liability.
We have reviewed the Company’s investigation report and are satisfied with its corrective / preventive actions to prevent a recurrence, where amongst other things (the Company, in consultation with the winch manufacturer), has removed the cross-over bars under the winches.
MPA has concluded its preliminary inquiry and whilst there was no loss of life involved arising out of this shipboard incident/accident, we have considered this as a case of serious injury. MPA intends to promulgate this case in our regular e-bulletin to the maritime industry to highlight to stake holders the hazards associated with mooring operations. In addition, the case was shared with MPA’s flag State control department to strengthen checks of mooring operations as part of the control and monitoring programme by MPA (as flag State) for Singapore-flagged ships, including FSC inspections / safety management audits for “RIO DE LA PLATA”.
-
On 27 April 2022, the Commission recommended that MacGregor Germany GmbH & Co., the manufacturer of the mooring winch, ensure that other operators using the same type of winch are aware that the transverse bar should be removed after the winch has been installed on the vessel to increase the safe operation of the mooring winch. (007/22)
On 18 May 2022, MacGregor Germany GmbH & Co replied :
We as MacGregor confirm that we will implement the aforementioned recommendation.
The estimated schedule for the related activities is as follows:
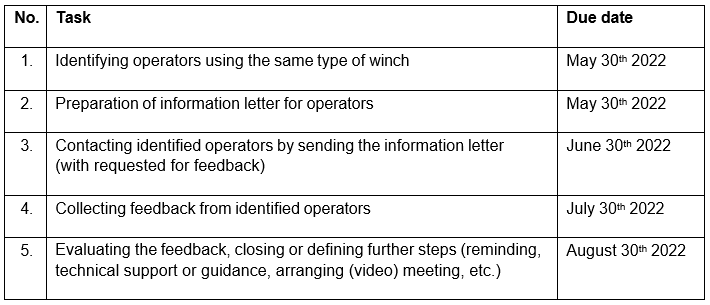
According to the estimated schedule, the final recommendation 007/22 will be implemented until 30th of June 2022. We will inform you once our related activities are completed.
Further steps might be necessary to ensure that our information was received and implemented if required. We will keep you informed in this regard too.
Hope to serve you with this feedback.
Appendix 1. Safe Job Analysis – Mooring Operations