In August 2016, bulk cargo ship Molly Manx was inbound to Dunedin (Ravensbourne pier) with a harbour pilot on board. On approach to the narrow passage between the Halfway Islands, the ship ran aground on a sandbank. Damage was limited to the bottom paintwork. Nobody was injured. Key lessons are that a bridge team must: work with the pilot on route (planning and monitoring); incorporate pilots into bridge resource management; and ensure they can be warned of risks by a correctly configured electronic chart display and information system. The Commission made three recommendations to Maritime NZ to address the safety issues identified.
Executive summary Tuhinga whakarāpopoto

- At about 0600 on 19 August 2016, the bulk carrier Molly Manx arrived off Port Otago after an overnight passage from Lyttelton. A harbour pilot boarded the vessel at about 0630 and, after exchanging information with the master, the vessel entered the narrow channel taking it to its berth.
- The Molly Manx was the maximum permitted length for vessels navigating the upper portion of the channel.
- The vessel had just passed Port Chalmers and was approaching a narrow passage between two islands known as the Halfway Islands with the pilot conducting the navigation of the vessel. Two tugs were in attendance: one connected to the stern of the vessel and one ranging ahead of the vessel, waiting to assist.
- As the vessel neared the Halfway Islands it deviated from the intended track and grounded on a sand bank. With the aid of the vessel’s engine and the tug connected to the stern, the vessel was able to reverse off the sand bank, after which it was manoeuvred stern-first back to Port Chalmers for assessment.
- There was no breach of the hull, and damage was limited to the bottom paintwork. Nobody was injured
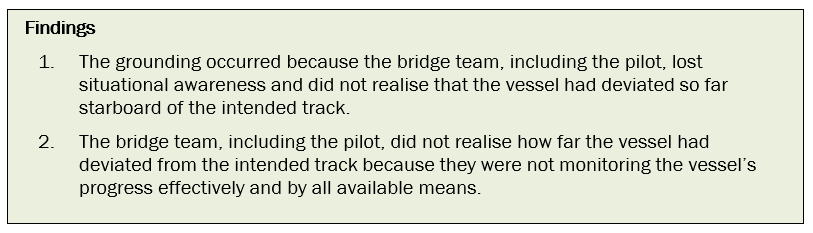
- The Transport Accident Investigation Commission (Commission) found that the vessel grounded because the bridge team lost situational awareness. Because the bridge team was not adequately monitoring its progress using all available means, they did not realise that the vessel had deviated so far starboard from the intended track.
- The Commission also found that: there was no formal shared understanding between the pilot and the vessel’s crew on what passage plan would be used; the vessel’s navigation equipment was not correctly configured for navigating in a narrow channel; and the standard of bridge resource management on the bridge leading up to the grounding did not meet good industry practice.
- The Commission identified four safety issues relating to the standard of passage planning and the performance of the bridge team.
- The Commission made three recommendations to the Director of Maritime New Zealand to address those safety issues identified.
- Key lessons arising from this inquiry include:
- there must be an absolute agreement and shared understanding between the vessel’s bridge team and the pilot as to the passage plan and monitoring against that plan
-
vessels’ bridge teams must actively promote and use the concept of bridge resource management, including the incorporation of pilots into the bridge teams, to manage voyages properly
- a vessel’s electronic chart display and information system (ECDIS) is an important system for monitoring the progress of the vessel and warning the bridge team when things could go wrong. It is essential that it be configured correctly for the phase of navigation and the proximity to navigation hazards.
Conduct of the inquiry He tikanga rapunga
- The Transport Accident Investigation Commission (Commission) was advised of the occurrence by email from Maritime New Zealand on 19 August 2016, the day of the occurrence. The Commission opened an inquiry under section 13(1)b of the Transport Accident Investigation Commission Act 1990 and appointed an investigator in charge.
- On 19 August contact was established with the Isle of Man flag administration and agreement was reached that New Zealand would lead the investigation and conduct the investigation on behalf of the Isle of Man.
- On 19 August two investigators travelled to Dunedin, where the Molly Manx was berthed. On 20 August the investigators conducted interviews with the crew of the vessel and collected evidence that included a download of the vessel’s voyage data recorder.
- On 21 August the investigators interviewed staff from Port Otago and the acting harbourmaster. They also gathered further documents relating to the port operations.
- On 22 August contact was established with the vessel’s operator, and documents relating to the company operation were obtained. Additional information was obtained from Maritime New Zealand and from the vessel.
- On 17 January 2017 investigators conducted further interviews with staff from Port Otago in order to clarify information.
- On 24 August 2017 the Commission approved the draft report to be circulated to interested persons for comment.
- The draft report was distributed to 12 interested parties on 4 September 2017, with the closing date for receiving submissions as 25 September 2017. Six submissions were received that included comments.
- The Commission has considered in detail all submissions made, and any changes as a result of those submissions have been included in the final report.
- On 25 October 2017 the Commission approved the report for publication.
Factual information Pārongo pono
Narrative
- At about 0600 on 19 August 2016, the bulk carrier Molly Manx arrived off Port Otago after an overnight passage from Lyttelton. The vessel was bound, with a cargo of phosphate rock, for the Ravensbourne fertiliser terminal, which was in the upper reaches of the harbour between Port Chalmers and Dunedin. The bridge team tested all the navigation and communication equipment and tested the main engine ahead and astern.
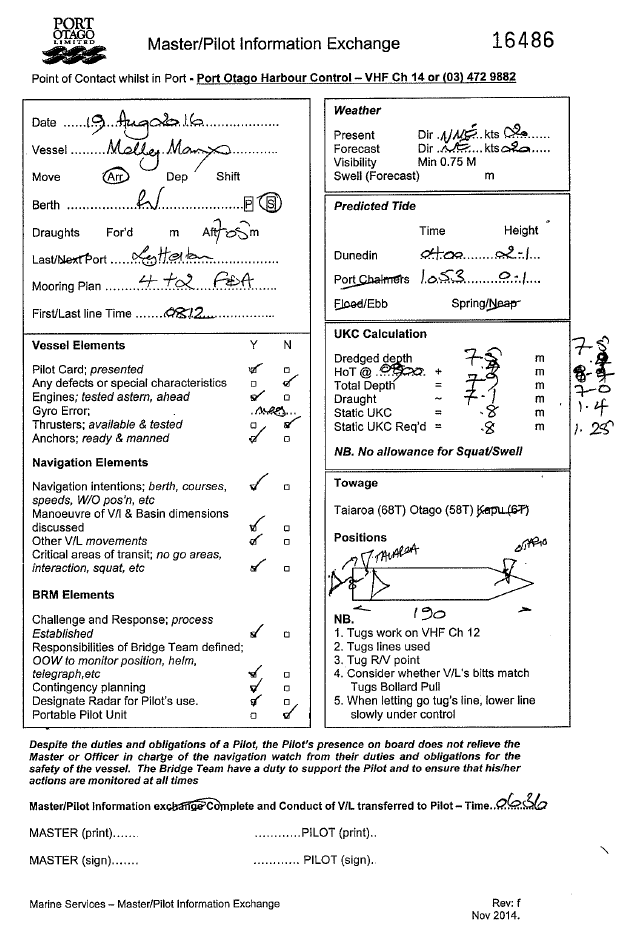
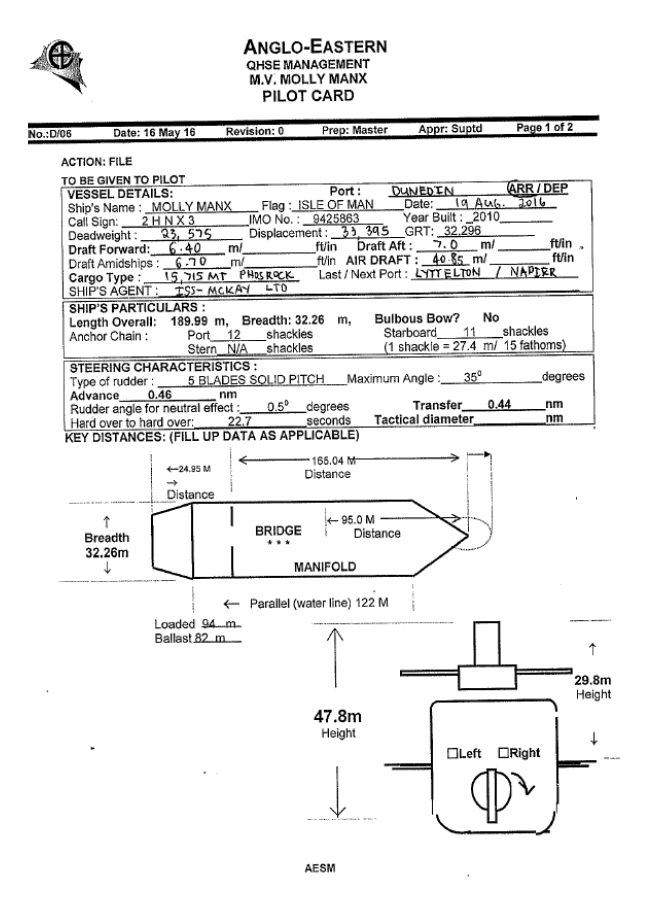
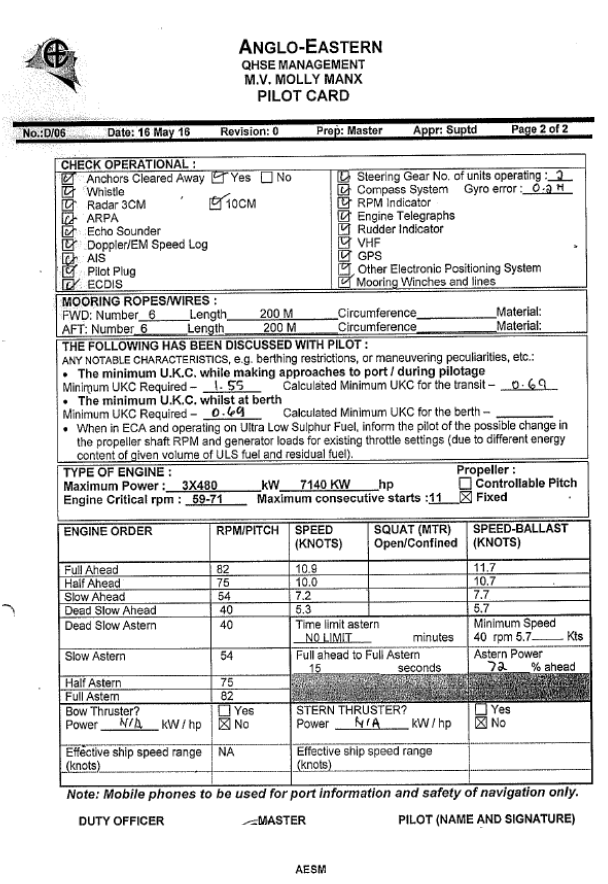
- An Otago Harbour pilot boarded the vessel at about 0630. The master and pilot conducted an exchange of information. The pilot explained the Otago Harbour Passage Plan and the Otago Harbour Passage Planning Guide. The passage planning guide was the document produced by the harbour authority that contained relevant navigational information to assist the vessel’s bridge team in constructing the preferred Port Otago passage plan into Port Otago. The master in turn explained the information contained on the vessel’s pilot card (an information card, form or checklist used to ensure that essential master-pilot exchange items are covered) (see Appendix 1). The pilot noted that the vessel’s arrival draught was deeper than that which the master had previously reported. The deepest draught was 7.1 metres (m), which was still within the maximum allowable draught of 7.4 m for berthing.
- The pilot then took the con from the master and the vessel headed towards the harbour entrance channel. The main engine was increased to full sea speed to achieve the optimum speed of 12 knots for the first section of the pilotage.
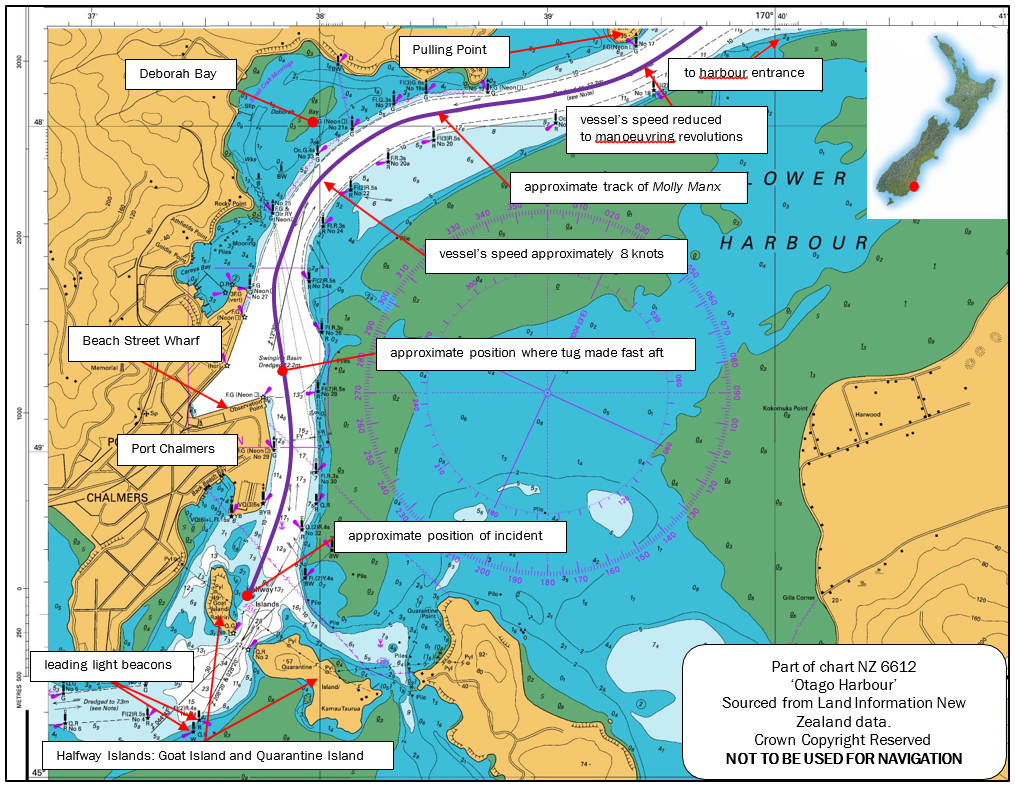
- At 0719 when the Molly Manx was passing Pulling Point (see Figure 1), the pilot requested a reduction in speed from full sea speed to manoeuvring speed, and by the time the vessel reached Deborah Bay (see Figure 1) it was making about 8 knots over the ground.
-
At about 0730, as the vessel passed Port Chalmers, the pilot reduced the engine revolutions to half ahead. Shortly afterwards the line of the tug Taiaroa was secured to the stern of the vessel. The Taiaroa then followed behind the Molly Manx with no weight on the line. The tug Otago proceeded ahead of the vessel, ready to assist with berthing.
- As the Molly Manx passed Port Chalmers, the pilot pointed out to the master the leading line beacons he intended to use to guide the vessel through the narrow gap between Quarantine and Goat Islands (referred to as Halfway Islands on the chart – see Figure 1). At that time the leading marks showed that the vessel was to starboard of the intended track, which the pilot was aware of and where he planned the vessel to be once he had commenced the turn to starboard.
- As the vessel approached the Halfway Islands the pilot was standing at the front of the bridge on or just to starboard of the centreline of the vessel, using the line of the deck cranes to judge the heading of the vessel. He occasionally left this position to check the vessel’s speed on the electronic chart display and information system (ECDIS) located in the aft-facing console behind him. The pilot said that he could see that the channel between the islands was clear and that he was “about on the leads [leading line beacons]”.
- The members of the bridge team, including the pilot, then felt a bump that they initially thought was the aft tug bumping the stern of the vessel.
- The pilot saw that the speed was reducing and he noted that the vessel’s head was swinging to starboard despite the 10 degrees of port helm being applied. Both the master and the pilot realised the vessel had grounded, and ordered stop engines, half astern and full astern in quick succession.
- The Molly Manx stopped in the water, aground on sand. The pilot called the tug Otago ahead of the vessel and ordered it to return and secure a line to the bow. The pilot ordered the aft tug Taiaroa to “lift off at 40 tonnes” (to pull away from the ship with a 40-tonne bollard pull (force)). The vessel started to move astern, at which time the pilot ordered the starboard anchor to be let go to one shackle (a vessel’s anchor chain is usually divided into several sections of equal length (usually 27.5 metres or thereabouts) joined by a special joining shackle. When the anchor and connecting chain are ‘let go’ from the windlass, the person in charge on the forecastle head pays out the cable by a specified amount by counting the joining shackles. Thus one shackle on deck would have the first joining shackle secured on the forecastle deck with the first 27.5 metres of cable and anchor leading through the hawse pipe and into the water) (27.5 m) of cable in an attempt to steady the bow.
- As the Molly Manx moved astern into deeper water, the starboard anchor was raised. The pilot then manoeuvred the vessel stern-first back to Port Chalmers where it was made fast alongside Beach Street wharf. Soundings of all the tanks and spaces on the vessel were taken to ensure that the watertight integrity had not been compromised.
- At about 1300 two pilots boarded the Molly Manx at Beach Street wharf and piloted it through the Upper Harbour to the fertiliser terminal at Ravensbourne. The operator of the vessel engaged a diving and salvage company to carry out an underwater inspection of the vessel to determine if any damage had occurred.
Environmental conditions
- The climatic conditions were described as a light northerly breeze creating a significant northerly wave chop in the harbour of wind against the tide. The visibility was good with clear skies. At the time of the grounding the sun was just rising.
- The tides for Dunedin on 19 August 2016 were as tabled in the New Zealand Nautical
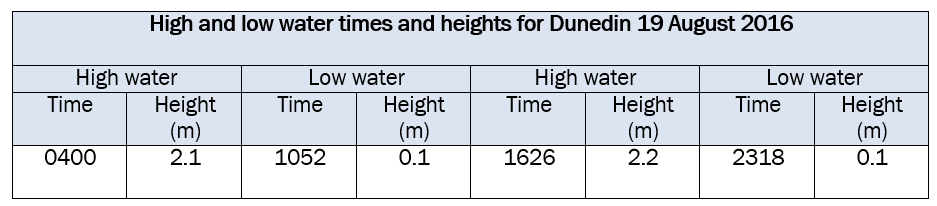
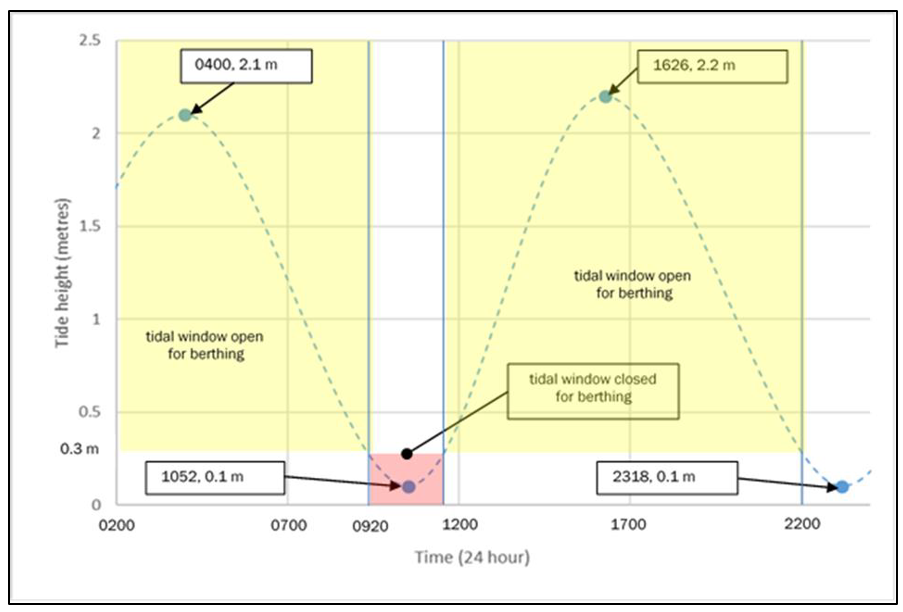
- The vessel could berth on either the flood tide or the ebb tide provided that there was a sufficient depth of water for the vessel to turn. Turning and berthing the vessel could only be achieved between certain times before and after high water; this is known as the tidal window (see Figure 3).
- The length of the Molly Manx was the maximum permitted for vessels transiting the Upper Harbour. It had a draught of 7.1 m, which gave it a tidal window that allowed the vessel to be swung around in the Upper Harbour to berth at the Ravensbourne fertiliser berth.
- On joining the vessel, the pilot had used the Port Otago pilot information sheet to confirm that the vessel could arrive off the berth within the tidal window, which he had then explained to the master (see Appendix 1).
-
The height of tide at the time of the grounding at the Halfway Islands was approximately 0.7 m based on the port data for Port Chalmers, the nearby standard port. The range of the tide was that of a spring tide.
Vessel details
- The Molly Manx was a bulk carrier and had its own shipboard cranes. It had been built in Cebu, Philippines in 2010. It was owned by Molly Marine Limited in the Isle of Man and was registered in the Isle of Man. It was operated by Anglo-Eastern Ship Management Limited of Hong Kong, and at the time of the accident it was chartered to LT Ugland Limited of the Isle of Man.
- The Molly Manx had a length overall of 189.99 m, a breadth of 32.26 m and a maximum draught of 12.826 m. It was powered by a Mitsui M.A.N. – B&W DE 6550MC-C (Mark 7) direct reversing diesel engine producing 8,400 kilowatts at maximum continuous rating driving a single fixed-pitch, right-hand-turning, five-bladed propeller.
- The Molly Manx was equipped with the range of navigational equipment standard for this type of vessel, including an ECDIS and backup system that was compliant with international and Flag State rules and regulations. This configuration meant that the vessel could use the ECDIS as its primary method of navigation and was not required to carry paper charts.
Electronic chart display and information system
-
The International Maritime Organization (IMO) described an ECDIS in the ECDIS Performance Standards (IMO Resolution A.817(19)) as:
… a navigation information system which, with adequate back up arrangements, can be accepted as complying with the up-to-date chart required by regulation V/19 & V/27 of the 1974 SOLAS Convention (The International Convention for the Safety of Life at Sea), by displaying selected information from navigation sensors to assist the mariner in route planning and route monitoring, and by displaying additional navigation-related information if required.
- The master and all navigational officers on board the Molly Manx were correctly certified and had undertaken both generic and type-specific ECDIS training.
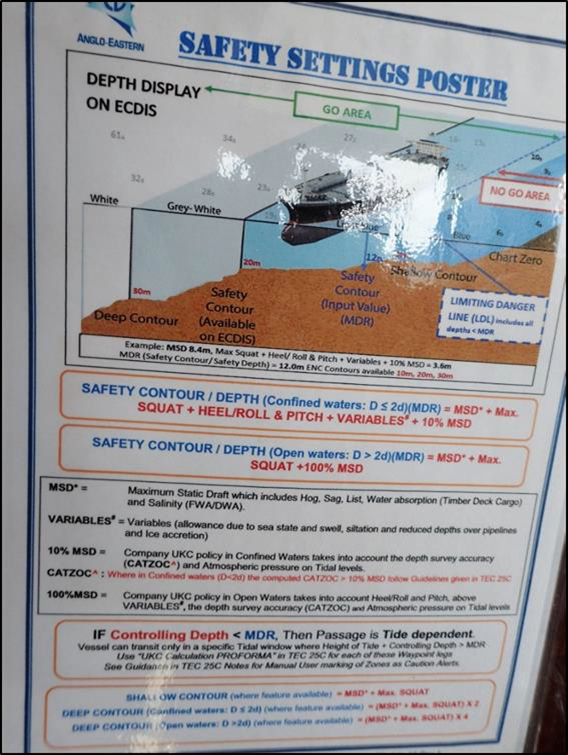
- User-defined safety settings are an important safety function when using an ECDIS. A failure to enter the correct safety settings can allow a vessel to enter unsafe waters without alerting the operator. To achieve a safe passage plan, users of ECDISs must understand how to determine accurately the correct value for a safety setting, as detailed in Table 2.
-
IMO specifications required an ECDIS to trigger certain alarms for the following conditions (see Table 2 on page 17):
-
if the vessel is predicted to cross the safety contour within a user-specified time
-
if the vessel is predicted to cross the boundary of a prohibited area or an area for which special conditions exist within a specified time
-
if the vessel deviates off course by a specified amount from the planned route; cross-track distance
-
if the vessel continues on its present course over a user-defined time or distance and is predicted to pass closer to an object that is shallower than the safety contour or an aid to navigation.
Passage planning
-
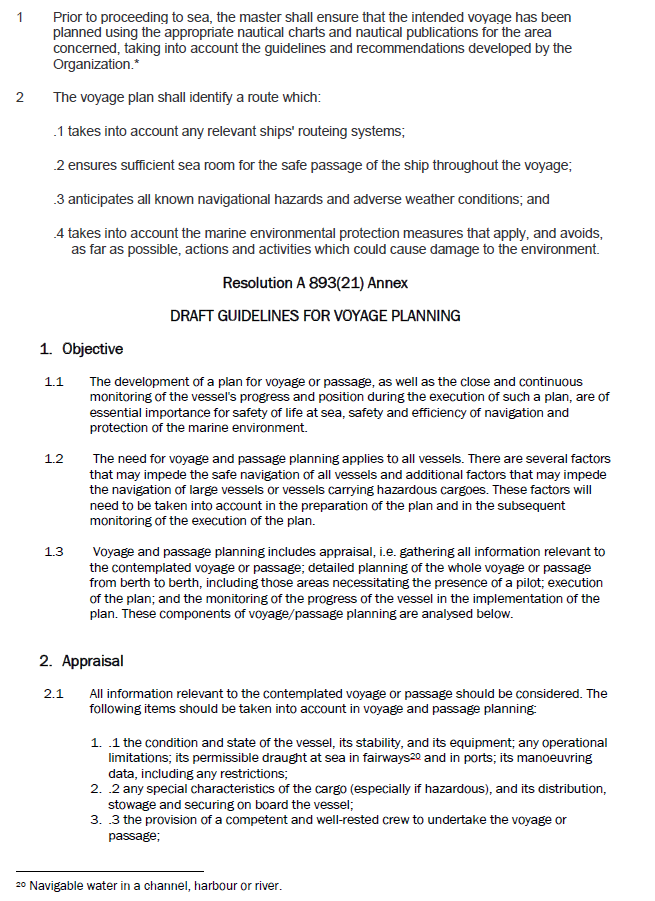
The IMO’s Resolution A.893(21), Guidelines for Voyage Planning, adopted on 25 November 1999 (see Appendix 3), describe voyage (passage) planning as:
1.1 The development of a plan for voyage or passage, as well as the close and continuous monitoring of the vessel’s progress and position during the execution of such a plan, are of essential importance for safety of life at sea, safety and efficiency of navigation and protection of the marine environment.
1.2 The need for voyage and passage planning applies to all vessels. There are several factors that may impede the safe navigation of all vessels and additional factors that may impede the navigation of large vessels or vessels carrying hazardous cargoes. These factors will need to be taken into account in the preparation of the plan and in the subsequent monitoring of the execution of the plan.
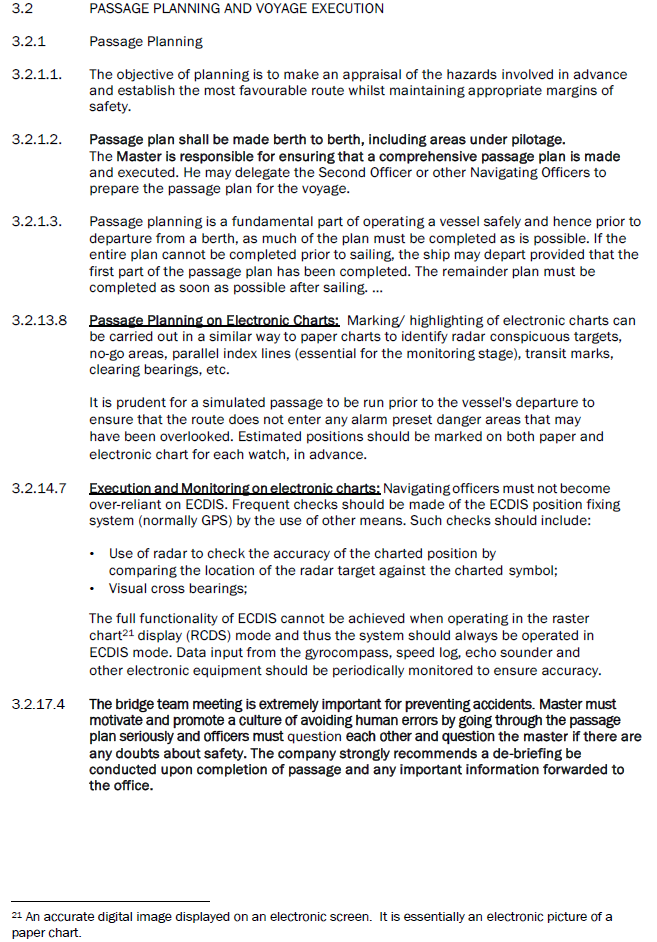
1.3 Voyage and passage planning includes appraisal, i.e. gathering all information relevant to the contemplated voyage or passage; detailed planning of the whole voyage or passage from berth to berth, including those areas necessitating the presence of a pilot; execution of the plan; and the monitoring of the progress of the vessel in the implementation of the plan.
A more detailed explanation of the requirements can be found in Appendix 3.
Bridge resource management
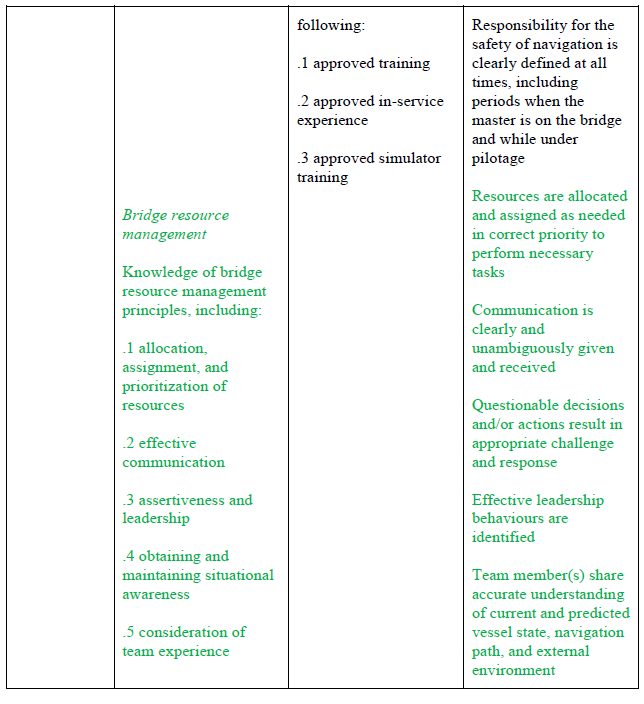
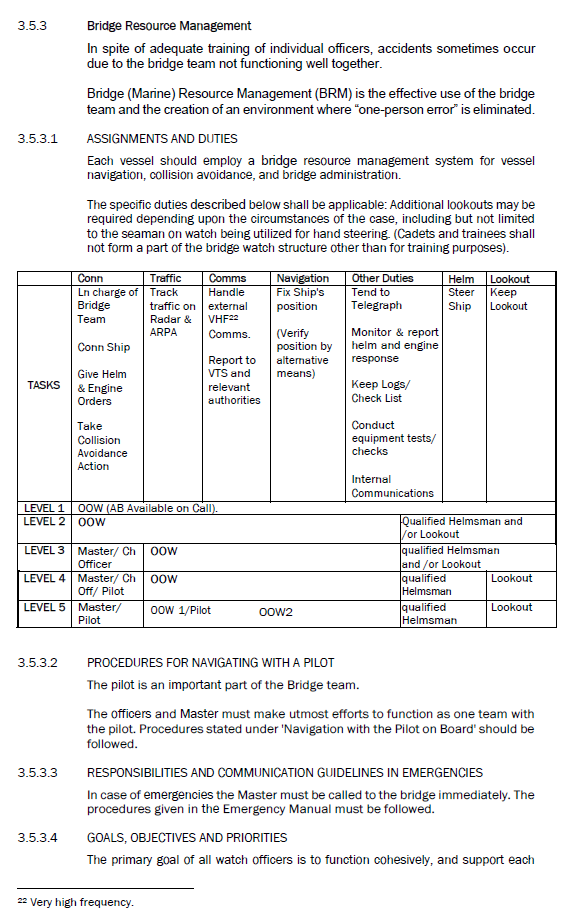
- Bridge resource management (BRM) was adopted in the early 1990s by the maritime industry as a safety and error management tool. It has since become an integral part of crew training and is included in the International Convention on Standards of Certification and Training and Watchkeeping developed by the IMO (see Appendix 2).
- BRM is described as the effective management and utilisation of all resources, human and technical, available to a bridge team, to help ensure the safe completion of the vessel’s voyage.
- Some essential aspects of BRM are good closed-loop communications (a technique used to avoid misunderstandings. When the sender gives a message, the receiver repeats this back. The sender then confirms the message, usually by using the word ‘yes’. When the receiver incorrectly repeats the message back, the sender will say “negative”, or something similar, and then repeat the correct message), participants sharing the same understanding of a planned passage, and maintaining situational awareness.
Analysis Tātaritanga
General
- A vessel grounding, for however short a time, is a serious occurrence that can cause damage to the vessel and the environment.
- Many large vessels successfully complete the transit of the Upper Harbour under pilotage every year. The following analysis discusses why on this occasion the vessel grounded. It also discusses four safety issues:
- the vessel’s bridge team and the pilot did not have a shared understanding of a common passage plan before the pilotage began. Consequently the pilot and the vessel’s bridge team had different understandings of the planned track to be followed and their respective roles in monitoring against the plan
- the IMO has set standards for passage planning that vessels must adhere to, but there is no corresponding requirement for the passage plans that pilots create and use to meet those same standards
- the crew were not using the ECDIS in the correct configuration required by the IMO and company standards when the grounding occurred
- the standard of BRM on board the Molly Manx during the Otago pilotage did not meet good industry practice.
- The length of the Molly Manx was the maximum permitted for a vessel transiting the Upper Harbour, and with a draught of 7.1 m there was little margin for error. This meant it was important for the transit to be carefully managed and monitored by the bridge team.
- The vessel was correctly certified and was manned with crew in excess of the safe manning certificate. The pilot who joined the vessel off the harbour entrance held a pilot’s licence that was current for piloting a vessel of the type and size of the Molly Manx in that port.
What happened
- The pilot had successfully piloted the vessel from beyond the entrance to Otago Harbour and was maintaining a speed that would allow him to berth the Molly Manx within the available tidal window. As the vessel approached Port Chalmers, the pilot reduced the speed of the vessel as the two tugs arrived to assist. One tug proceeded ahead of the vessel while the other was secured to the stern. Having the tug secured to the stern would have allowed the pilot to use it as a means of reducing speed or to assist with steering. The speed of the vessel and the configuration of the assisting tugs were appropriate for the passage between the Halfway Islands.
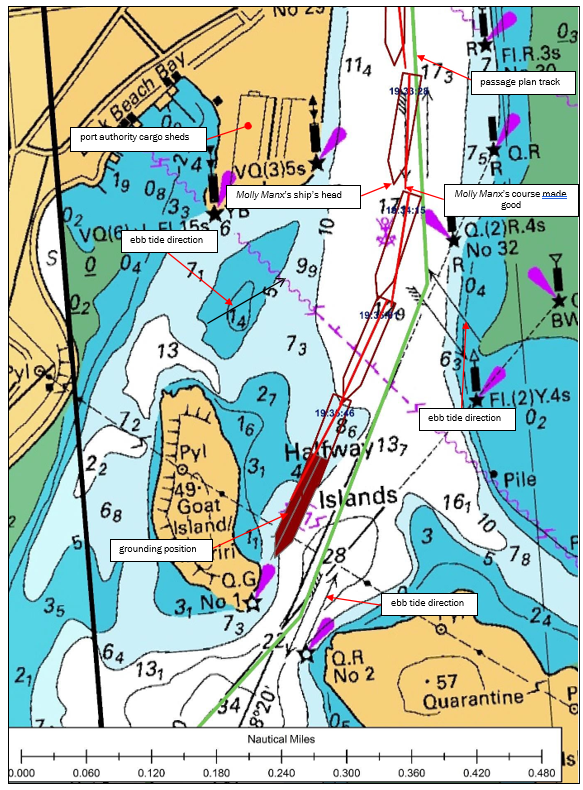
- The Molly Manx passed Port Chalmers and a log storage area and storage sheds. The ebb tide as shown on the chart (see Figure 3) would normally have pushed (set15) the vessel from left to right (port to starboard) as the vessel approached the narrows. However, the Otago Harbour pilots were aware that during an ebb tide the vessel would be first affected by the tidal stream emanating from behind Goat Island that would set the vessel from right to left (starboard to port). It was for this reason that the pilot was comfortable with being to starboard of the planned track as the vessel was passing the storage sheds, in anticipation of the vessel being set back onto the planned track before navigating between the islands.
- When the vessel passed the storage sheds, the pilot ordered starboard helm to start the turn into the channel to pass between Quarantine and Goat Islands and to counteract his prediction that there would be a strong set from right to left from the ebb tide flowing between Goat Island and the Port Chalmers peninsula (see Figure 3).
- The pilot was standing at the front of the navigating bridge either on the centreline of the vessel or one or two paces to starboard. From his position he could see clearly down the channel between the islands and the leading line beacons beyond. From his position he was not able to see either the radar or the ECDIS screen. He was navigating the vessel by eye with an occasional check on the vessel’s speed log readout on the panel above the forward bridge windows.
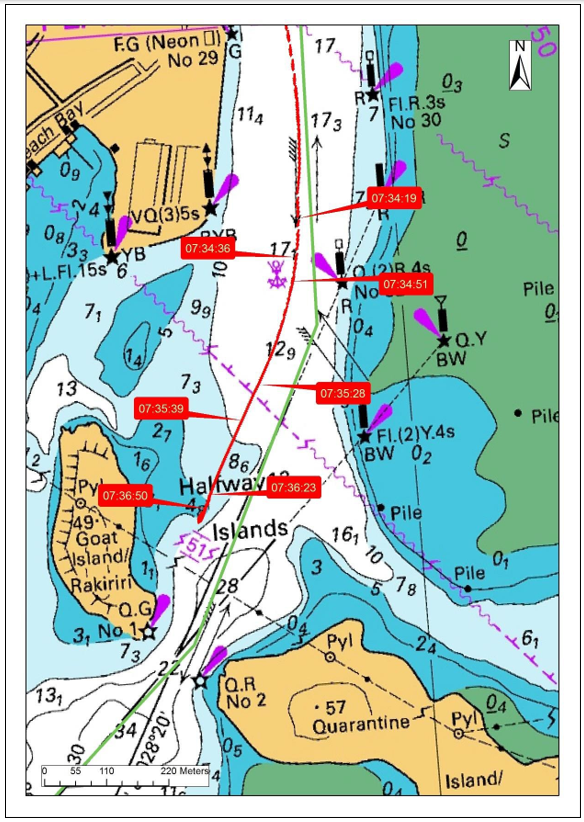
- Using data downloaded from the vessel’s voyage data recorder it was possible to calculate the vessel’s heading and match that to the true course and speed over the ground at the time (see Figure 2. The data showed that from 0734:20 the tidal stream between Goat Island and Port Chalmers did set the vessel from right to left as predicted by the pilot. However, the pilot adjusted the heading of the vessel to counter this set and the vessel remained to starboard of the planned track.
- The vessel then entered the area where it began to be set in the opposite direction, from left to right, then moved further to starboard of the planned track.
- The pilot made a succession of helm orders for 5, 10 and then 15 degrees of port helm and then ordered the helm to “amidships” in anticipation of the change in direction of the tidal set. The pilot then noticed that the vessel was to starboard of the line of the leading beacons. He ordered 5 then 10 degrees of port helm and then ordered the helm to amidships.
- However, although the bow of the vessel was pointing towards the gap between the islands, the vessel was still too far to starboard of the planned track, and the bow of the vessel entered the area of shallow water inside of Goat Island and grounded. The momentum of the vessel carried it over the shallow water, causing it to swing to starboard (see Figure 5).
- Until the pilot felt the vessel grounding, he had not appreciated how far to starboard of the planned track the vessel was. He had lost awareness of exactly where the vessel was in the channel and the influence that the tide was having on its progress. The risk of this happening is high when navigating large vessels in narrow channels using only visual references to monitor the vessels’ progress. It is why all available means by all available persons should be used to monitor the progress of a vessel along its planned track. These points are discussed in more detail in the following sections.
- The pilot realised that something was wrong when he, along with the rest of the bridge team, felt a bump. He noticed that the speed of the vessel was slowing and the vessel’s bow was swinging to starboard despite his having just applied port helm. He realised from these indicators that the vessel was grounding and immediately ordered the engine to stop and then astern and for the tug secured aft to pull right aft. In doing so the pilot was able to manoeuvre the vessel off the bank and back into deeper water.
Passage planning
Safety issue: The vessel’s bridge team and the pilot did not have a shared understanding of a common passage plan before the pilotage began. Consequently, the pilot and the vessel’s bridge team had different understandings of the planned track to be followed and their respective roles in monitoring against the plan.
Safety issue: The IMO has set standards for passage planning that vessels must adhere to, but there is no corresponding requirement for the passage plans that port authorities create and use to meet those same standards.
- When a pilot joins a vessel prior to the pilotage it is the first opportunity for the master and bridge team to: talk to the pilot; clarify any issues that may have been identified during the preparation of the passage plan; and ensure they are satisfied with the planned transit. At this stage the pilot needs to be fully integrated into the bridge organisation so that the whole team works as a cohesive body and has a shared understanding of the passage plan.
- Before any pilotage act begins, it is essential that the pilot and the master (including other members of the team) have a shared understanding of the passage plan. That did not happen in this case. As often happens, the pilot intended to navigate to the standard port company passage plan, and the vessel had its own passage plan, which differed from that of the port company.
- An essential part of integrating the pilot into the bridge team is the pilot and master exchange of information, a briefing that should include all members of the bridge team. The briefing is a bilateral exchange of important information where everyone is made aware of: any changes to the proposed plan; the handling characteristics of the vessel; and any notable ‘dynamic’ information such as weather and tides for the transit.
- The port passage plan was available over the internet from the Port Otago website. The channel is narrow and there is little scope for deviating from the plan without leaving the navigational channel. The preferred courses were presented as smooth, curved lines without any marked waypoints, turn radii or off-track limits. Without that information the vessel’s crew would not have been able to replicate it in their own navigation systems, such as the ECDIS. The vessel was required to plan the passage in accordance with the IMO convention standards and guidelines (Chapter V, Safety of Navigation, of the Annex to the International Convention for the Safety of Life at Sea and Resolution A.893(21) Guidelines for Voyage Planning) (see Appendix 3), but there was no international or New Zealand requirement for the port companies and their pilots to follow the same standards when developing their own generic passage plans. The Port Otago passage plan as presented on its website would not meet the IMO standards or other reputable guidelines available to mariners on voyage planning (Other best-practice guidelines also contain valuable advice on bridge watchkeeping in general and voyage planning in particular. They include: the United Kingdom’s Maritime and Coastguard Agency’s guidance on Chapter V, Safety of Navigation, of the Annex to the International Convention for the Safety of Life at Sea; the Nautical Institute’s Bridge Team Management – A practical guide; and the International Chamber of Shipping’s Bridge Procedures Guide.)
- When the pilot joined the Molly Manx he and the master discussed the vessel’s characteristics and went through the Otago Harbour passage plan.
- However, the vessel had its own passage plan loaded into the ECDIS, which differed from that of Port Otago. Because the vessel’s plan was the plan loaded into the ECDIS, that is what the bridge team, excluding the pilot, was using to monitor the vessel’s progress. Meanwhile, the pilot was navigating the vessel to the Port Otago passage plan, using visual references as he had been trained to do. The bridge team, which now included the pilot, was not aligned in its thinking and did not share the same understanding of the plan. This dynamic was going to make effective BRM difficult to achieve, which is discussed in the following section.
- The New Zealand Port and Harbour Marine Safety Code is a voluntary national standard. The Code recommends that, “Up-to-date passage plans and guidance should be published, and be available to harbour users and the masters of visiting vessels” (see Appendix 6).
- One method of ensuring that an approved passage plan is available on board would be for port companies or harbour authorities to make available to vessels properly constructed and validated passage plans that meet the port-specific standards and guidelines included in Chapter V, Safety of Navigation, of the Annex to the International Convention for the Safety of Life at Sea (SOLAS), and Resolution A.893(21) Guidelines for Voyage Planning. Such a system would assist in on-board passage planning and allow a vessel to be better prepared when the pilot boards. This action would greatly assist the smooth transition of the pilot into the bridge team at a time of typically high workload and little time before the pilotage begins.
- More vessels are using ECDISs as the primary means of navigation, and this will increase in the future. As it was on board the Molly Manx, the passage plan to the berth is usually loaded into the vessel’s ECDIS. Ideally, passage plans generated by port companies should be to the same IMO standards that vessels are required to meet, and should be compatible for use in an ECDIS.
- Many vessels transit more than one New Zealand port. It would greatly enhance safety if the passage plans were, as far as practicable, in a standard format and could be found at one site. Vessels routed to several New Zealand ports would be able to access from one place standardised passage plans for several ports, even before they departed from their previous overseas ports.
- Currently there can be issues with uploading standardised passage plans into an ECDIS, because ECDIS manufacturers have proprietary systems that require specific formats. However, that will shortly change. The International Hydrographic Organization and the International Electrotechnical Commission standard for ECDISs (IEC 61774 Edition 4, September 2015) from August 2017 includes a route exchange format that will make it easier for data transfers. In the future it will be possible to send passage plans to all vessels in the correct format to be uploaded directly into the ECDIS system, thereby reducing the possibility of navigating officers making errors when loading them into ECDISs. However, this facility was not available at the time of the accident and therefore was not able to be used by the bridge team on this occasion.
- The Commission has made recommendations to Maritime New Zealand to promote the use of standard passage plans by all New Zealand harbour authorities.
Molly Manx electronic chart display and information system
Safety issue: The crew were not using the ECDIS in the correct configuration required by the IMO and company standards when the grounding occurred.
- The Molly Manx was approved to use an ECDIS as a primary means of navigation and as such did not have to carry or use paper charts for navigation.
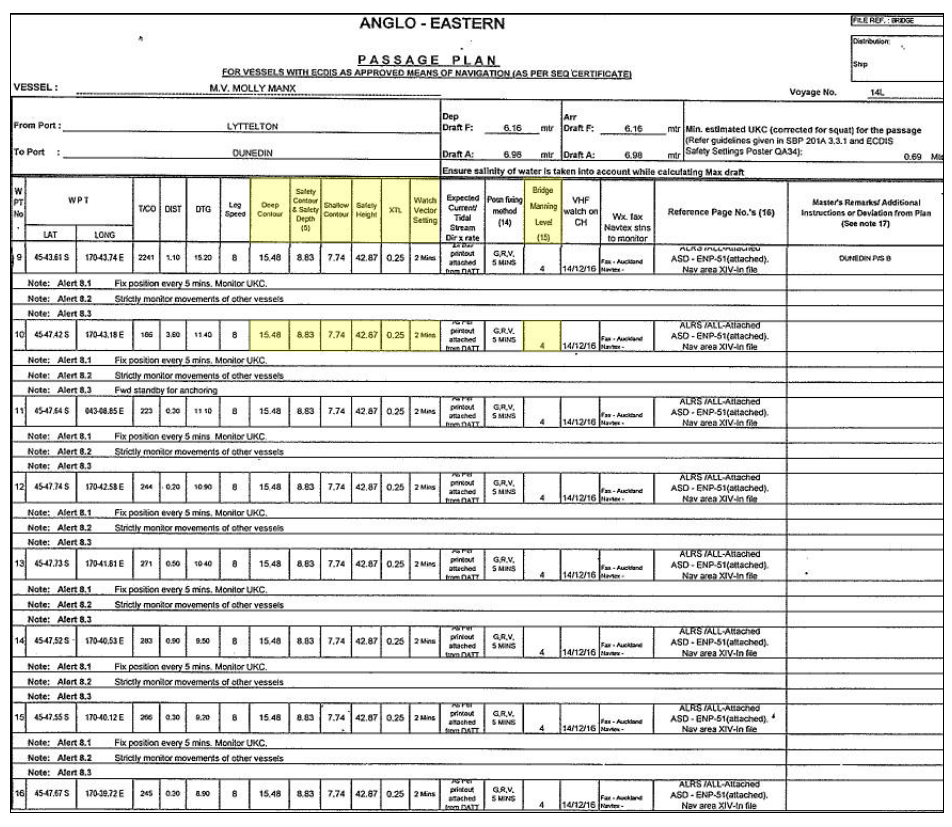
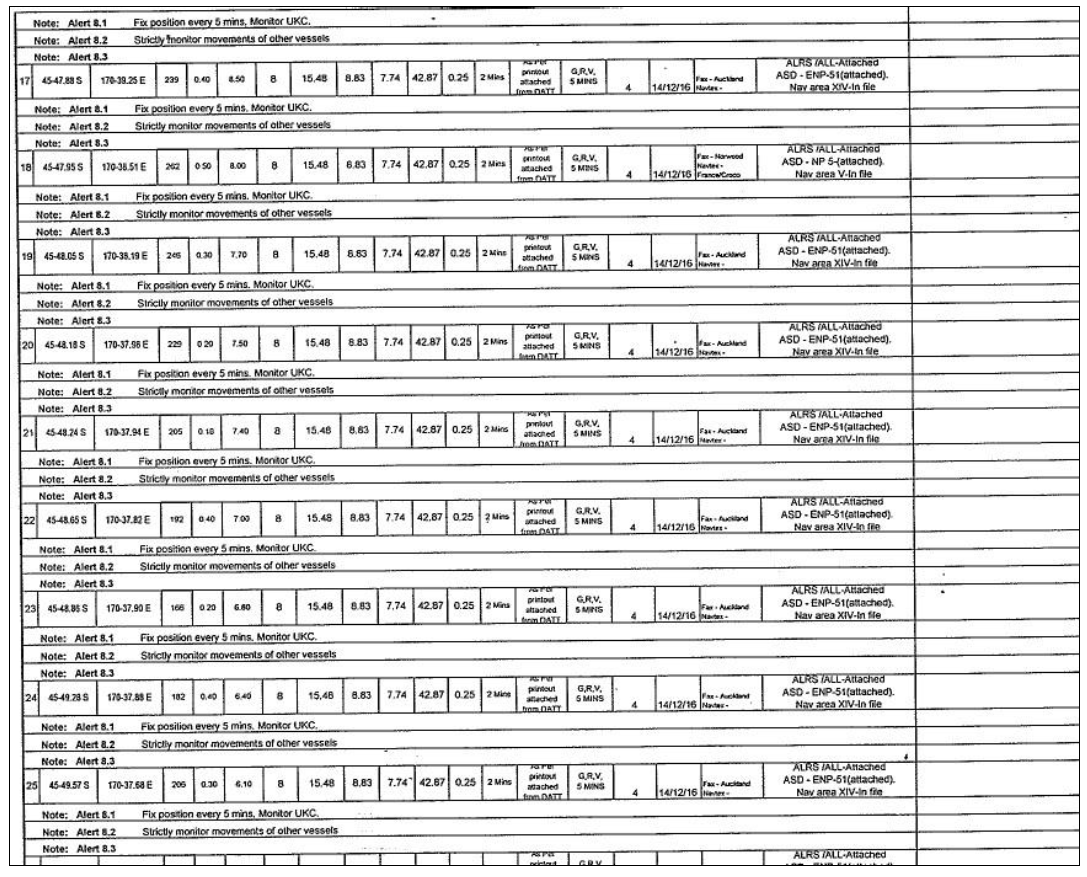
- User-defined safety settings are an important safety function when using an ECDIS. A failure to enter the correct safety settings can allow a vessel to enter unsafe waters without alerting the operator. To achieve a safe passage plan, users of ECDISs must understand how to determine accurately the correct value for a safety setting as detailed in Table 2 on page 16. The Molly Manx’s passage plan included settings for the deep contour, safety contour and safety depth, shallow contour, cross-track limit and watch vector settings (look ahead).
- Some of the values of user-defined ECDIS safety settings in use on board the Molly Manx differed from the values stated in the vessel’s passage plan and from the usual default settings.
- The cross-track distance to either side of the vessel was set at 0.25 nautical miles or 463 m as per the passage plan. However, the narrowest width of the Port Otago channel was approximately 100 m. The vessel would therefore have been 413 m outside the channel before the cross-track distance alarm would activate. At the position of the grounding the vessel was approximately 75 m off track. The settings in the ECDIS were not appropriate for the intended passage into Port Otago.
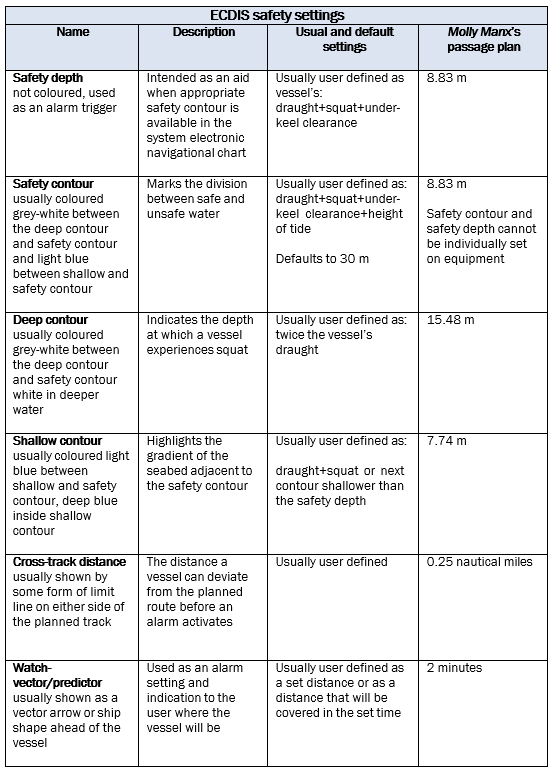
- The watch vector or predictor was required to be set for two minutes according to the passage plan. At the time of the grounding the ECDIS display showed that the vector was set at 10 minutes rather than two minutes as specified in the vessel’s passage plan. In a winding channel such as Otago Harbour, setting the watch vector to 10 minutes would very likely cause the head of the vector to be constantly outside the safe navigable water within the channel, which means it would be in a constant state of alarm. Apart from creating alarm management issues for the officer of the watch (OOW), it was unable to alert the bridge team to any safety hazards ahead.
- Accurate user-defined settings are essential if an ECDIS is to provide the level of navigational safety expected of it. This accident shows how ineffective it can become if the settings that have been entered are incorrect.
Bridge resource management
Safety issue: The standard of BRM on board the Molly Manx during the Otago pilotage did not meet good industry practice.
Implementation of BRM on board
- Achieving a high standard of BRM during the pilotage to Port Otago was going to be difficult because the fundamental requirement of all working to the same passage plan had not been met. Nevertheless, effective BRM could still have prevented the grounding, but it was essentially absent amongst the bridge team.
- The OOW and the helmsman were part of the bridge team, but they were not included in the briefing between the master and the pilot. The absence of the OOW, the relieving OOW and the helmsman from the briefing was a missed opportunity to ensure that everyone was sharing the same understanding, and reinforced the need to engage in challenge and response and ensure that the pilot was incorporated into the bridge team.
- The navigable channel through Otago Harbour to Dunedin is narrow. For a vessel the size of the Molly Manx there are very few possible variations to the preferred courses. Even if the OOW had been monitoring the progress of the vessel against the vessel’s passage plan with agreed off-track limits, the vessel’s deviation to starboard of the track could and should have been noticed and raised with the master and pilot. However, the ECDIS had not been correctly configured for the transit of the narrow channel, and the OOW had not been invited to challenge the master or pilot if the vessel deviated from the intended route.
- As the vessel entered the Otago Harbour pilotage the OOW was relieved. The relieving OOW was not briefed by the master on what was expected of him or made aware of significant information from the master-pilot exchange of information. He was therefore not fully incorporated into the bridge team.
-
Despite the pilot advising the master at the master/pilot exchange that he welcomed being challenged by the bridge team, and explaining the contents of the Port Otago Master/Pilot Information Exchange sheet (see Appendix 1), which includes the notation:
Despite the duties and obligations of a Pilot, the Pilot’s presence on board does not relieve the Master or Officer in charge of the navigation watch from their duties and obligations for the safety of the vessel. The Bridge Team have a duty to support the Pilot and to ensure that his/her actions are monitored at all times.
The pilot said that after the OOWs had changed he soon realised that he was working very much on his own. It was a situation that the pilot said he was familiar with. As difficult as it will be to encourage a bridge team to engage fully in the conduct of a vessel when it is not their normal culture to do so, a pilot should nevertheless challenge the navigation team to do so, as should a navigation team do in a reciprocal situation where a pilot lapses into a one-person operation. A breakdown in BRM can never be attributable to only one of the participants.
- The relieving OOW assumed responsibility for: operating the engine telegraph; monitoring the helmsman and ensuring the correct helm was applied; checking the under-keel clearance; and checking the vessel’s position on the ECDIS. These were important tasks. Both the master and the OOW noticed the vessel deviating to starboard, but neither spoke up and alerted the pilot to the vessel’s position. There was silence on the bridge as the vessel ran aground.
- The company’s safety management system had comprehensive sections on BRM and the requirement for passage planning from berth to berth (see Appendix 5) (as contained in Chapter V, Safety of Navigation, of the Annex to SOLAS, Regulation 34 Safe Navigation and Resolution A.893(21) Guidelines for Voyage Planning) (see Appendix 3 for relevant parts).
- However, including a requirement to practise good BRM and planning the passage in a safety management system does not fulfil a company’s and master’s obligations in that regard. Putting the concepts into practice is the key. Unless managers and masters believe in, promote, practise and drive good BRM skills, they are unlikely to succeed.
- The Commission would normally make a recommendation to the Flag State administration for the vessel to address through Flag State control any deficiencies in bridge practices. However, the vessel is now under different operation and has been re-registered with a different Flag State.
Appendix 1. Port Otago pilot information sheet and the vessel’s ‘pilot card’
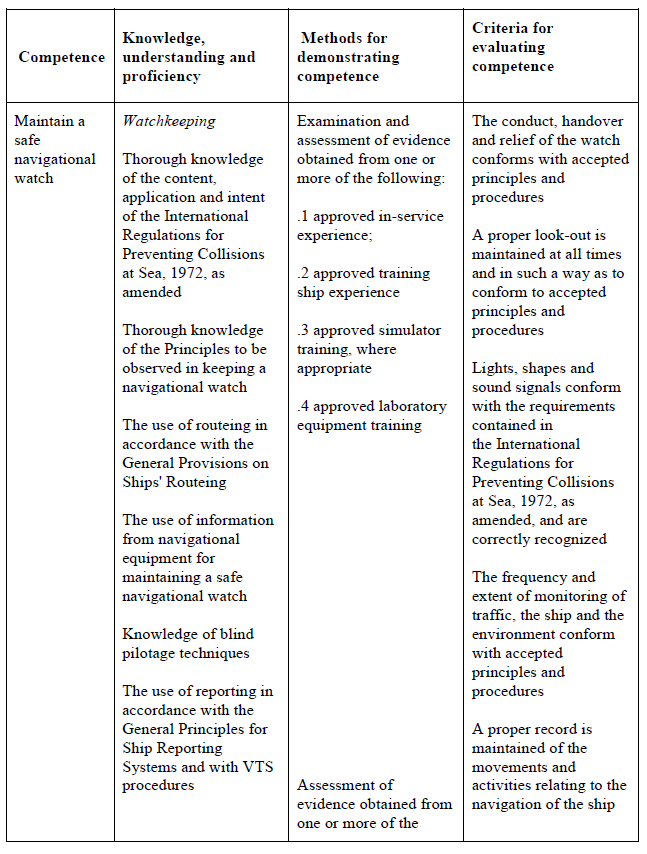
Appendix 2. Standards of training, certification and watchkeeping Manila 2010, code Chapter II, table A-II/1
Table A-II/1 Specification of minimum standard of competence for officers in charge of a navigational watch on ships of 500 gross tonnage or more
Function: Navigation at the operational level
Appendix 3. SOLAS Chapter V, Regulation 34 Safe Navigation and Resolution A 893(21) Annex
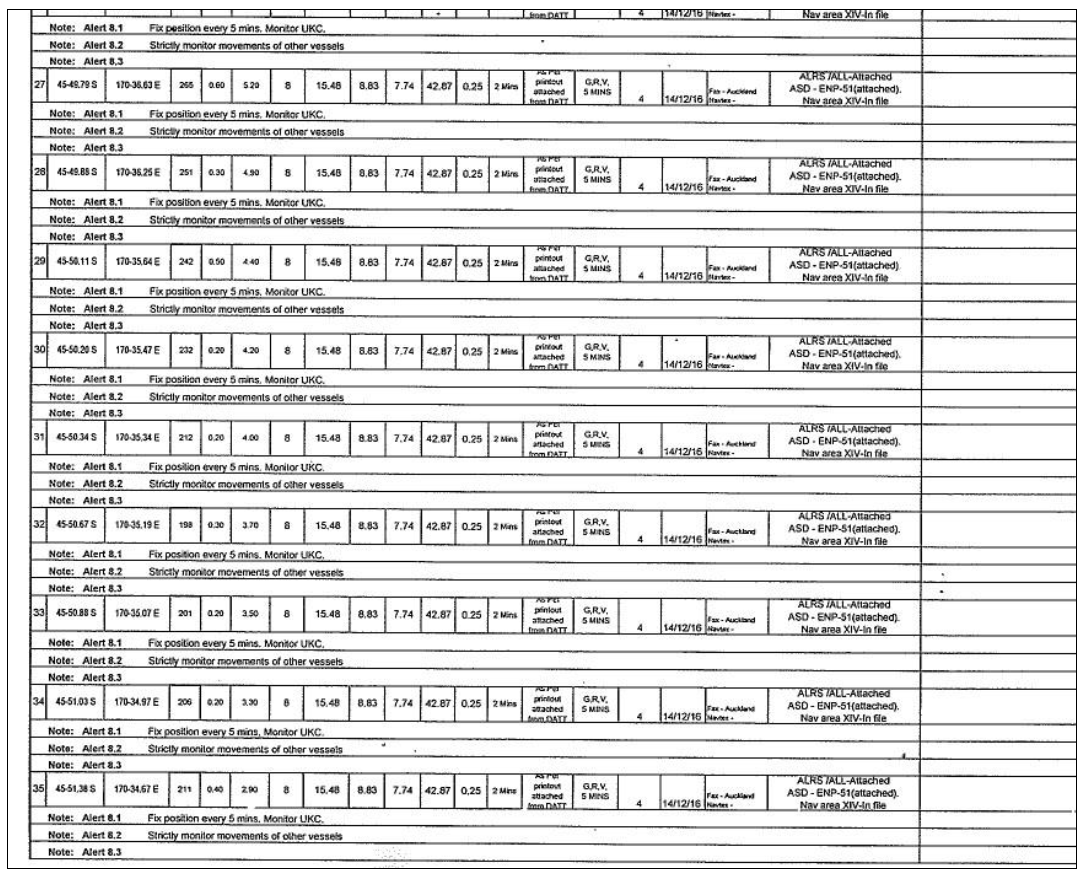
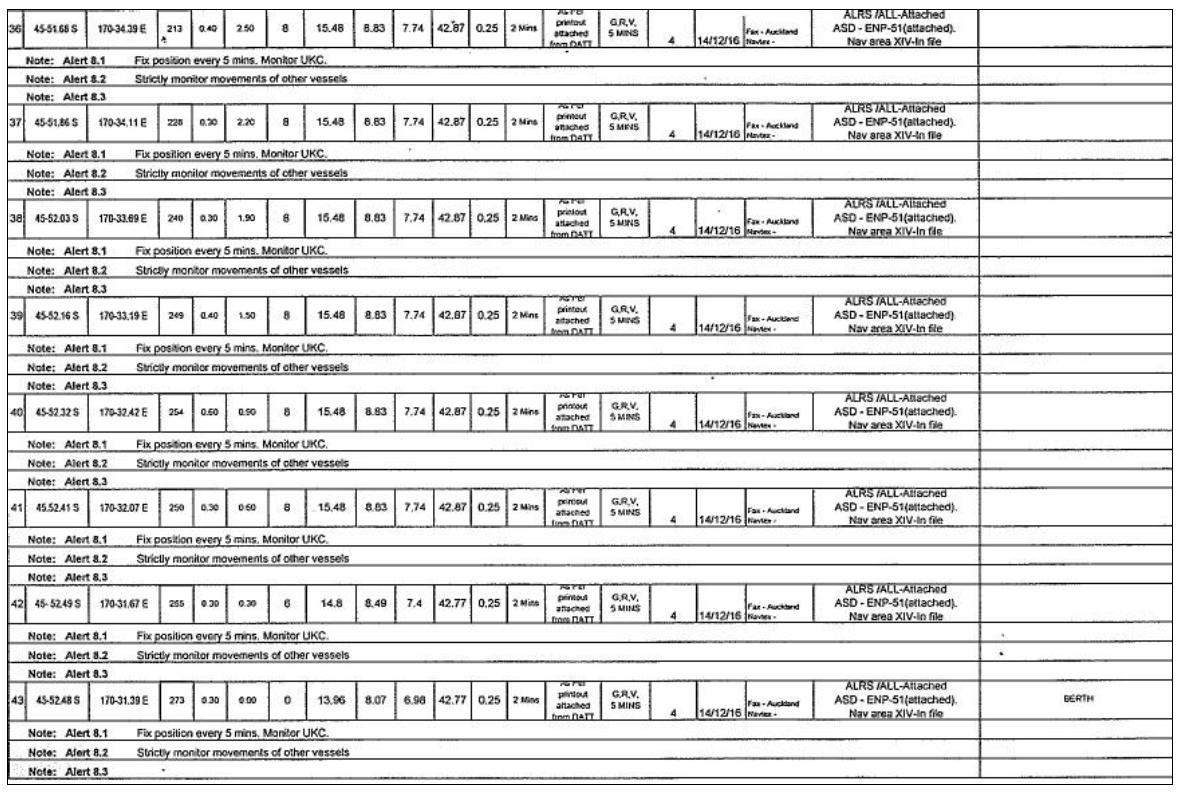
Appendix 4. Relevant parts of the Molly Manx’s passage plan – Otago Harbour
Appendix 5. Excerpts from Anglo-Eastern Ship Management’s shipboard procedures manual
Appendix 6. Extracts from New Zealand Port and Harbour Marine Safety Code