On 2 July 2015, the container ship Madinah was preparing to arrive at the port of Lyttelton. While rigging the port-side accommodation ladder, the bosun clipped his safety harness to a plastic-coated wire and stepped onto the ladder to lift the handrails into place. The wire broke, and he fell into the sea. Despite immediate rescue efforts and a two-hour search involving several boats and a helicopter, he was never found.
Executive summary Tuhinga whakarāpopoto

- On 2 July 2015 the container ship Madinah was preparing for arrival at the port of Lyttelton. Part of those preparations involved the bosun (deck crew foreman) and a deck trainee rigging the port-side accommodation ladder over the ship’s side in readiness for the ship’s docking.
- Both the bosun and the deck trainee were wearing safety harnesses. The bosun sent the deck trainee to fetch buoyancy vests, which were required to be worn for any task outside the ship’s railing. When the trainee returned the bosun had already swung the accommodation ladder over the side, clipped his safety harness to a plastic-coated wire and walked along the accommodation ladder to try to lift the handrails into place.
- In doing so the bosun lost his balance and fell into the sea. The wire to which he had clipped his safety harness had broken. A crew member on the deck threw a lifebuoy into the water near the bosun. The bosun was last seen swimming towards the lifebuoy.
- The pilot launch that was heading towards the Madinah at the time arrived in the area and started the search. Despite an extensive search using several other small craft and a helicopter for the next two hours, the bosun was never found.
- The Transport Accident Investigation Commission (Commission) found that if the bosun had been wearing a buoyancy vest his chances of surviving would have been significantly greater. It also found that the wire rope to which the bosun had connected his safety harness broke because it was severely corroded and also that it had not been constructed and installed in accordance with best industry practice.
- Two safety issues identified were: there was no dedicated formal procedure for rigging the accommodation ladders and gangways on board; and although the procedures on board for responding to a man overboard met industry best practice, the shipboard response to the emergency did not follow those procedures.
- A third safety issue identified was the use of plastic-coated wire for safety-critical applications. If the plastic coating becomes damaged, salt water can enter and become entrapped in the coating, which causes accelerated corrosion. The plastic coating makes it virtually impossible for the wire to be inspected or surveyed properly. The Commission has raised this issue in a previous inquiry and made recommendations to the Director of Maritime New Zealand to address the issue.
- The vessel’s manager has taken safety action to address other safety issues discussed later in the report. Therefore, the Commission has not made any new recommendations arising from this inquiry.
- Key lessons arising from this inquiry included:
- where it is necessary for a crew member to work over the side of a ship when at sea, they must wear a safety harness attached to a designated strong point and must wear a buoyancy vest
- plastic-coated wires must be treated with caution. Seafarers and surveyors alike must not make assumptions about the condition of any wire that they cannot see, especially when the wire has a safety-critical purpose and is required by rules, regulations or procedures to be examined thoroughly
- a man-overboard situation requires timely and intuitive actions by the crew in order for the rescue to be successful. Crew should follow quick-reference checklists to ensure that: the alarm is raised in the appropriate way; the position of the casualty is recorded and tracked; and the ship is returned to the casualty in the most expeditious way.
Conduct of the inquiry He tikanga rapunga
- The Transport Accident Investigation Commission (Commission) learned of the accident the following day from media reports; opened an inquiry under section 13(1)b of the Transport Accident Investigation Commission Act 1990; and appointed an investigator in charge.
- On 3 July contact was established with the Hong Kong flag administration and agreement was reached that New Zealand would lead the investigation and conduct the investigation on behalf of Hong Kong.
- On 3 July two investigators travelled to Napier, the Madinah’s next port of call. On 4 July the investigators conducted interviews with the crew of the vessel and collected evidence that included a download of the vessel’s voyage data recorder.
- On 16 July one investigator travelled to Lyttelton to interview staff from Lyttelton Port of Christchurch and gather further evidence.
- On 20 July contact was established with the missing seaman’s next of kin.
- Extra information was sourced from Maritime New Zealand, New Zealand Police, the vessel’s manager and the vessel itself.
- On 24 June 2016 the Commission approved the draft report to be circulated to interested persons for comment.
- The report was distributed to nine interested persons on 26 July 2016, with the closing date for receiving submissions as 16 August 2016. Three submissions were received that included comments and five submitters declined to comment
- The Commission has considered in detail all submissions made and any changes as a result of those submissions have been included in the final report
- On 28 September the Commission approved the report for publication.
Factual information Pārongo pono
Narrative
- On 2 July 2015 at around 0700, the Hong Kong-registered container ship Madinah arrived off the port of Lyttelton on the east coast of the South Island of New Zealand after an overnight voyage from Port Chalmers (Dunedin).
- The master was informed that the vessel would not be berthing until early afternoon the same day and chose to let the vessel drift off the port of Lyttelton until the pilot boarding time.
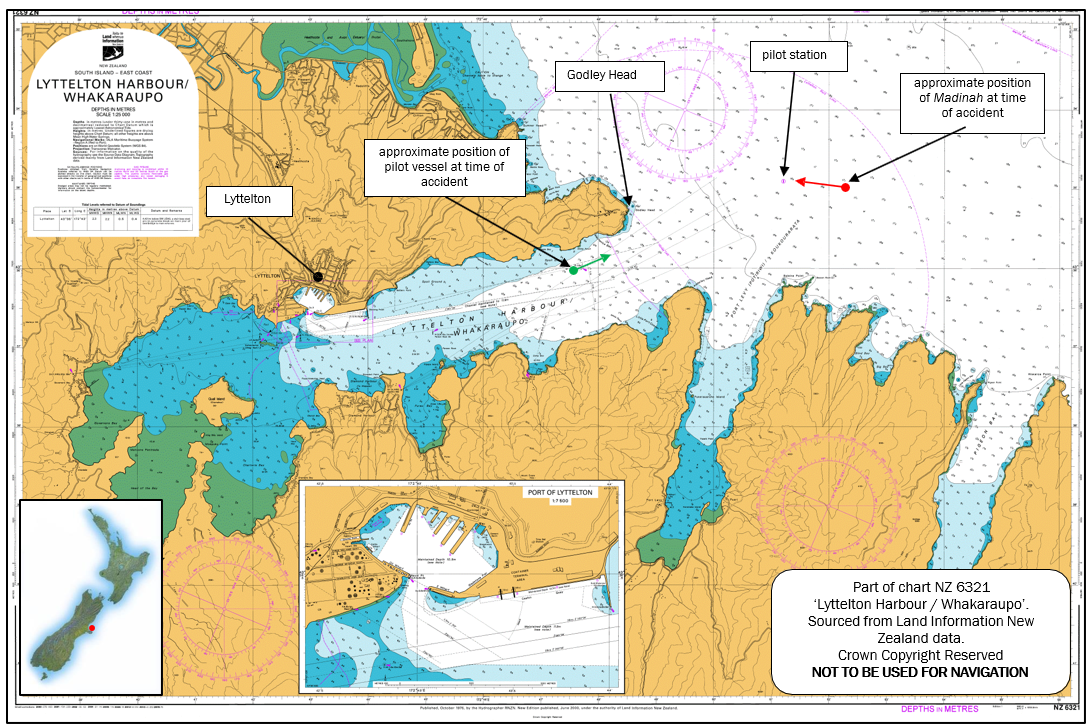
- The crew were engaged in deck maintenance during the morning. At about 1130 the master asked the bosun to rig the port-side combination pilot ladder. The bosun, accompanied by two able-bodied seamen, rigged the combination pilot ladder and made other preparations for the ship’s arrival at Lyttelton. At 1230 the Madinah began the journey towards the pilot station (see Figure 1), the position where the pilot would normally board the vessel. The master and the second officer were on the bridge.
- At the time of the accident the wind was reported to be north-easterly at approximately 10 knots with a north-easterly swell of about one metre. The visibility was good and the tide was flooding.
Events on the main deck
- At about 1300 the master asked for the port accommodation ladder to be rigged before the crew went to their mooring stations. The bosun and the deck trainee proceeded to the port accommodation ladder station. When they arrived the bosun told the deck trainee to get two buoyancy vests from the crew changing room, which was inside the accommodation.
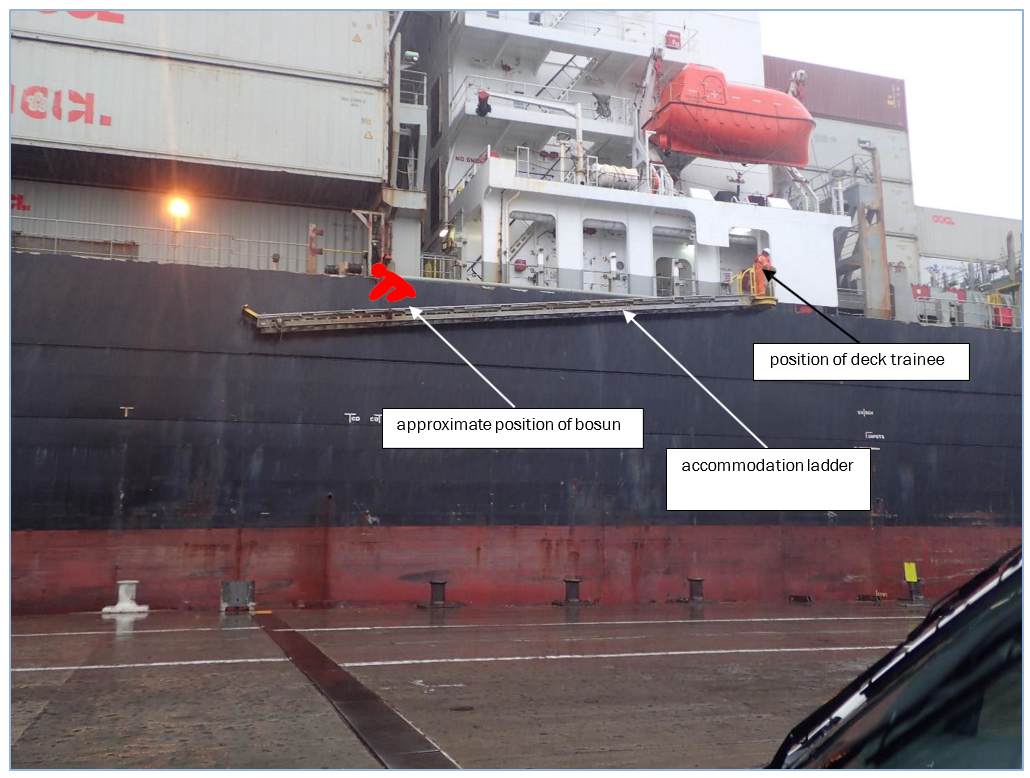
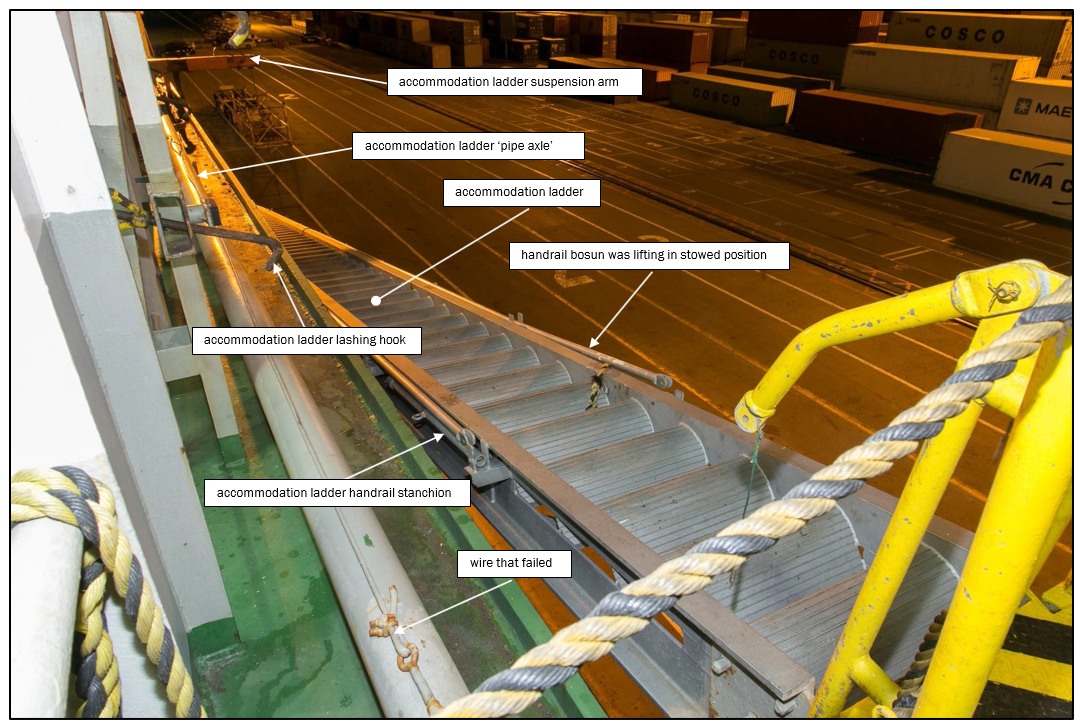
- The deck trainee returned from the changing room wearing his own buoyancy vest and carrying one for the bosun. However, the bosun had already removed the lashings and lowered the accommodation ladder to below the main deck level. The deck trainee stood on the top platform of the accommodation ladder, from where he saw that the bosun had walked more than halfway down it and was crouched down trying to lift the outboard handrail from its stowage position (see Figure 2).
- As the deck trainee watched, the handrail snapped back into its stowage position, causing the bosun to lose his balance and fall into the sea. The bosun was wearing a safety harness connected to a wire, but as his body weight came on the safety harness line the wire parted and the bosun fell into the sea.
- The deck trainee immediately called the bridge on his very-high-frequency (VHF) portable transceiver (a transceiver is a radio that is capable of both transmitting and receiving calls on certain frequencies) and reported that the bosun had fallen overboard. He then ran along the main deck towards the stern to locate a lifebuoy. Meanwhile another crew member who was working near the stern of the ship had heard the commotion and a splash. He grabbed a nearby lifebuoy and threw it overboard. The bosun was seen trying to swim an estimated 10-15 metres to the lifebuoy.
- Those crew members in possession of VHF radios heard the deck trainee’s call and made their way to the deck to assist. The chief officer made his way to the stern of the ship, where he saw the bosun some distance away in the water. He called the master for instructions and was told to stand by at the pilot boarding station. Some time later the chief mate heard on his VHF radio that the Madinah was proceeding to the man-overboard position to assist in the search. He made his way to the bow and sent one of the crew to get binoculars from the bridge to help look for the bosun.
Events on the navigating bridge
- On hearing the VHF radio message from the deck trainee, the master immediately stopped the engine and ordered the helm put hard to port (the side from which the bosun had fallen). Both he and the second officer made their way to the port bridge wing from where they saw the bosun in the water. The master saw that a lifebuoy had been thrown towards the bosun, so he decided not to release the man-overboard lifebuoy (a man-overboard lifebuoy is a dedicated man-overboard lifebuoy that rests in a quick-release cradle (one on each navigation bridge wing) and has a smoke signal and a light that both activate when the lifebuoy is released) from the port bridge wing.
- The second officer telephoned the third officer and asked him to commence preparing the vessel’s rescue boat (one of a vessel’s survival craft specially designated, under the International Maritime Organization’s International Convention for the Safety of Life at Sea, with certain design features to expedite the launching, recovery and handling of injured persons). The second officer then contacted the Lyttelton port control on VHF channel 12 and advised them that they had a man overboard. The call was answered by one of two pilots who were on board the pilot vessel en-route to meet the ship at the pilot boarding ground. He advised that the pilot vessel would be there as soon as possible to assist.
- At about 1316 the master called the pilot and asked whether he should turn the Madinah around and return to the man-overboard position or wait for the pilot vessel. A pilot on board the pilot vessel replied that it was probably best to wait for the pilot vessel before turning. At that time the pilot vessel was about seven minutes from the Madinah.
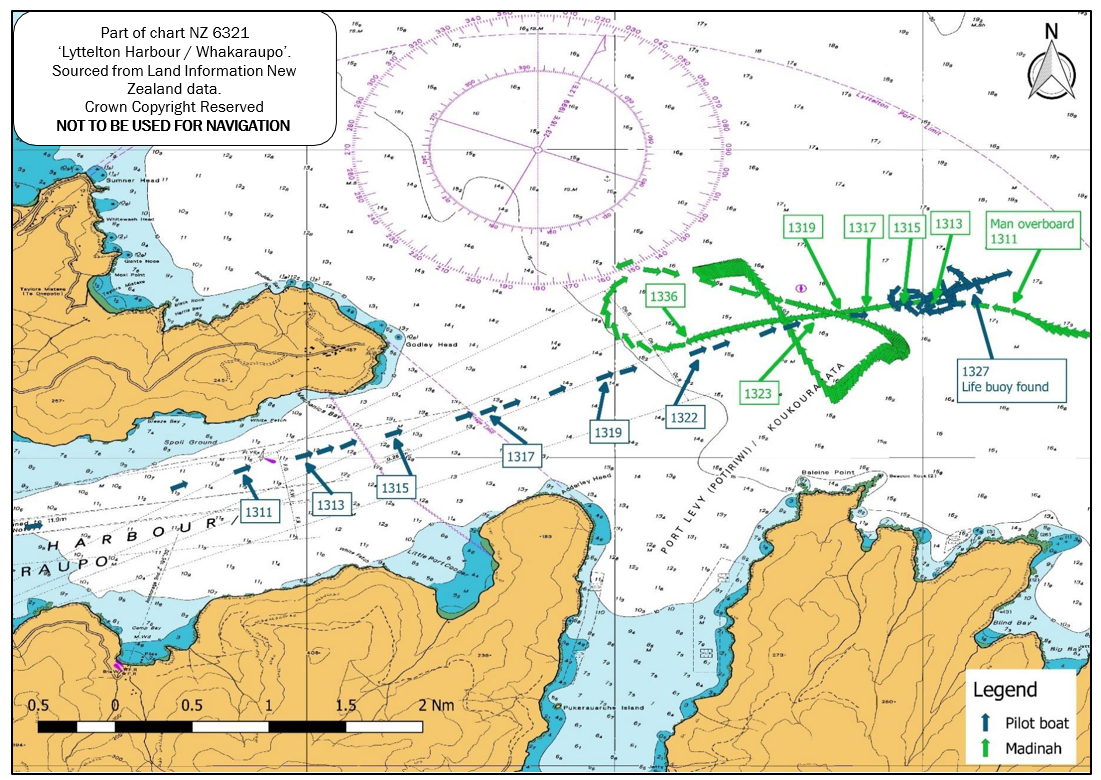
- At 1336 the pilot vessel requested that the Madinah return to the man-overboard position. The master turned the vessel around and returned to the general area of the man-overboard position. At about 1342, as the Madinah was returning to the man-overboard position, the third officer reported that both lifeboats were unlashed and ready to be lowered.
- At about 1354 the master ordered a crew muster and head count, after which all available crew were distributed around the vessel’s decks to assist in searching for the bosun. Once the vessel had returned to the approximate position of the man overboard, the master maintained the vessel in this position while the other smaller vessels that had responded to the call conducted the search.
Events on the pilot vessel
- When the pilot vessel received the call from the Madinah it was approximately 3.6 nautical miles from the ship. The pilot estimated that it would take them 12 minutes to get to the man-overboard position.
- One of the pilots advised port control of the situation and requested that they inform the Coastguard and the ‘Westpac rescue’ helicopter and ask other vessels to assist. Port control also informed the Police and the harbourmaster of the emergency.
- On the way to the accident site the crew of the pilot vessel were unable to locate the lifebuoy or the bosun, so they asked the Madinah to direct them. The Madinah’s crew had kept the lifebuoy and bosun in sight for as long as possible, but by the time they were asked by the crew of the pilot vessel for guidance they had lost sight of the bosun and the lifebuoy and were only able to direct the pilot vessel to an approximate area. At about 1333, about 20 minutes after the bosun had been lost overboard, they found a hard hat and a pair of working gloves belonging to him.
- A pilot requested Lyttelton Harbour Radio to provide more assistance. A fishing vessel, two port tugs, two coastguard vessels, several workboats from Lyttelton and a fast rescue boat from an anchored tanker responded and a grid search was initiated. The rescue helicopter arrived at the scene and started to conduct an expanding circle search. The outbound container vessel stopped to the north of the search area and provided a static search platform using its increased height of eye.
- At about 1449 the control of the search was handed to the New Zealand Police search and rescue co-ordinator.
- At about 1523 the outbound container ship was stood down from the search. At about 1540 the helicopter was stood down, and the search was suspended at 1618 due to failing light and weather conditions. The pilots then boarded the Madinah and brought the vessel into Lyttelton port.
- The bosun has not been found.
Analysis Tātaritanga
Introduction to the issues
- Preparing an accommodation ladder for use is a routine task carried out many times a day across the world on vessels of all sizes. It is not unusual for a crew to prepare the accommodation ladder before a ship arrives at the dock. This requires them to work outside the rail (often referred to as ‘over the side’). Having crew members work over the side is a risk that has been widely recognised by the industry for many decades.
-
In 2014 the United Kingdom P&I Club8 issued Technical Bulletin Number 42/2014, which stated:
The UK Club’s claims statistics show that many serious injuries (or deaths) are caused by falls from gangways or embarkation ladders. The Club’s risk assessors frequently visit ships where these are badly rigged, in a poor condition or witness dangerous working practices. Many accidents occur during the rigging of the gangway. The process of rigging the stanchions and the side ropes is inherently dangerous as there can be little for crew members to hold on to until this is completed. Crew should always wear a safety harness and lifejacket during this operation. Securing of the safety harness line can sometimes be difficult as there can be little to clip on to and movement can be restricted by the length of the harness line.
- The following analysis discusses the circumstances of what happened in this case. It also discusses the following issues:
- The lack of a consistent procedure for rigging an accommodation ladder while still at sea
- The design and failure of the wire that the bosun had connected his safety harness to
- The shipboard emergency response to the bosun falling into the sea
What happened
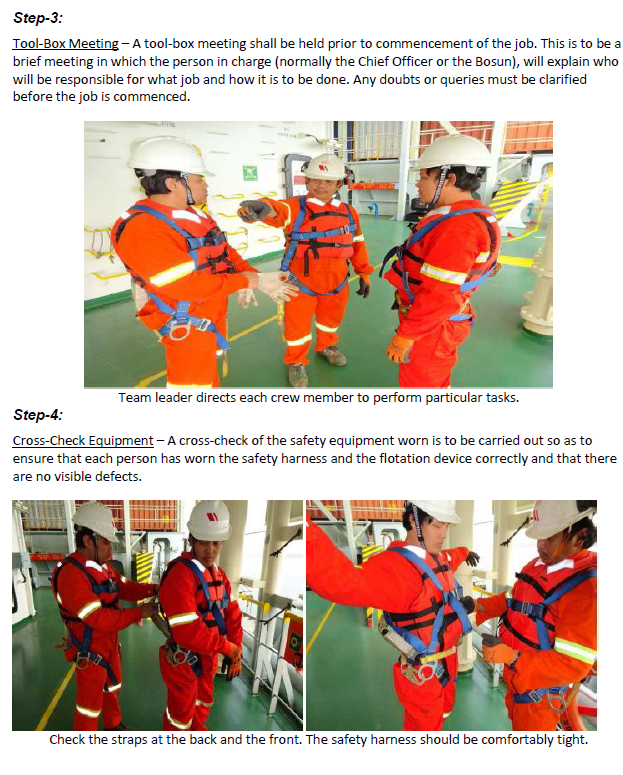
- When the bosun and the deck trainee went to prepare the accommodation ladder the bosun was aware of the need for the correct personal protective equipment. Both he and the deck trainee were wearing their safety harnesses, and he had sent the deck trainee to retrieve their buoyancy vests from the crew changing room.
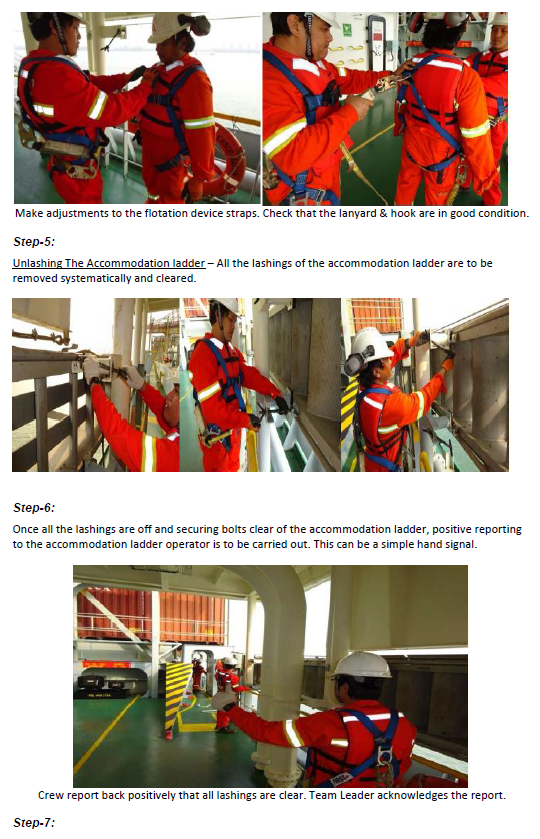
- While the deck trainee went to collect the buoyancy vests, the bosun started unlashing the accommodation ladder, swinging it out and lowering it to a level where the handrails could be rigged. This part of the operation could be accomplished safely from the vessel’s deck because it did not require him to go over the side.
- However, he then walked out onto the accommodation ladder, connected his safety harness onto the plastic-coated wire rope and attempted to rig the handrails without waiting for the deck trainee to return with the buoyancy vests.
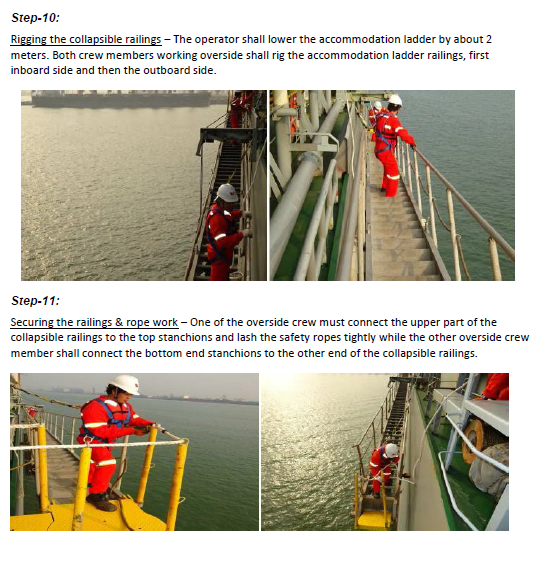
- Rigging the handrails was usually a two-man operation. The handrails comprise a long aluminium pipe supported by pivoting stanchions along its length. The geometry of the handrail is such that when one end is lifted it tends to cause the other end to “dig in”. Normal practice on board was to use two crew members to raise both ends simultaneously. Lifting the hand rail from the middle causes both ends to “dig in” and results in the handrail snapping back down, in this case with sufficient force to cause the bosun to lose his balance and fall off the accommodation ladder.
- It is unclear why the bosun walked out onto the accommodation ladder without waiting for the deck trainee to return with his buoyancy vest. He possibly felt secure in the fact that he was wearing a safety harness and would not therefore fall into the sea. However, the wire he clipped on to was not of sufficient strength to arrest his fall.
- According to studies of ‘human factors’, individual actions can be classified in several ways; in 1990 James Reason proposed some distinctions that have become widely accepted. Firstly, he made an important distinction between two broad groups of individual actions that increase risk (Walker, 2004).
-
Errors: those occasions in which an individual’s planned sequence of mental or physical activities fails to achieve their intended outcomes, and when these failures cannot be attributed to the intervention of some chance agency (Reason, 1990).
-
Violations: deliberate deviations from an organisation’s safety procedures drawn up for the safe or efficient operation and maintenance of plant or equipment (Health and Safety Executive, 1995).
- In this case the non-wearing of a personal flotation device appeared to be an exceptional violation. Exceptional violations appear as isolated departures from authority, not necessarily indicative of individuals’ typical behaviour patterns or condoned by management (Reason, 1990). They are not considered exceptional because of their extreme nature; rather they are considered exceptional because they are neither typical of the individuals nor condoned by authority. What makes exceptional violations particularly difficult for an organisation to deal with is that they are not indicative of individuals’ behavioural repertoire and, as such, are particularly difficult to predict. Usually when individuals are confronted with evidence of their behaviour and asked to explain it, they are left with little explanation (Shappell & Wiegmann, 2000).
Failure of the wire to arrest the bosun’s fall
- The wire to which the bosun attached his safety harness was plastic coated. It was rigged between two eye bolts that had been fitted to the accommodation ladder suspension arrangement (see Figures 4 and 5).
- There was no record on board the Madinah of when and who had fitted the eye bolts. Each of the four accommodation ladders (one either side of the accommodation and one either side at the pilot boarding station on the main deck) fitted on the Madinah had been similarly modified. However, only the port-side accommodation ladder had a wire strung between the eye bolts.
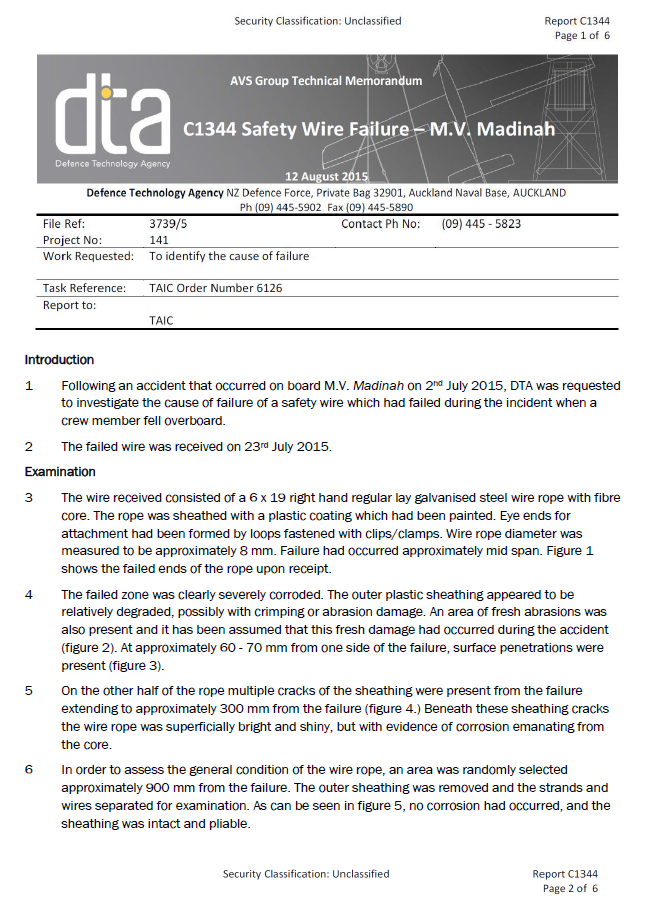
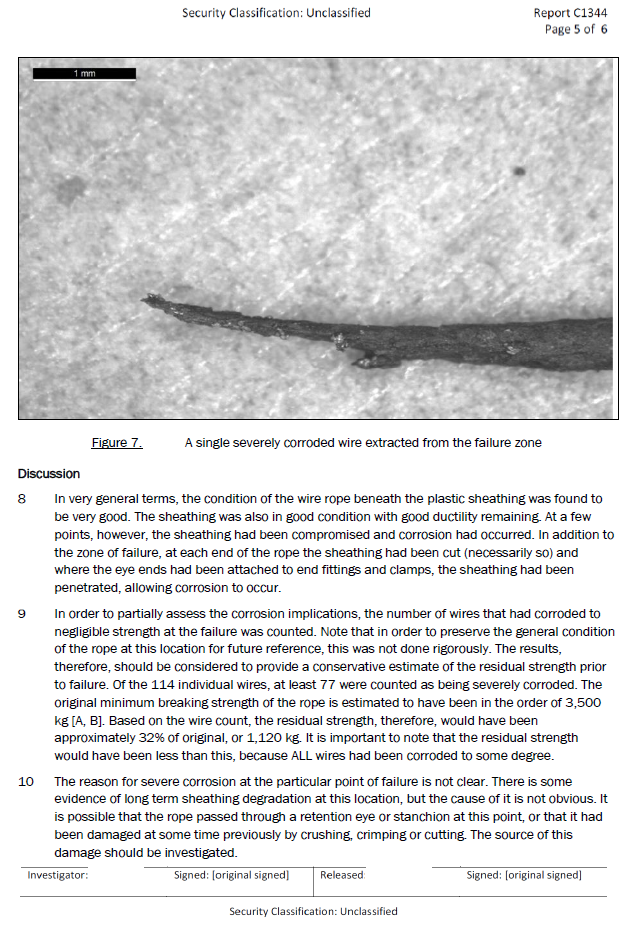
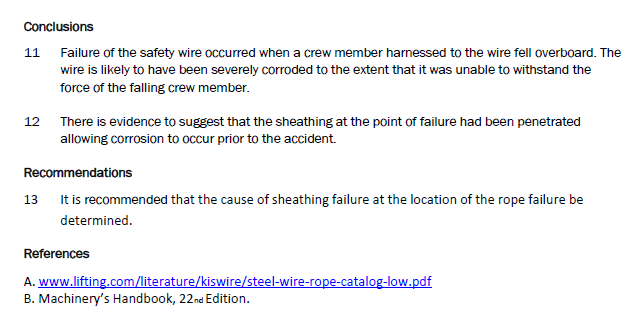
- This wire was removed from the vessel after the accident and sent for examination and testing by an independent contractor engaged by the Commission. The independent contractor reported that the “wire rope was a 6 x 19 right hand regular lay galvanised steel wire rope with fibre core of approximately 8 mm diameter. The rope was sheathed with a plastic coating which had been painted. The original minimum breaking strength of the rope is estimated to have been in the order of 3,500 kg” (see Appendix 1).
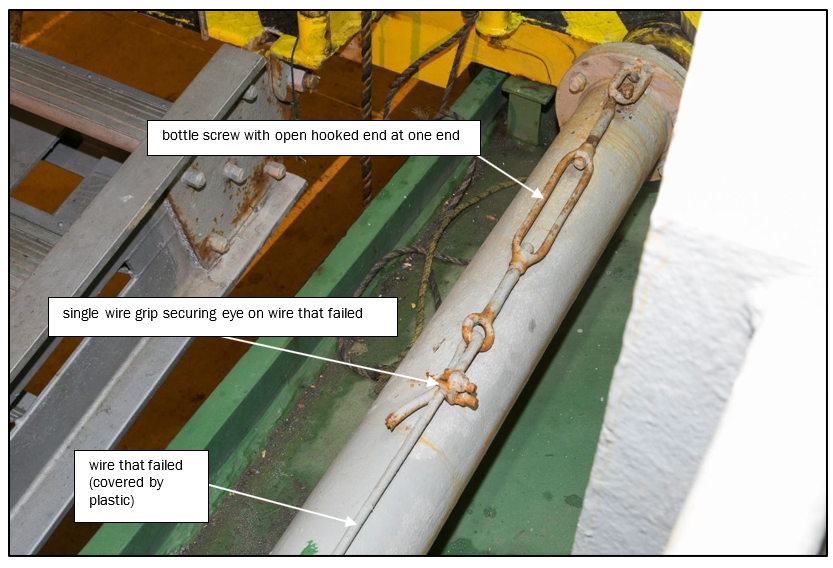
- A soft eye had been formed at each end of the wire rope using a single wire grip. At the forward end of the wire rope the soft eye had been formed through the eye of a bottle-screw or turnbuckle, which was in turn hooked over the eye bolt (see Figure 5).
- There was no record on board the Madinah to show when the wire had been fitted. The wire was not entered into the planned maintenance system or wire rope register. Therefore there was no record of it ever having been examined, maintained or tested.
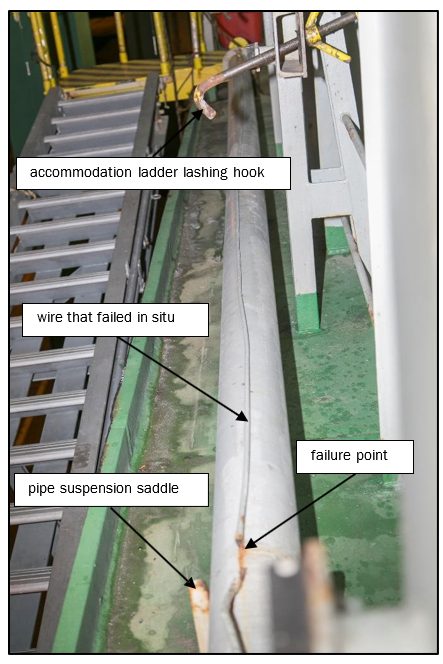
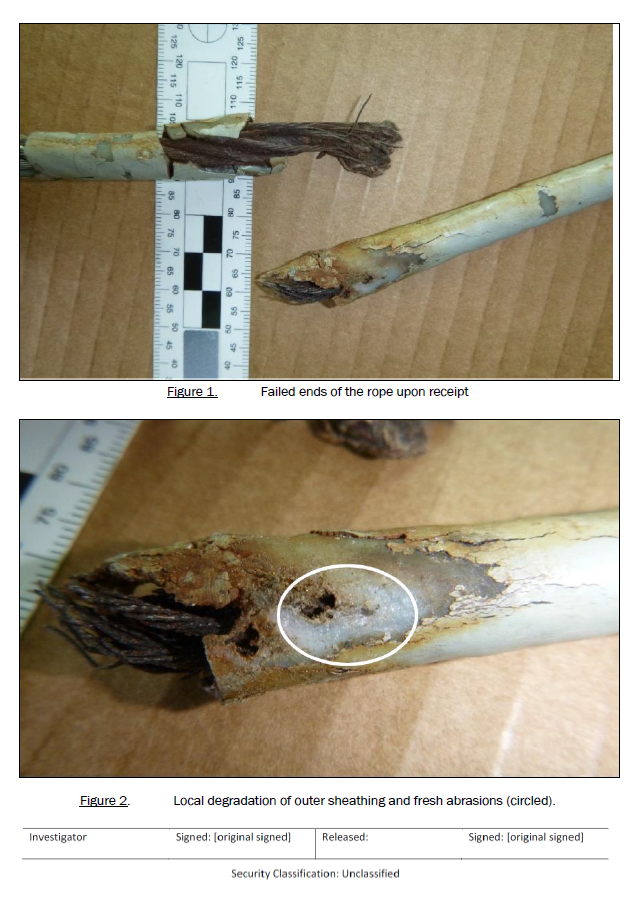
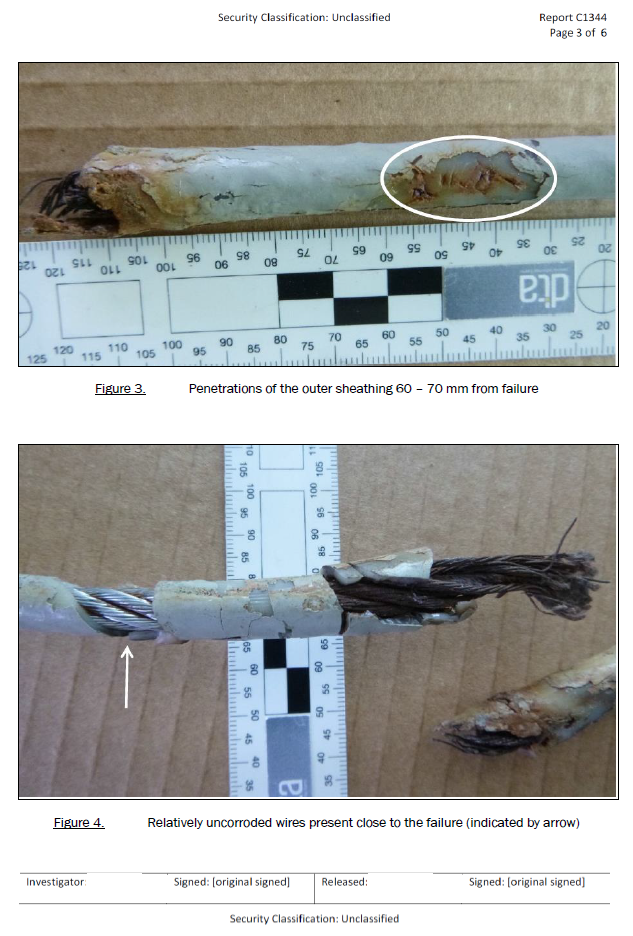
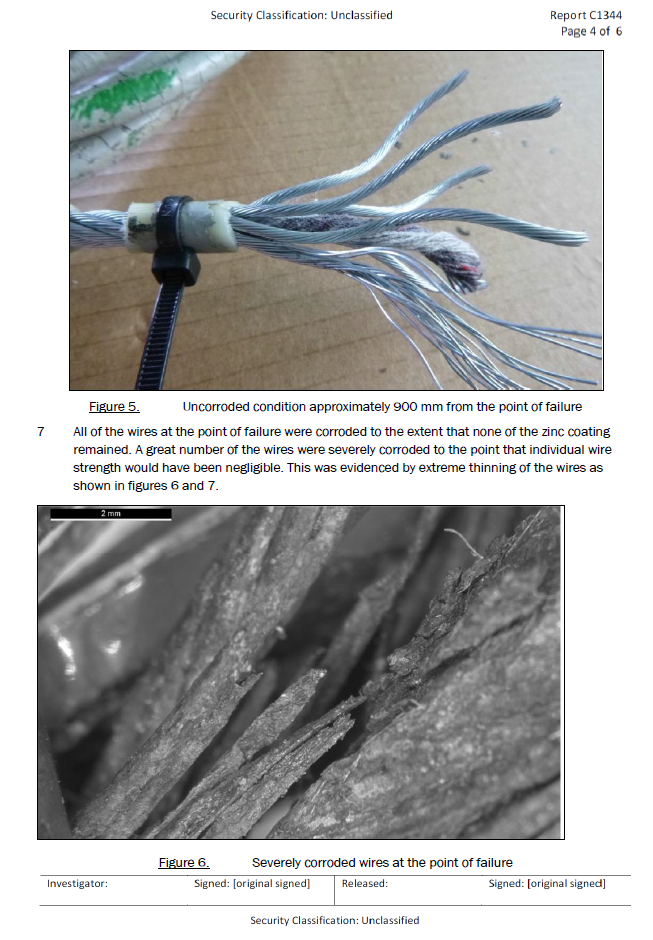
- The point where the wire failed was severely corroded. There were holes in the plastic sheathing in the area of the failure (see Appendix 1). This had allowed water to penetrate through the sheathing and corrosion to form.
- An expert on ropes, chains and fittings (Bridon International Limited) stated that best practice was not to use plastic-covered wire rope when wire grips were to be used. It further stated that to attain an 80% of rope minimum breaking load for an eight-millimetre-diameter wire rope, a minimum of three wire grips should be used. The method used for forming the eyes at each end of the wire rope did not therefore comply with industry best practice. Even though the eyes were not the part of the wire that failed, this lack of best practice was of concern.
- It is about as likely as not that the wire rope was originally intended to be used as a safety lifeline. There was no other logical reason for it being fitted. If this was the case a safety lifeline, which is critical equipment, should have been constructed to industry best practice and regularly maintained. The complete assembly, including the attachment points, should have been assessed for adequate strength and made up of permanent components. The use of an open hook on the bottle screw was another potential point of failure.
- The use of plastic-coated wire for any rigging that is required to be inspected frequently is unsafe. The Commission has raised this issue in another report involving the failure of a plastic-coated wire sling used for launching and retrieving a lifeboat (MO-2014-202 Lifting sling failure on freefall lifeboat, general cargo ship Da Dan Xia, Wellington, 14 April 2014).
- Encasing steel wire in plastic sheathing when it is to be used in the marine environment has significant implications for maritime safety, especially when the wire must be regularly inspected and maintained in order to remain fit for purpose.

- Arising from that report the Commission recommended that the Director of Maritime New Zealand submit the report to the International Maritime Organization (IMO) and raise the implications that plastic-sheathed wire ropes have for maritime safety through the appropriate IMO safety committee for its consideration (recommendation 002/15). Maritime New Zealand accepted the recommendation and submitted the report to the Ship Systems and Equipment subcommittee of the IMO on 16 March 2016 as document SSE.3/INF.4. This document was considered and noted by the subcommittee and the information will be available for future reference.
- This report will also be submitted to the IMO Casualty and Statistics working group as further evidence of the need for action to address the safety issue of plastic-coated wires in the maritime environment.
Procedures
- At the time of the accident there was no dedicated procedure for rigging an accommodation ladder on board the ship. As part of its international safety management system the company had procedures in place for personnel working aloft and over the side of the vessel. The procedure required a risk assessment to be made before a permit to work could be issued and the work be undertaken (see Appendix 3).
- However, this procedure would normally have been used for special or one-off tasks. It would have been highly unusual for a safety management system to require a permit for a routine task of rigging an accommodation ladder, particularly when a permanent procedure could easily be introduced.
- When the crew were interviewed it was apparent that there was a normally followed practice of using safety harnesses and buoyancy vests while rigging the accommodation ladder. However, there were some variances in the methods used that created some risk as described in the following paragraphs.
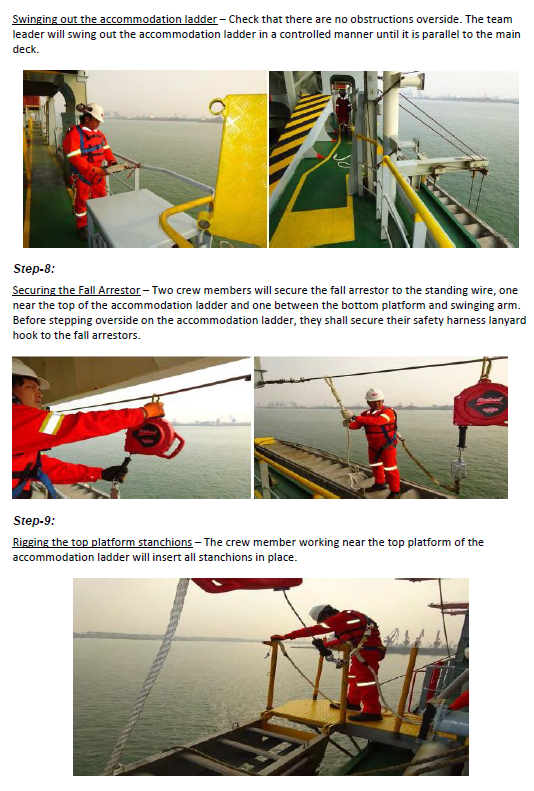
- At each end of the accommodation ladder a gantline had been attached to a dedicated strong point, which allowed the crew rigging the accommodation ladder a certain amount of free movement along the length of the ladder when their safety harnesses were attached to it. The vessel had also been supplied with two fall-arrester devices, which could be attached to dedicated strong points on the vessel to further assist the crew when rigging the accommodation ladder. For the most part the crew used this satisfactory arrangement but occasionally they connected their safety harnesses directly to the ship’s handrails instead.
- It is an unsafe practice to use a vessel’s handrails as an anchor point for safety harnesses, because the material condition and strength of the rails are unknown. They are often only lightly welded and would not provide sufficient guaranteed strength to withstand the load of a falling person.
- The bosun did not use either of these arrangements when he went over the side onto the accommodation ladder. Instead he clipped his safety harness onto the wire that had been strung between two eyebolts fitted to the pipe-axle.
- Crew members who usually rigged the accommodation ladder were aware of the wire rope between the eye bolts, but did not use it as they considered it unsafe due to its appearance.
- A proper risk assessment for rigging an accommodation ladder would have identified the necessary strong points to which to attach the fall arresters. Once these strong points had been included in a procedure any other practice, including clipping on to the handrails and any use of the wire that failed would have been a departure from the standard procedure.
- Having rules, regulations and guidelines does not in itself ensure compliance, nor does simply repeating the rules and regulations in on-board documentation. The responsibility for ensuring compliance with legislation and company operating procedures rests firstly with the ship owner or operating company, then with senior staff on board who have the responsibility for ensuring crew compliance. It is this chain of responsibility that is espoused in the International Safety Management Code, and if the chain is broken in some way the crew who are most likely to encounter a local hazard or threat are at higher risk of having an accident.
- In this case the vessel’s managing company had not conducted a risk assessment and had not developed a formal procedure for rigging any of the four accommodation ladders on board the Madinah, and neither had the senior on-board management or the crew who were performing the task. Having a standard procedure for rigging an accommodation ladder while the ship was at sea might not have necessarily prevented this accident, for the reason given above. However, by not having one there was a heightened risk of such an accident occurring.
Search and rescue
- Losing someone overboard from a ship is a long-recognised and well documented risk associated with any maritime activity. IMO and the International Chamber of Shipping provided standard procedures to ensure the best and consistent method of responding to a person lost overboard. These procedures were incorporated in the Madinah’s safety management system, but the crew did not follow all of them. It is difficult to say whether the bosun could have been saved if the correct procedures had been followed. Regardless of that question, it is a key lesson for mariners that man-overboard procedures ought to be well practised and followed because in other circumstances they could make the difference between life and death.
-
The IMO International Convention on Standards for Training, Certification and Watchkeeping, 1995 revision, required that seafarers be provided with “familiarization training” and “basic safety training” as shown below
Section A-VI/1
Mandatory minimum requirements for safety familiarization, basic training and instruction for all seafarers.
Safety familiarization training:
1.Before being assigned to shipboard duties, all persons employed or engaged on a seagoing ship, other than passengers, shall receive approved familiarization training in personal survival techniques or receive sufficient information and instruction, taking account of the guidance given in part B, to be able to:
1.communicate with other persons on board on elementary safety matters and understand safety information symbols, signs and alarm signals;
2.know what to do if:
a person falls overboard, …
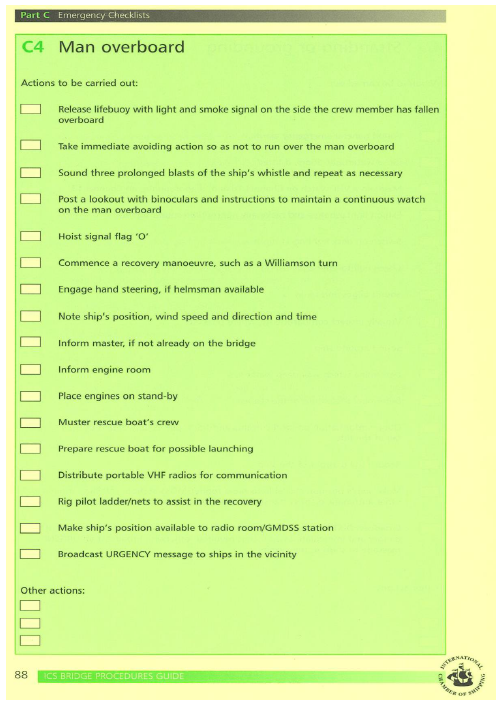
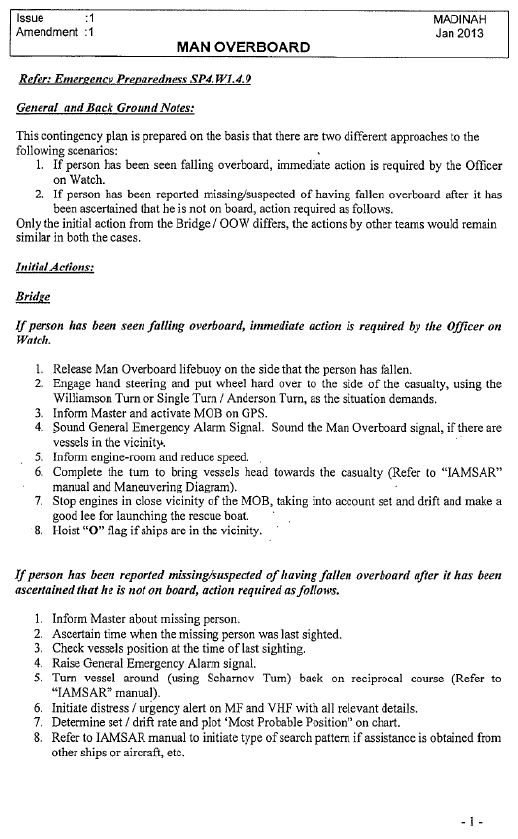
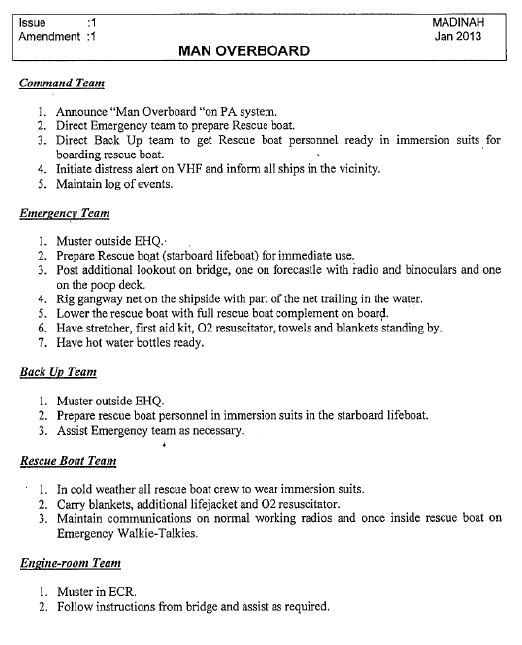
- The vessel’s manager had a man-overboard procedure as part of its safety management system (see Appendix 2), which gave clear instructions on the procedure to be followed in the event of a man overboard. The procedure paraphrased the details outlined in the International Chamber of Shipping’s Bridge Procedures Guide, Part C Emergency Checklists, C4 man overboard (see Appendix 5).
- The International Convention for the Safety of Life at Sea requires crews of vessels to conduct Fire, Abandon Ship and other emergency drills at regular intervals. The most recent man-overboard drill on board the Madinah had been held on 20 May 2015 (about six weeks before this accident) and prior to that on 17 February 2015.
- The proper man-overboard procedures outlined in the appendices to this report are based on the premise of immediate, intuitive actions to: raise the alarm; record the position of the event; return the ship to the scene as soon as possible; and render assistance.
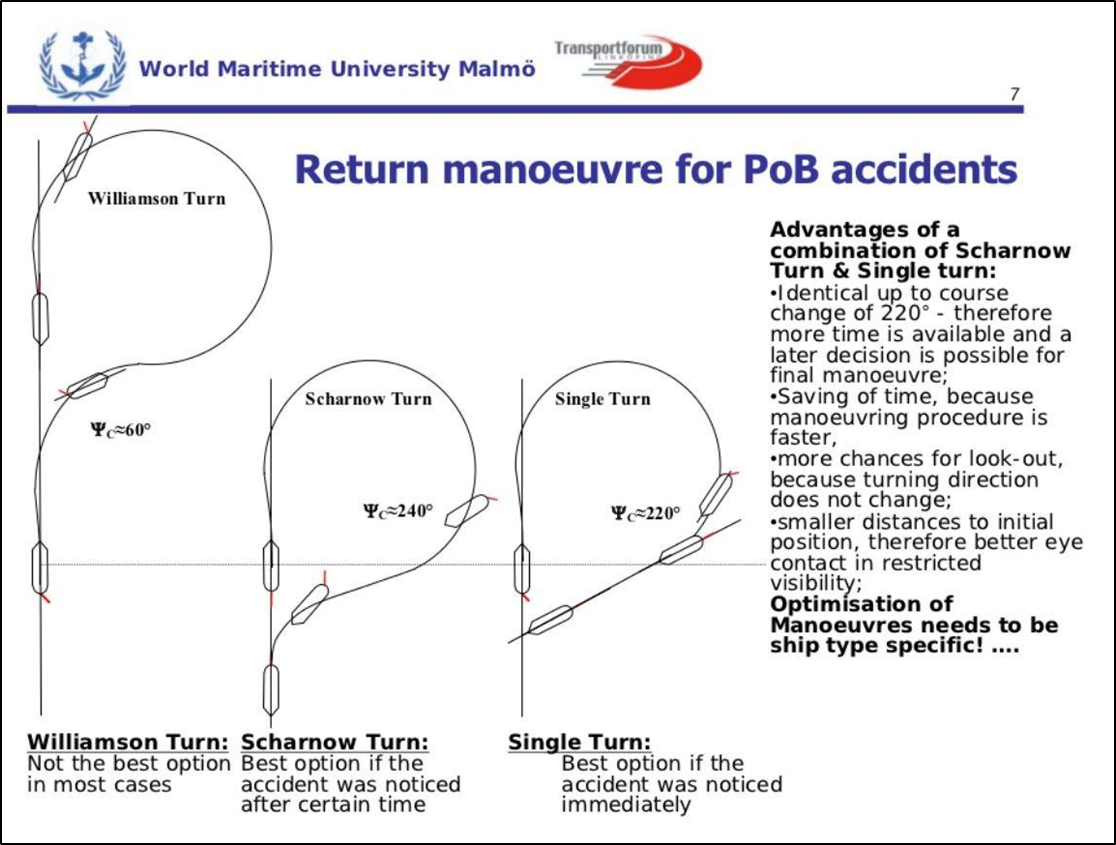
- The immediate and intuitive actions for a man-overboard scenario (see Appendix 5) would be to: commence a recovery manoeuvre (see Figure 8); note the ship’s position; release a lifebuoy with a light and smoke signal; sound the appropriate sound signal on the vessel’s whistle; sound the general alarm; and post lookouts with binoculars to maintain a continuous watch on the man overboard.
- The actions of the Madinah’s bridge team were not intuitive. They did not: note the ship’s position; release a lifebuoy with a light and smoke signal; sound the appropriate signal on the ship’s whistle; or sound the general alarm. Instead of immediately manoeuvring the vessel to return to the man-overboard position the master asked the pilot on the pilot boat whether he should start a Williamson turn. At this point the Madinah was still close to the man-overboard position and had sufficient room and depth of water to return to the man-overboard position relatively quickly.
- Acknowledging that the Madinah was at that moment proceeding to the pilot station and co-ordinating with the pilot for boarding, once the man overboard occurred this should have taken precedence and the focus of the master and crew should have turned to responding immediately to the emergency.
- Had the Madinah transmitted a distress call on the international distress and calling VHF frequency, channel 16, it would have alerted all the vessels and radio stations in the vicinity, including the pilot vessel, of the need for assistance and provided the necessary positional information.
- In this case the most effective means of raising the alarm on board the ship, sounding the general alarm, was not used. Consequently, not all of the crew were available to help manage the recovery. Instead of broadcasting the alarm externally over the dedicated emergency distress radio channel, the master was engaging directly with the pilot vessel. Eventually the situation was escalated to involve all of the available external resources. However, time was lost.
- The position where the bosun went overboard was not well marked or recorded. Consequently, the searching vessels had difficulty locating the correct search area. Again, potentially valuable time was lost.
- In such cases it is good seafaring practice for the ship to return immediately to the position of the man overboard. The ship has the means to do so, has the best information, and has the high search platform better suited to searching for small people in the water.
- This accident highlights the importance of having an effective emergency response checklist to prompt the correct procedures to follow in a high-workload situation, and the efficacy of using the checklist.
Appendix 1. Report on status of failed wire
Appendix 2. Madinah, man-overboard procedure
Appendix 3. Madinah, working aloft – overside permit
Appendix 4. Madinah, procedure for safe rigging of accommodation ladders/accommodation ladders

Appendix 5. International Chamber of Shipping’s Bridge Procedures Guide (Third edition), Part C Emergency Checklists, C4 man overboard