On 27 February 2016, the bulk carrier Mount Hikurangi had just completed loading a cargo of logs at the port of Tauranga. The ship's crew were involved in applying chain lashings to the logs that had been loaded above deck when a deck cadet fell from the stack of logs 10 metres onto the wharf below, then into the sea. The deck cadet did not survive this fall. His body was recovered by divers a number of hours later. The deck cadet was not wearing a safety harness attached to a fall arrestor while working close to the edge of the log stack, despite a company requirement to do so.
Executive summary Tuhinga whakarāpopoto


- On 27 February 2016, the bulk carrier Mount Hikurangi had just completed loading a cargo of logs at the port of Tauranga. The ship’s crew were involved in applying chain lashings to the logs that had been loaded above deck when a deck cadet fell from the stack of logs 10 metres onto the wharf below, then into the sea. The deck cadet did not survive this fall. His body was recovered by divers a number of hours later.
- The deck cadet was not wearing a safety harness attached to a fall arrestor while working close to the edge of the log stack, despite a company requirement to do so.
- The Transport Accident Investigation Commission (Commission) found that the crew on Mount Hikurangi routinely did not follow company procedures by working on top of log cargoes without the required safety harnesses.
- The Commission also found that there was little evidence of a strong safety culture on board Mount Hikurangi at the time.
- The safety actions taken by the ship operator and Maritime New Zealand negated the need for the Commission to make any recommendations.
- Key lessons arising from the inquiry include:
- all crew members must wear safety harnesses, preferably connected to fall arrestors, when working at height
- a strong safety culture must be established and promoted from the highest levels of management on board a ship. It must be encouraged, monitored and enforced throughout all levels of the organisation so that best safety practices are followed.
Factual information Pārongo pono
Background
- At the time of the accident Mount Hikurangi was preparing to carry a cargo of logs on deck.
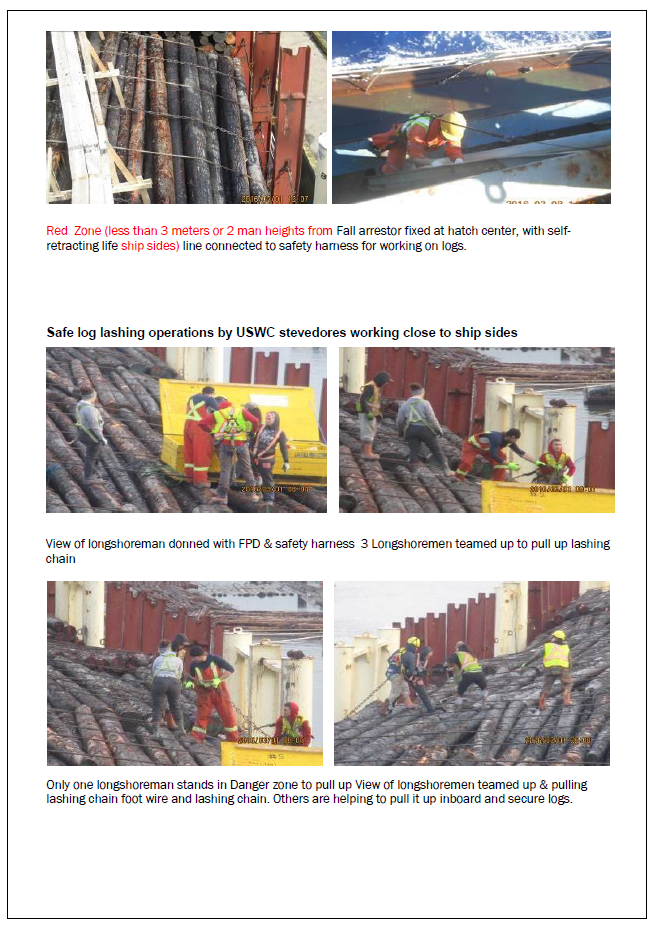
- In preparation for loading, the crew rigged stanchions on both sides of the ship adjacent to all of the hatches, to retain the logs in a block stow. Once the logs were loaded, a series of wire and chain lashings was rigged across the entire stow to secure the logs.
- The procedure for securing log cargo on Mount Hikurangi was laid down in the approved ship’s cargo securing manual.
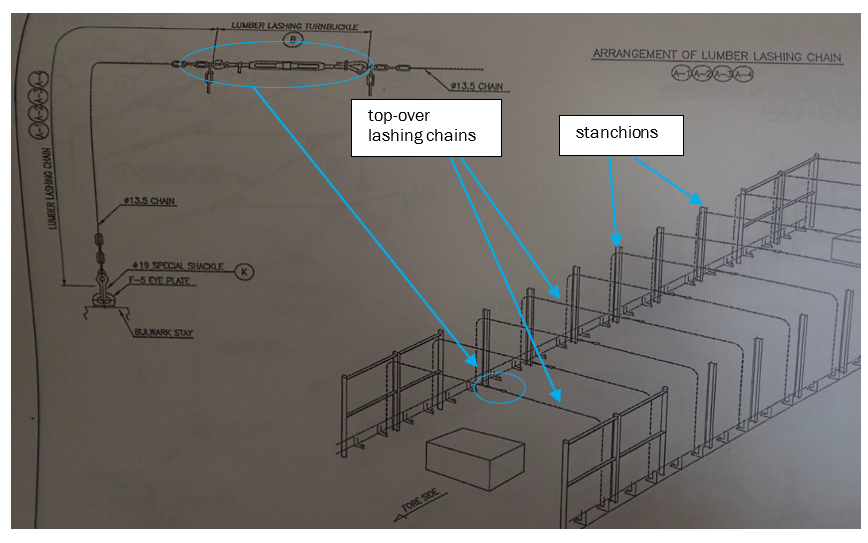
- Chapter 5 of the operator’s Fleet Regulations also laid down the voyage procedure when carrying a cargo of logs. In respect of lashing deck cargo, paragraph 13 of the procedure made reference to the International Maritime Organization’s Timber Code: Code of Safe Practice for Ships Carrying Timber Deck Cargoes 2011 (Timber Code) and the ship’s cargo securing manual. Specifically, it referred to the requirement for rigging lumber lashing chains, also known as top-over lashing chains.
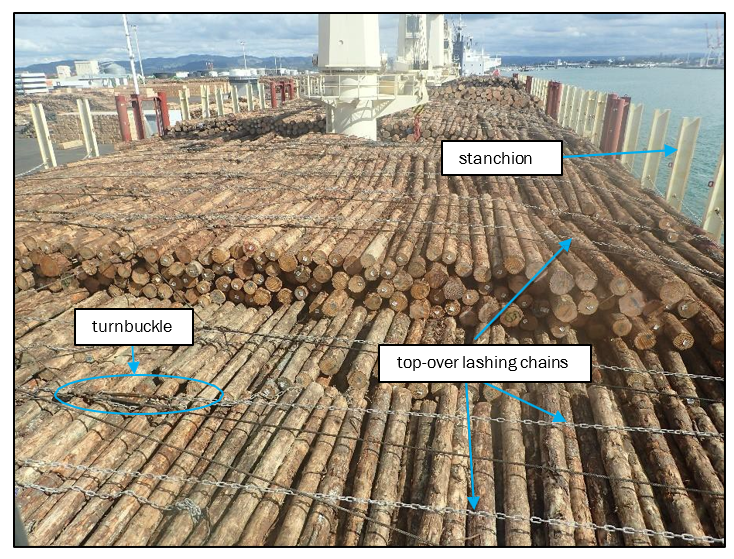
- Each top-over lashing chain was shackled to a deck eye-plate. The other end of the chain had a rope eye attached through the last link. The rope eye was suspended over the top of each stanchion (see Figure 4) so that the chain was easily accessible whilst lashing the logs. At the time of the accident the crew were rigging the chain lashings (see Figures 1 and 2). They used a ship’s crane to haul each chain inboard over the logs.
- One at a time, the port and starboard lashing chains were lifted across the logs by the ship’s crane. They were connected near the centreline with a turnbuckle, which was used to increase the tension in the chains. The tension increased the vertical friction force between the logs at the outer part of the stow and, together with other types of lashing, helped to achieve a secure stow. The final lashing configuration was the same at all hatches (see Figures 1 and 2).
Narrative
- At 1530 on 24 February 2016, the Hong Kong-registered bulk carrier Mount Hikurangi secured portside alongside number nine berth in the port of Tauranga in a ballast (empty) condition.
- At 2015 the vessel commenced loading a full cargo of logs in the cargo holds and on top of the hatch covers as deck cargo. The loading of logs continued for the next three days.
- At about 0600 on 27 February 2016, a ship’s cargo securing team comprising the boatswain (bosun), three able-bodied seamen (AB) one ordinary seaman and a deck cadet were securing the log cargo above number 5 hatch.
- The weather was fine and dry. There had been some rain the previous evening but the surface of the logs was dry at the time of the accident.
- Before the crew commenced work the chief officer briefed them to secure the cargo in accordance with the instructions contained in the cargo securing manual. At the same time, he checked that they were wearing appropriate personal protective equipment (PPE). The cadet was dressed in an overall, safety helmet, high-visibility vest and safety boots fitted with removable pull-over spikes designed for walking on logs. On completion of the briefing the crew commenced securing the log cargo above number 5 hatch.
- At about 0900 on 27 February 2016, all cargo loading operations had been completed. The crew that had secured the log cargo above number 5 hatch commenced securing the log cargo above number 2 hatch, using number 1 crane to haul the chains across the logs (see Figure 3).
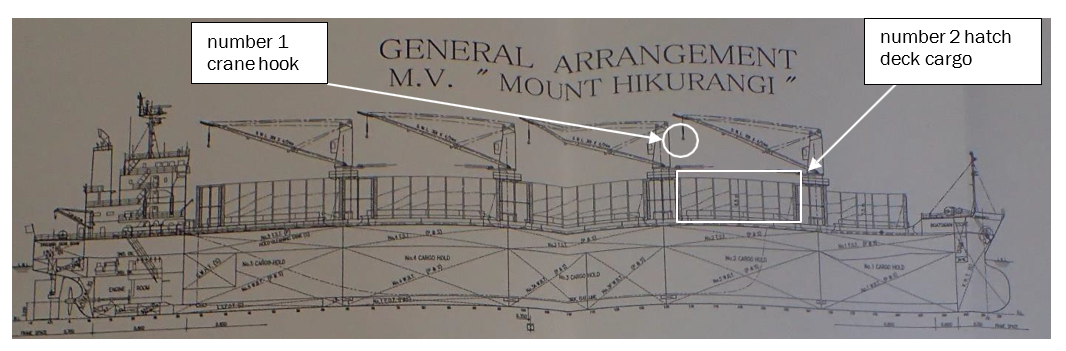
- The crew used a short wire strop and small hook attached to the main crane hook to drag the chains across the logs. The bosun had tasked the deck cadet with hooking each lashing chain on to the small hook (see Figure 4).

- At about 0911 the deck cadet positioned himself adjacent to the aftermost stanchion on the port side of number 2 hatch in preparation for hooking on the lashing chain. He was standing at the edge of the log cargo about eight metres above the ship’s main deck, which was 10 metres above the quay and 12 metres above the waterline. As the lifting hook was lowered in front of him he bent down to hook on the lashing chain, which had been hung over the top of the stanchion with the rope eye (see Figure 4). Once the cadet had hooked the chain on to the lifting hook he stood up and remained next to the stanchion whilst the crane driver hoisted and slewed the crane to drag the chain across the logs, where it was unhooked by the bosun. The crane hook was then returned to the port side to receive the second lashing chain.
- The cadet grabbed the wire and bent down to hook on the second lashing chain. He stood up momentarily before bending down again. About four seconds later, as the main crane hook was being raised, the cadet fell overboard, striking the quay and falling into the water. The bosun raised the alarm on his portable radio.
- The deck lashing crew ran to the ship’s side and the third officer went down to the quayside with a lifebuoy. The master, who was in his cabin at the time, heard the emergency call on his portable radio and went to the port bridge wing. He called the emergency services and the ship’s commercial agent.
- At about 0930 a police patrol boat arrived and commenced searching for the cadet. HMNZS Manawanui was also berthed in Tauranga at the time of the accident. The crew of Manawanui were alerted by the police and responded by providing divers to search for the cadet.
- At about 1150 the divers entered the water and about 10 minutes later they located the cadet’s body.
Experience of the deck cadet
- The deck cadet had commenced employment with Pacific Basin Shipping (HK) Limited on 17 September 2015. He had joined Mount Hikurangi, his first vessel, on 22 September 2015.
- The cadet had completed the joiner’s familiarisation checklist within 48 hours of joining, as required by the operator’s safety management system. This included familiarisation with the permit to work8 system on board in relation to enclosed space procedures, working aloft and hot work.
- The cadet had been involved in loading and discharging logs on four previous occasions.
- Prior to the accident on 27 February, the cadet had rested for 16.5 hours on 26 February and had had six hours of rest on 27 February prior to commencing work at 0600. Fatigue is not considered to have been a contributing factor to the accident.
Hazard identification and risk assessment
- The operator’s Fleet Regulations addressed risk management using the following process:
- assessing operational tasks at all levels for the possibility to cause injury, damage or loss. The ‘Hazard Identification and Risk Assessment’ document on board provided generic risk assessments for onboard operations
- periodic reviews of the document to ensure that any additional hazards and risks in operations on board were identified and discussed before carrying out the operations
- six-monthly formal reviews by the master
- a brief and informal risk assessment prior to “each and every task”. This was described as a “3W” risk assessment where the following questions were posed:
- What can go wrong?
- What factors can cause it to go wrong?
-
What should be done to prevent it going wrong?
There was no requirement to record that the 3W risk assessment had taken place.
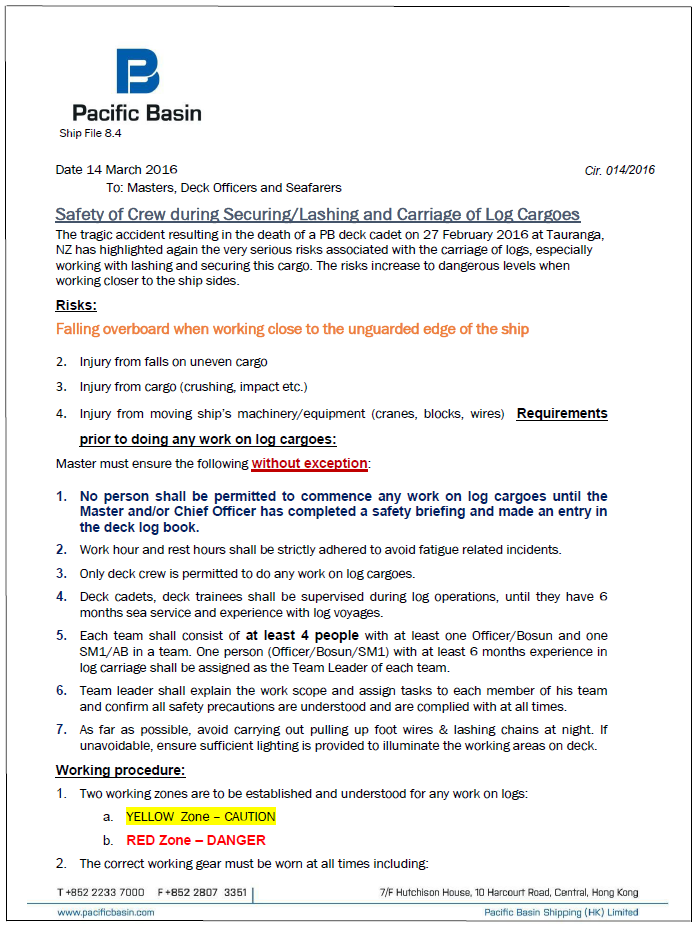
- There was a risk assessment for “working aloft” and “over the side” that did consider falling from height and falling overboard. The control measures included, but were not limited to:
- consideration be given to working under the permit-to-work system (the permit-to-work system is a safety measure whereby seafarers must get written permission from senior officers before they can perform high-risk tasks including, but not limited to, working aloft, welding and entry to enclosed spaces. An operator’s safety management system will identify which activities must be carried out under a permit to work)
- young or inexperienced persons not required to work aloft or over the side unless accompanied by experienced seafarers or under adequate supervision
- all seafarers are required to wear safety harnesses, and safety nets are to be rigged where appropriate.
- A risk assessment and hazard identification had been carried out by the operator for loading logs, but it had not identified falling from height during lashing operations as a hazard.
-
However, the operator’s Fleet Regulations referred to access and the safety of the crew when working on logs. It stated that:
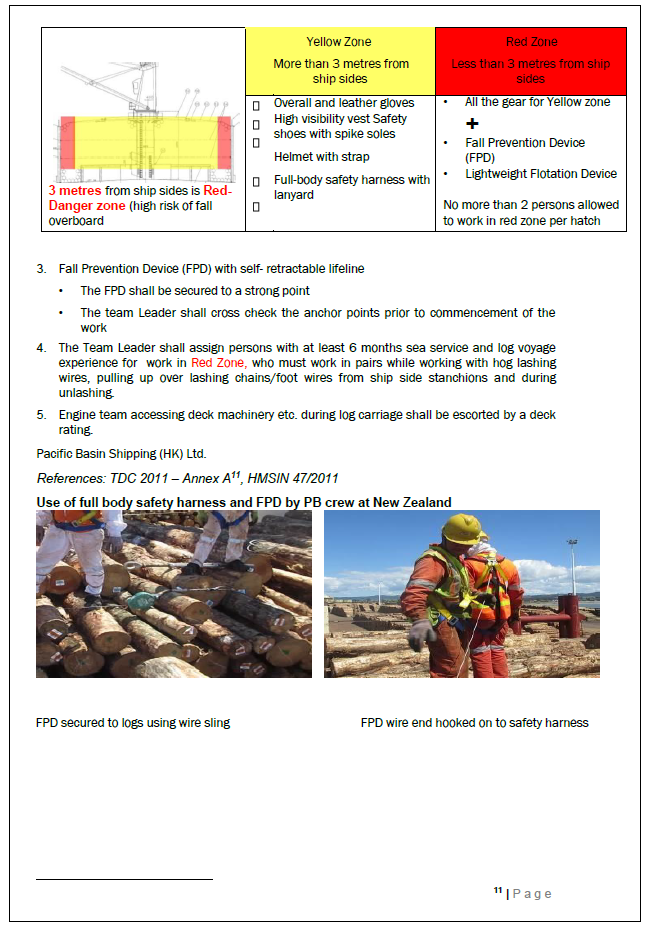
retractable lanyards (fall arrestors), safety harnesses and log spike shoes should form part of the PPE while working on log cargoes. Working on timber deck cargo is a hazardous operation and only the deck crew should be permitted to work on timber deck cargo
-
The Fleet Regulations also required adherence to the International Maritime Organization’s Timber Code. This code included guidance for developing procedures and checklists for the safe loading, carriage and discharge of timber deck cargoes. It stated that:
Personnel working on cargo stowed at heights 2m and above, within 1m of an unguarded edge, should if deemed necessary be protected from falls with fall restraint equipment such as a safety harness or other fall restraining devices approved by the Administration.
-
An entry in the chief officer’s cargo logbook, written on 24 February 2016, included a standing order that:
Anyone on the main deck or logs must be worn (sic) 1. safety helmet 2. safety shoes and spikes 3. Hi-vis vest 4. Safety belt
- The following PPE was available to the crew involved in cargo securing operations:
- boots
- attachable boot spikes (to assist movement when walking on top of logs)
- gloves
- safety helmets
- full-body safety harnesses
-
fall-arrestor devices.
There were 12 safety harnesses and six fall-arrestors on board.
Internal audit
- The operator had carried out an internal audit of Mount Hikurangi about five months before the accident, between 8 and 10 September 2015. In respect of the safety management system the audit identified two non-conformities and seven observations. The senior officers on board Mount Hikurangi at the time of the accident were also on board at the time of the audit.
-
Of the two non-conformities identified by the auditor, non-conformity number 02/2015 required corrective action by:
Regular inspection to be strictly carried out to verify training effectiveness. A special officers meeting held to enhance critical importance of safety practice – not tick box culture.
-
Amongst the recommendations for continual improvement, the auditor recommended that all officers and crew take a positive interest in and adopt a proactive approach to enhancing loss-prevention techniques:
This will help to improve on 3W risk assessment and hazard identification, self-check and taking adequate safety measures to prevent any accident/incidents and personal injury.
The auditor also recommended that the crew be encouraged to carry out risk assessments for both critical and routine jobs.
Appendix 1. Pacific Basin’s risk assessment circular