Fatal helicopter crash. An Airbus AS350 B3e helicopter ZK-ITD was being flown from the operator’s base in Milton to a client’s cherry orchard near Alexandra to conduct frost protection operations. The helicopter conducted a series of turns immediately before, and after, reaching the township of Lawrence. Soon after, the helicopter made a descending right-hand turn through nearly 160 degrees before entering a left-hand spiral dive that ended in a near vertical nose-down impact with the ground. The helicopter was destroyed and the pilot (the sole occupant) did not survive.
Executive summary

(Credit: Lister Helicopters Limited)

What happened
- On Thursday 16 September 2021, an Airbus AS350 B3e helicopter, ZK-ITD, was being flown from the operator’s base in Milton to a client’s cherry orchard near Alexandra to conduct frost protection operations.
- The flight departed approximately one hour before the beginning of morning civil twilight (when the centre of the rising sun’s disc is 6° below the horizon). It proceeded normally until just before reaching the township of Lawrence.
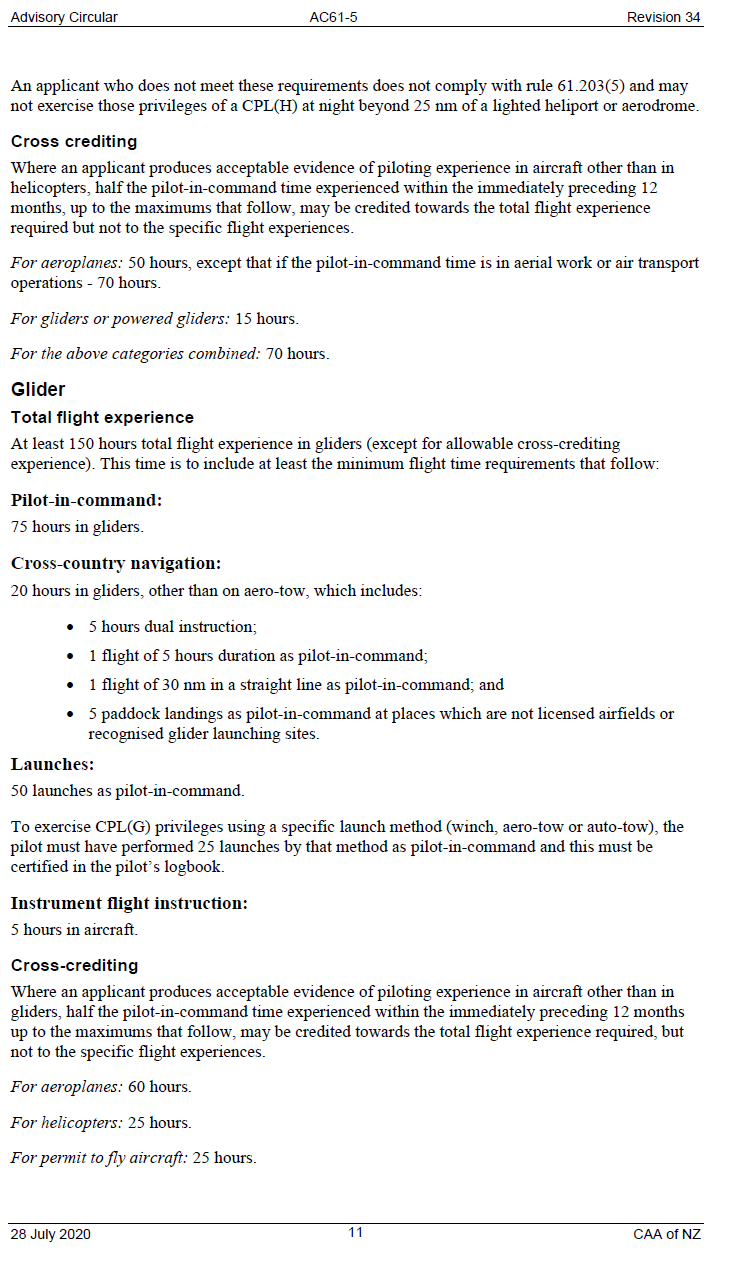
- The helicopter conducted a series of turns immediately before, and after, reaching the township of Lawrence. Soon after passing Lawrence, while over the Lammerlaw Range, the helicopter made a descending right turn through nearly 160° before entering a left spiral dive that ended in a near-vertical nose-down impact with the ground.
- The helicopter was destroyed on impact and the pilot (the sole occupant) did not survive.
Why it happened
- The helicopter had departed the operator’s base one hour after the moon had set and one hour before the beginning of morning civil twilight. It was close to the darkest part of the night.
- The pilot almost certainly encountered cloud in the vicinity of Lawrence and was very likely attempting to manoeuvre around it. With increasing cloud cover and little or no terrestrial light in the Lammerlaw Range area it was very likely that the pilot lost their clearly defined horizon soon after passing Lawrence.
- The helicopter continued to climb straight ahead for nearly three minutes before the pilot very likely became disorientated. The pilot’s disorientation very likely resulted in a high angle of bank turn, followed by the rapid descent of the helicopter, which was consistent with spatial disorientation and loss of control of the helicopter.
- The pilot had met the currency requirements for their restricted night rating. However, it had been about nine years since the pilot had last logged instrument flying practice. It was very unlikely that the pilot was proficient in flight with sole reference to aircraft instruments at the time of the accident.
-
Two safety issues were identified:
1. The rules and guidance information for night Visual Flight Rules (VFR) are ambiguous. This could lead to night VFR pilots flying longer distances than permitted at night and encountering night-flying conditions outside their capabilities.
2. The current rules for and guidance on instrument currency for night VFR do not adequately mitigate the risks of inadvertent flight into conditions where the clearly defined horizon is lost. - The Transport Accident Investigation Commission made two recommendations to the Director of Civil Aviation to address these safety issues.
What we can learn
- It has long been known that instrument flying skills are perishable and need to be regularly refreshed. This equally applies to night flying.
- The risk of losing a clearly defined horizon by not remaining clear of cloud and in sight of the surface increases when flying at night. An immediate transition to instrument flight is required to maintain situational awareness and control of the aircraft in order to re-establish a clearly defined horizon.
- Visual night cross-country flying requires additional training and different skills from those required for visual night flying near a lighted aerodrome or heliport.
- The use of tracking technologies to supplement onboard Emergency Locator Transmitters can significantly reduce the time taken to locate missing aircraft.
- Cockpit video recorders, where fitted, can provide valuable information about causes of accidents and help avoid reoccurrences.
Who may benefit
- All pilots and operators, and those who use the services of helicopters, especially those who are involved in night operations such as frost protection, may benefit from the findings and recommendations in this report.
Factual information Pārongo pono
Narrative
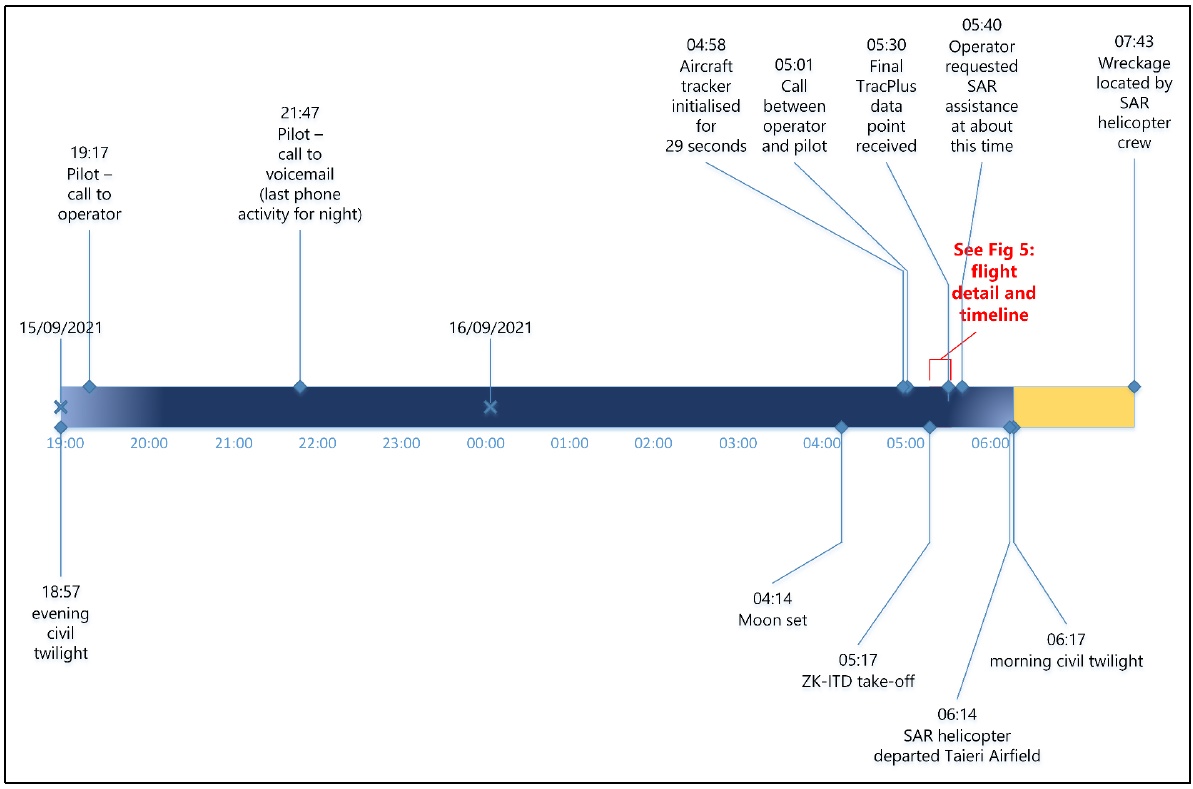
- At 0517 (times in this report are in New Zealand Standard Time (Universal Coordinated Time +12 hours) expressed in the 24 hour format) on Thursday 16 September 2021, ZK-ITD (the helicopter), an Airbus AS350 B3e helicopter, departed from Lister Helicopters’ (the operator’s) base near Milton. The moon had set about one hour before departure, and it was about one hour before morning civil twilight. The pilot was the sole occupant and was not wearing any Night Vision Imaging System, nor were they qualified or equipped to do so. The purpose of the flight was to ferry the helicopter to a cherry orchard near Alexandra, a flight of 62 nautical miles (NM) (115 kilometres [km]), to conduct a frost-protection operation (the operator referred to it as ’frost fighting‘ in their exposition. An exposition is a document detailing the policies and processes that underpin the way an organisation goes about its day-to-day business). The flight would normally have taken about 30 minutes. The helicopter did not arrive at the intended destination.
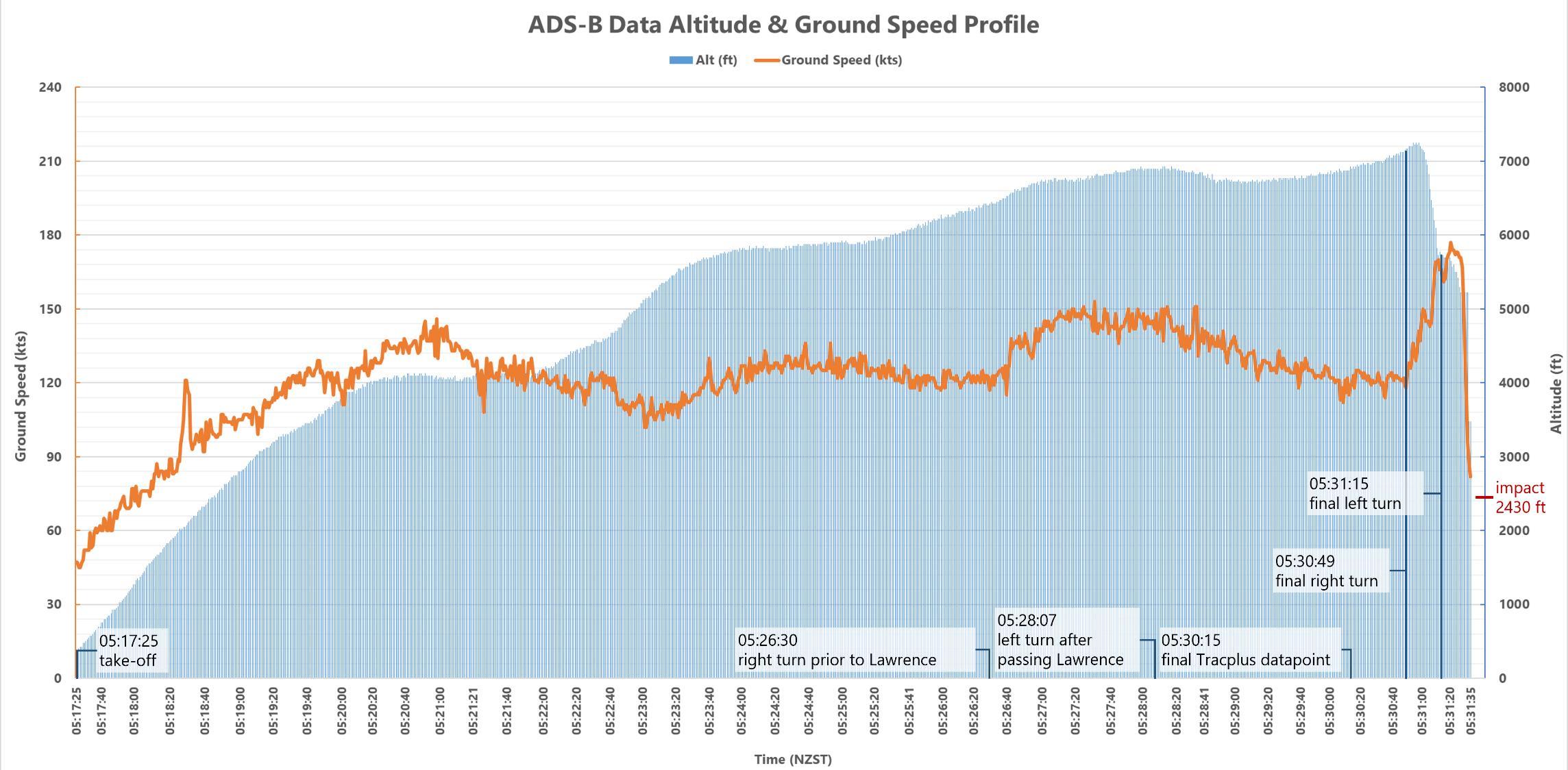
- The flight path of the helicopter was recorded by the Airways New Zealand (Airways) Automatic Dependent Surveillance – Broadcast (ADS-B) system. At 0526:36 the helicopter made a right turn immediately before the township of Lawrence (see Error! Reference source not found.) at an altitude of 6475 feet (ft) (2000 metres [m]) above mean sea level (AMSL). This was the first in a series of turns in the next four minutes.
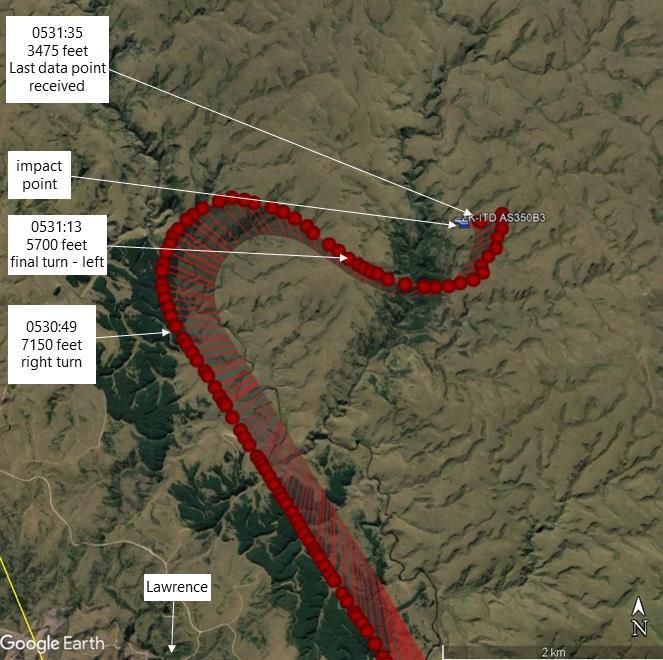
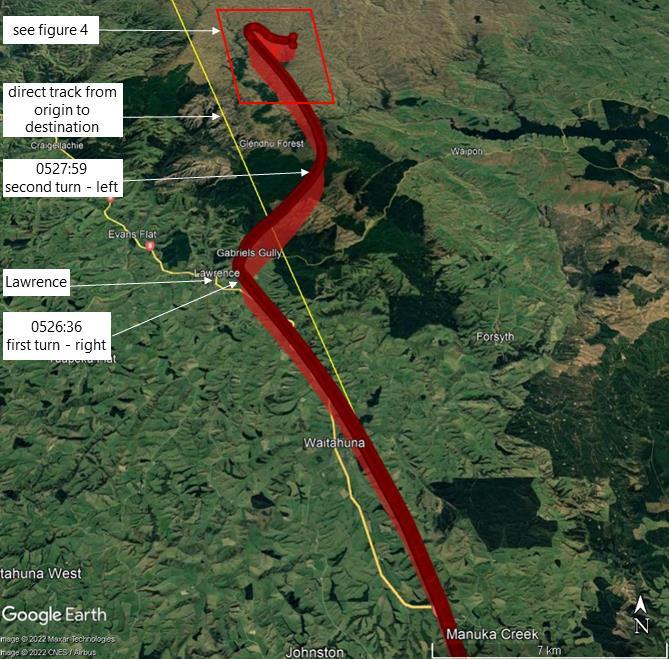
- The last ADS-B data point was received at 0531:35. At that time the helicopter was at an altitude of 3475 ft (1060 m) AMSL and on a track of 293° (see Figure 4). There were several data points recorded after this time; however, they were determined to be ‘coasted’ data points and not from the helicopter. Moments later the helicopter struck the ground in a near vertical nose-down attitude, at an elevation of about 2430 ft (740 m). See Figure 5 for the flight timeline, with altitude and airspeed.
- The helicopter was destroyed as a result of the impact and post-impact fire. The pilot did not survive the accident.
- The pilot had flown a frost-protection operation with the same helicopter at the same orchard on the previous morning (Wednesday 15 September 2021). They had not expected to be required for Thursday morning. After a change in the weather forecast, the client contacted the operator (the operator was also the Chief Pilot of the company. The term operator is used throughout this report) at about 1820 on Wednesday evening to request the aircraft for the next morning. The operator recalled telling the client that it was too late to safely deploy the helicopter that evening, but that the helicopter could be there after first light the following morning.
- The pilot phoned the operator at 1917 on Wednesday and was informed of the task for the following morning. The last recorded activity that night on the pilot’s phone was at 2147.
- On Thursday 16 September 2021 at 0458 the aircraft tracker activated for 29 seconds then shut down again, consistent with the aircraft power being turned on briefly during the pilot’s pre-flight inspection.
- There were two calls at 0501 between the operator and the pilot, the first a 4 second call from the operator to the pilot, followed by a 66 second call from the pilot to the operator. There were no further calls or text messages to or from the pilot’s phone until 0541, when the operator made six attempts to call the pilot’s phone. The last attempt was at 0607.
- The operator advised the Commission that at about 0500 they had discussed the lighting conditions with the pilot before departure, as being clear and starry at the operator’s base at the time. The operator advised the Commission that they told the pilot to use their discretion in departing when it was light enough and when the pilot was happy with the conditions.
- The helicopters in the operator’s fleet were fitted with navigation tracking systems that, once powered up, provided real-time updates of helicopter locations that could be viewed using a cell-phone application. The operator recalled checking the flight-tracking application on their phone at about 0530 and realised the helicopter had departed, but that the tracking information was no longer being updated.
- At about 0540 the operator contacted the owner of another local helicopter company to request search and rescue (SAR) assistance.
- At 0614, after being refuelled and the helicopters’ role equipment re-configured for a search and rescue operation, the SAR helicopter departed for the search area from the SAR helicopter company’s base at Taieri Airfield. The pilot of the SAR helicopter later recalled that the cloud base in the search area had been about 1800–2000 ft (550–610 m) AMSL when they arrived in the area at about 0630. Because of the nature of the terrain, this meant the cloud was down to the ground in many places, including the accident site.
- The operator also tasked another of their pilots to take a company aircraft to search for the missing helicopter.
- The Emergency Locator Transmitter (ELT) from the helicopter did not activate. The operator passed the last recorded tracking data point received from the helicopter tracking system to the owner of the SAR helicopter. The Rescue Coordination Centre supplied the helicopter’s last known location, derived from ADS-B data, to the SAR helicopter crew to help with the search.
- Initially the search was unable to find the crash site because of low cloud, often on the ground. By 0743 the cloud base had lifted further up the hill, sufficient for the SAR helicopter crew to locate the wreckage and to land nearby. The wreckage was at 2434 ft (742 m) AMSL, just below the cloud base at the time it was located.
- The arriving SAR helicopter crew reported high humidity with damp ground and patches of fog when they landed. The crew also reported several small fires still burning around the accident site, which self-extinguished soon after they arrived.
Personnel information
Pilot
- The pilot, aged 36 years, had been issued with a Commercial Pilot Licence (Helicopter) in November 2008. They had been issued with a ‘B’ category flight-instructor rating in May 2011, with the last renewal conducted in April 2021.
- The pilot held a restricted night rating (for night operations within 25 NM of a lighted heliport or aerodrome) issued according to the Civil Aviation Authority (CAA) Advisory Circular 61-5 (AC61-5) Pilot Licences and Ratings – Commercial Pilot Licence (see Appendix 1), first meeting the requirements in October 2008. This meant they could exercise the privileges of a Commercial Pilot Licence (Helicopter) at night but not beyond 25 NM of a lighted (not defined in CARs) heliport (see paragraph 2.70) or aerodrome. The pilot was also issued with a restricted night VFR instructor approval in September 2010.
- The pilot’s last flight-crew competency check with the operator had been conducted in June 2021 in accordance with the operator’s exposition and the Civil Aviation Rules (CARs).
- At the time of the accident the pilot had a total flight time of about 4230 hours, of which about 1200 had been on the AS350 aircraft type (includes both Airbus Helicopters AS350 and EC130 helicopters as they share a type certificate). The pilot had flown about 63 hours of night flying, including 4.2 hours the previous night.
- The most recent night flights recorded in the pilot’s logbook before this had been 1.0 hour on 8 October 2020 and 3.0 hours on 1 October 2020. There were no night flights recorded in the pilot’s logbook between October 2014 and October 2020.
- The pilot had logged a total 20 hours’ instrument flight time, of which 14.5 hours had been simulated in flight and 5.5 hours had been conducted in an approved ground simulator. The pilot’s last simulated instrument flight had been conducted in April 2012.
Pilot medical information
- The pilot held a class 1 medical certificate with no restrictions, valid until 30 October 2021.
- The pilot’s medical history was reviewed during the investigation by the Commission’s Medical Consultant (the Commission’s Medical Consultant holds the following qualifications and fellowships: Bachelor of Medicine and Bachelor of Surgery with Honours (MB ChB (Hons)), Fellow of Faculty of Occupational Medicine (FFOM), Fellow of the American College of Occupational and Environmental Medicine (FACOEM), Fellow of the Australasian Faculty of Occupational and Environmental Medicine of the Royal Australasian College of Physicians (FAFOEM), Fellow of the Australasian Faculty of Public Health Medicine (FAFPHM), Fellow of the Faculty of Occupational Medicine of Ireland (FFOMI), Fellow of the Royal College of Physicians of Ireland (Occupational Medicine) (FRCPI(OM)), Fellow of the Australasian College of Aerospace Medicine (FACAsM), Master of Public Policy (MPP), Diploma in Aviation Medicine (DAvMed), Diploma of Industrial Health (DIH), Fellow of the Aerospace Medical Association (FASMA)), based on communications and medical records from the Civil Aviation Authority, the pilot’s aviation medical examiner and their general practitioner. The Medical Consultant determined that there was nothing of relevance to this accident in the pilot’s recorded medical history.
- The injuries sustained during the accident limited the autopsy examination. The Medical Consultant was in communication with the coroner’s pathologist throughout the examination and considered the autopsy findings and the full autopsy report. The autopsy identified an underlying heart condition. No evidence of performance-impairing substances was found.
- Commission investigators interviewed two people who had been in direct contact with the pilot in the 72 hours before the accident. The interviewees stated the pilot had rested following the previous morning’s flying and was not known to be suffering from any personal health or fatigue issues. There had been no noticeable change in the pilot’s demeanour.
Aircraft information
- ZK-ITD was an Airbus AS350 B3e helicopter, serial number 7815, constructed in March 2014 by Airbus Helicopters in France. The AS350 B3e helicopter is fitted with a single Safran Arriel 2D turboshaft engine.
- The helicopter had 3136.8 hours’ total flying time since new recorded in the aircraft maintenance logbook as of 15 September 2021.
- The helicopter had been imported into New Zealand in July 2014 and registered as ZK-IOJ. The aircraft had had several owners before the operator took possession in January 2019, at which time the registration was changed to ZK-ITD (a change of registration for a newly purchased aircraft to suit personal preference, or to maintain a fleet-wide standard, is not unusual).
- A Review of Airworthiness was carried out on 8 June 2021 at 3082.5 hours’ total time in service; no defects were observed. The next Review of Airworthiness was due on 25 May 2022.
- On 6 August 2021, with 3085.7 hours’ total time in service, it was recorded in the helicopter logbook that the scheduled 600- and 1200-flight-hour inspections and 24-month calendar inspections had been carried out. The helicopter had been repainted and reweighed, with the new basic empty weight of 1331.0 kilograms (kg) recorded in the logbook. The helicopter logbook showed that all required inspections had been carried out at this time.
- A review of the airframe and engine records of life components and repetitive inspections found no non-compliance with the manufacturers’ instructions. The helicopter flight manual was not available for review because of damage from the accident.
- Airworthiness directives were checked against the CAA’s airworthiness directive schedules. There were no outstanding airworthiness directives applicable to ZK-ITD.
- The operator had its own fuel supply for use by company helicopters. Evidence of the fuel load taken was not available to the investigation; however, the operator recalled that with the type of operation to be flown, the pilot should have departed from the operator’s base with a full fuel load, taken from the operator’s own supply tank.
- The fuel supply chain and quality of the fuel were reviewed by investigators. The fuel provider confirmed that the sample testing had proved satisfactory, and the fuel had met the required specifications. Other aircraft belonging to the operator used the same fuel before and after the accident, with no reported concerns.
Meteorological information
- The MetService area forecast issued at 2311 on 15 September 2021 and valid from 0300 to 0900 on 16 September 2021 for the area around the operator’s base, was for broken cloud16 with bases between 1200 ft and 1700 ft (610 m and 915 m) AMSL and tops between 6000 ft and 7000 ft (1520 m and1830 m) AMSL. Visibility was 20 km reducing to 5000 m in rain with an approaching cold front. The forecast for the Otago area where the flight proceeded was for broken cloud with bases between 2000 ft and 3000 ft and tops between 5000 ft and 6000 ft. Visibility was forecast as 30 km reducing to 500 m in localised fog and freezing fog patches. Freezing level was forecast over the Otago region between 3000 ft and 3500 ft.
- The wind was forecast (Area Clyde (CY) valid 1200 to 0600 UTC) to be from the southwest at 10 knots (kt) at 3000 ft increasing to west-southwest and 20 kt at 10,000 ft.
- The Terminal Aerodrome Forecast for Dunedin Aerodrome (the nearest aerodrome to the flight route), issued at 2309 on 15 September 2021, was valid from midnight until 1800 the following day. For the time of the flight, it forecast the surface wind as variable at 2 kt and 30 km visibility with clear skies. There was a 30% probability of visibility reducing to 500 m in freezing fog between 0100 and 0800.
- The National Institute of Water and Atmospheric Research (NIWA) weather station in Balclutha, 16 km south-west of the operator’s base, recorded a relative humidity of 88% and a temperature of +5°C at 0520, three minutes after the time the helicopter departed.
- By comparison, the NIWA station at Alexandra, 64 km north-northwest of the accident site, showed relative humidity rising to 98% and temperature lowering to ‑0.3°C at 0530, about the time of the accident.
- A local helicopter pilot flying southwest from Taieri to Kaitangata flew past the operator’s base at about 0506. The pilot, operating on night-vision goggles, reported that the cloud base in the area was about 2200 ft (670 m) AMSL, with cloud extending to the west.
-
CARs Part 91.301 Visual Flight Rules (VFR) meteorological minima for flight in uncontrolled airspace requires:

However, Part 91.301(c)(1) states that:
a helicopter may operate in Class G airspace with a flight visibility of less than 5 km if manoeuvred at a speed that gives adequate opportunity to observe other traffic or any obstructions in order to avoid collisions.
Illumination
- The moon set at 0414 (see mooncalc.org), about one hour before the helicopter departed the operator’s base.
- The beginning of morning civil twilight was published as 0617 (Aeronautical Information Publication New Zealand Gen 2.7 – 6). Sunrise was at 0641 (see suncalc.org).
- As a result, there was virtually no background illumination to give a clearly defined horizon.
Recorded data
- The helicopter was fitted with TracMap GPS and TracPlus™ navigation and tracking systems that recorded its flight path. The flight path of the helicopter was also recorded by Airways’ ADS-B tracking system. Collectively, the tracking systems provided an accurate record of the helicopter’s flight path for the duration of the flight.
Flight recorders
- The helicopter was not fitted with a flight data recorder or a cockpit voice recorder, nor was it required to be. However, the helicopter was fitted with a Vehicle and Engine Multifunction Display (VEMD), an Engine Data Recorder (EDR) and an Electronic Engine Control Unit (EECU). The VEMD was designed to record and display a range of engine- and airframe-related parameters, including any exceedances of the manufacturer’s limits. The VEMD does not record control inputs or position.
- The helicopter’s VEMD, EDR and EECU were damaged in the accident. They were removed and sent to the Bureau d’Enquêtes et d’Analyses (BEA) (the BEA was the International Civil Aviation Organization’s Annex 13 representative for the state of manufacture (France) of the helicopter and engine). in France to determine if any information could be extracted. The BEA was able to download the engine performance data for the last 32 flights from the VEMD. The data identified nothing unusual for the 32 flights, including the accident flight. There were no recorded engine exceedances or malfunctions. No data could be recovered from the EDR or EECU because of fire damage.
-
The summary of the BEA report states:
Flight report: The last recorded flight was flight 1556 and was identified as the flight of the event. It lasted 22 min 45s. There was no failure, nor overlimit recorded.
Failure report: The last failure recorded was related to flight 1513, 43 flights before the flight of the event.
EPC [in-flight engine power check]: The last EPC was good and was done during flight 1553, three flights before the accident flight.
Other digital data sources used in the inquiry
- The pilot’s cell phone records included times and durations of calls and details of text messages between the pilot and other parties, including the operator and client on the day of the flight and the previous day.
Site and wreckage information
- Terrain
The accident site was 15 km northeast of Lawrence at an altitude of 2434 ft (742 m) AMSL. The terrain was generally rolling, with gullies and small valleys leading up to the Lammerlaw Range north of the site. - The surface consisted of tussock grass and some groups of small trees, predominantly around the valleys. There was a thin layer of soil over a solid clay base.
Impact
- The helicopter descended in a left spiral dive, striking the ground in a near-vertical nose-down attitude with a very high rate of descent.
Wreckage
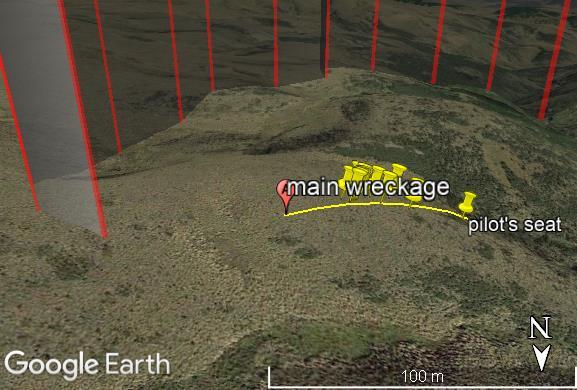
- The right rear window was located about 340 m from the main wreckage, on a bearing of about 090° true. The right rear door and left rear window were located together on the same line about 180 m from the main wreckage. They were all located outside the flight path of the helicopter as it descended (see Figure 7). The majority of the helicopter wreckage, including the engine and both main and tail rotors were located close to the initial impact point.
- The left skid and flight step were buried at a depth of about 1 m into the clay. Some small pieces of the nose of the aircraft, and some parts of the instrument panel, were buried to the right and forward of the left skid.
- The orientation of the helicopter on initial impact was assessed as being on a heading of about 150° true. The main wreckage, including the pilot’s seat and other items, were displaced outwards and to the right of the direction of impact (see Figure 8 and Figure 9).
- The impact of the helicopter removed the top layer of soil, leaving a small crater. The fuselage of the helicopter was lying next to the crater. The blades were still attached to the main rotor hub and were in the topsoil layer immediately in front of the nose impact point (see Figure 10). There were breakages in the Starflex™ main rotor hub and two of the three vibration-damper springs were thrown clear of the wreckage.
- The rear section of the tail boom, including the tail rotor and tail rotor gearbox were largely intact with damage consistent with the impact forces, and located to the north of the initial impact point.



Organisational information
Operator
- The operator held a CARs Part 119 Air Operator Certificate and a Part 137 Agricultural Aircraft Operator Certificate, issued by the CAA. The operator’s certificate permitted operations in accordance with the operator’s exposition, which did not permit the operator to conduct VFR air-transport operations at night.
-
The operator, according to the CAA website guidance on frost protection, was also permitted to conduct operations under CARs Part 91 General Operating and Flight Rules. The CAA website included the following guidance for frost protection (see Helicopter frost protection):
Frost protection operations can be carried out for hire or reward under Part 91 of the Civil Aviation Rules.
Pilots engaging in frost protection must hold a Commercial Pilot Licence, Helicopter, and a current night rating.
Any related flights with passengers on board, such as reconnaissance flights to survey vineyards, must be done by the holder of a Part 119 Air Operator Certificate.
The New Zealand Helicopter Association has published a standard operating procedure for Aerial Frostfighting Operations which provides guidance on managing risks.
-
The operator’s exposition contained a section on frost fighting (also known as frost protection, the term used by the CAA). The following are extracts from the manual (emphasis as in the original):
Hazards
• All frost fighting work must be carried out with visual reference to the ground, if a risk of losing this visual reference to the ground exists then the operation must stop immediately.
• Frost fighting is only approved if the pilot has thoroughly inspected the area to be treated in ‘daylight conditions’ prior to commencing operations. This requires that the aircraft be positioned to the scene of operations in time to carry out the necessary inspections in daylight.Callout Procedures
• The client must be advised of the latest time that a Frost Fighting callout will be accepted. That time is calculated by adding the time needed to get the aircraft and crew prepared, the ferry flight time required and the site inspection time. This total time then needs to be deducted from evening civil twilight to establish the final callout time.
Aviation Industry Association New Zealand AIRCARE™ Accreditation Programme
-
The operator was accredited to the Aviation Industry Association New Zealand AIRCARE™ Accreditation Programme (see AIRCARE™) on 25 November 2020. The accreditation was valid for three years. The standards in the AIRCARE™ programme for which the operator was accredited were listed on its Certificate of Accreditation as:
• Safety Management System – QA and Risk Management
• Environmental – Discharges – GROWSAFE
• Environmental – Discharges – SPREADMARK – Aerial
• Environmental – Amenity Values – Noise Abatement -
The Aviation Industry Association New Zealand, which includes the New Zealand Helicopter Association as a division, developed the AIRCARE™ programme to assist members to meet industry best-practice flight-safety and environmental-management systems. The AIRCARE™ website includes the following statement:
The rules and standards incorporated in this programme not only represent best industry practice but compliance with them will also provide independently assessed assurance that participants in the programme are performing at a level that consistently ensures compliance with regulations and industry codes of practice.
- The AIRCARE™ resources available included Frost Fighting Standard Operating Procedures, which outlined the roles and responsibilities of all participants in frost-fighting operations, including management, pilots and clients.
-
Pilot responsibilities included:
He/she is fully aware of the requirements of these procedures particularly in relation [to] ferry flight after Evening Civil Twilight and before Morning Civil Twilight.
He/she fully understands the dangers of losing visual reference with the ground during operations and establishes practices that do not allow this to occur.
-
The AIRCARE™ document included a comprehensive Hazard Register with Controls. Included in this register was the following risk control for loss of spatial orientation:
Hazard identified Potential harm Hazard controls Loss of spatial orientation Serious or fatal • Always maintain visual reference with the ground
• Don’t carry out cross-country flight to and from the block being treated**While not explicitly stated, the advice on cross-country flights would logically only apply to night flights
CAA Night Visual Flight Rules
-
The eligibility requirements for a Commercial Pilot Licence are listed in CARs Part 61, under Subpart E Commercial Pilot Licences (for simplicity, this report refers to the rules and guidance for commercial helicopter pilots. However, the rules and guidance for private helicopter pilots are substantially similar and the same lessons apply). The requirements for a night rating, as part of Part 61.203 (a), include:
(5) if the person seeks to exercise commercial pilot privileges during the night, have night flight time experience acceptable to the Director (the Director of Civil Aviation).
- CAA Advisory Circulars (ACs) contain guidance on standards, practices and procedures that the Director has found to be acceptable means of compliance with the associated rules and legislation.
-
AC61-5 stated that helicopter pilots required the following experience (holders of private or commercial aeroplane licences do not have an ‘operations within 25 NM’ option):
For night operations within 25 NM of a lighted heliport or aerodrome:
- 2 hours dual instrument flight instruction in helicopters; and
- 10 hours night flight time in helicopters including:
o 5 hours dual instruction
o 2 hours solo including 10 solo take-offs, translation circuits and landings at night.However, where an applicant has completed 5 hours night flight time in helicopters including 2 hours dual instruction, 2 hours solo, and 2 hours dual instrument flight instruction in helicopters, the applicant may exercise the privileges of a PPL(H) [Private Pilot Licence (helicopter)] at night.
For night operations beyond 25 NM of a lighted heliport or aerodrome (night cross-country):
- 10 hours dual instrument instruction in helicopters of which no more than 5 hours may be instrument time in a synthetic helicopter flight trainer; and
- 10 hours night flight time in helicopters including:
o 5 hours dual instruction
o 2 hours solo including 10 solo take-offs, translation circuits and landings at night
o 3 hours night cross-country training which is to have been conducted in accordance with the syllabus set out in Appendix II of this advisory circular.An applicant who does not meet these requirements does not comply with Rule 61.203(5) and may not exercise those privileges of a Commercial Pilot Licence (helicopter) at night beyond 25 NM of a lighted heliport or aerodrome.
-
CARs Part 1 Definitions and Abbreviations defines a heliport as:
any defined area of land or water, and any defined area on a structure, intended or designed to be used either wholly or partly for the landing, departure, and surface movement of helicopters.
It defines a cross-country flight as:
a flight which extends more than 25 nautical miles in a straight-line distance from the centre of the aerodrome of departure.
- CARs Part 1 Definitions and Abbreviations does not define ‘lighted heliport’.
- See Appendix 1 for the complete night-flying advice contained in AC61-5.
Spatial disorientation
- Spatial disorientation is described as a state characterised by an erroneous sense of one’s position and motion relative to the plane of Earth’s surface. It is caused by the orientation senses within the body (vision (eyes), vestibular (inner ear) and proprioceptors (receptors within the subcutaneous tissues)) misrepresenting a person’s position in space (United States Department of Transportation, 2010).
- In normal circumstances, the visual system is dominant and provides approximately 80 per cent of raw orientation information sent to the brain for processing. When visual cues are poor, missing or absent entirely, the brain relies on information provided by the vestibular and proprioceptive system for orientation. However, both systems are less accurate than vision and both systems are susceptible to illusions. This can result in the brain receiving conflicting sensory information and misinterpreting the way in which the individual is orientated or moving.
The vestibular system is prone to several common illusions that can affect pilots during flight. The system is designed to sense motion on the ground and is therefore more limited and less reliable when exposed to manoeuvres typical of those flown in an aircraft that has three axes of rotation (for a comprehensive review of how the vestibular system works, see Demir & Aydin (2021)). Provided adequate visual cues are available, these will take precedence over the information transmitted by the vestibular system, and a pilot can correctly interpret their orientation despite the presence of any illusions. - When a pilot lacks the visual cues required to orientate themselves correctly, spatial disorientation can occur. The primary visual signal for referencing orientation is the ability to determine where the horizon is, and the loss of this reference typically occurs when flying either in cloud or on dark (moonless) nights when there is little terrestrial lighting. It has been estimated that almost every pilot will experience an episode of spatial disorientation in their flying career (Australian Transport Safety Bureau, 2007). When a pilot becomes spatially disorientated, the aircraft will continue to respond normally to the pilot’s control inputs, which are based on the pilot’s perception of their orientation in space. This can lead to a departure from the intended flightpath but will not necessarily result in any aircraft limits being exceeded. Spatial disorientation accidents are frequently fatal, with some studies placing fatality rates as high as 80–90 per cent.
-
Given the prevalence of spatial disorientation during flight, there is an extensive body of international industry guidance material available to pilots. Much of this guidance material is captured in the Australian Transport Safety Bureau (2007) research and analysis report. To avoid becoming spatially disorientated during night flight, the report recommends the following:
Pilots should seriously weigh the option of rescheduling a flight if it would otherwise involve night VFR operations. If night VFR operations are conducted, then pilots need to consider the amount of celestial light that will be available, including information about the phase of the moon, and whether high level cloud will reduce the amount of light that would increase the challenges of night operations (Australian Transport Safety Bureau, 2007, p. 24)
-
To recover from being spatially disorientated, pilots must rely on their flight instruments and be able to interpret and trust the information that is provided correctly, despite experiencing what can be powerful and disorientating motion sensations incongruent with what is displayed on the instruments.
When a pilot’s vision is compromised by darkness or bad weather conditions… acceleratory motion cues can cause the development of SD (spatial disorientation) however, the pilot usually avoids it by referring to the aircraft instruments for orientation information. If the pilot is unskilled at interpreting the instruments, if the instruments fail or, as frequently happens, if the pilot neglects to look at the instruments, those misleading motion cues inevitably cause disorientation.
A pilot is far less likely to become disoriented if he or she uses the instruments as soon as out-of-cockpit vision is compromised and stays on the instruments until continuous contact flying is assured. (Davis, Johnson, Stepanek, & Fogarty, 2008, p. 185)
- Research on spatial disorientation indicates that, for helicopter pilots who are not instrument rated, loss of control can occur within about 60 seconds when they lose a clearly defined horizon. Many regulatory and aviation safety agencies have taken steps to highlight the dangers of spatial disorientation for non-instrument-rated pilots, including through the educational videos 178 Seconds to Live for aeroplane pilots and 56 Seconds to Live for helicopter pilots. See Appendix 2 for a summary of recent occurrences of spatial disorientation reported in New Zealand and Australia.
Analysis Tātaritanga
Introduction
- The accident flight was a positioning flight from the operator’s base in Milton to a client’s cherry farm near Alexandra and was being conducted as a night VFR flight.
- The pilot had spent the previous night at the same property, conducting frost-protection flights after repositioning the aircraft during the day in accordance with the operator’s procedures. The pilot therefore had some familiarity with the area of operations and the route to and from the destination. They had recently flown the route to and from during daylight hours only.
- The following section analyses the circumstances surrounding the event to identify those factors that increased the likelihood of the event occurring or increased the severity of its outcome. It also examines two safety issues that have the potential to affect future operations adversely.
What happened
- The flight proceeded normally until immediately before Lawrence. Tracking data showed the track over the ground was consistent with, although much higher than, the tracks the helicopter had previously flown to and from the same destination. The previous flights were conducted during daylight with the same pilot the previous day and a different pilot from the operator the day before that.
- Immediately before and after the township of Lawrence, there was a series of turns. The turns were followed by an apparent loss of control of the helicopter, which then spiralled down, striking the ground.
Avenues of inquiry
- The Commission considered several potential contributing factors to the loss of control of the helicopter and the subsequent high-energy vertical impact with terrain. Some of these potential contributing factors are discussed below.
Medical
- The pilot was 36 years old and held a valid class 1 medical certificate with no restrictions. The pilot’s aviation medical examiner and their general practitioner had not identified any underlying medical conditions in the pilot.
- The pilot’s post-mortem examination identified an underlying heart condition, the nature of which a cardiologist stated may cause cognitive impairment. This raised the possibility that medical impairment caused or contributed to the accident. The Commission assessed this alongside other evidence outlined below, including the environmental conditions and the conduct of the flight.
- The pilot’s partner did not recall noticing any change in the pilot’s demeanour in the days leading up to the accident flight, including the evening before the accident flight.
- A review of the pilot’s recent history indicated there were no fatigue issues and they were observed to be in good health, with no noticeable changes to their demeanour reported by those close to them leading up to the accident.
- Of more significance, during the flight the pilot conducted precise manoeuvres that appeared to be very controlled and deliberate and in direct response to the environmental conditions they were encountering. Those manoeuvres were inconsistent with sudden medical incapacitation or cognitive impairment.
- Had a sudden medical event occurred causing pilot incapacitation, the flight profile would very likely have been different from the one flown. The recorded flight path was consistent with pilot spatial disorientation in the final stages of the flight. While the inability to conduct a comprehensive autopsy meant the Commission could not fully exclude a medical event causing incapacitation or cognitive impairment, the Commission considered that it was very unlikely that the pilot suffered a medical event leading to a loss of control. See paragraphs 3.39 to 3.56.
- There was no presence of any performance-impairing substances.
Mechanical
- The helicopter was maintained in accordance with the manufacturer’s instructions, with no outstanding maintenance requirements, defects or airworthiness bulletins in effect at the time of the accident.
- As discussed in paragraph 2.34, the helicopter should have departed with a full fuel load. This was supported by the operator’s comments, the type of operation to be flown and the finding of fire at the accident.
- The helicopter’s empty weight was 1331.0 kg (established by re-weighing on 6 August 2021) and the maximum allowed take-off weight was 2250 kg. Allowing for a full fuel load of 427 kg (540 litres converted at specific gravity of 0.79, as per the Airbus Helicopters AS350 B3e Flight Manual), this left about 492 kg of usable weight for the pilot and any cargo or operations equipment. No evidence of any significant extra cargo (evidence of a standard away kit, including blade tie-downs, covers and spare oil, was found at the scene) was found at the accident scene, nor was any expected. It was therefore virtually certain that the helicopter weight and centre of gravity were within limits.
- Further to the evidence in paragraph 2.48, the BEA concluded that there was no sign of failure of the monitored aircraft systems before the accident.
- Signature marks on the main rotor hub were consistent with the blades rotating at speed on impact.
- The helicopter’s initial turns by Lawrence, first to the right and then to the left, showed that the helicopter was under control. It was also very unlikely that there were any mechanical or system malfunctions during this time.
Environmental
- The moon had set approximately one hour and 15 minutes before the accident. The beginning of morning civil twilight was at 0617, about one hour after the helicopter had departed the operator’s base, and the sun was not due to rise until 0641.
- There were several built-up areas in the initial segment of the flight. When the helicopter first took off, and until just past Lawrence, it is very likely that there was light available to provide a clearly defined horizon from terrestrial sources such as houses, streetlights and vehicles.
- It was close to the darkest part of the night when the helicopter took off and there would have been insufficient light for a clearly defined horizon in the Lammerlaw Range area, after passing Lawerence.
Cloud
- The weather forecast and reports and the observations of another pilot who flew past the operator’s base and of the first responders who located the accident site, indicate it was virtually certain that there was cloud in the vicinity of Lawrence as the helicopter approached.
- The highest terrain on a direct track from Milton to the orchard was about 3300 ft AMSL at about 42 NM (78 km) into the flight (just after the halfway point) with other high ground in the second half of the flight. The helicopter had maintained a climb since departure from Milton, passing 3300 ft about four minutes after departure and continuing to climb to the ultimate altitude of 7250 ft AMSL (2200 m).
- MetService observations and calculations relating to Otago on 16 September 2021 showed the sky was clear at the operator’s base at the time the helicopter departed. The first cloud would have been located about 8 NM (14 km) after departure, with the estimated cloud tops at about 3700 ft AMSL, increasing to an estimated altitude of about 7100 ft AMSL near the accident site (see Figure 11).
- There are a number of possible explanations for the pilot’s decision to climb well above the height of the maximum ground elevation on the flight path, and these include:
-
to climb above the cloud layer, with the expectation that there would be clear air at the destination
-
to climb sufficiently to see the lights at the destination as early as possible, to give a clearly defined horizon in the dark area of the Lammerlaw Range after passing Lawrence
-
to give the maximum safety buffer over the rising terrain
-
a combination of some, or all, of the above
-
At night, cloud is only visible in the presence of light, such as light from the ‘glow’ of a built-up area or moonlight. It is very likely that any cloud present would have only been visible with the aid of terrestrial lighting, such as the lights of Lawrence. There was no moonlight at the time of the flight to illuminate cloud away from terrestrial lighting.
(Credit: MetService)
- The only celestial lighting available above the cloud layer would have been from starlight. In ideal situations, starlight could give adequate illumination to see some types of cloud if there were no light pollution to reduce the effectiveness of the eye. The aircraft instrument lights would have been on during the flight, normally at a low setting (by necessity, bright enough for the pilot to be able to read the instruments with normal vision. This would contrast to a cockpit set up for Night Vision Imaging System operations, where the instruments have special lighting that has less impact on the visual acuity of the system), but still providing some light pollution that would affect the pilot’s night vision. It is very unlikely that the pilot would have been able to see the cloud tops in the available starlight or have a clearly defined horizon.
- It was very likely that the pilot was attempting to avoid cloud when they initially turned right just before Lawrence. They then attempted to re-establish a flight path direct to their destination when turning left after passing Lawrence.
- With increasing cloud cover and diminishing terrestrial light as the flight progressed past Lawrence, it is exceptionally unlikely that the pilot would have been able to see any cloud present before losing their clearly defined horizon.
- The loss of a clearly defined horizon at night can be caused by a lack of suitable light sources or cloud obscuring any light sources that are available, even if the aircraft remains clear of cloud. It can also be caused by flight into cloud or visible moisture.
- The pilot was not qualified for flight in cloud (ss they did not have an IFR qualification) and the aircraft was not certified for flight in icing conditions (see AS350 B3e flight manual), so the options available to the pilot, once they lost their clearly defined horizon, included:
-
turning into known clear air, usually through 180° to return along the flight path
-
attempting to climb to the top of the cloud level
-
descending to warmer air.
- The first option, to turn through 180°, is the most difficult to execute for a non-instrument rated pilot when attempting to fly on instruments. However, it is usually the safest option with regard to the conditions. If the turn is not completed successfully, it can rapidly lead to spatial disorientation.
- The second and third options are easier to achieve, for a non-instrument rated pilot when flying on instruments. However, they are risky when the extent of the cloud base and tops is unknown.
Icing
- The freezing level was forecast to be between 3000 and 3500ft AMSL over the Otago region.
- A pilot can expect icing when flying in visible precipitation, such as rain or cloud droplets, and the temperature is between +2°C and −10°C (Federal Aviation Administration, 2023).
- The consequences of ice accretion include:
-
changes to the shape of the blade aerofoil, and therefore changes to its lift coefficient
-
an increase in the blade’s drag coefficient
-
an increase in the aircraft’s gross weight.
The first two factors influence the helicopter’s lift/drag ratio, which in turn degrades the rotor thrust/rotor drag ratio when the total reaction leans further away from the axis of rotation.
Icing then can initially be detected by the need for more power as rotor rpm falls off when increased rotor drag begins to take its toll. Since ice accretion is almost always uneven throughout the disc, the resulting vibration gives the pilot an additional warning of ice buildup.
-
The temperatures the helicopter was flying in were in the range for aircraft icing and the formation of icing cannot be ruled out entirely. However, there are several factors that indicate that it is unlikely.
3.38.1. The helicopter appears to have remained above the estimated cloud tops until the very end of the flight. Flight in visible moisture45 is a prerequisite for ice formation.
3.38.2. The helicopter continued to climb throughout the flight, including gaining 200 ft in the beginning of the final right turn. Icing will increase the weight of the aircraft, and generally also reduces the lift available, thereby requiring increased power to continue climbing and maintaining airspeed. In extreme cases there is no further power available, and the aircraft begins to descend.
There is no indication from the evidence available that this occurred in this instance.
Spatial disorientation
- Spatial disorientation as a possible cause is a well-documented contributing factor to accidents at nighttime.
- VFR pilots are trained to always have a clearly defined horizon, to protect against experiencing spatial disorientation and a subsequent loss of control of their aircraft in flight.
-
Flying at night requires a skill set that is different from flying during the day, because of the reduction in visual cues. In September 2020 the CAA revised its Good Aviation Practice booklet on night VFR to assist pilots. A section on illusions begins with:
It is good practice to fly at night by regular reference to instruments, even when external lighting provides good visual cues, because visual and spatial illusions can provide misleading information, and visual reference can be suddenly lost. Use your awareness of illusions to avoid these pitfalls (Civil Aviation Authority of New Zealand, 2020).
- It was therefore recognised by the CAA that it is important for a pilot to have at least a basic knowledge and understanding of, and proficiency in, the skills required to fly at night with sole reference to an aircraft’s flight instruments. The fewer visual cues available, the greater the reliance the pilot must have on their instruments, keeping in mind that night VFR is still governed by the visual flight rules, with the emphasis on maintaining a clearly defined horizon.
- The requirement for instrument skills was reflected in the minimum number of hours of dual instrument instruction required before a pilot is issued with a night rating. However, there was no requirement for instrument currency, which is discussed further in paragraphs 3.68 to
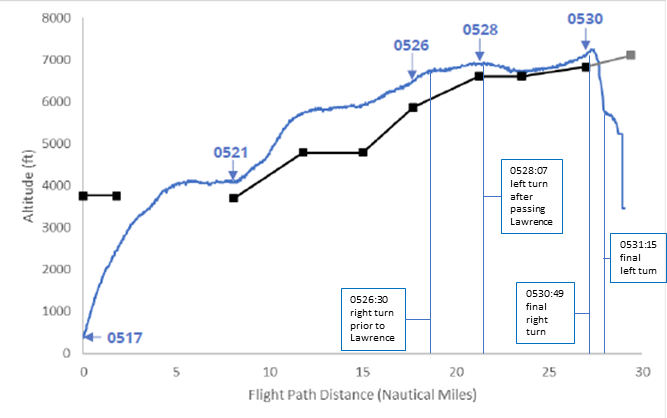
- Approaching Lawrence, a definite and deliberate course change was made. Initially there was a turn to the right through 53°, taking 20 seconds. The rate of turn equated to 159° a minute, slightly less than a rate one turn46. The helicopter climbed about 200 ft (60 m) during the turn, at a climb rate of about 600 ft per minute (182 m per minute). While the climb rate was higher than ideal with reduced visual cues, it was consistent with the climb rate before the turn (see Figure 5).
- The previous flights, conducted during daylight hours, had generally followed the road. At night on the same route, the only significant terrestrial light was emitted at the townships and through other cultural lighting along the way. In contrast, the area towards which the pilot turned was uninhabited and had minimal or no terrestrial lighting.
- The change in course was very likely an attempt to avoid cloud visible to the pilot near the township of Lawrence. The cloud in the area was broken (see para 2.36) and would have allowed some visibility of lights from the ground for the pilot. The region to the right of the track would have appeared darker, potentially giving the illusion of no cloud being present in that area (see also the Commission report AO-2019-005 (Transport Accident Investigation Commission, 2023) in which the pilot experienced a similar visual illusion).
- About two and a half minutes after the alteration in course, the helicopter entered a second right turn at an altitude of 7150 ft (2180 m) AMSL, this time with a rate of turn of about 400° per minute, or more than double a rate one turn. The angle of bank was calculated to average about 37°, based on recorded groundspeed and rate of turn.
- Initially climbing about 100 ft in 7 seconds, the helicopter then descended at a rate of descent in excess of 4200 ft (1280 m) per minute (turning through almost 160 degrees and initially climbing, then descending to 5700 ft AMSL in 24 seconds) during the turn. The helicopter then immediately entered a descending and tightening left turn, descending about 3200 ft to a near-vertical nose-down impact with terrain.
- At high angles of bank, a pilot would likely start feeling the effects of the increased loading. Unless properly managed, an increased loading can have a disorientating effect on a pilot, especially if they move their head during the turn with reduced visual cues.
- Moving their head to look where they were going would be a normal reaction for a VFR pilot, as they would be more used to looking outside the aircraft while flying visually than following the instrument-flying requirement to keep their head still and their eyes scanning the helicopter instrument panel.
- Soon after passing Lawrence, and approaching the Lammerlaw Range area, the pilot was flying into an area of reduced visibility and very likely lost their clearly defined horizon. The helicopter continued to climb straight ahead for nearly three minutes before the pilot very likely became disorientated.
- The pilot had not logged any instrument flying in the past nine years. They also did not have a night cross-country rating or an Instrument Flight Rules (IFR) rating. The pilot was therefore very unlikely to be proficient in flying by sole reference to the instruments, and this was exacerbated by the urgency of needing to transition rapidly from flying by reference to visual cues.
- Non-instrument rated pilots who are not proficient at flying on instruments will require a degree of concentration when conducting basic instrument skills, such as the scan required to maintain a straight and level attitude. Any additional manoeuvres, such as turning the aircraft, will demand more cognitive resource as the pilot is now subjected to vestibular illusions (see paragraph 2.75) and must adapt their scan accordingly to counter this. In this case, the pilot was able to continue flying past Lawrence for several minutes in an apparently controlled manner before the final right turn.
- It is possible that the final right turn was an attempt by the pilot to reverse course and re-establish a clearly defined horizon. However, it cannot be discounted that the turn itself was the result of the pilot becoming spatially disorientated.
- The high angle of bank and the lack of a clearly defined horizon during the right turn would significantly increase the risk of spatial disorientation and then the loss of control of the helicopter. The time from when the helicopter began the final right turn until impact with the ground was about 60 seconds (see para 2.79).
Summary
- The investigation found that there was no evidence of a mechanical issue with the helicopter and that it was very unlikely a medical event occurred. A helicopter is a dynamically unstable aircraft and must remain under positive control by the pilot.52 The two controlled turns before the final right turn indicate the helicopter was being positively controlled by the pilot, making a medical event very unlikely. Had the pilot suffered a medical event, the flight profile leading up to the accident would very likely have been different from the one flown.
- The prevailing environmental conditions meant that the pilot, who was very likely not proficient flying solely on instruments at the time of the accident, very likely did not have a clearly defined horizon. These factors, together with the aircraft’s tracking data during the last minute of the flight, are consistent with pilot spatial disorientation.
Other factors that affect safety
Night-flying rules
Safety issue 1: The rules and guidance information for night VFR are ambiguous. This could lead to night VFR pilots flying longer distances than permitted at night and encountering night-flying conditions outside their capabilities.
- The Commission found ambiguity existed around what was permitted under the night VFR rules and guidance.
- Ambiguity, regardless of intention, creates opportunities for differing interpretations – including for rules to be read to allow the most leniency possible.
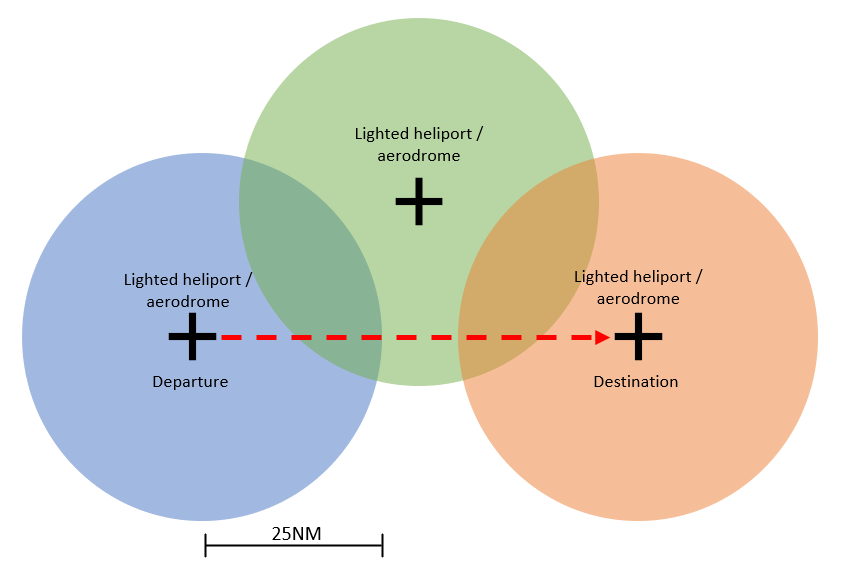
- The wording of AC61-5 is ambiguous in light of the rules regarding what a pilot who was restricted to operations within 25 NM of a lighted heliport or aerodrome was permitted to do. It is unclear whether such a pilot could transit from point A to point B provided they were always within 25 NM of any lighted heliport or aerodrome (ie, the departure and destination were within 50 NM). There is further ambiguity around whether a third intermediate lighted heliport or aerodrome could be used as a waypoint en route to facilitate even longer flights at night (see Figure 12).
- The Commission sought clarification from the CAA on the above interpretation of the CARs. The CAA responded that while AC61-5 could be clearer, the intent was that a pilot travelling beyond 25 NM from their point of departure at night would require the higher standards of the night cross-country rating.
- The 25 NM restriction at night appears to be unique to New Zealand, with all other major jurisdictions restricting night VFR flights to the aerodrome circuit or requiring pilots to have a full night cross-country rating. The CAA’s position is that it is commonly referenced within the Rules/advisory circulars that the 25 NM radius is the limiting distance for flights to be considered cross country. The Commission was unable to determine the relevance of the 25 NM limit.
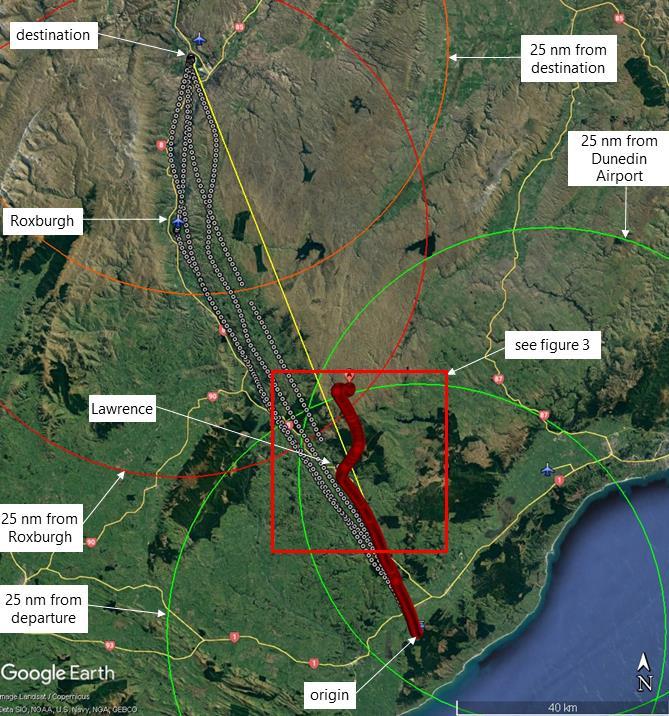
- The operator advised the Commission that as the flight was within 21 NM of Dunedin, and then used Roxburgh and Alexandra for short ‘hops’ within 25 NM of each other meant that in their view there was no requirement for a night cross-country rating for this flight (see Figure 13). The operator’s interpretation of AC61-5 appears to be different from CAA’s own interpretation of the intent of AC61-5, as stated by the CAA to Commission investigators.
- According to the Aeronautical Information Publication New Zealand, neither Roxburgh nor Alexandra had aerodrome lighting. However, the exact lighting that would be required for a helicopter to operate at those aerodromes at night was not defined in the CARs.
- There is no clear definition of what constitutes a ‘lighted’ heliport. This adds further to the potential for pilots to incorrectly interpret night VFRs.
- During the investigation, Commission investigators became aware of different interpretations, among other helicopter pilots and operators, of what is permitted under the rules for visual night flying.
- The investigation found a safety issue in that the current rules and guidance for visual night flying, and night currency requirements, do not adequately mitigate the risks of conducting visual flying at night. The Commission has made a recommendation in Section 6 to address this.
Instrument currency requirements for night flying
Safety issue 2: The current rules on and guidance for instrument currency for night VFR do not adequately mitigate the risks of inadvertent flight into conditions where a clearly defined horizon is lost.
- The pilot was a Category B helicopter flight instructor with about 4230 hours’ total flight time. Their logbook showed they had a restricted (25 NM) night rating with a total of about 63 hours’ night-flying experience, consisting predominantly of instructing students, with some night frost-protection flying.
- The pilot’s logbook recorded 20 hours’ instrument flight time, all of which were simulated, with no flight time logged showing flight in actual instrument meteorological conditions (IMC) with sole reference to aircraft instruments. The last entry in the pilot’s logbook recording the pilot flying by reference to instruments was in April 2012, about nine and a half years before the accident.
- The pilot was an experienced aviator and was trained in and qualified for restricted night flying, and also exceeded the minimum instrument flight time (but not the qualification) required for an unrestricted night rating. The Commission could not identify from the pilots’ logbook whether the pilot had done the cross-country flight training component of a night cross-country rating.
- The pilot met the currency requirements for the restricted night rating that they held. However, the pilot’s logbook recorded no instrument flight time in the nine years preceding the accident. They would therefore have been very unlikely to be proficient in this skill.
-
The importance of instrument currency for pilots is summed up by Davis et al (2008) when discussing spatial disorientation:
The important factors to the pilot in preventing SD (spatial disorientation) are confidence, competency, and currency in instrument flying. It is virtually assured that a non-instrument-rated pilot who penetrates instrument weather will develop SD within a matter of seconds, just as a competent instrument-rated pilot will develop it if he or she flies in weather without functioning flight instruments. Regarding instrument flying skill, one must ‘‘use it or lose it,’’ as they say. For that reason, it is inadvisable (and perhaps illegal) for a pilot to be in command of an aircraft in instrument weather if he or she has not had a certain amount of recent instrument flying experience.
- AC61-5 requires a pilot to have a minimum experience of two hours’ dual-instrument-flight instruction in helicopters to operate within 25 NM of a lighted heliport or aerodrome at night. A minimum of 10 hours’ dual-instrument-flight instruction in helicopters (of which no more than five hours may be instrument time in a synthetic helicopter flight trainer) is required for a night cross-country rating, to fly beyond 25 NM of a lighted heliport or aerodrome at night.
- At the time of the accident there was no requirement for ongoing instrument recurrency training or competency assessments once the applicable night rating was awarded.
- Flying with reference solely to instruments is a perishable skill, and pilots who held IFR ratings were required to undertake refresher training as per CARs Part 61.807 with 3-month and 12-month requirements.
- A non-IFR-rated pilot was not required to maintain instrument flight currency. Such a pilot flying under VFR who lost the required visual cues is unlikely to have the instrument flying competency and ability to transition to flying by sole reference to instruments. A loss of visual cues can occur suddenly and without warning, having a startle effect on the pilot with the associated risk of further exacerbating the situation.
- The SKYbrary article ‘Inadvertent VFR Flight into IMC’ (instrument meteorological conditions) gives a concise review of the threats, likely errors and risk management required if a pilot inadvertently loses visual reference. While it is written with a Private Aeroplane Pilot Licence holder in mind, the lessons contained are relevant to any pilot licence holder without an instrument rating.
- The pilot exceeded the minimum requirement for instrument time for their restricted night rating by a factor of 10, and they had almost double the required instrument hours for a night cross-country rating. However, they had not logged any instrument time in more than nine years at the time of the accident. The importance of instrument currency is discussed in paragraph 2.78.
- The lack of any requirements for recent experience in instrument flight for a VFR pilot at night was a safety issue given the recognised difficulty when transitioning from flight with visual reference to the ground to flight with sole reference to aircraft instruments. The Commission has made a recommendation in Section 6 to address this.
Emergency Locator Transmitter (ELT)
- The ELT not activating when the helicopter struck the ground is of concern. The ELT is designed to emit an emergency broadcast signal, usually including a location, when an aircraft experiences g-forces consistent with an accident. The broadcast signal is used by SAR teams to aid in locating accident sites. Expedient location of a crashed aircraft increases the chances of survival for the occupant/s, although the pilot did not survive this accident.
- The exact cause of the failure of the ELT to activate could not be determined. However, it is as likely as not that the impact forces were outside its design parameters.
- Despite not having an ELT location on which to base their search pattern, the SAR helicopter crew were able to locate the wreckage about 73 minutes after commencing their search. The biggest delay was almost certainly caused by the time taken for the cloud base to lift above the accident site.
- The availability of tracking data from the onboard helicopter tracking system and the available ADS-B data combined to give searchers a small and accurate area in which to search for the wreckage. These systems almost certainly reduced the size of the search area and the time taken for searchers to find the accident site.
- The Commission has previously made recommendations (Transport Accident Investigation Commission, 2014) to the CAA to improve the performance of ELTs. The importance of technologies to track and to locate has been an item on the Commission Watchlist since 2015 (Transport Accident Investigation Commission, n.d.). These technologies improve people’s chances of surviving aircraft accidents and incidents. The Commission has also commented on technologies to locate vessels and rail vehicles. This accident reinforces those recommendations.
Cockpit video recorders
- Cockpit video recorders are now available, and the Commission has recommended that these be fitted to helicopters and other general aviation aircraft to help explain how accidents occur. The Commission acknowledges the efforts aviation industry participants have made in developing affordable video, audio and data recorders, and the regulators’ work to enable fitment of these technologies via Supplemental Type Certificates. Where fitted, these recorders can provide valuable information about causes of accidents and help avoid recurrences. The helicopter in this accident was not fitted with a cockpit video recorder, potentially denying investigators valuable insights into the progress of the flight.
Appendix 1. Advisory Circular AC61-5 Night extract