TAIC final report into the runaway of nine wagons finds wagons were not properly secured and rolled back onto a locomotive. Moderate damage but no injuries. Findings include breakdowns in communication, training, and safety culture. Recommendations regarding shunt staff training, unsafe practices and under-reporting, and remote-control equipment.
Executive summary Tuhinga whakarāpopoto


What happened
- At about 0125 (times in this report are in New Zealand Daylight Time (Universal Coordinated Time +13 hours) expressed in a 24-hour format) on 23 January 2025, a KiwiRail scheduled train service and two rail crew arrived at Port Otago. They needed to position 25 wagons into the rail marshalling area (consisting of four storage roads for rail wagons) for the trans-shipping (the movement of containerised freight on to a ship) of its containerised freight.
- The crew placed the first nine wagons into road 1 and repositioned the locomotive to connect on to the next wagons for road 2.
- The crew were having difficulty connecting the locomotive’s coupling system to the wagons, and were unaware that the first set of wagons previously placed in road 1 had started to move and was rolling towards their location.
- Once the connection was made between the locomotive and the first wagon, the rail operator connected the air hoses for the operation of the train’s brake system.
- Just as the rail operator exited from between the locomotive and the first wagon, the wagons from road 1 collided with the locomotive.
- No one was injured and the locomotive and wagon sustained moderate damage.
Why it happened
- Limited radio communication between the crew led to approved securing processes for wagons not being followed or confirmed, and therefore the brakes on the wagons in road 1 released.
- The crew did not secure the wagons correctly. Correct procedure required the residual air to be exhausted from the air-brake pipe, hand brakes (the device that secures the wagon’s brakes to wheels, limiting movement) to be applied to three wagons and a wooden chock (timber wedge block to stop rail vehicles’ wheels from rolling) to be placed between the wheel and rail interface (the surface location that connects the wheels on the rail vehicle to the rail head).
What we can learn
- Clear and concise communication between train crew is crucial when undertaking safety-critical work.
- Adequate training and the correct application of non-technical skills is critical when work practices change, allowing the crew to recognise and apply appropriate safety controls to manage risk.
- Strong safety leadership, a just culture, assurance testing and regulatory oversight ensure that safety-critical systems are adequately managed.
Who may benefit
- Rail personnel and organisations that conduct safety-critical operations may benefit from the findings in this report.
Factual information Pārongo pono
Background
- The Y20 shunt (the number KiwiRail uses to identify the job and crew) (the train) operates up to five times a day, moving container wagons between the Dunedin rail yard and the Port Otago rail storage facility, located in Port Chalmers (see Figure 3).

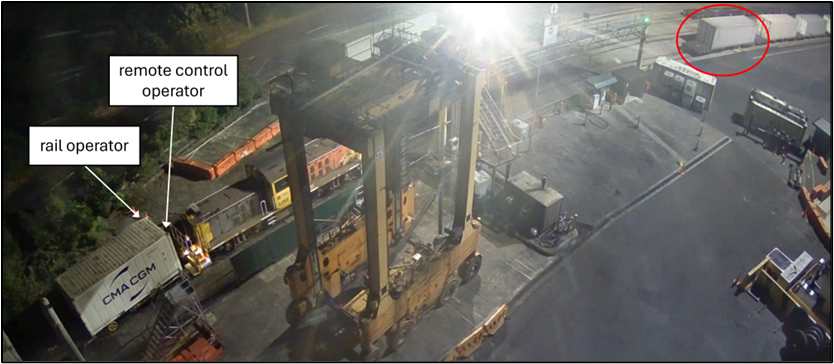
- The Y20 shunt operation requires a two-person crew: a remote-control operator (RCO) and a rail operator (RO).
- The RCO uses a remote-control pack to remotely move the train forwards and backwards and to apply the train’s brakes during shunting operations within rail yards (see Figure 4).

- The freight marshalling yard consists of four stabling (the area to hold rail wagons) roads (see Figure 3 above). When conducting shunts, the RO informs the RCO of the number of wagons (a rail vehicle used to move freight and containers) to be moved into each stabling road. The RO is also responsible for applying the wagons’ hand brakes, removing the air from the braking systems and securing wooden chocks under the wagons’ rear wheelsets to prevent them moving.
Narrative
- At about 2300 on 22 January 2025, a two-person crew, consisting of an RCO and an RO) arrived at the Dunedin rail yard to begin their shift.
- The RCO had just returned from leave and was on their first shift back. They reviewed the new rule-change documentation, then obtained the daily information bulletin (DIB) (a paper document that outlines the day’s rail movements and additional information about a section of railway) as a part of their prestart book-on procedure. The DIB outlined rail operations on the section of track between Dunedin and Port Otago, about 11 kilometres (km) north of Dunedin at Port Chalmers.
- The RCO met with the RO, discussed the work plan and held a prestart safety meeting with the Dunedin rail operations team leader.
- At 2330, the RCO carried out safety function checks (a series of safety checks to ensure the train is fit to operate) on the remote-control pack and locomotive.
- The RCO and RO then attached 25 wagons to the shunt locomotive (DSG 3251) before getting into the locomotive cab for the journey to Port Otago.
- The RCO called train control (controls the movements of trains and rail vehicles on the rail network) on the locomotive’s radio to request authority to proceed from Dunedin to Port Otago. At 2353, train control placed signals at proceed, and the train with 25 wagons departed for Port Otago.
- At 0120:31, the train arrived at Port Otago to place 25 wagons into the freight marshalling yard, ready for the containers to be removed.
- The RO disembarked from the locomotive cab and took up position on the ground, approximately 2 metres (m) away. The RCO also disembarked from the cab and entered the locomotive’s front-right refuge area (the safe ride position to stand in when moving in a rail yard).
- The RCO released the brakes on the 25 wagons and moved the train into road 1 with the intention of stabling the first ten wagons.
- Over the portable radio, the RO advised the RCO that they had counted off the required wagons and asked the RCO to stop the train.
- The RO then alerted the RCO that they may have miscounted the wagons and that there could be only nine instead of ten.
- The RCO directed the RO to uncouple the remaining wagons and advised that if they were short a wagon, they could get it on the next movement into road 2.
- At 0121:27, the RO lifted the wagon air taps (controls the flow of air for a train’s braking system) at the cut-off point (when the wagons are split from their connection) and instructed the RCO to move the train forward to uncouple the connection between the wagons.
- The RCO pulled the wagons down to the end of road 1, where the RO confirmed that there were only nine wagons, not ten as planned.
- The RO stabled (held a wagon or rail vehicle in a stationary position within a rail road) the remaining 16 wagons and applied one hand brake on the leading end wagon.
- The RO then walked forward to set the track points (the mechanical system that can direct rail vehicles on to different rail roads) for the locomotive to enter road 2 in the next rail movement. The RCO and RO communicated over the radio, but they didn’t come to a clear understanding of who was to complete the stabling process for the wagons in road 1.
- As the RCO applied the wagon and locomotive brakes using the remote control pack, they unintentionally moved the brake valve tap (the device fitted to a wagon or rail vehicle to control the air from a train’s braking system) of the first wagon with their hand. This caused an 11 kilopascal (kPa) spike of air pressure to move down the wagon brake pipe, resulting in the release of all the wagons’ brakes.
- Neither the RCO nor the RO were aware that the brakes had been released.
- At 0125:56, the RCO informed the RO that they had lifted the brake valve taps and cut off the locomotive from the wagons.
- The RCO then positioned the track points at the end of road 1 to enter road 2 and travel back towards the RO and the remaining 16 wagons.
- As the RCO travelled down road 2, they radioed the RO to ask whether the next movement would be for 11 wagons. This radio call went unanswered.
- On arrival back at the connection area, the RCO and RO both attempted to couple the remaining wagons to the shunt locomotive.

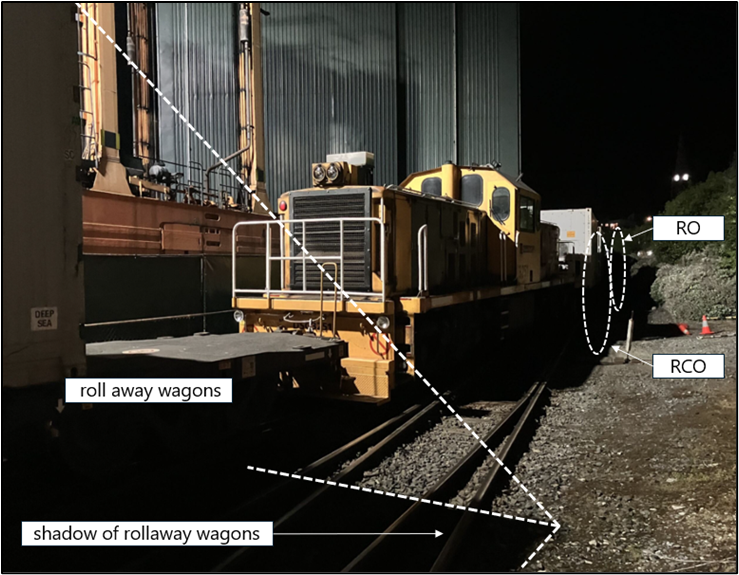
- At 0128:38, the nine wagons on road 1 started rolling down the descending gradient towards the crew’s location (see
Figure 5). - At 0129:28, the RCO tried to connect the remaining 16 wagons to the shunt locomotive, but because of the curvature of the track the wagon coupler connection would not align and lock in place. At the same time, the nine unsecured roll away (the term used for rail vehicles moving when they are unattended) wagons had moved approximately 15 m towards the crew (see Figure 6).
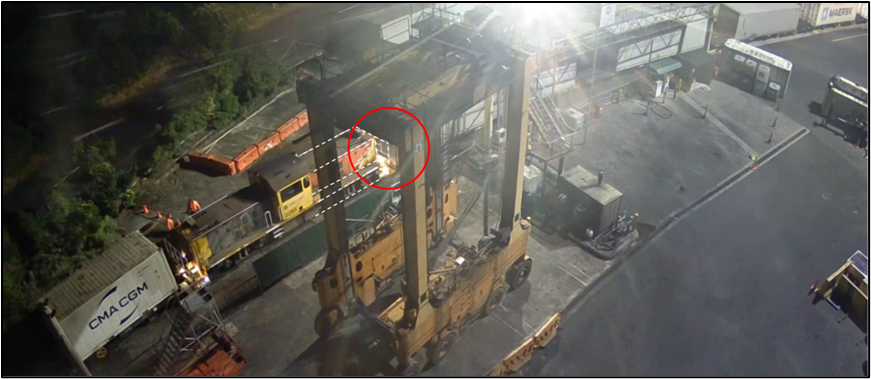
- At 0130:20, the RCO advised the RO that they had successfully coupled the locomotive to the wagon’s coupler. The RO then went between the wagon and locomotive to join the two air-brake hoses together. The crew were still unaware of the wagons slowly moving towards them (see Figure 7).

- After joining the hoses, the RO moved out from between the wagon and the locomotive. About three seconds later, the RCO noticed a large shadow moving towards them. The RCO yelled at the RO, “get out of the way” and applied the locomotive’s emergency brake using the remote-control pack (see Figure 8).
- At 0130:30, the nine wagons totalling 472 tonnes (t) collided with the front of the locomotive and remaining 16 wagons. The impact caused the locomotive to be pushed backward approximately 1.2 m at a speed of 3 kilometres per hour (km/h) (see Figure 9).
- The force of the collision caused the locomotive and wagon buffer that were previously connected to the remaining 16 wagons to part and separate by approximately 1 m (see Figure 10).

- The crew were uninjured. They stabled the wagons and locomotive before calling the KiwiRail manager. The manager attended in the capacity of Rail Incident Coordinator (RIC) and started an initial investigation.
Personnel information
- The RCO was employed by KiwiRail in September 2009. They completed the theory and on-job training, achieving full final certification on 11 December 2018. A safety observation (a practical on-job observation completed every eight months by a certified rail assessor to assess whether a rail worker is competent to retain their current licence to operate) assessment was completed on 22 May 2024, and the RCO was deemed competent.
- KiwiRail’s drug and alcohol testing of the RCO after the incident produced a negative (clear) result.
-
The RO was employed by KiwiRail in November 2023. They completed the theory and on-job training, achieving full final certification on 11 August 2024. A safety observation assessment was competed on 2 December 2024, and the RO was deemed competent.
-
KiwiRail’s drug and alcohol testing of the RO after the incident produced a negative (clear) result.
Train/vehicle information
- DSG 3251 is a diesel-electric locomotive used for remote-control shunting operations within freight marshalling yards and transferring freight short distances on the main line. Built by Toshiba Corporation, these locomotives were commissioned into New Zealand’s rail service between 1981 and 1983.
Recorded data
- The train’s locomotive was fitted with a Tranzlog data recording system (this system records and stores operational data from the locomotive). The relevant data was obtained by the Commission and used in this investigation.
Site and wreckage information
- The combined weight of the nine wagons involved in the collision was 472 t, and they were approximately 126 m long.
Tests and research
- Commission investigators attended KiwiRail’s Hillside workshop in Dunedin to test the train’s brake functionality and remote-control operations.
- Commission investigators observed the testing carried out by KiwiRail and obtained the results, including:
- function testing of the remote-control pack
- air-brake and mechanical testing of the wagon’s braking system
- emergency train-brake stop button
- radio call testing to train control.
Organisational information
KiwiRail Holdings Limited (KiwiRail)
- KiwiRail is a New Zealand state-owned enterprise. It operates trains and rail vehicles, controls rail movements on the national rail network and maintains the railway infrastructure as the rail access provider.
Previous occurrences
Uncontrolled roll away data
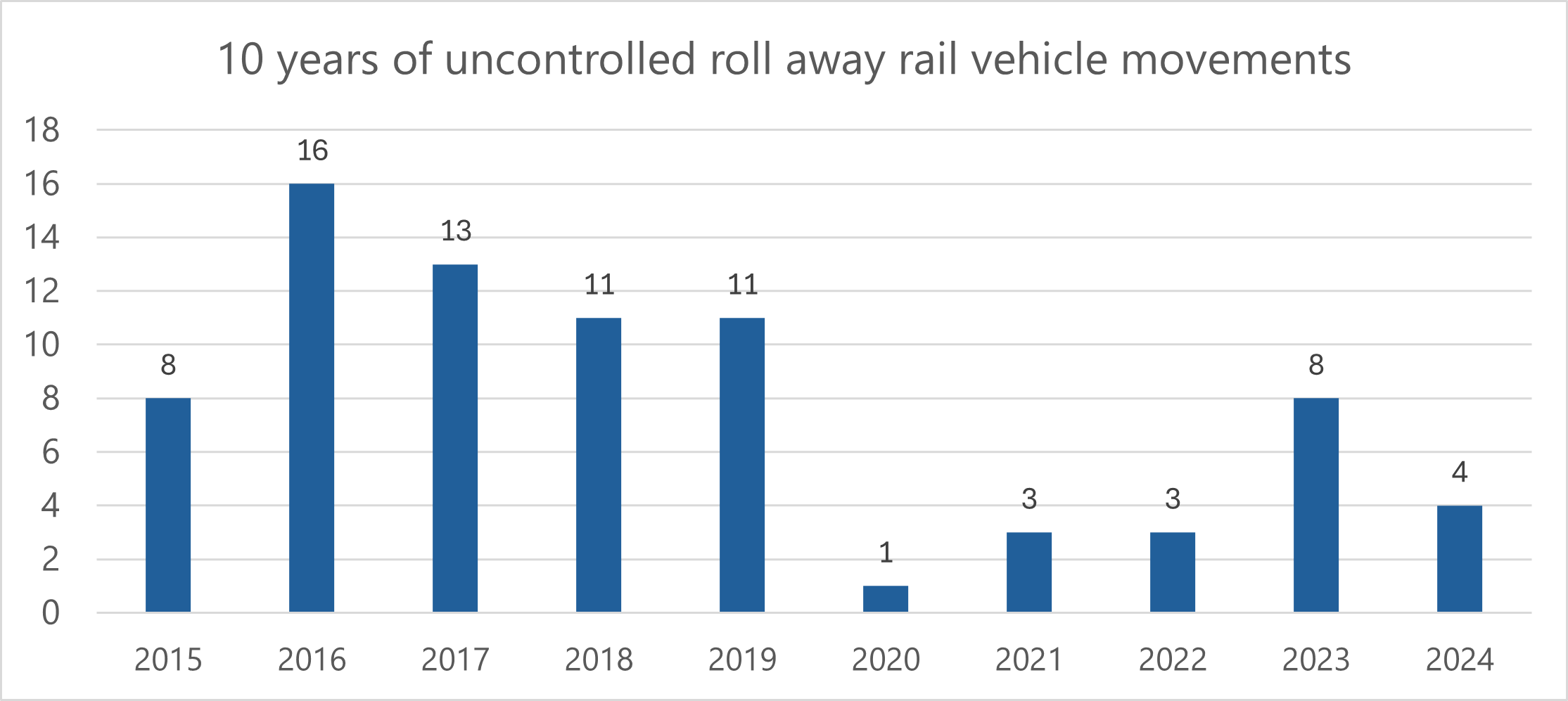
- The Commission obtained KiwiRail’s uncontrolled roll away data, for 2015 to 2024 (see Figure 11).
- The locations of the uncontrolled roll away occurrences are shown in Figure 12.

RO-2021-105
- On 25 September 2021, a remote-controlled shunting locomotive and wagon rolled off the wharf into the sea at Picton. The remote-control operator was distracted and did not maintain awareness of the movement.
- The Commission’s investigation (Transport Accident Investigation Commission, 2023) identified several contributing factors, including:
- lack of engineering protections
- inadequate support for newly qualified staff in safety-critical roles.
- The Commission made the following recommendations.
- That KiwiRail ensures that safe working procedures are in place to manage site-specific risks associated with staff undertaking shunting activities. (Recommendation 004/23)
- On 26 April 2023, the Commission recommended that KiwiRail installs a more effective engineering solution to prevent rail movements entering the Picton rail linkspan without authorisation. (Recommendation 005/23)
-
KiwiRail took the following action:
This recommendation is accepted by KiwiRail, and it is being implemented. We will confirm a timeline for these actions to be completed with your staff at our regular relationship meetings. In addition to our response of 22 February 2023, a KiwiRail Industrial Council (KIC) Safer Shunting working group has been set up which meets regularly. The purpose of this group is to ensure that KiwiRail improves the shunting safety outcomes within KiwiRail using people v plant principles. Works collaboratively with our union partners using High Performance High Engagement (HPHE) principles. To develop a future state shunting strategy that is aligned to current and new assets and the RNIP funding model. Understand the risks associated with shunting and manage these risks, so far is reasonably practicable
In line with KiwiRail’s response of 22 February 2023 to the draft recommendation, as part of the IREX project a preferred option has been identified for a series of automatic derailers that will be interlocked with the linkspan structure. This recommendation is accepted and the anticipated time line for completion is end of 2024.
RO-1998-115
- Train 823, with a rake (a number of rail wagons attached to each other) of 18 empty coal wagons, was journeying from Lyttelton to Ngakawau. It stopped, and the locomotives were detached for servicing. Shortly after, the wagons began an uncontrolled movement eastward along a downhill grade toward Christchurch. They crossed two level crossings before they could be stopped.
- The Commission issued the following recommendations(Transport Accident Investigation Commission, 1999).
- Procedure enforcement: rigorously apply and audit compliance with rules for securing detached wagons before uncoupling locomotives (Recommendation 103/98)
- Operational change: discontinue or critically revise the practice of detaching wagons and leaving them on the main line without secure protections (Recommendation 102/98).
-
Tranz Rail took the following safety actions:
At Middleton instructions have been issued to ensure the normal method of handling trains requiring locomotive servicing is to berth them on other than the main line. Tranz Rail will continue its ongoing education od assuring compliance with all the rules and operating instructions including the securing of detached wagons left on the main line.
Analysis Tātaritanga
Introduction
- On 23 January 2025 at 0125, a scheduled train shunt service arrived at Port Otago. During the positioning process, nine wagons stabled in the freight marshalling yard rolled away uncontrolled. They collided with the locomotive while the crew were connecting the next set of wagons.
- The following section analyses the circumstances surrounding the event to identify those factors which increased the likelihood of the event occurring or potentially increased the severity of its outcome. It also examines any safety issues which have the potential to adversely affect future operations.
Securing rail wagons
- Stabling rail vehicles and securing them in a safe manner when not in use is critical for safety and operational reasons. Unsecured wagons can move in an uncontrolled manner owing to gravity and vibration. This poses serious risk to workers, equipment and infrastructure, especially in rail yards with gradients or busy operations.
- In KiwiRail’s shunting operation, the risk of a roll away was mitigated by two essential procedures that staff were expected to adhere to: first, applying a full service to the air brakes; and, as a secondary measure, applying park/hand brakes. Without compliance with either of these procedures, a roll away was likely to occur.
- To stable and secure a rail vehicle, KiwiRail has rules and procedures in place that outline the sequential steps to be taken to effectively mitigate the risk of an uncontrolled rail-vehicle movement (see Figure 13).
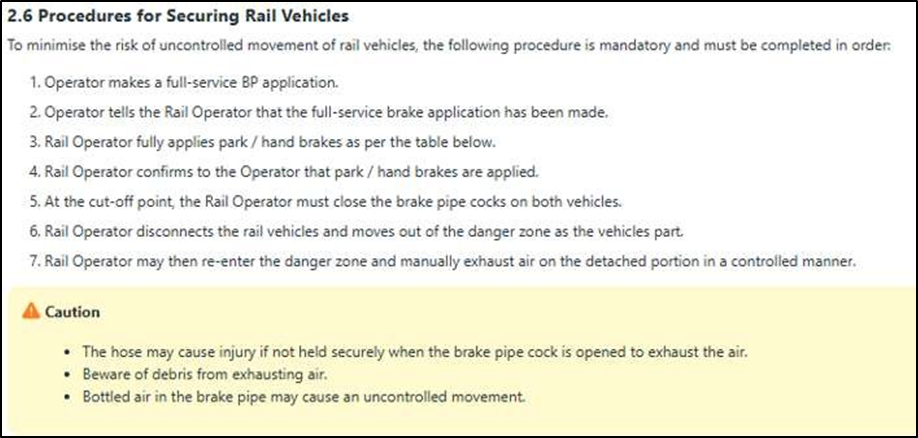
- In this incident, neither step 1 (full-service brake pipe application), step 3 (park/hand brake application) nor step 7 (manually exhaust the air) occurred. In addition to the specified rules and procedures, there was a local instruction that required the placement of a wooden chock under the rear wheel of each wagon. This too was not completed
- The only step taken to stable and secure the nine wagons was applying the full-service train brake. This process was compromised at the time of the brake application (see below).
Why was the full-service brake application ineffective?
Train air-brake systems
- A rail vehicle's air-brake system is a critical component in maintaining operational safety, both when the train is in motion and when it is stationary. The air-brake system has been in use since 1860, and has underpinned railway safety around the world.
- The air-brake system operates by using compressed air to move mechanical parts to apply and release brake blocks to the wheels of rail vehicles. While it plays a critical role in rail-vehicle safety, the system is vulnerable to failure if correct procedures are not followed.
- The key features of the air-brake system are outlined in Figure 14.
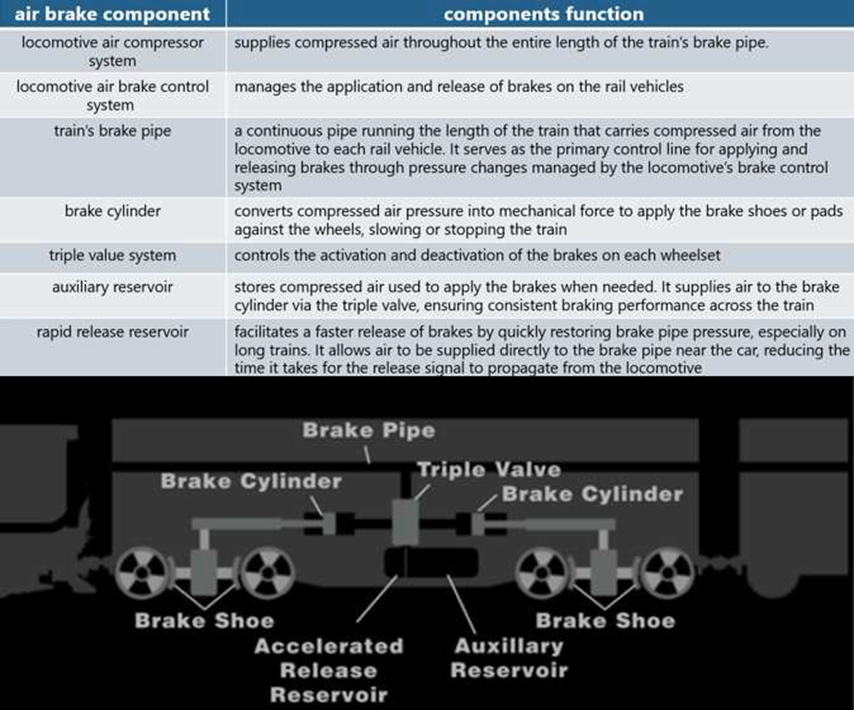
- The air-brake system works primarily by controlling air pressure throughout the length of the train. The brake pipe is continuous and is connected between each wagon by a flexible brake-pipe hose that allows continuous air flow to the end of the train. (see Figure 15).

- To allow the train to roll freely with the brakes released, the brake pipe must be pressurised to 550 kilopascals (kPa) (the air pressure required to release the braking system). Figure 16 depicts, in light blue, the locomotive’s compressor and brake pipe fully charged with the brakes in a release position on the wagon.

- To apply the train’s brakes, the locomotive engineer reduces the air pressure in the brake pipe, using the controls in the cab or on a remote-control pack.
- This brake-pipe reduction in air pressure activates the triple-valve system on each wagon, with the level of braking corresponding to the amount of reduction of air pressure from the brake pipe.
- The air is released from the train’s brake pipe into the atmosphere from the front of the locomotive, while the auxiliary reservoir on each wagon moves air into the brake cylinders, moving the brake rigging (the equipment that attaches to the brake cylinders and wagon to allow the brakes to function) to apply the brake shoes on to the wagon’s wheels.
- Figure 17 depicts, in dark blue, a reduction of air pressure from the brake pipe, which applies the brakes to the rail vehicles wheels.

- Once the desired level of braking has been achieved, the locomotive engineer or RCO can release the brake. This initiates the process of recharging (the period for the brake pipe to replenish the air pressure back to 550 kPa) the brake pipe with air pressure back up to 550 kPa, allowing the train’s wheels to roll freely.
‘Air pressure spikes and bottling the air’
- To achieve an effective brake application, the air must be released into the atmosphere, and the brake-pipe pressure must become equalised throughout the length of the train. This process is called ‘equalisation’ and the longer the train, the longer the equalisation process will take.
- The yellow line in Figure 18 depicts the air releasing but not yet being equalised throughout the train. If the brake pipe has not reached equalisation and the air flow is interrupted from full release, it can cause an air spike (a rise in air pressure back through the brake pipe) to be forced back through the brake pipe against the releasing air flow from the front of the locomotive.

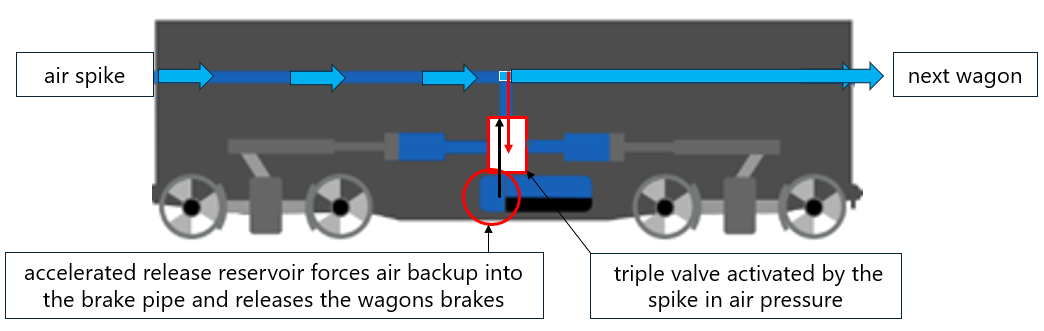
- A rise in air pressure against the releasing air sends a false signal to each of the wagon’s triple valves, resulting in the brakes being released. Once the first wagon is affected, it is accelerated when the auxiliary reservoir releases pressurised air back into the brake pipe. This causes a cascading effect that progressively releases the brakes on each subsequent wagon (see Figure 19).
- This is exacerbated when the air in the wagons brake pipe is closed off by moving the brake pipe tap to the closed position, this is called ‘bottling the air’ (when air pressure is left in the wagon’s brake pipe and the shut off taps are closed).
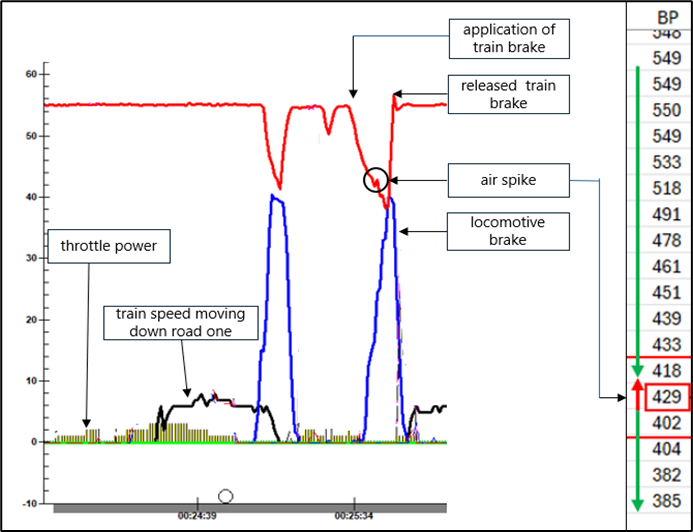
- In this incident, the locomotive’s Tranzlog data recorded an 11 kPa rise in brake-pipe pressure while the RCO was applying the brakes to the nine wagons on road 1. It is virtually certain that this pressure spike and the bottled air triggered the release of the air-braking system (see Figure 20).
- Had the air in the train’s air-brake pipe equalised along all nine wagons, the spike in air pressure would not have occurred and the wagons in road 1 would have held in place for a period of time (see Figure 21).

Training of rail personnel
Safety issue 1: The training delivered by KiwiRail did not provide the shunting crew with sufficient knowledge about the air-brake system and how to manage its associated risks. This reduced the crew's ability to identify and respond to a potential release of the air-brake system in stabled wagons.
- Training staff in safety-critical operations is essential for the safety of personnel and to maintain the integrity of safe systems of work, where failure can lead to serious harm or loss of life.
- Effective training ensures that personnel fully understand operational risks and how to manage them, increasing the likelihood that established procedures are followed. It also reduces the likelihood of incidents or accidents caused by human error, such as complacency or ineffective communication.
-
KiwiRail’s theory training for new employees covers KiwiRail’s Operating Rules and Procedures (the rules), including the seven-step process for stabling and securing rail vehicles (see Figure 14 above).
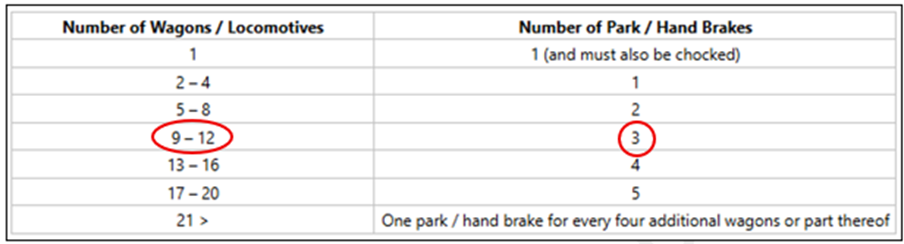
- In addition, KiwiRail’s hand-brake ratio table specifies the number of hand brakes that must be applied per number of wagons to safely hold them in place for more than one hour (see Figure 22). The nine wagons that were involved in the incident should have had three hand brakes applied, but none had been used.
- The Commission found from interviewing the crew that during their communications the RO and RCO did not verbally confirm with each other what tasks each was doing and whether those tasks were complete. A breakdown of clear radio communication resulted in a misunderstanding and led to the RO assuming the RCO had applied the hand brakes, which they hadn’t.
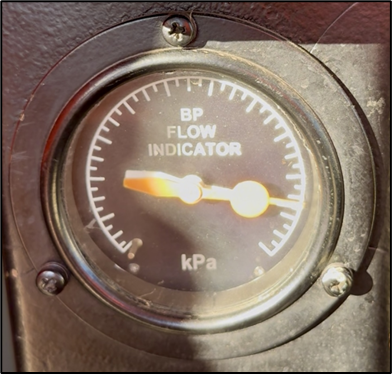
- KiwiRail’s locomotive fleets are equipped with air-flow gauges in the cab to assist locomotive engineers in determining when equalisation has been achieved. This is when the white and orange needles in the gauge align with each other and stop moving (see Figure 23).
- The RCO’s remote-control unit did not include any visual indicators to assist the RCO determine when brake-pipe reduction had fully equalised. In the absence of such aids, the RCO had to rely on their judgement and experience to estimate when equalisation had occurred, and the stabling process could begin, and the air tap could be lifted. This increased the likelihood of incomplete equalisation and an unintended release of air.
- Commission investigators conducted two tests to record the time for nine wagons to reach equalisation. They received results of 14.3 seconds (s) and 15.4 s.
-
The training provided to staff in relation to securing rail vehicles did not include air-brake equalisation requirements, or the time needed for wagons to reach equalisation before the stabling process could be initiated. Additionally, the Commission found that KiwiRail’s training did not cover the following areas:
- the risks of not reaching equalisation of air-brake application and bottling air in the wagons
- the consequences of an air spike on the air-brake system
- why a full-service air-brake application must be used when stabling wagons.
- Without learning and understanding these fundamental elements of the air-brake system, rail staff could not be expected to understand all the risks associated with stabling wagons and why the correct procedure needed to be followed.
- In this incident, the RCO was not aware that they had moved the tap on the wagon as air was still equalising within the brake pipe. Lifting the tap too early caused the system to release the applied brakes, leaving the rake of wagons unsecured when the RCO detached the shunt locomotive.
- Had adequate training been provided to staff on equalisation timings for air-brake applications, it is likely the RCO would have identified that equalisation had not yet occurred before uncoupling the locomotive from the wagon rake.
Safety culture
Safety issue 2: The safety culture in KiwiRail’s shunting crew at Port Otago is poor with a high level of acceptance of rule violation and at-risk behaviours. This increases the likelihood of accidents and incidents.
- The Commission found that this incident occurred as a result of non-compliance with rail-vehicle stabling procedures.
- Compliance with procedures is an example of an administrative control, which is less effective than engineering controls, substitution or elimination. Administrative controls are vulnerable to human error and non-compliance and therefore should not be solely relied upon to keep a system safe.
- Compliance with procedures is known to be affected by several interacting factors (Kuiper, et al., 2022). These factors differ depending on the context, but generally non-compliance is common when:
- the benefits of non-compliance are perceived as higher than the benefits of compliance
- potential punishment is not perceived as certain and severe
- other people are seen to not comply
- the rules and the authorities are not perceived as legitimate
- the rules are not easy to comply with, and the person lacks the ability to comply
- the person has the opportunity not to comply.
- Compliance is also more likely when underpinned by a strong safety culture. The Commission found several indications that the rail-safety culture at Port Otago needed strengthening, particularly with respect to the high levels of acceptance of both rule violation and at-risk behaviours.
- Commission investigators obtained and reviewed CCTV (closed-circuit television) footage for the ten days before the incident. This footage captured 88 individual rail-vehicle stabling movements. The Commission found all 88 movements involved non-compliance with the rules. Furthermore, 11 of the rail-vehicle movements involved staff moving into unsafe positions, placing them at risk of harm or injury (see Figure 24).

- To further understand the safety culture and performance in KiwiRail shunting yards, the Commission obtained roll away data that showed that in the last 10 years there have been 78 roll aways involving the incorrect stabling of rail vehicles.
- The evidence collected and analysed by the Commission indicates that within KiwiRail’s shunt yards there was a poor safety culture which included:
- walking though gaps less than 10 m wide while the shunt movement was approaching
- a crew member trying to retrieve a wheel chock from beneath a wagon as it was moving
- disconnection of the locomotive from the rake of wagons before the application of hand brakes
- crew leaving stationary wagon rakes with the air bottled in the wagon’s brake pipe
- crew not securing the wagon rake with the correct number of hand brakes
- crew not securing the wagon rake with a wheel chock.
- A strongly implemented safety culture is fundamental to how workplaces function. It sets the tone for organisational values, behaviours and expectations around safety, ensuring that everyone from leadership to frontline staff understands their role in maintaining a safe working environment.
- When safety is deeply embedded in workplace operations, it becomes a shared responsibility rather than a compliance task. A proactive approach encourages continuous improvement, reduces risk and promotes a culture where safety is not just a priority but a core part of everyday decision-making.
- Safety culture has long been described as encompassing several aspects of culture, including an informed culture, a reporting culture, a just culture, a flexible culture and a learning culture (Reason, 1997) (see Figure 25).
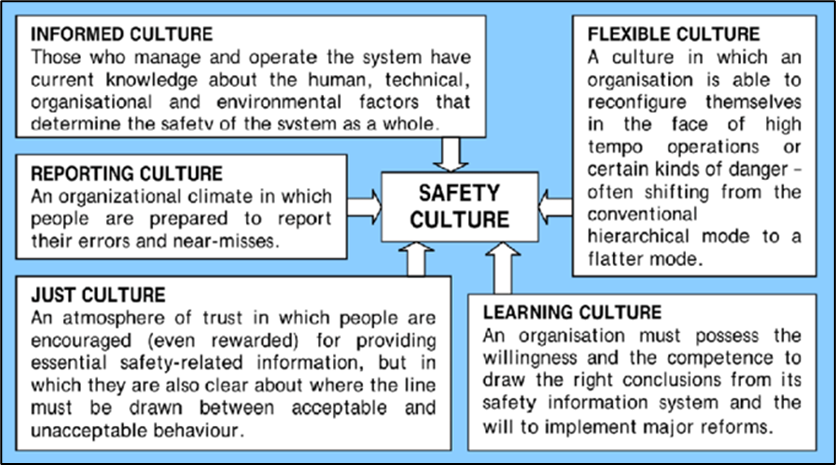
- One important component of safety culture is a learning culture – where the organisation has the willingness and competence to draw the right conclusions from its safety information system, and the will to implement changes.
-
On 12 January 2023, two years before this incident, a rake of nine wagons rolled away at Port Otago rail marshalling yard, resulting in an uncontrolled movement. KiwiRail carried out an investigation and found the following:
Risk misperception/poor hazard identification by the Rail Operators involved.
Safety critical rule violations by the Rail Operators that led to an unsecured rake of 9 wagons moving 150m.
Failed defences that were available for use but not used by the Rail Operators involved (Handbrakes, Exhausting of air, chocks). The failure of the Operators to use these controls led to the uncontrolled movement
-
In relation to the organisational culture, the investigation report stated:
During the investigation, it quickly became clear that the human factors listed above (Complacency/desensitisation to hazards, Behavioural beliefs, and Passive tolerance of rule violations) indicate dysfunctional characteristics within the work culture.
- KiwiRail’s 2023 investigation report found that while many of its suggested corrective actions were completed, most of them were unlikely to address the safety-culture issues identified. The Commission found this indicated a gap in the organisation’s ability to implement changes based on information in its safety system and highlighted a potential weakness in its learning culture.
-
One finding in the KiwiRail 2023 investigation report identified the potential to improve safety culture:
Tranzlog reviews – more frequent review of Tranzlog downloads could help the business identify gaps in shunting behaviour.
- However, the Commission found no evidence that KiwiRail had been completing the safety-audit process using Tranzlog downloads at Port Otago that could have identified non-compliance practices.
- It is very likely that with closer monitoring of compliance with procedures and other safety measures, KiwiRail could have identified safety risks in its shunting operation, potentially preventing the incident occurring.
Non-reporting of incidents
- Another important component of safety culture is a reporting culture – an organisational climate in which people are prepared to report their errors and near misses (Reason, 1997).
- The Commission reviewed a period of 10 days before the incident. No incidents had been reported despite CCTV evidence showing frequent non-compliance with procedures over this period.
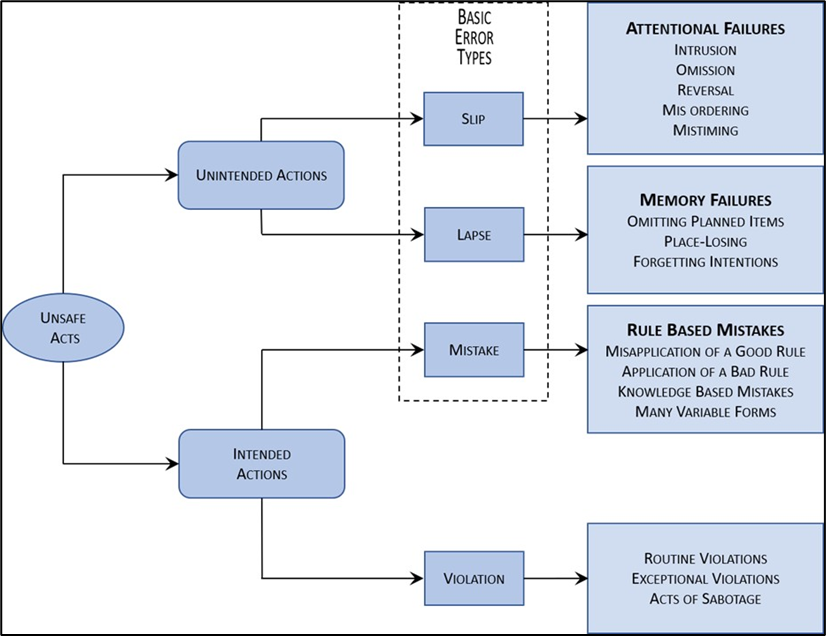
- Without consistent reporting, organisations are unable to identify why non-compliance is occurring or make changes to reduce future incidents. For example, while this incident involved rule- and knowledge-based errors by KiwiRail crew members, other non-compliance rail events in Port Otago rail facility could have been the result of slips, lapses or violations, and may require different responses and interventions (see Figure 26). Organisations are unable to respond appropriately if non-compliance is not being reported.
- While the Commission was unable to identify the factors driving KiwiRail’s under-reporting of shunting issues, the lack of reporting indicates a poor reporting culture among KiwiRail’s crews within the Port Otago rail yard.
- It is virtually certain that non-compliance with safe shunting procedures is being under-reported in the Port Otago rail yard, hindering KiwiRail’s ability to monitor and respond appropriately.
Emergency response plans
Safety issue 3: When the emergency stop button is applied on the remote-control pack, there is no automatic alert through to train control when the locomotive is stationary. This could result in a delay in implementing a response to an emergency, particularly if the remote control operator was incapacitated after applying the emergency stop.
- Engineering systems can put mechanisms in place for when human performance and time-based control applications are not sufficient. Systems such as automatic radio emergency response alerts (automatic radio emergency response alerts are sent to train control when brakes are placed in the emergency position, or the braking system loses air) are common in other parts of the rail industry, within New Zealand and around the world.
- Not having such systems installed in shunt locomotives and remote-control packs could lead to delays in responses to emergencies and create additional time delays in rendering assistance.
- The Commission found that the emergency stop button on the remote-control pack that was being used at the time did not send an alert to train control when activated. The RCO involved in this incident mistakenly believed that train control would be alerted when the emergency stop button was applied.
- The remote-control pack was function tested. It was confirmed that the pack was operating as expected and that train control was not alerted when the emergency stop button was applied when the locomotive was stationary.
-
KiwiRail and Commission investigators completed an additional test on 5 May 2025 with the same type of remote-control pack. They confirmed that activating the emergency stop button in a stationary position did not result in an emergency call to train control. When interviewed, KiwiRail’s head of engineering stated:
The remote control was not configured to alert train control when the emergency stop button was applied, or when the vigilance (time) cycle was exceeded whilst in remote control mode or when the locomotive is stationary and operating below 5 km/h.
- It is common practice for crews to work alone at certain rail yards and sidings. This presents a significant risk; in the event of an incident or accident, there is no established emergency response plan or safety oversight in place to support the crew.
- If an automatic alert system had been fitted to the emergency stop button of the remote-control pack to activate at a lower speed tolerance, it is very likely that train control would have received an emergency alert call. Train control was not aware of the collision, therefore was not able to respond immediately, apply any safety barriers or render any medical assistance to the rail crew if required.