A train was wrong routed onto a line not adjacent to a station platform. Two passengers got off and walked across the Main Line. Train control didn’t know, and rail traffic wasn’t blocked from passing through. Nobody hurt. KiwiRail fixing wrong routing of passenger trains at Rolleston, instructing crews on disembarking passengers when platform unavailable. Safety-critical personnel must communicate about who is doing what, when, to complete tasks safely.
Executive summary Tuhinga whakarāpopoto

What happened
- At about 1802 on 3 September 2019, the daily TranzAlpine service was approaching Rolleston station on a return journey from Greymouth to Christchurch. The train was incorrectly routed onto the West Main Line. The platform at Rolleston could not be accessed from this track, and two passengers who disembarked walked across the East Main Line without the knowledge of train control.
- The process of disembarking the two passengers from the train took a matter of seconds to complete. However, they were disembarked onto the ballast between the West and East Main Lines and crossed the East Main Line without any form of blocking protection being established.
Why it happened
- When the train driver and train controller became aware that the train had been routed onto the incorrect line, neither made an attempt to contact the other to discuss the situation and formulate a recovery plan.
- The decision to disembark the passengers between the tracks was based on the train driver’s own assessment that it was a low-risk operation. It did not include any input from the onboard service manager, who was responsible for passenger safety.
- KiwiRail has subsequently created a direction to train control using a semi-permanent bulletin to prevent passenger trains being routed to the West Main Line at Rolleston. KiwiRail has also drafted instructions to train crews for the controlled disembarkation of passengers when a platform is not available.
What we can learn
- All personnel involved in safety-critical operations should adhere to the principles of non-technical skills to ensure that all parties have a common understanding of what is required to complete tasks safely.
Who may benefit
- All train crews and train controllers will benefit from the findings and key lessons in this report.
Factual information Pārongo pono
Narrative
- On 3 September at about 0815, a TranzAlpine passenger train (service number 803) (Service numbers are assigned to trains to denote the geographical areas, types of train and directions of travel. In this instance, ‘803’ denotes a passenger train travelling on the Midland line in the down (south/west) direction, whereas ‘804’ denotes a passenger train travelling on the Midland line in the up (north/east) direction. Other types of train, such as freight and coal trains, are similarly assigned service numbers that denote their particular modes of operation) departed Addington station en route to Greymouth with a scheduled arrival time of 1315.
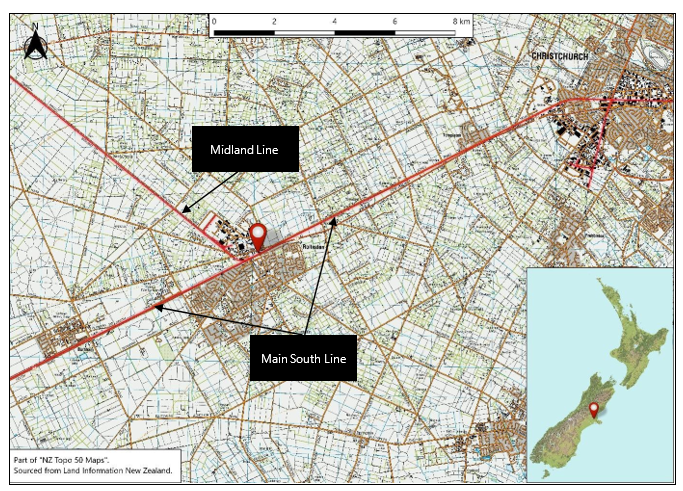
- At approximately 0833, two passengers were waiting to embark on the Rolleston station platform, which was about 26 kilometres west of Christchurch. The two passengers had not pre-booked using the operator’s website and consequently were not included on the passenger manifest prior to their embarking at Rolleston. The manifest informed TranzAlpine staff where passengers were embarking and disembarking along the journey.
- During the journey from Christchurch to Greymouth, the train traversed two separate train control (the national train control centre housed in Wellington Railway Station, where train movements and track occupations are authorised by train controllers) areas. Christchurch to Rolleston was controlled by the Main South Line (MSL) controller, and Rolleston to Greymouth was controlled by the Midland controller. Once the passengers had embarked the train at Rolleston, the train continued its journey to Greymouth.
- At about 1404, the train commenced its return journey from Greymouth to Christchurch as service 804. At about 1802 the train was approaching the MSL control area and appeared on the MSL train controller’s panel.
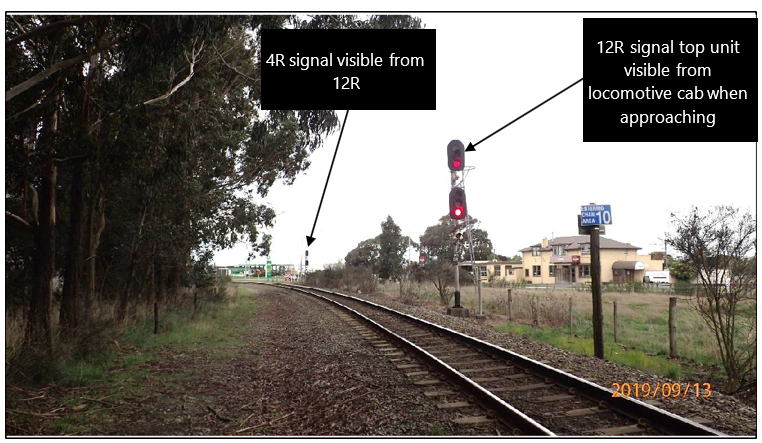
- The train controller was engaged in other control activities and service 804 was stopped briefly at 12R signal (see Figure 3), which was required to be cleared to proceed by the train controller. When the controller became aware that 804 was stopped at 12R signal, they set the signal for 804 to proceed to the MSL control area and traverse Rolleston via the West Main Line (see Figure 3). The usual route for passenger trains was to traverse the East Main Line to allow the train to stop alongside the platform if required.
- At 1802:59, 12R signal was cleared to proceed and the train driver (the driver) started to move the train forward. When 12R signal was set to proceed, the signalling system locked the route ahead of the train to ensure that the points could not be moved. At 1803:30 the train passed 12R signal and entered Rolleston station limits.
- Around this time the driver realised that the route was set for the West Main Line, not the East Main Line, which was required to bring the train alongside the platform to disembark passengers.
- At 1807:14 the driver continued along the set route and stopped the train on the West Main Line, adjacent to the platform but separated from it by the East Main Line (see Figure 4).
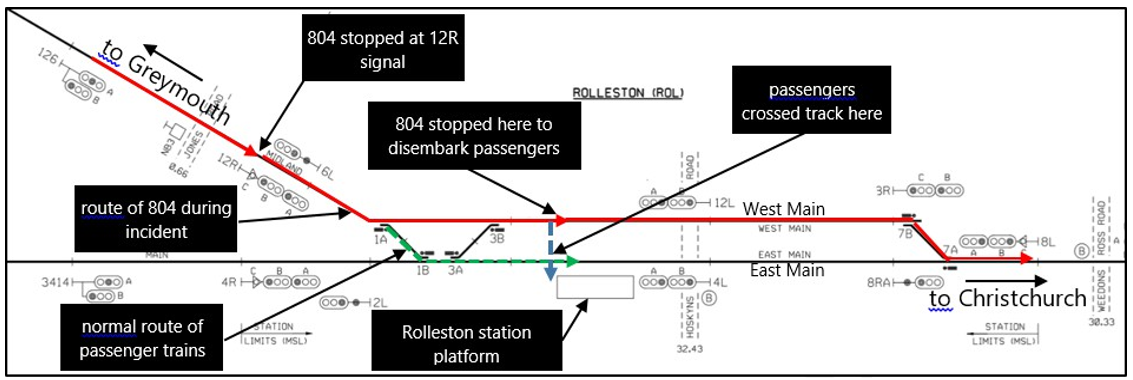
- The driver, having decided to disembark the passengers from the West Main Line, discussed the situation with the train manager, who then arranged for the passengers to be disembarked. Two passengers disembarked from the train onto the ballast between the train and the East Main Line. They then walked across the East Main Line track to reach the platform at Rolleston station.
- At 1808:56 the train departed Rolleston en route to Christchurch.
Personnel information
- The MSL train controller had about six months’ experience in the role and held all relevant qualifications and current certification.
- The driver had 15 years’ experience in the role and held all relevant qualifications and current certification.
Additional information
Midland line train movements
- The Midland line typically had 10 to 12 scheduled train movements per day, consisting of coal trains, freight trains and passenger trains, as well as other track movements such as hi-rail inspection vehicles and work trains. The majority of these track movements were routed into and out of the Midland control area from the MSL control area via the West Main Line at Rolleston.
- In order to bring passenger cars alongside the platform at Rolleston, passenger trains needed to be routed via the East Main Line. This did not preclude non-passenger rail traffic being routed via the East Main Line, but it was more efficient for them to travel via the West Main Line.
Analysis Tātaritanga
Introduction
- The safe separation of rail traffic and people on the rail corridor is a fundamental premise of any rail operation. Robust and proven rules and procedures exist that must be followed by all personnel prior to their entering the rail corridor to ensure that sufficient protection is in place.
- On this occasion, two passengers were required to cross an operational railway track without any means of protection because the train had been directed onto the wrong track in error.
- The following section analyses the circumstances surrounding the incident to identify those factors that increased the likelihood of the event occurring or increased the severity of its outcome. It also examines any safety issues that had the potential to adversely affect future operations.
Unintended routing
- On the day of the incident the MSL was being controlled by a recently qualified train controller. The controller had completed 11 weeks’ train control classroom training in March 2019, followed by 14 weeks’ live training under the instruction of a senior train controller. The live training included learning to route passenger trains via the East Main Line at Rolleston. The MSL controller had been qualified to operate solo for eight weeks.
- Around the time of the incident the train controller was engaged in radio and telephone conversations with various work parties. The train controller reported that they were aware train 804 was due to arrive at the MSL control area and had been monitoring the train’s progress on ‘GeVIS’, a KiwiRail software application that displays a dynamic geographical location of trains on the network.
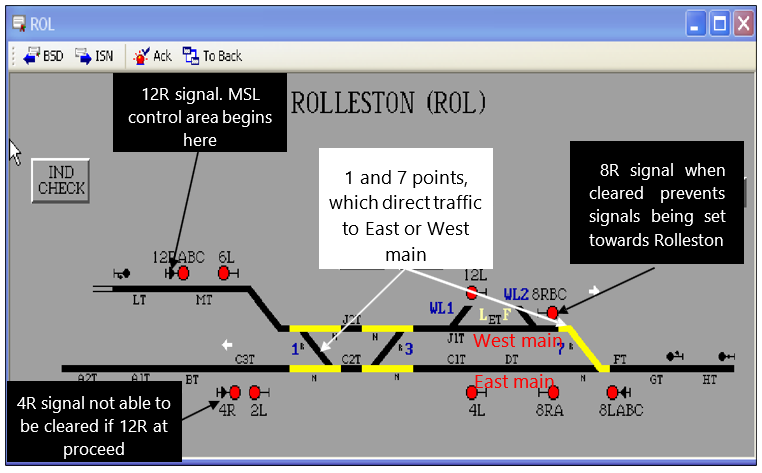
- Although the train controller reported that they thought they had set the route for the East Main Line in preparation for the arrival of 804, the route at Rolleston was set for rail traffic to travel via the West Main Line. The train control graph showed that the most recent train movement through Rolleston had been routed via the West Main Line about four hours earlier. Routing rail traffic to either the East or West Main Line required the train controller to move two sets of points, namely 1 and 7 points (see Figure 5).
- The train controller saw that train 804 was stopped outside the MSL control area at 12R signal. Knowing that passenger trains ran on a priority schedule and were not to be stopped where it could be avoided, the train controller cleared 12R signal to proceed.
- Afterwards, on realising the route was set for the West Main Line, the train controller immediately attempted to set the correct route using the East Main Line. However, the signalling system was already in the process of clearing 12R signal as set for the West Main Line and it rejected any further commands from the train controller.
- The relatively inexperienced train controller had not set the East Main Line in preparation for the arrival of the passenger train. The unintended routing of the train to the West Main Line was not in itself unsafe.
Decision to disembark passengers
- On approach to the MSL control area, the driver observed signals that indicated the train would have to stop at 12R signal (see Figure 6). The driver was aware that stopping at the normal distance from 12R signal meant the train would be stopped across the Jones Road level crossing, which was to the west of the signal. This would result in road traffic being blocked until the signal was cleared. Because of this, the driver decided to pull the train up as close as possible to the signal to clear the level crossing behind the train.
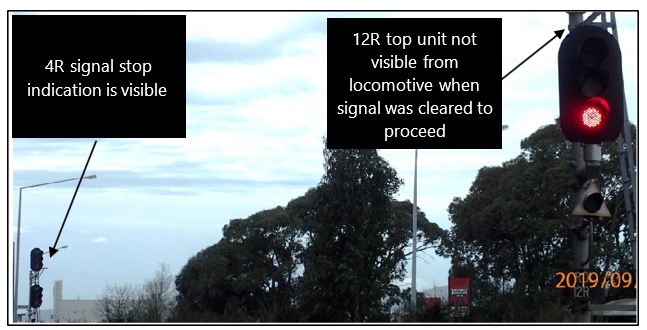
- By pulling the train up close to the signal, the driver’s view of the signal was partially obscured from inside the locomotive. Only the bottom unit of the signal was visible (see Figure 7).
- The driver reported that the train had been stopped for about five minutes before 12R signal was cleared and a proceed indication on the bottom unit of the signal was observed. While the train was stopped the driver saw 4R signal on the MSL, and noted it was at red (stop) (see Figure 7). When 4R signal displayed stop, rail traffic travelling towards Christchurch on the MSL was prevented from entering the Rolleston section. The driver recalled being aware of this.
- Had the driver taken action to observe the entire 12R signal and not just the bottom unit, they would very likely have seen that the top unit was showing that the route was set for the West Main Line. This would have provided an opportunity for the driver to stop and speak to the train controller and rectify the wrong-routing issue. However, the driver only observed a proceed signal on the bottom unit and acted on it in the expectation that the route was correctly set for the passenger train.
- The driver, having observed the proceed indication on 12R signal, began moving the train towards Rolleston and entered the MSL control area.
- The driver stated that, as the train rounded a left-hand curve towards Rolleston, they visually checked number 1 points. The driver stated that they saw they were set towards the West Main Line and not the expected East Main Line.
- The driver had been informed earlier by the train crew that there were two passengers to disembark at Rolleston. The driver knew that travelling along the West Main Line meant the train would not be able to stop alongside the platform, which was required to disembark passengers.
- The driver reported assessing the risk of disembarking the passengers onto the ballast between the tracks and the passengers walking to the platform escorted by a member of the train crew. This assessment considered:
- knowledge of how the signalling system worked and the protection it would provide
- the clear view of the rail corridor in both directions from the locomotive cab for any approaching rail traffic
- the short distance the passengers would have to walk to the safety of the platform.
- The driver assessed that, under the circumstances, it was the safest and most expedient option, and decided to proceed.
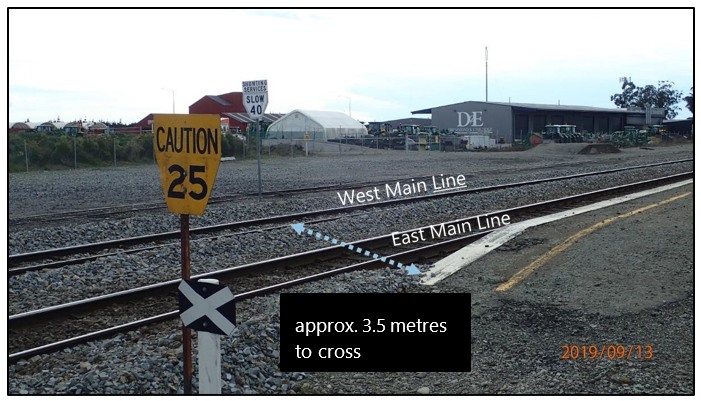
- The driver communicated this decision to the train manager, who explained the situation to the disembarking passengers. The train manager reported to the driver that the passengers were willing to step down onto the ballast and walk the 3.5 metres over the East Main Line and onto the platform.
- The driver made no attempt to contact train control after becoming aware that the train had been wrong routed, nor did they make contact with the onboard service manager (OSM) to discuss a plan for disembarking the passengers. The OSM was responsible for all aspects of passenger safety but was not included in the decision-making process regarding the passenger disembarkation. The lack of effective communication is discussed further in section 3.33.
- Once the train had stopped on the West Main Line, the train manager assisted the two passengers from the train and waited until they were clear of the rail corridor before informing the driver that the disembarkation was complete. When the passengers stepped safely onto the platform, the driver began moving the train and departed Rolleston towards Christchurch.
- Given the safety implications of passengers walking across a track, it was an operation better suited to oversight by the OSM. However, on this occasion the OSM was left out of the communication and decision-making process. When the OSM finally became aware of the events taking place, it was too late to intervene as the passengers had already disembarked.
- While the driver was in charge of the overall safe operation of the train, the OSM bore responsibility for the safety and wellbeing of the passengers. The OSM was assisted by the train manager, who was to follow the direction of the OSM in matters of passenger safety.
Communication between driver and train control
- The train controller did not attempt to contact the driver of train 804 after the train passed 12R signal, and as a result remained unaware that passengers were disembarking at Rolleston until after the incident was reported to KiwiRail.
- The lack of communication between the train controller and the driver resulted in there being no form of blocking protection, other than that provided by the signalling system interlocking, to protect the passengers crossing the East Main Line.
- This would have potentially put the passengers who were crossing the track at risk had any rail traffic been in the same section.
- Had the train controller and the driver communicated to discuss the situation, the requirement for the passenger disembarkation would likely have become apparent and a joint plan established to carry it out safely.
- The driver was of the view that the disembarkation process could be carried out safely; however, it would have been prudent to advise train control of the situation. Train control had a more complete picture of what was happening on the network, whereas the driver based the safety assessment only on what was visible at the time.
Signalling system protection
- Setting the signal at the northern end of Rolleston to proceed meant that signals could not be cleared in the opposite direction towards Rolleston. This effectively blocked that section of track for the sole occupancy of train 804.
- Similarly, the signalling system would not allow 4R signal (see Figure 5) to be set to proceed as it was interlocked with 12R signal to provide flank protection.
- This combination of signalling system protection on the East Main Line from the north and south directions had the effect of blocking any train movements from entering Rolleston on the East Main Line while the passengers were crossing it on their way to the platform. It would not, however, have had any effect on rail traffic that could have already been in the section at the time.
Non-technical skills
- The Rail Safety and Standards Board of the United Kingdom defines non-technical skills as “the cognitive, social and personal resource skills that complement technical skills and contribute to safe and efficient task performance”. While technical skills describe what you need to do and know for a given safety-critical task, non-technical skills describe how you do that task. The non-technical skill components can be broken down further into sub-categories that include situational awareness, conscientiousness, communication, decision-making and action, co-operation and working with others, workload management and self-management.
- All the key personnel involved in this incident had undergone training in non-technical skills. Nevertheless, the incident highlighted the dangers that can still occur when non-technical skills are not used, or not used effectively. On this occasion, when the train was stopped at 12R signal it was a good opportunity for the driver to confirm the full signal indication. It would have become immediately apparent that the train was about to be wrong routed and should have triggered communication between the driver, train control and the train crew to regain situational awareness and ensure there was a common mental model for all involved.
- If the train controller had been made aware before the train passed 12R signal that passengers were disembarking at Rolleston, the route could have been corrected or electronic blocking could have been applied to provide additional protection for the passengers crossing the East Main Line.
- Similarly, had the OSM been included in the driver’s risk assessment and decision-making process, alternative options for disembarking the passengers safely could have been considered, such as the passengers remaining on the train and returning by taxi to Rolleston.
- The wrong routing of the train by the train controller was a relatively straightforward situation that could have been resolved safely. Resolving it required a better use of non-technical skills, particularly communication skills, by all those involved.
- The Transport Accident Investigation Commission (Commission) has raised the issue of non-technical skills in several rail occurrence reports, including in a recommendation to the Chief Executive of Waka Kotahi NZ Transport Agency (002/12):
- The Commission recommends to the Chief Executive of the NZ Transport Agency that (the agency) require the Executive of the National Rail System Standard to develop standards to ensure that all rail participants meet a consistently high level of crew resource management, and communication that includes the use of standard rail phraseology.
- As a result of this recommendation KiwiRail implemented training programmes that included the principles of non-technical skills. All personnel involved in this incident had been trained to some extent in these principles. This incident highlighted the importance of ensuring that the principles remain prominent in workers’ minds as an important tool in planning for any safe-working scenario.
- On 3 April 2017, Waka Kotahi NZ Transport Agency said it was continuing to work with KiwiRail on addressing the recommendation. At the time of publication the recommendation remains open.
Procedures
Safety issue: No procedures were in place to direct train crews and controllers in the action to be taken in the event of berthing on the West Main Line.
- At the time of the incident there was no rule promulgated by KiwiRail stipulating that passenger trains must travel via the East Main Line at Rolleston, nor were there any procedures recommending actions to be taken in the event that a passenger train had to berth on the West Main Line. KiwiRail relied on the local knowledge of train controllers to ensure that passenger trains were routed correctly.
-
Since the incident KiwiRail has promulgated Semi-Permanent Bulletin (a means of promulgating a change to operating procedures or rules with immediate effect, without having to change the existing rulebook in entirety) 913, which includes new instructions for berthing passenger trains at Rolleston and states in part:
All passenger trains must be berthed on the East Main at Rolleston to facilitate passenger pick up and set down.
Exception: The West Main may be used to berth passenger trains only when the East Main is obstructed (e.g. disabled train, track fault) and authorised by the Network Control Manager.
Train crew are to be consulted on any West Main berthing.
- KiwiRail has also provided the Commission with a draft version of a train crew response plan for all passenger services on the KiwiRail network throughout New Zealand. This plan outlines the actions to be taken to disembark passengers safely if passenger trains cannot be berthed at a platform.
- Due to the actions taken by KiwiRail to address the issue, the Commission does not intend to make a recommendation on this matter.