Circumstances of this fatal helicopter crash into dense forest included: risky take-off towards and over treetops; old worn engine lacked power; and aircraft not airworthy. Also private pilot licence conditions breached (flying for payment or reward). Lessons about obeying Civil Aviation Rules; reporting concerns; CAA monitoring of nominally private aviation participants.
Executive summary Tuhinga whakarāpopoto

- On 27 March 2017, a two-seat Robinson Helicopter Company R22 helicopter, registration ZK-IHA, was carrying a slung load as part of a local aerial hunting operation near Reefton. Shortly after take-off, while the helicopter was climbing over densely forested terrain, the helicopter and load struck the tree canopy and then the terrain. The helicopter was destroyed, and the pilot, who was the sole person on board, was fatally injured.
- The Transport Accident Investigation Commission (Commission) found that the helicopter likely experienced a low rotor-revolutions-per-minute event during the accident sequence. However, it could not be determined if this event occurred before the initial impact with the tree canopy or during the subsequent descent. The Commission was unable to determine conclusively why the helicopter struck the tree canopy and subsequently the terrain. However, it was likely due to either:
- the engine not delivering the demanded power, or
- the pilot inadvertently not maintaining a suitable clearance above the tree canopy.
- The Commission found that the environmental conditions at the time of the accident had the potential to affect the safe conduct of the flight.
- The Commission found that the engine was in a condition that would have likely prevented it being capable of producing the maximum specified power.
- The Commission found that the pilot lifted off and flew the helicopter over densely forested terrain, when other take-off directions were available that offered less risk in the event of an aircraft emergency.
- The Commission found that the pilot had conducted a commercial flight, which was beyond the privileges of the pilot’s private pilot licence.
- The Commission found that the helicopter had not been maintained in accordance with the manufacturer’s instructions and the Civil Aviation Rules, and the engine showed signs of wear that were inconsistent with the hours recorded in its logbook.
- The Civil Aviation Authority’s regulatory and surveillance controls for the non-commercial aviation sector were broadly aligned with international standards and recommendations for this sector. Therefore, the Commission has not made any new recommendations.
- The key lessons identified from the inquiry into this occurrence are:
- all aviation participants have a responsibility to ensure they comply with the Civil Aviation Rules, which are in place to ensure the safe conduct of flight
- aviation participants who have concerns about other participants should raise these concerns through the Aviation Related Concerns system, as they have the potential to prevent accidents and incidents occurring
- the circumstances of this accident show the importance of the regulator continuing to monitor sectors of the industry it deems to have a low consequence of failure.
Factual information Pārongo pono
Narrative
- On 27 March 2017, a two-seat Robinson Helicopter Company R22 helicopter, registration ZK-IHA (the helicopter), was carrying a slung load as part of a local aerial hunting operation near Reefton. Shortly after take-off, while the helicopter was climbing over densely forested terrain, the helicopter and load struck the tree canopy and then the terrain. The helicopter was destroyed and the pilot, who was the sole person on board, was fatally injured.
Background
- At about 1000 that day, the pilot had received a phone call from a hunt manager who was located near Kaikōura on the east coast of the South Island. The hunt manager ran a business providing organised hunting expeditions for clients. The hunt manager had cancelled an expedition on the east coast that day due to poor weather conditions and was trying to organise an alternative expedition for their client. The hunt manager checked if the weather was suitable around Reefton and if the pilot was prepared to fly the client on a local hunting trip. The pilot agreed to the request, so the hunt manager and their client travelled to the pilot’s property in Reefton, where the helicopter was hangered.
The flight
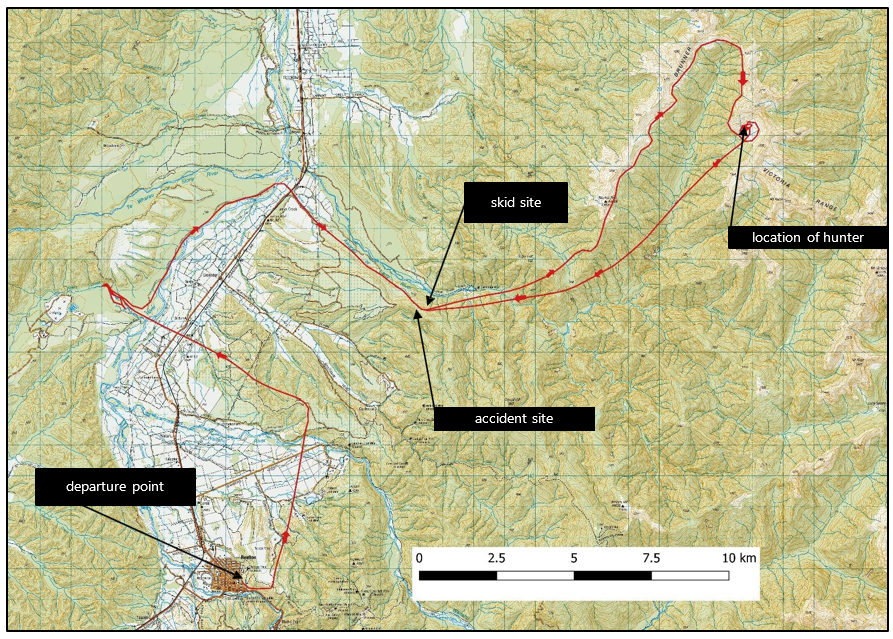
- The pilot prepared the helicopter for flight and at about 1740 departed with the client on board (see Figure 3 for the flight path). They first travelled to Giles Creek, where the client shot a wild pig. The pilot landed, shut down the helicopter and prepared the pig carcass for recovery at about 1750. The pilot hooked the load onto the helicopter’s cargo hook using a rope strop and flew the helicopter to a skid site in the Larry River valley, where the pilot dropped the pig carcass without landing. They departed the skid site and continued flying.
- While near Mount Pelion (Mount Pelion is in the Victoria Range, east of Reefton), the client shot a deer. They landed and the pilot again shut down the helicopter to prepare the deer carcass for recovery. They agreed that the client would remain on the ground while the pilot dropped the carcass off then returned to continue the hunt. The pilot departed at 1832 with the carcass slung underneath from the cargo hook.
- At 1839, the pilot returned to the skid site and attached the pig carcass to the same strop as the deer carcass. At about 1841, the pilot departed from the skid site and headed towards their property at Reefton.
- Approximately 20 seconds after the helicopter departed, and while climbing over densely forested terrain, the helicopter and load struck the tree canopy and then the terrain. The accident occurred approximately 11 kilometres north-east of the pilot’s property.
- The client was unaware of the accident and was later contacted by the hunt manager after the helicopter had not returned. The client was subsequently retrieved from their location in another helicopter.
Personnel information
- The pilot was familiar with aerial hunting, initially as a shooter for many years and latterly as a pilot. The pilot maintained two separate logbooks, one for helicopter and another for microlight flying. This was normal practice for pilots who flew different categories of aircraft.
- The pilot had commenced flight training for a helicopter licence in March 2006, and at the time of the accident held a current private pilot licence for helicopters, with type ratings for Robinson Helicopter Company R22 and R44, and Guimbal Cabri G2 helicopters. The pilot’s most recent biennial flight review had been completed on 29 July 2015. The pilot had completed additional training to be able to undertake sling load operations and night-time flying under visual conditions within 25 nautical miles of an aerodrome.
- The pilot’s most recent logged flight in the accident helicopter had been on 26 July 2015. Three flights in other helicopters had been recorded since then, with the most recent flight occurring in November 2015. The pilot had logged 329.5 hours’ total helicopter time.
- The pilot’s microlight logbook recorded a biennial flight review having been completed on 6 March 2017, 20 days prior to the accident. The pilot held a current flight instructor rating for microlight aircraft and had flown a range of microlight fixed-wing and autogyro aircraft. The pilot’s total logged microlight time was 935 hours.
- The pilot had a current medical certificate (Class 2) appropriate for the grade of licence. It had one restriction that half spectacles must be readily available. These were found in the wreckage.
- The Coroner-authorised toxicology report did not identify anything of aeromedical concern.
Aircraft information
- The helicopter was a Robinson Helicopter Company R22 HP, serial number 0188, and powered by a four-cylinder, horizontally opposed Textron Lycoming O-320-B2C engine. It had been manufactured in the United States in 1987 and was first operated in Australia as registration VH-HHF. In March 1999 it had been imported into New Zealand and registered as ZK-HHF. The registration had been changed to ZK-IHA in February 2000. The pilot had purchased the helicopter on 22 November 2006 through a private company.
- The helicopter had undergone a 2,200-hour airframe and engine major overhaul in August 2007 and records indicated that it had been flown for 327.7 hours since that time.
- The helicopter’s technical log had no entries for the 12 months prior to the accident. The last recorded 100-hour maintenance check had been on 18 March 2016. At the time of this check the helicopter airframe and engine had accrued 4,727.7 hours’ total time in service.
- The helicopter’s review of airworthiness had expired 10 days prior to the accident, on 18 March 2017.
- The R22 main rotor blades were limited to a 12-year calendar life from the date of manufacture. The main rotor blades fitted to the helicopter had passed their 12-year calendar life on 28 June 2016.
Meteorological information
- At the time of the accident there was an upper-level trough moving across the country with a series of complex fronts affecting the surface conditions. The infrared and visual images showed clear sky from Hokitika up to the Reefton area.
- The aviation forecast for the West Coast area was for occasional rain clearing from the south by midday, with isolated rain showers about and near Hokitika that were expected to clear during the afternoon.
- The Reefton automatic weather monitoring station was located 11 kilometres south-west of the accident site and about 224 metres lower in altitude. Data records from the station at the time of the accident were:
- wind speed: 2 knots
- wind direction: 128° true
- temperature: 19°Celsius
- dew point: 15° Celsius
- atmospheric pressure: 1,010 hectopascals.
- The rescue pilot who attended the accident recalled there being an easterly wind of about five knots; clear sky; and atmospheric pressure of 1,009 hectopascals at the time they were at the accident site.
- The sun position at the time of the accident was 9° above the horizon at 282° true. The sun was due to set at 1935 and evening civil twilight was at 2003.
Wreckage and impact information
- The helicopter’s descent path was marked by damage to the trees. The damage to the tree tops where the helicopter blades initially struck the tree canopy was relatively minor. However, the lower tree damage before that point and where the suspended load struck the trees was more substantial. The damage to the trees indicated that the helicopter had descended at an angle of approximately 37° on a heading of 225° true, before striking a large tree stump. The slung load and rope strop had been released before impact with the ground and were located about eight metres rearward of the main helicopter wreckage. The cargo hook was found in the released position.
- The tail section (Figure 5) of the helicopter was found lying inverted about six metres forward of the main helicopter wreckage. The damage to the tail section indicated that it had been partially damaged by a main rotor blade strike and subsequently separated from the main wreckage due to an impact with a tree. A severed piece of the tail boom upper skin was found about 30 metres to the right of the main wreckage (relative to the direction of the aircraft path through the trees).

- The main rotor assembly (Figure 6) was still attached to the helicopter, with the blades lying together. One blade was severely damaged and there were chordwise crease marks along the blades. The aluminium fuel tank had ruptured, allowing any fuel to drain out. The fuel system was connected to the engine through a fuel strainer, which was found to still contain fuel when inspected at the accident site.

- The helicopter wreckage was removed from the crash site and taken to the Commission’s technical facility in Wellington for further examination. The engine, sprag clutch assembly and upper sheave were removed and taken to a maintenance facility to be disassembled and inspected.
- The lamp filaments in the ‘Low Rotor RPM (revolutions per minute)’ and ‘Low Oil Pressure’ warning lights were found to have been stretched, which indicated that these pilot warning lights were on at the time of impact.
- The engine controls were found in the following positions:
- the ignition switch was in the ‘BOTH’ magnetos position (on)
- the carburettor heat was selected to OFF (pushed in)
- the collective lever was raised near the top of the seat cushion
- the throttle grip had rolled to the closed position.
- The helicopter’s hour meter was found to have been disabled. The reading was 4,734.7 hours, only seven hours more than what had been recorded on 18 March 2016.
- The Pilot’s Operating Handbook and the technical log were required to be in the aircraft but were later found at the pilot’s home.
- The pilot’s phone was found at the accident site. Call records indicated that the pilot had not answered or made any calls or text messages while flying the helicopter on the day of the accident.
- A Garmin 60CSx handheld global positioning system (GPS) had been installed in the helicopter and was found at the accident site. It had been permanently connected to the helicopter’s power supply and configured to switch on with the main battery switch and start to record an ‘Active Log’ file.
- The GPS unit had limited memory capacity for log files, so when the active log memory was full the oldest active log file would be overwritten by the newest. The earliest active log file retrieved from the GPS memory was dated 12 November 2016, and other files covered all flights since, including the accident flight.
Analysis Tātaritanga
Introduction
- While transporting animal carcasses as part of an aerial hunting operation, the helicopter and slung load struck the tree canopy and then the terrain. This section discusses why the helicopter struck the tree canopy and other factors associated with this accident.
- The following analysis also discusses the various factors that could have contributed to the accident, and the regulatory regime around private recreational aviation.
What happened
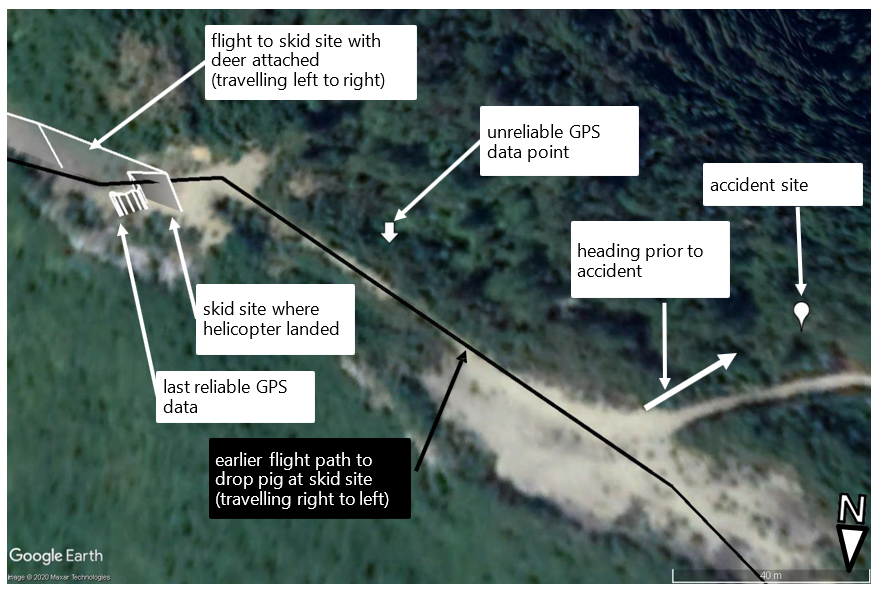
- The data recovered from the GPS (see Figure 4) recorded the helicopter’s position at 10-second intervals. The helicopter approached the skid site from an easterly direction, which was along the rising terrain to the south of the open area. The helicopter then slowed, and landed at the skid site near where the pilot had left the pig earlier.
- The GPS data showed the helicopter was on the ground for approximately 30 seconds. During this period, the pilot would have needed to rearrange the rope strop to attach both animals. The GPS data then showed the helicopter lifting and departing. The last GPS data point, which was approximately between the departure location and the accident site was considered unreliable due to the accident sequence. The unreliability of Garmin GPS data just prior to an accident has been noted in previous investigation reports (Australian Transport Safety Bureau investigation report AO-2011-102, page 68). However, the pilot unlikely conducted any manoeuvres to gain altitude, as this would have resulted in additional GPS data points being recorded. Instead, the path was likely similar to the earlier flight path (see Figure 4) with a final turn onto the accident heading.
- The tree damage indicated that the helicopter was flying approximately south-west immediately before impact (see Figure 4). While it indicated that the helicopter and load entered in close proximity, the final locations of the helicopter and its load were separate. The cargo hook was in the released position, which indicated that the pilot likely jettisoned the load after the load made contact with the tree canopy. This suggests that the pilot was conscious at the time of the accident and was attempting to recover from the situation or minimise the consequences.
- The damage observed on one of the main rotor blades was consistent with the main rotor having ‘coned’ (bending upwards from the mast head more than normal). Similar damage was observed on the other blade, but it was masked by more significant impact damage from a tree. Coning is the result of power being delivered by an engine being insufficient to maintain the rotor blades’ rotational speed under load. If the rotational speed decreases below a critical limit (the low rotor-RPM limit), the situation is unrecoverable. The illumination of the Low Rotor RPM caution light was also indicative of the main rotor being at low RPM.
-
In regard to responding to low rotor RPM, the United States Federal Aviation Administration Helicopter Flying Handbook (FAA, 2012) recommended:
as soon as a low rotor rpm condition is detected, apply additional throttle if it is available. If there is no throttle available, lower the collective.
- If the pilot had experienced low rotor RPM while at a maximum power setting, the only available options to recover the rotor RPM would have been to lower the collective, resulting in a descent, or release the load. An examination of the drive train showed that the engine power setting was low just before impact. This indicated that the pilot was likely responding to a low rotor-RPM event at this time.
- However, the damage to the helicopter and the helicopter’s descent path through the tree canopy meant the investigation could not rule out a low rotor-RPM and subsequent rotor-stall event occurring before the descent through the tree canopy. It was about as likely as not that the low rotor-RPM event occurred as a result of the load becoming entangled with the trees as the pilot attempted to climb above them, which then led to the descent through them.
Possible contributing factors
- The circumstances surrounding the accident suggested that either both the helicopter and the load inadvertently made contact with the tree canopy, or the pilot was unable to maintain sufficient clearance from the tree canopy. The investigation considered what roles the environmental conditions, the condition of the helicopter and the operation of the helicopter may have had in the accident.
Environmental factors
Unfavourable wind
- The wind at the time of the accident was light and variable, but generally it was a tailwind from the south-east. During the Commission’s inspection the day after the accident, late afternoon thermal activity was observed at a similar time to the accident to create short periods of wind gusts estimated at up to 20 knots in strength (based on the Beaufort scale for land, it was termed a ‘fresh breeze’ at 17-21 knots). and from random directions. It was possible that the pilot experienced a sudden tailwind gust during take-off. If a sudden tailwind gust had occurred, it would have reduced the helicopter’s rate of climb in a critical phase of flight. The pilot may not have recognised the cause, but would have seen the effect and likely have increased collective to maintain the height and climb angle to clear obstacles. The extent to which it contributed to the accident could not be determined.
Visual impairment
- At the time of the accident the sun was low on the horizon directly ahead of the flight track. The pilot was wearing a hat at the time of the accident, but did not have sunglasses. It was possible that the pilot’s vision was affected by the sun, and the trees being in shadow limited the pilot’s ability to determine the helicopter’s height above the tree canopy. The extent to which this contributed to the accident could not be determined.
Carburettor icing conditions
- Carburettor icing conditions presented a moderate risk (according to a standard risk chart published by the Civil Aviation Safety Authority of Australia on its website) at the time of the accident.
- The Pilot’s Operating Handbook (RHC, 1979) noted that ice formation was possible in the induction system when the air temperature was between -4° and 30° Celsius and the dew point was 0-15° lower than the air temperature. At 1800 the automatic weather station in Reefton recorded a temperature of 18.9°, with a dew point 4° lower at 14.9° and a relative humidity of 69%.
- Robinson Helicopter Company discussed the risk of carburettor ice in Safety Notice 25 (RHC, 2012). It advised that carburettor heat may be necessary during take-off because the engine responds to power demand from aerodynamic loads rather than a fixed throttle setting, so is more vulnerable to the formation of induction ice. The carburettor heating control was found in the OFF position, but the carburettor was badly damaged and the status could not be confirmed at both ends of the control linkage.
- While the previous flights may suggest that icing conditions were not severe enough to affect flight significantly, the risk that ice formed in the carburettor during the accident flight still existed. Similarly, the perishable nature of the evidence for assessing whether ice formed in the induction system meant that the Commission was unable to determine whether it contributed to the accident.
Condition of the helicopter
- The condition of the helicopter at the time of the accident had the potential to reduce the available power from the engine, and therefore the ability of the pilot to maintain sufficient clearance from the tree canopy. This section discusses the helicopter’s condition at the time of the accident and what effects it may have had.
Engine performance
- The post-accident engine examination found debris in the combustion chambers, which indicated that the engine was likely running when the helicopter collided with the tree stump.
- An independent engineer examined the helicopter’s engine for the Commission and made the following observations:
- the inlet and exhaust valve faces showed evidence of not sealing properly. Excessive carbon deposits had accumulated under the inlet valve heads
- the exhaust valve guide wear was greater than acceptable limits and greater than usual for an engine at the stated life
- the crankcase bearing shells were worn more than expected for the engine life
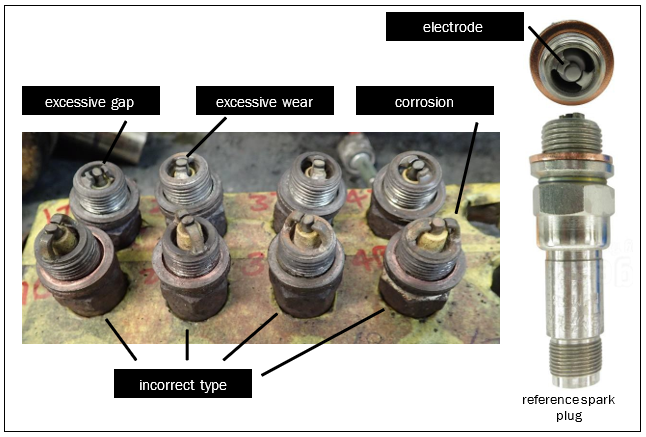
- all spark plugs worked when tested but the electrodes had worn beyond the manufacturer’s allowable limits (Champion Aerospace, 2014). The spark gaps were also excessive (see Figure 7)
- the bottom set of spark plugs was the wrong type for the engine
- both magnetos were working correctly and the timing was correct
- accident debris was present in the combustion chambers
- the overall engine wear suggested it was closer to the end of its reconditioned life than at the start as recorded in the logbook.
- While the helicopter’s engine was likely running just prior to impact, the reliability and maximum power available would have likely been affected by the engine’s poor condition.
- The helicopter had been operating at a similar altitude and weight prior to the accident flight; however, the issues identified may have resulted in the engine not providing the desired power when demanded. The extent to which this contributed to the accident could not be determined.
Fuel exhaustion
- It was unlikely that the helicopter ran out of fuel. The fuel tank ruptured during the crash sequence and the tank was empty. However, fuel was observed in the fuel system and the filter was clean. Witnesses observed the pilot filling the fuel tank before take-off, to what appeared to be the full capacity of the fuel tank. The fuel consumed prior to the accident was estimated from GPS-recorded flight times. This calculation showed that the helicopter should have had about one hour of usable fuel remaining at the time of the accident.
Helicopter loading
- The helicopter was likely to have been operating within normal load limits at the time of the accident.
- The helicopter’s maximum allowed gross weight was 590 kilograms. The last weight and balance data for the helicopter and the weights of the pilot, load, known items on board and calculated fuel remaining were used to determine the approximate weight and balance.
- When the pilot took off from the skid site with both carcasses, the estimated weight was about eight kilograms under the maximum gross weight.
Operation of the helicopter
- There were marks on the ground where the pilot had dragged the second carcass across to the helicopter and hooked it on, but there were no other drag marks leading away from where the helicopter lifted off. This shows that the helicopter had sufficient power available for the pilot to establish a hover high enough to lift the load clear of the ground. However, the pilot still needed to climb the helicopter during the take-off to clear the obstacles along the flight path safely. To achieve this, several techniques were available.
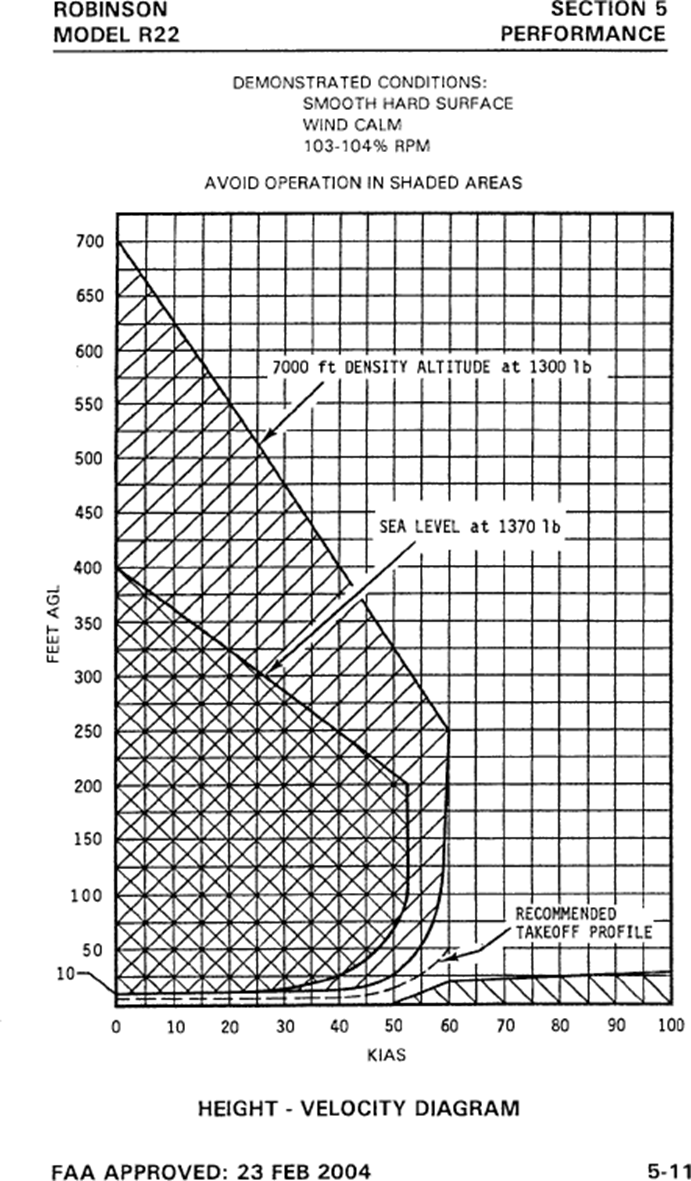
- Robinson Helicopter Company described the standard take-off technique in the ‘Normal’ section of the Pilot’s Operating Handbook as, once a stable hover has been achieved, to “lower nose and accelerate to climb speed following profile shown by height-velocity diagram in Section 5”. (See Appendix 1 for the referred height-velocity diagram.) The diagram showed the helicopter flying level below 10 feet (three metres) above ground level until around 40 knots, at which point a climb could be initiated.
- Another technique was a maximum performance take-off, which was used to clear nearby obstacles in the flight path. The technique, as described in the Principles of Helicopter Flight (Wagtendonk, 1996), involved using the maximum available power to climb at a steep angle. The condition of the engine, as discussed in the previous section, and the limited evidence available meant that it was not possible to determine if the pilot used this technique and did not have sufficient power, or if another technique was used to depart the skid site.
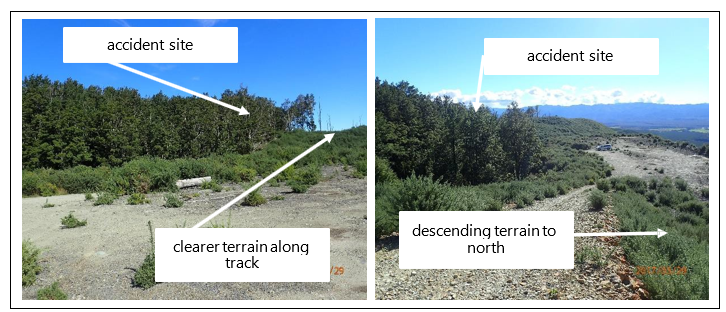
- There are several factors that a pilot must consider when planning and executing a take-off and departure. If a path over clear terrain is available for the helicopter to gain sufficient altitude and airspeed, it provides a better opportunity to land the helicopter safely in an emergency.
- While the exact take-off technique and profile could not be established, the area adjacent to the densely forested accident site was clearer terrain. The clearer terrain also extended in the direction of the helicopter’s track. Clear and descending terrain was also available on a north-easterly track from the skid site. The investigation was unable to determine if the pilot had sufficient time or control of the helicopter to direct it towards a more suitable area before striking the tree canopy.
Helicopter airworthiness and regulatory aspects
Unapproved maintenance
- The CAA permitted an owner/pilot to carry out limited preventive maintenance as listed in Appendix A of Part 43 of the Civil Aviation Rules and in the Pilot’s Operating Handbook. For the accident helicopter, this included the replacement of spark plugs. All work should have been carried out in accordance with the maintenance manual and have been recorded in the aircraft log. The detailed examination of the airframe and the aircraft logbooks revealed the following maintenance issues:
- a dent in the tail rotor blade had not been patched in accordance with the Robinson Helicopter Company R22 maintenance manual
- the battery system had an unapproved modification that included non-aviation components
- the handheld GPS installation was an unapproved modification that included non-aviation components
- the under surface of the main rotor blades had started to delaminate and had an unapproved repair that was not in accordance with any Robinson Helicopter Company maintenance procedures. The bonding strip showed signs of glue failure having already started
- the engine-hour meter had been disabled by modifying the wiring and fitting non-aviation components.
- None of the maintenance issues mentioned above was likely to have contributed to the accident. However, they should have been addressed by a qualified, licensed aircraft maintenance engineer and in accordance with the maintenance manual to ensure that they did not adversely affect the helicopter’s performance.
Airworthiness
- No helicopter flights had been logged in the technical log for at least the previous 12 months, and the hour meter showed it had flown seven hours. The pilot’s most recent logged flight in the helicopter had been on 26 July 2015, but the GPS data indicated that the helicopter had flown since. The GPS logged every flight to the capacity of its memory and it had recorded 25 hours’ flight time in the previous three months. Based on the pilot’s fuel card purchases and an average fuel consumption rate for the helicopter, the pilot had purchased enough fuel for 45 hours’ helicopter flying time in the previous 12 months. The engine had logged 327.7 hours since its last major overhaul and seven in the previous 12 months, but evidence of the actual engine wear indicated many more hours than that.
- For an aircraft to remain airworthy and safe for flight it must be operated and maintained in accordance with the Civil Aviation Rules. A number of factors would have affected the helicopter’s airworthiness:
- the main rotor blades had exceeded their 12-year finite calendar life by eight months
- the engine-hour meter had been disabled
- the technical log had not been used to record flight hours for nearly 12 months since the most recent maintenance
- unapproved maintenance and modifications had been carried out on the helicopter
- the review of airworthiness had expired without a time extension
- the Pilot’s Operating Handbook and technical log were not carried in the helicopter
- a fire extinguisher was not fitted.
Conduct of the aerial hunting operation
- The hunt manager reported that they had introduced the hunter to the pilot, but had not been involved in negotiating any costs or terms of the flight. The hunt manager recalled that the hunter had discussed the flight with the pilot and had agreed to pay for the flight. The amount that the hunter had agreed to pay far exceeded the actual cost of the fuel for the flight. As such, it is likely that the pilot was intending to carry the hunter for reward without holding a commercial pilot licence or operating under an air operator certificate. Under the Civil Aviation Rules a pilot was required to have a commercial pilot licence to take passengers for hire or reward and that operation needed to be conducted under an air operator certificate. These requirements were in place to ensure that a high level of safety was afforded to these operations.
CAA oversight of private aircraft owners and pilots
- The investigation found multiple examples of the pilot/owner operating outside the privileges extended to a private pilot or aircraft owner and not complying with the Civil Aviation Rules. Therefore the investigation broadly examined the CAA oversight of private aircraft owners and pilots.
- The CAA’s regulatory principles for and approach to regulating safety in the civil aviation system were described in its Regulatory Operating Model (CAA, 2014). These principles and approach underpinned the CAA’s strategic direction and underlying policies and procedures.
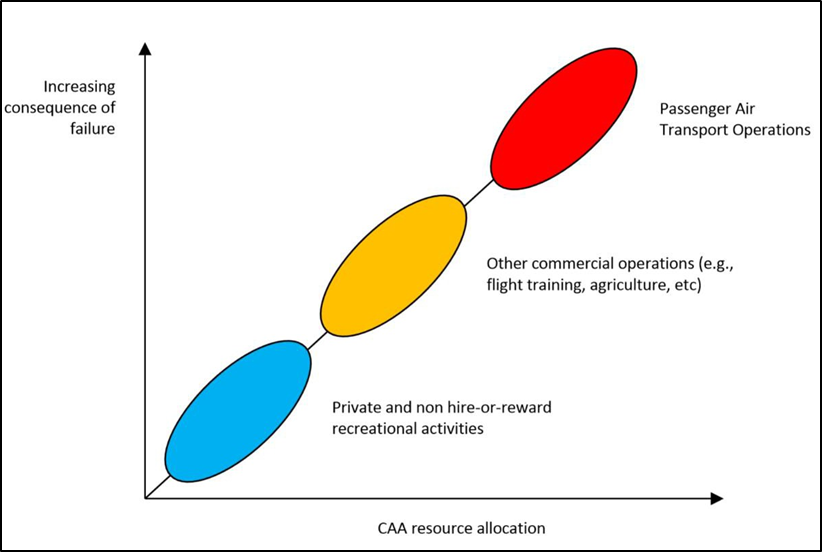
- To implement the Regulatory Operating Model, the CAA directed its activities using a consequence-based approach. It allocated its finite operating resources where it believed the greatest consequences of non-compliance lay – commercial and air transport operations. Fewer regulatory resources were allocated to the non-commercial sector, where the CAA believed there were “lower consequences of failure and impact on the safety of third parties”. This concept is depicted in Figure 9.
- Under this regulatory environment, the CAA relied on non-commercial aviation participants being responsible for safety and complying with regulatory requirements, and to a lesser extent on regulatory and surveillance activities.
-
The allocation of fewer resources to the regulation of the non-commercial sector and a reliance on its participants being responsible for safety and complying with regulatory requirements were broadly in accordance with the International Civil Aviation Organization’s (ICAO’s) International Standards and Recommended Practices – Annex 6, Operation of Aircraft, Part II:
The [ICAO Air Navigation] Commission endorsed the philosophy established during initial development of the Annex that the owner and pilot-in-command must assume responsibility for the safety of operations in non-commercial operations where travel is not open to the general public. In such operations the Standards and Recommended Practices need not be as prescriptive as those in Annex 6, Part I, due to the inherent self-responsibility of the owner and pilot-in-command. The State does not have an equivalent “duty of care” to protect the occupants as it does for fare-paying customers in commercial operations.
- When non-commercial aviation participants do not take self-responsibility for compliance with regulatory requirements, regulatory and surveillance activities are the only controls in place to provide safety assurance. In the non-commercial sector of aviation, this is principally through the Inspection Authorisation system and the Aviation Related Concerns system.
- The Inspection Authorisation system incorporates reviews of airworthiness conducted on a periodic basis by Inspection Authorisation holders. Individuals who hold certificates of Inspection Authorisation are monitored and reviewed by the CAA using a risk-based approach to ensure they perform their inspections in accordance with the CAA’s expectations. The pilot/owner of the helicopter had allowed the helicopter’s review of airworthiness to expire before the accident.
- The Aviation Related Concerns system was based on the public and other aviation participants making submissions to the CAA regarding concerns about aviation matters. Some aviation participants interviewed for this investigation had had concerns that the pilot was not fully compliant with the Civil Aviation Rules. These participants had not submitted their concerns using the Aviation Related Concerns system as they had believed it was the responsibility of the CAA to identify and investigate any irregularities. In addition, they had believed that reporting concerns to the CAA may have reputational impacts on them within the small aviation community. The limitation of the Aviation Related Concerns system within small communities affects its effectiveness in controlling risk.
- The pilot had gained a private pilot licence. It is therefore reasonable to conclude that the pilot understood the privileges granted by the issue of that licence and the requirement to comply with the Civil Aviation Rules. The CAA regulatory and surveillance controls broadly aligned with international standards and recommendations and were based on that premise. The CAA did not detect non-compliance in this instance, nor is it reasonable to expect that it would have. The investigation was unable to determine why the pilot did not comply with the Civil Aviation Rules or the extent to which the non-compliance contributed to the accident. However, this accident serves as a reminder to pilots of their responsibility to operate within the privileges of their licences and in accordance with the Civil Aviation Rules.
Appendix 1. R22 height-velocity diagram