On 2 November 2013 a British Aerospace Jetstream 32 aeroplane taking off from Auckland Airport started to veer left from the runway centreline. The captain was initially able to correct the heading change, but at about 90 knots the turn became uncontrollable. The aeroplane slowly ran off the left side of the runway before the captain could bring it to a stop. No-one was injured and there was no damage to the aeroplane or any airport infrastructure.
Executive summary Tuhinga whakarāpopoto

- On 2 November 2013 a British Aerospace Jetstream 32 aeroplane taking off from Auckland Airport started to veer left from the runway centreline. The captain was initially able to correct the heading change, but at about 90 knots the turn became uncontrollable. The aeroplane slowly ran off the left side of the runway before the captain could bring it to a stop. No-one was injured and there was no damage to the aeroplane or any airport infrastructure.
- The Transport Accident Investigation Commission (Commission) made the following findings:
- the uncommanded turn to the left during take-off was caused by a faulty steering selector
- the defective component within the steering selector could not be determined because of incomplete overhaul records
- the isolated nature of the component failure in this occurrence, and the actions the manufacturer had previously undertaken, meant that additional changes to the relevant maintenance procedures were not warranted.
- The Commission made no recommendation as a result of its inquiry.
- The key lesson identified from the inquiry into this occurrence was:
- prompt action by a pilot on recognising a loss of directional control during take-off or landing will minimise the risk of a runway excursion.
Factual information
The flight
- On Saturday 2 November 2013, a British Aerospace (British Aerospace merged with Marconi Electronic Systems in 1999 to become BAE Systems) Jetstream 32 ZK-VAH (the aeroplane) was being used for scheduled services to and from Auckland. At about midday a replacement crew arrived from Wellington to complete the remainder of the day’s flying. The outgoing crew informed the replacement crew that there were no faults or concerns with the aeroplane.
- At 1455, with 14 passengers on board, the engines were started for a flight to Taupo. A tight turn to the left through about 180º was required in order to leave the terminal parking area. The captain said a combination of full nose wheel steering, asymmetric power (a difference in power or thrust between the left and right engines) and asymmetric braking was required to turn the aeroplane. The aeroplane was then taxied to runway 23 Left (see Figure 1).

- At about 1501 the aeroplane was given clearance to take off. The weather was fine with a light crosswind from the left. The captain said that the power was increased progressively on both engines and the aeroplane accelerated normally. She kept the aeroplane on the runway centreline initially by the use of nose wheel steering.
- After the first officer had made the standard ‘70 knots’ (a knot is a speed of one nautical mile per hour, equal to 1.85 kilometres per hour) airspeed check call, the captain transferred directional control from the nose wheel steering to the rudder pedals. At about this time the crew noticed a slight swing to the left. This was corrected by applying some right rudder. The aeroplane subsequently started to veer left again. The captain was unable to counter the second veer to the left using full right rudder, and the aeroplane drifted towards the edge of the runway.
- The captain called “stopping” as she closed both power levers. She then used a combination of nose wheel steering and asymmetric braking to try to keep the aeroplane on the runway. The first officer relayed the “stopping” call to the control tower during this time. The aeroplane came to a stop in the grass about 15 metres (m) from the runway (see Figure 2).
- The engines were shut down and the passengers kept on board until emergency services arrived. No-one was injured and there was no damage to the aeroplane or ground installations as a result of the runway excursion (a runway excursion occurs when an aeroplane leaves the runway surface, either at the end of the runway (an overrun) or off the side (a veer-off)). The aeroplane was later towed to a hangar to await the arrival of Commission investigators.

Personnel information
- The captain held an air transport pilot licence (aeroplane) issued in 2007 and a current class one medical certificate. She had obtained her Jetstream 32 type rating in November 2005 and joined the operator in July 2012 as a captain. At the time of the occurrence she had accrued 5,131 flight hours, including 2,212 hours on the Jetstream 32.
- The captain’s previous line check had been on 18 June 2013. She had flown 22 hours in the preceding 30 days and 2.2 hours in the preceding seven days. She had had a rest day on the day before the occurrence and said that she had been well rested and fit to fly on the day of the occurrence.
- The first officer held a commercial pilot licence (aeroplane) issued in 2008, and a current class one medical certificate. He had obtained his Jetstream 32 rating in September 2012, soon after joining the operator. At the time of the occurrence the first officer had accrued 1,250 flight hours, including 320 hours on the Jetstream 32.
- The first officer’s previous line check had been on 17 December 2012. He had flown 32 hours in the 30 days preceding the occurrence and 10 hours in the preceding seven days. The two days prior to the occurrence had been free of duty. He said he had been well rested and fit to fly on the day of the occurrence.
Aircraft information
- The Jetstream 32 was a development of the Jetstream 31 that had been first certificated in 1982. It was powered by two Garrett AiResearch (later Honeywell Aerospace) TPE331 turbo-propeller engines and capable of carrying a two-pilot crew and 19 passengers.
- The aeroplane had been manufactured in the United Kingdom in 1992 and flown for seven years in the United States before being sold to an operator in New Zealand and then to one in Australia. In June 2012 the aeroplane had been returned to New Zealand, registered as ZK-VAH and joined with three other Jetstream aeroplanes in the operator’s fleet (in October 2014 the operator ceased all operations).
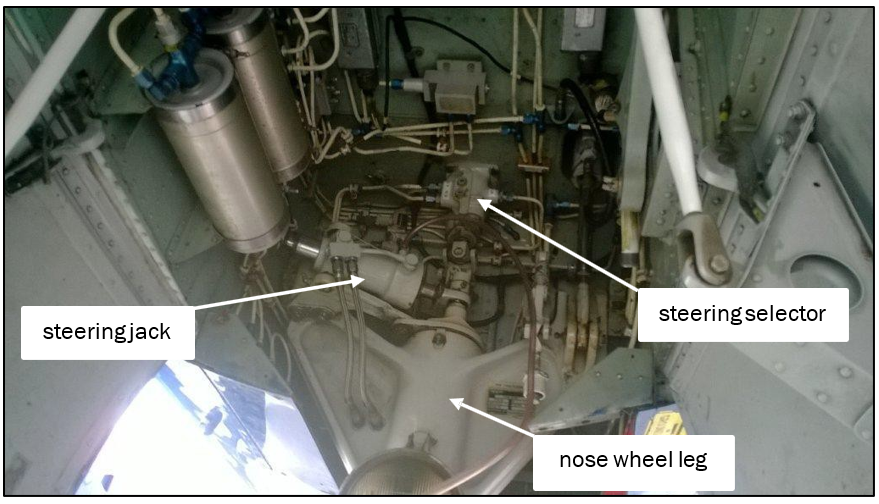
- Nose wheel steering was controlled through a tiller (handle) located on the left side of the cockpit next to the captain’s seat. A mechanical linkage connected the tiller to the steering selector, which directed hydraulic pressure to a steering actuator mounted on the nose gear housing (see Figure 3). The actuator turned the nose wheel. A feedback loop ensured that the nose wheel position matched the tiller movement and position.
Maintenance defect history
- On 8 February 2013, 10 months before the incident, a pilot had reported that during take-off the aeroplane “yawed [turned] left significantly”. Full right rudder had been used to keep the aeroplane aligned with the runway. During an examination of the aeroplane a nose wheel axle nut was found to be cracked and the steering jack determined to be faulty. Those items were replaced. No other fault was found with the steering system, so the aeroplane was returned to service. At the time it had flown 18,724 hours and completed 29,646 landings (cycles).
- On 9 August 2013, three months before the incident, a crew had reported that during take-off the aeroplane drifted left. Loose play was found in several components of the nose wheel steering system. The steering jack was bled of any trapped air and the main wheel brake units were swapped around. The flight deck steering handle was also replaced. Testing was unable to replicate the problem and the aeroplane was returned to service. Pilots were asked to report any further concerns. On 18 October 2013, two months before the incident, with no further problems reported, the defect was recorded as rectified.
- On the day of the occurrence, 2 November 2013, the aeroplane had accrued 18,909 flight hours and 29,978 landings.
Recorder information
- The aeroplane was fitted with a flight data recorder that recorded 11 parameters, including the heading, airspeed and the torque and propeller speed of both engines. The recorder was removed and sent for downloading of the data. The cockpit voice recorder was not accessed.
- The data showed that the first veer to the left occurred as the aeroplane speed approached about 70 knots. The second veer left started at about 90 knots. The engine power was reduced to flight idle at about 100 knots.
- The data showed that power was increased simultaneously on both engines for the take-off and that there was no asymmetric power as the aeroplane accelerated. After the captain commenced the rejected take-off, more reverse power was applied to the right engine than to the left engine as the captain attempted to turn the aeroplane back to the right.
- Aerodrome ground surveillance data showed that during the attempted take-off the aeroplane maintained the runway centreline for about 200 m before starting to move left. The move to the left was corrected for about 100 m and the aeroplane was returned to near the centreline, where it stayed for about the next 200 m. The aeroplane then veered increasingly to the left and ran off the runway about 600 m from the start of the take-off roll.
Testing of nose wheel steering system
- An initial examination of the aeroplane identified no engine, main undercarriage or brake system anomalies. The focus of the investigation then moved to the nose wheel steering system.
- The nose wheel was placed on a greased plate to enable it to turn easily while it supported a normal load. The hydraulic system was then pressurised. Repeated movements of the nose wheel tiller were unable to produce an uncommanded left turn. No abnormalities were identified by this test.
- Samples of hydraulic fluid were taken for analysis, including from the hydraulic line close to where the steering jack and steering selector were located. The samples were subjected to a spectroscopic analysis, which confirmed that the fluid was of the correct type with no anomalies.
- The steering jack and steering selector were then removed for detailed examination by two different approved overhaul facilities in the United States.
- A functional check and disassembly of the steering jack found no fault that may have contributed to the uncommanded left turn.
- The overhaul facility that examined the steering selector identified two related faults during testing. Following “full counter-clockwise input to the selector, upon release the valve would stick and allow fluid to continually flow from [a] port” (this was the port that commanded a left turn); and “excessive internal valve leakage was observed”. The overhaul facility then disassembled the selector and found that the faults were caused by ‘spring boxes’ being out of adjustment. The spring boxes balanced the hydraulic pressure between the control pressure commanded by the pilot and the resultant steering forces from the nose wheel position.
- The overhaul facility stated that because the steering selector locking tabs were still intact before disassembly, the misadjustment “must have been directly related to the springs”. These faults would direct hydraulic pressure to go to the left-turn side of the steering actuator. The overhaul facility further commented in its report that “the probable cause of the spring boxes being out of adjustment is due to fatigue of the spring” and that from its experience this was “an isolated incident”.