A seafarer suffered serious head injuries when lifting equipment failed during an improvised operation. Damaged lifting gear had remained in service and the non-routine task was not adequately planned, risk-assessed or supervised. This report highlights lessons on lifting operations, equipment control, and implementing safety management systems on board.
Executive summary Tuhinga whakarāpopoto

What happened
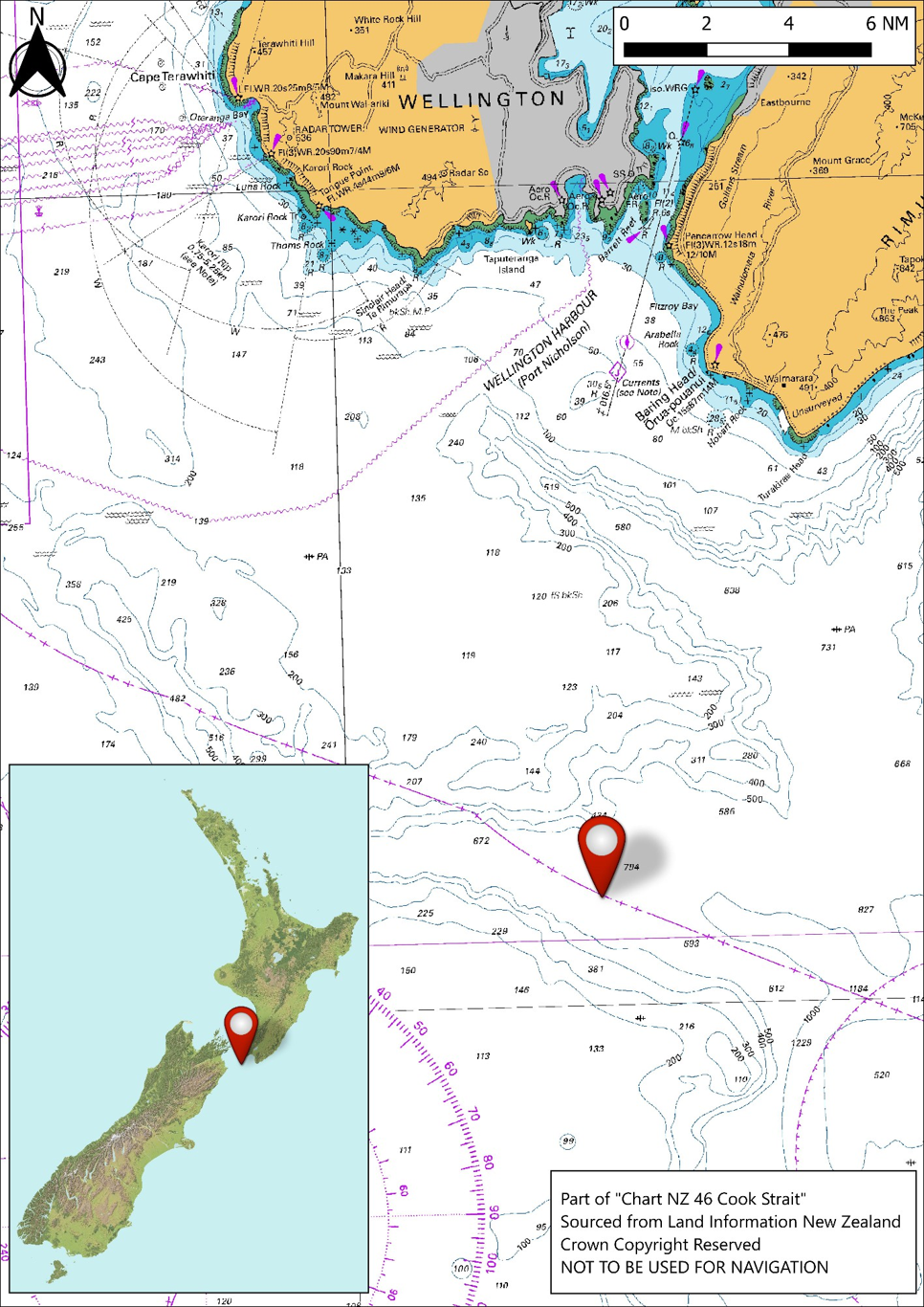
- On 20 March 2025, the Singapore-flagged bulk carrier Thor Nitnirund was drifting in Cook Strait, waiting for an available berth in the Port of Wellington.
- The weather had been rough in the days leading up to the occurrence and, as a result, two cargo lashing chains had washed off the deck and were trailing over the ship’s side.
- The crew devised a plan to retrieve the lashing chains using an improvised lifting system powered by a mooring winch.
- As the second lashing chain was hauled on board by the crew, a web sling, used to anchor the lifting system to the ship’s structure, failed. This caused components from the lifting system to strike one of the able seamen (AB), who then fell into the bosun.
- The AB sustained serious head injuries which required medical evacuation by helicopter.
Why it happened
- The web sling used to anchor the lifting system was damaged and in overall poor condition, causing its strength to be significantly reduced.
- There was no record of when the web sling was purchased. It is very likely that the sling was inherited from the previous operators.
- It is virtually certain that the bosun picked up the web sling to use it without realising it had not been subject to the maintenance and inspection regime contained in the ship’s safety management system (SMS).
- The work was not properly risk-assessed, planned or supervised, as recommended by industry best seafaring practice. It is likely that the crew did not have an appreciation of the risks associated with the job.
- A toolbox meeting was conducted in the cargo office rather than at the worksite, reducing the crew’s ability to visualise how the lifting system would work, and to identify and mitigate hazards.
What we can learn
- Standing in the bight of a line (a curved or slack section of rope forming a loop) should always be avoided as it is a high-risk area. Opportunities to identify and monitor such a risk should take place during pre-task risk assessments and from oversight of the task in progress.
- Lifting operations should always be properly planned, risk-assessed and supervised to ensure the work is carried out safely.
- For an SMS to be effective, it needs to be well understood on board and implemented to maintain, inspect and document ship’s equipment.
- An SMS is more effective when audit and compliance actions ensure that a ship’s senior officers fully understand their role in implementing the SMS in all ship operations.
Who may benefit
- Maritime operators, seafarers, regulators and training institutions may all benefit from the findings and recommendations in this report.
Factual information Pārongo pono
Narrative
- Thor Nitnirund was a Singapore-registered bulk carrier, operated by Thoresen Shipping Singapore Pte. Limited (the company), on a voyage charter to load a cargo of logs in Wellington, New Zealand.
- On 18 March 2025 the vessel arrived in Cook Strait, en route to the Port of Wellington. The ship drifted, awaiting its berth availability. During this time the weather was inclement, with southerly winds ranging from 25 to 35 knots (kt) and moderate to rough seas.
- On 20 March 2025 at about 0700 (Times in this report are in New Zealand Daylight Time (Universal Coordinated Time +13 hours) and expressed in a 24-hour format), the bosun (abbreviated version of boatswain: foreman or supervisor of the deck crew), deck fitter, deck boy (deck rating apprentice) and deck cadet (deck officer apprentice) assembled on the bridge for the daily work-planning meeting. At this meeting the chief officer (deck officer next in rank below master, head of the deck department; also known as the first officer) allocated work to each member for that day.
- Between 0825 and 0845 the same team and two additional able seamen (ABs) (experienced seafarers competent to perform normal duties on deck) assembled in the ship’s cargo office for a toolbox meeting about the allocated work. One of the jobs was lashing chains used for securing logs. Owing to the rough conditions in the Cook Strait, the ends of two lashing chains, weighing about 75 kilogrammes (kg) each, had fallen over the ship’s side and were trailing in the water. The chief officer had assigned the deck crew to retrieve them.
- At about 0945, after the bosun and the two ABs had finished another assigned job, they started preparing to retrieve the two lashing chains from over the ship’s side. They assembled on the starboard side of the forecastle deck, where they laid out an 18 millimetre(mm) polypropylene tiger rope (a composite rope with a nylon core and polyester cover).
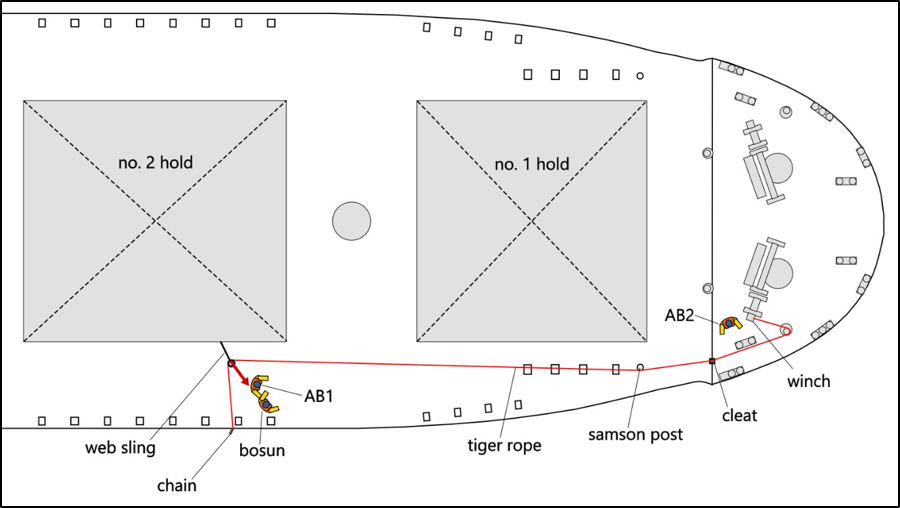
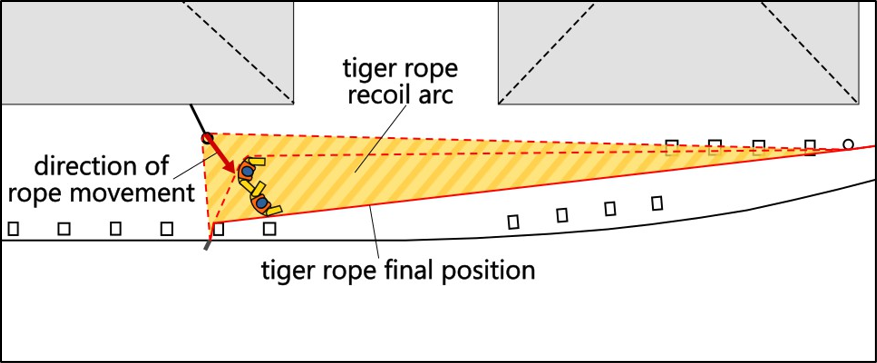
- The bosun planned to use the warping end (a cylinder-like fitting at the end of winch or windlass shafts, used mostly for auxiliary purposes such as hauling ropes across a deck or for handling additional mooring lines) on the forward starboard winch and the tiger rope to pull the chain on deck in bights (a loop in a rope or chain) (see Figure 3).
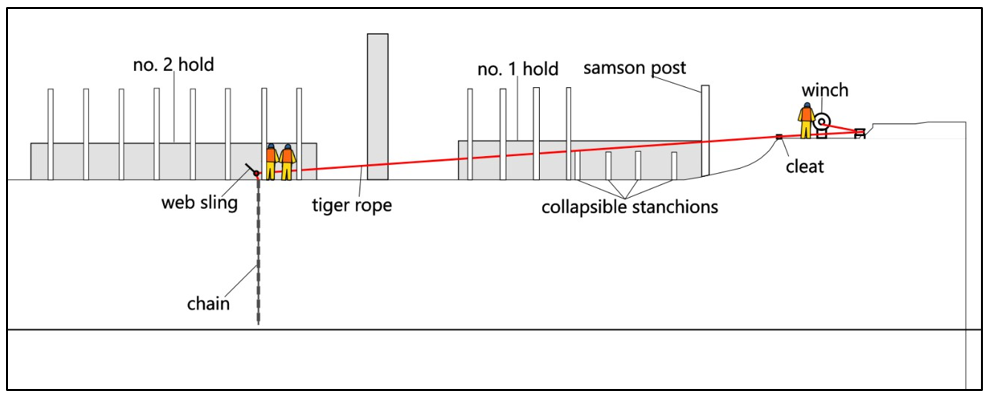
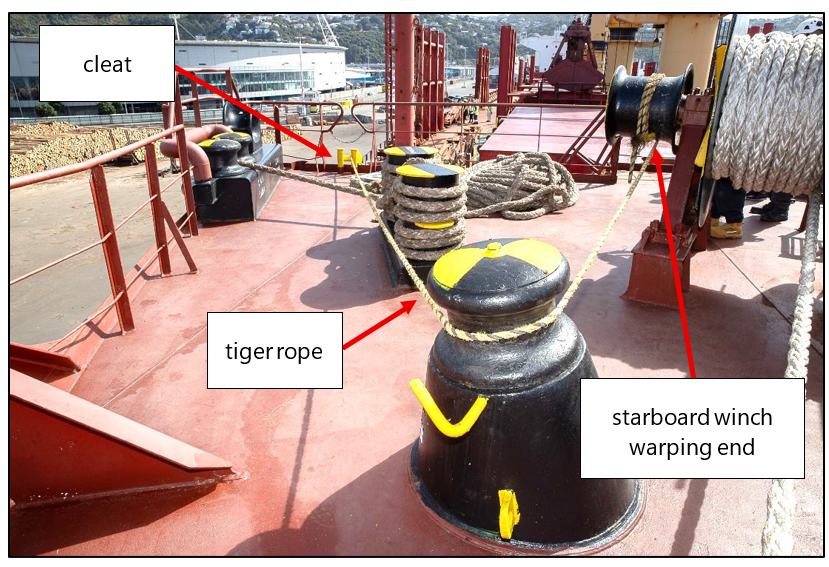
- The crew ran the tiger rope aft from the starboard mooring winch, through a cleat (deck fitting with two projecting horns, used for securing or controlling ropes) and outboard of the collapsible stanchions (a vertical support structure used to secure cargo, such as logs, on the upper deck of a ship) at no. 1 hold to the forward end of no. 2 hold (see Figure 3, 4 and 5).
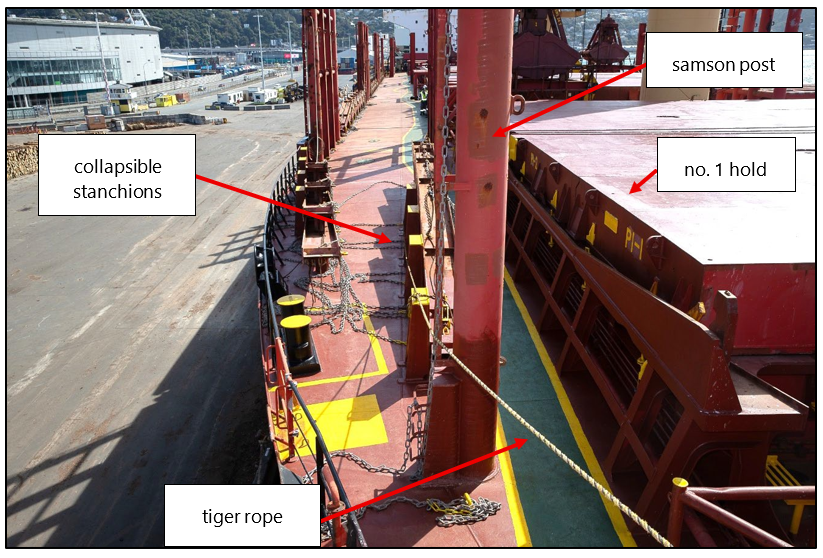
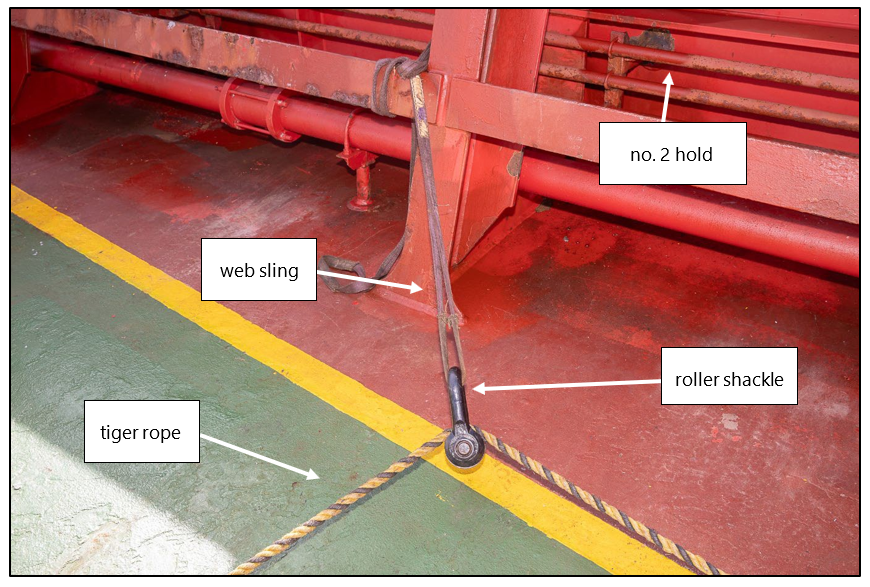
- At no. 2 hold, they rigged one end of a 1-tonne safe working load (the mass or force that can be applied to a piece of lifting equipment, lifting device or accessory to safely lift, suspend or lower without fear of breaking) flat synthetic strop (referred to as a web sling) to the coaming (vertical structure around a hatch, or other opening in the deck, to prevent water ingress) at no. 2 hold. The crew attached a roller shackle to the other eye of the web sling, and the tiger rope was passed through the roller shackle, making a 90-degree bend (see Figure 6). The tiger rope was then attached by another shackle to the lashing chain.
- At 0949, the bosun and one AB (AB1) stood at the starboard side of no. 2 hold, next to the web sling and roller shackle. The other AB (AB2) went to the forward mooring deck to operate the starboard mooring winch (see Figure 7). They lifted the first chain which came up easily. They then started lifting the second chain.
- At about 0955, the web sling parted, causing the tiger rope to recoil across the deck. The tiger rope and shackle struck AB1 with significant force in the back of the legs. This caused them to strike their head on the deck and collide with the bosun before both crew members landed near the ship’s bulwarks. The bosun got to their feet a few seconds later and went to assist the injured AB.
- The bosun reported to the bridge via radio that AB1 was injured. The third officer answered the call on the bridge and woke the second officer to attend to the injured AB.
- The second officer went on deck with a first aid kit and stretcher. By about 1020, the second officer, with the help of other crew members, shifted the injured AB to the ship’s hospital (dedicated medical room with medical supplies onboard ship). The master (the ship’s captain, the highest ranked officer onboard the ship) met them there and assessed the AB’s condition.
- At about 1045, the master informed the company of the accident and called for shore-based medical advice. The crew then administered first aid in accordance with the medical advice received.
- By 1134, the master had sent an email to the shipping agent (person who acts for one or more of the parties with an interest in the ship charter; the same agent may act on behalf of the ship owner and the charterer) and asked for assistance to evacuate the injured AB to a hospital for medical attention.
- The shipping agent called the Rescue Coordination Centre New Zealand (RCCNZ) and requested a medical evacuation (medevac).
- At about 1349 a helicopter arrived at the ship. At 1405 the injured AB was winched up to the helicopter and flown to Wellington Hospital where they were treated for their injuries.
- Three days later on 23 March 2025, the Thor Nitnirund berthed at Aotea Quay at the Port of Wellington.
- The injured AB remained in Wellington Hospital until 20 April 2025, when they were repatriated to Thailand where their treatment and recuperation continued.
Personnel information
- The master held overall authority and responsibility for the safety of the vessel, the people on board, the cargo and the environmental effects of the maritime operation. The master had held command for 10 years and had 25 years’ seagoing experience. The master had first taken command of Thor Nitnirund in October 2023 for about one year and had rejoined the ship on 17 February 2025.
- The chief officer progressed in rank from third officer to chief officer over a 10-year period. The chief officer joined Thor Nitnirund in October 2024, and this was their first assignment in the role. On board Thor Nitnirund, the chief officer was second-in-command of the vessel and in charge of the deck department. The chief officer’s duties included navigation watches, deck administration, responsibility for deck maintenance, cargo planning and preparation of lashing gear. As well as holding responsibility for ensuring a safe work environment on deck, the chief officer was the delegated ship safety officer and accident prevention officer.
- The bosun had 15 years’ experience working at sea on vessels like Thor Nitnirund. They had worked for the company for five years and had been promoted to the bosun’s role in the year before the accident. The bosun joined Thor Nitnirund in December 2024.
- The injured AB had five years’ experience working at sea. This was their first trip sailing as a newly promoted AB. They had joined the ship on 17 February 2025.
Ship information
- Thor Nitnirund was a bulk carrier, registered in Singapore and owned and commercially operated by Thoresen Shipping Singapore Pte Limited.
- The ship’s International Safety Management (ISM) Manager was Thoreson & Co. (Bangkok) Limited (the operator). A Document of Compliance was issued to them on 16 December 2021, which certified that the ship met ISM requirements.
Meteorological information
-
On 18 and 19 March 2025, the weather in the Cook Strait was from the south, with winds ranging from 25 to 40 kt, and moderate to rough seas. The ship’s crew were restricted to working inside the ship’s accommodation block.
- On 20 March 2025, at the time of the accident, the ship’s anemometer recorded a southerly wind of 27.5 kt. The sea state was recorded in the logbook as moderate to rough.
Recorded data
- Commission investigators downloaded data from the ship’s voyage data recorder, as well as footage from the closed-circuit television (CCTV) camera located on the starboard bridge wing, capturing the accident.
Tests and research
- The Commission engaged an independent expert to determine the web sling’s residual strength (see section 3 for a discussion of the test results).
Previous occurrences
MO-2014-203 Fatal injury, Purse seine fishing vessel, Captain M. J. Souza, 24 August 2014
- On 24 August 2014, crew on board the purse seine fishing vessel (a type of fishing vessel that uses a purse seine net to encircle a school of fish), Captain M. J. Souza, were engaged in a routine fishing operation when a safety choker line broke under load and recoiled, striking a crew member in the head. The crew member died instantly. The choker line parted because of its deteriorated condition and the incorporation of a bowline knot, which significantly reduced its overall breaking strength.
- The safety management system (SMS) on board the Captain M. J. Souza did not effectively manage the purchase, storage, inspection and retirement from service of the ropes on board.
- On 29 September 2016, the Commission recommended (recommendation 020/16) that Talley’s Group Limited, the operator of the Captain M. J. Souza, review its internal auditing procedures to ensure that auditors make realistic assessments based on actual practices observed on board. They should seek verification that crew are following documented procedures and that the procedures are appropriate to the task. They should record audit findings together with any safety actions taken as a result of the audit (Transport Accident Investigation Commission, 2016).
- On 20 October 2016, Talley’s Group Limited informed the Commission that they had taken the following safety actions:
- implemented a programme to improve health and safety culture on board
- increased managerial oversight of documented health and safety procedures and compliance on board
- implemented a revised assurance process to ensure health and safety protocols are being applied
- provided additional third-party health and safety training to officers and crew
- improved communication structures between senior management and senior vessel staff
- set out company expectations regarding health and safety on board
- engaged an independent health and safety expert to audit compliance with health and safety procedures and, if appropriate, put in place an effective change management programme.
MO-2019-203 Bulk log carrier Coresky OL. Crew fatality during cargo-securing operation, Eastland Port, Gisborne. 3 April 2019
- On 3 April 2019, crew on board the bulk carrier Coresky OL were using a crane to tension a wire rope to secure the load. When a wire snapped, equipment recoiled, striking and fatally injuring a seaman. The Commission found that the wire snapped because of the load from the crane and configuration of blocks. Crew lacked information and guidance on hazards and doing this work safely.
- The operator’s SMS was not supported by an effective safety assessment of log-cargo securing operations, which should have identified the hazards present. This resulted in ineffective controls to mitigate the risks to crew when completing these tasks.
- On 21 May 2020, the Commission recommended (recommendation 004/20) that Shih Wei Navigation Company Limited (Taiwan), the operator of the Coresky OL, carry out a comprehensive safety assessment of vessels engaged in carrying and securing deck log cargo to ensure appropriate procedures and guidance were contained in the SMS and that a safe system of work was established (Transport Accident Investigation Commission, 2020).
- The ship’s operator provided the Commission with the following safety actions taken:
- The company shared an internal investigation report, as to the lessons learnt, to the fleet for all crew’s attention
- The company revised the relative SMS procedures and checklists according to the findings of the internal investigation, including:
- Carrying Timber Deck Cargoes
- Crew Re-Training Report for familiarisation with safe Cargo Securing Operations engaged by ship’s crew
- Checklist of Check Points & Typical Damages Permit to work for deck timber lashing
- Record of Personal Protective Equipment (PPE) on board.
- The company required the crew to examine all cargo-securing equipment with defective equipment found removed from service. The company also supplied some new securing materials in next port of call, Zhenjiang, China after Incheon
- The company enhanced the education and training of newly joined crewmembers, especially for log carried [sic]
- The company issued a fleet circular (E-Circular 20-11/ Attention for the lashing of timber loading on deck and risk assessment) on 8th April 2020.
Analysis Tātaritanga
Introduction
- During rough conditions in the Cook Strait, two lashing chains were washed over the side of Thor Nitnirund. The lashing chains were still attached to deck fittings and trailing over the ship’s side. The crew devised a plan to haul the lashing chains back on board using an improvised lifting system powered by a mooring winch.
- The crew used a web sling to anchor the lifting system to the ship’s structure. As the crew lifted the second lashing on board, the web sling failed. Components of the lifting system recoiled, striking an AB who then fell to the deck and into the bosun. The force of the impact caused serious head injuries to the AB who required medical evacuation from the ship by helicopter. The bosun did not incur any significant injuries.
- The following section analyses the circumstances surrounding the event to identify those factors that increased the likelihood of the event occurring or increased the severity of its outcome. It also examines any safety issues that have the potential to adversely affect future operations.
The failed web sling
- The web sling that failed during the accident was a flat synthetic web sling with a 1-tonne safe working load.
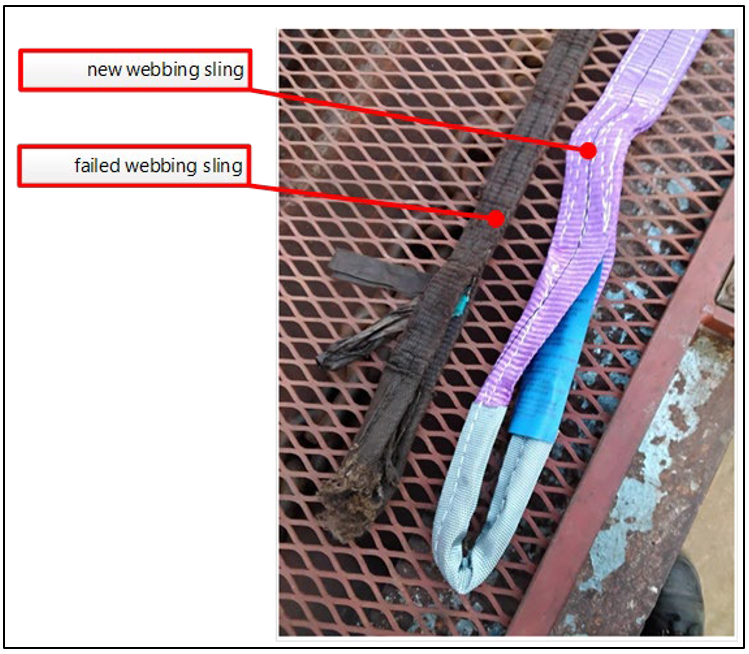
- The Commission examined the failed web sling and found that it was saturated with oil and generally in poor condition (see Figure 8). The bearing surface of the eye was completely cut in half and frayed. On assessment of the cut, investigators noticed that some of the frayed material appeared dirty, and only a portion of the webbing fibres appeared clean. This indicated that some of the webbing had been chafed before the accident, resulting in a partial cut that damaged the sling.
- Such a cut can normally be attributed to using a sling on a sharp edge – an edge that is not rounded or an edge that is rounded but with a diameter too small for the webbing – causing damage to the webbing under load.
- The clean fibres represented the remaining webbing material that had failed during the accident.
- Web slings are designed in a way that the stitching should be the first point of failure if the sling is overloaded. In this accident, the webbing material failed while the stitching remained intact, further indicating that the webbing material was damaged before the accident.
- The Commission engaged an independent expert to test the residual strength of the web sling. The generally accepted safety factor of a web sling is 6:1 (Ministry of Business, Innovation & Employment, 2012). This means that a sling with a 6-tonne minimum breaking load (the minimum load or force to be achieved before the lifting equipment risks breakage or any change that causes the load to loosen) has a 1-tonne safe working load.
- During the testing, a gradual load was applied to the sling and the sling failed when the load reached 2.86 tonnes. The sling’s webbing did not break, but the stitching near the eye end failed, as designed.
- Testing revealed that while the sling withstood a load greater than its 1-tonne safe working load, it failed at only 48% of its expected minimum breaking load of 6 tonnes.
- Taking into consideration all available evidence, the Commission found that previous damage to the eye of the web sling and its overall poor condition contributed to its failure.
- The purpose of visual examinations and periodic inspections and examinations of web slings is to identify any damage to the sling.
- When damage is discovered, the sling should be removed from circulation. Instructions to this effect and to support this process were not contained within the ship’s SMS.
Onboard inspection and control of loose gear
Safety issue 1: The ship’s SMS did not ensure that all equipment used for lifting operations was maintained in a safe condition. As a result, an unsafe piece of equipment remained in service and failed, resulting in a serious injury.
- The company purchased the Thor Nitnirund in 2021. The company advised the Commission that in preparation for recommissioning, they replaced all the loose lifting gear on the ship. All loose lifting gear was subject to the inspection and quality control processes prescribed in the ship’s SMS. However, these safety processes did not ensure that substandard lifting gear was identified and removed from the ship.
- As a result, the crew used a web sling that was in a poor condition, resulting in its failure under load. The following paragraphs describe how the SMS failed to support the crew in identifying and maintaining safe lifting gear for use on board.
Requirement for maintenance and inspection of ship’s equipment
- The Thor Nitnirund was registered in Singapore and was therefore subject to Singaporean law. Singapore had given effect to the International Convention for the Safety of Life at Sea (SOLAS) and the International Safety Management (ISM) Code through the Merchant Shipping (Safety Convention) Regulations.
- In ISM Code section 10, ‘Maintenance of the ship and equipment’, subsection 10.1 states that the company should establish procedures to ensure that the ship is maintained in conformity with the provisions of the relevant rules and regulations and with any additional requirements that may be established by the company.
- In meeting these requirements, subsection 10.2 states that the company should ensure that:
- inspections are held at appropriate intervals
- any non-conformity is reported with its possible cause, if known
- appropriate corrective action is taken
- records of these activities are maintained.
- Subsection 10.3 also states that the company should:
- identify equipment and technical systems the sudden operational failure of which may result in hazardous situations
- ensure that their SMS provides specific measures aimed at promoting the reliability of such equipment or systems. These measures should include the regular testing of standby arrangements and equipment or technical systems that are not in continuous use.
- Examples of such equipment would include loose lifting gear and webbing slings.
- Further, subsection 10.4 notes that the inspections should be integrated into the ship’s operational maintenance routine.
Thor Nitnirund’s SMS
- In this case, the ship’s SMS contained a procedure for the maintenance of cargo gear and loose lifting gear (SOPM/08). The procedure required the chief officer and chief engineer to ensure that:
- the cargo gear’s structure, greasing, wire rope, spare blocks and loose gears (sic) are examined before using
- if any are found worn out more than limit (sic), they shall be replaced
- to examine all lifting accessories/loose lifting gear before being put into use for the first time and after any substantial alteration or repair to any part liable to affect its safety.
- Once the equipment was in service the ship’s SMS required that:
- all lifting accessories/loose lifting gear are thoroughly examined by the chief officer and chief engineer every four months
- any lifting gear found to be worn out shall be removed from service.
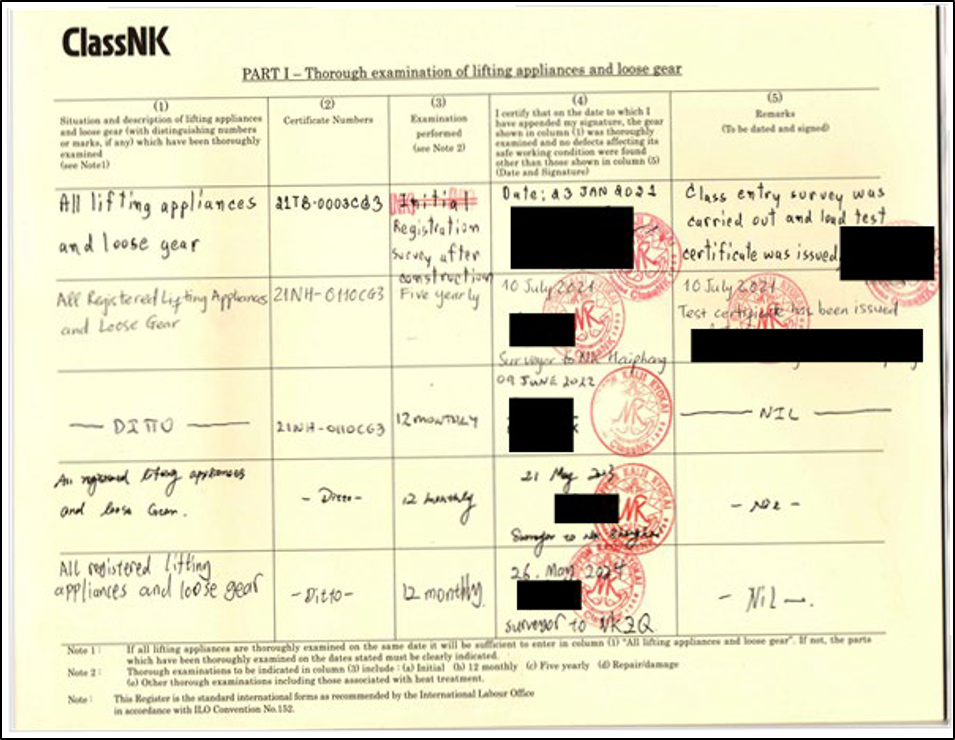
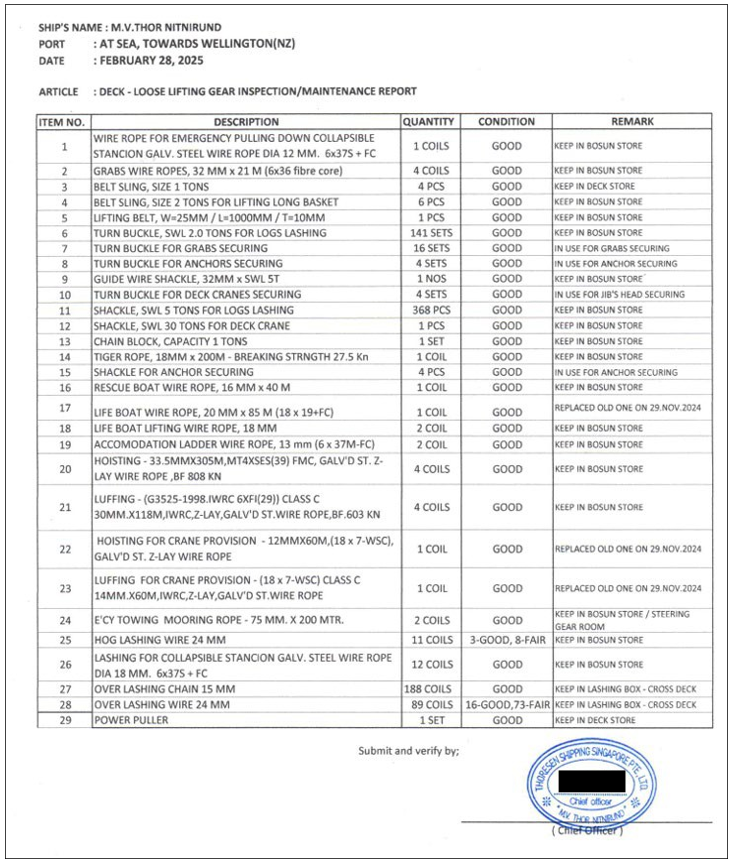
- The SMS included a register for all loose lifting gear (see Appendix 1). This register listed categories of equipment rather than individually itemised pieces of equipment. For example, the web sling used during the accident was a belt sling with 1-tonne safe working load, and the 'corresponding line item in the register was ‘belt sling, size 1 tons [sic]’ (see Figure 9). An assessment carried out on 28 February 2025 recorded that there were four of these slings and that their condition was ‘good’.

- The SMS met requirements to have loose gear periodically inspected by a competent person. To do this effectively, the onboard system requires a means of identifying each item of loose gear so that there can be no confusion over the condition of each item. Furthermore, damaged and time-expired equipment should be removed from use and discarded from the ship at the next port. Neither the register nor the slings seen on board by Commission investigators were itemised or individually identifiable, making it impossible to identify which slings had been examined. The web sling that broke on the day of the accident had no identifying information or inspection tag attached to it.
- Given the condition of the failed web sling, the Commission found it was very unlikely that it was one of the four web slings recorded to have been thoroughly examined and found to be in good condition (as shown on the SMS Lifting Gear Register).
- The ship’s operator told the Commission it had replaced all loose lifting gear, such as slings, when it took over control of the ship, and it had not replaced the slings since then. The Thor Nitnirund’s SMS did not ensure individual identification of each item of loose gear. Therefore, the Commission could not confirm if the failed sling was one of the slings referred to in the SMS documents or if it was a condemned sling that should have been removed from circulation and discarded. The Commission considers it is very likely that the failed web sling was inherited from the previous operator and remained on board the vessel in addition to the slings included in the SMS Lifting Gear Register.
- The SMS required the chief officer or the chief engineer to carry out the planned maintenance and inspections and to follow the instructions contained in the SMS. It would be reasonable to expect that a competent person inspecting the web sling would have recognised its deteriorated condition and the impact of the frayed cut on its safe working load. Given the condition of the web sling, the Commission considers it unlikely that the web sling had been inspected by the chief officer or the chief engineer as required by the SMS.
- It is likely that the crew underestimated the importance of the sling to the lifting system and did not recognise the dangers that would be present using the rigged lifting system under load. As a result, the bosun did not consider that, despite its deteriorated condition, the web sling was unsuitable as a component in the lifting system devised to retrieve the lashing chains from over the ship’s side.
Storage of loose lifting gear
- There are several reasons an unregistered sling could remain on board and be used by the crew, without being subject to the SMS quality assurance.
- The loose lifting gear was stored in the deck store, located in the ship’s forecastle. Commission investigators found indications of poor housekeeping in the deck store (see Figure 10). An organised deck store helps ensure that items can be easily located and that a proper inventory of equipment can be maintained, clearly separating in-use and out-of-service equipment.
- Because the loose gear did not have individual identification tags it would not be obvious to crew if any specific loose gear had been examined. It is virtually certain that the bosun picked up the sling to use without realising it had not been subject to the SMS quality assurance. Equipment can be damaged between periodic inspections, so it is essential that all components of a lifting system are inspected before use.

- While the only inspections prescribed in the SMS were to be conducted by the chief officer and chief engineer, it is good seamanship practice for crew to visually inspect any equipment before its use. Upon presentation of the failed sling at the jobsite before starting work, its poor condition should have prompted the crew to examine it further. Had they done so, they may have noticed the frayed cut.
- The poor condition of the web sling was identifiable under visual examination. The International Maritime Organization (IMO) defines an inspection as ‘an assessment carried out by a responsible person to ascertain if the lifting appliance or loose gear is in good working condition for continued safe use’ (International Maritime Organization, 2026). The ship’s SMS assigns the responsibility for these inspections to senior officers (chief officer/chief engineer). On board Thor Nitnirund, the chief officer delegated the planning and execution of the job to retrieve the lashing chains to the bosun. Such a delegation without further oversight of the job indicates that they did not fully understand the roles, responsibilities and requirements of the ship’s SMS (see Onboard implementation of the SMS, paragraphs 3.56–3.62).
- There are no specific standards for training ships’ crews to inspect and recognise weaknesses in lifting gear. On-the-job training and experience are generally relied upon to fill this gap. However, the IMO’s International Convention on Standards of Training, Certification and Watchkeeping for Seafarers (STCW), particularly Tables A-II/1 and A-II/2 (these set out the mandatory minimum requirements for certification of masters and chief mates on ships of 500 t gross tonnage or more), requires deck officers to demonstrate general competence in the operation and management of shipboard cargo-handling gear. This responsibility includes performing periodic and pre-operational inspection of lifting gear and its components, understanding the concept of safe working load and how the safe working load can be reduced through certain rigging practices.
Standing in an unsafe area
-
During the lifting operation the bosun and AB1 were standing in the bight of the lifting system (see Figure 11). By doing so, both crew members were in danger of being struck by components of the lifting system when it failed.
-
The web sling and shackle served to redirect the tiger line to pull the lashing chains on deck towards the hatch coaming. As such, the web sling was susceptible to additional load from the weight of the chain and the opposing pulling force from the mooring winch. Failure of the web sling under strain resulted in the tiger rope and shackle projecting towards the two crew members in an instant.
-
The risk associated with standing in the bight of a line or lifting arrangement is well known in the maritime industry and is incorporated into basic seamanship training. Opportunities to identify and monitor such a risk commonly take place during pre-task risk assessments and oversight of the task in progress.
Planning and execution of safe work
Safety issue 2: The ship's SMS included procedures to conduct risk assessments and toolbox meetings. However, the onboard implementation of the SMS and the operator’s audit follow-ups did not ensure that non-routine tasks were properly planned and safely executed.
Risk assessment and risk awareness
- In 2016, the Transport Safety Investigation Bureau (TSIB) of Singapore, published a report that investigated an accident in which a crewmember was killed by a snap-back of a mooring line (Transport Safety Investigation Bureau, 2019). The report highlighted the Maritime & Coastguard Agency of UK’s Code of Safe Working Practices for Merchant Seafarers (COSWP). The Maritime and Port Authority of Singapore (MPA) released Shipping Circular No. 25 of 2017, which recommended either carrying the COSWP on board or providing appropriate safe working practices in the SMS (Maritime and Port Authority of Singapore, 2017).
- At the time of the Thor Nitnirund accident, the 2024 issue of COSWP was available on board.
-
Section 1.2.6 of the COSWP deals with risk awareness and risk assessment. It also breaks down and promotes the adoption of a four-level process for risk assessment:
Level 1 – deals with generic risk assessments and should be contained in the company’s SMS in the form of policies, procedures and work instructions
Level 2 – risk assessment details the task-based risk assessment (TBRA) used when generic risk assessments are not suitable for specific tasks and non-routine tasks
Level 3 – describes the use of a toolbox talk. The toolbox talk is another form of risk assessment carried out in support of a TBRA
Level 4 – covers personal assessment of risk through informal assessment of day-to-day risks carried out as you are working, and in life generally.
Toolbox meetings
- The ship’s SMS contained the policies and procedures to manage risk on board. The SMS included identification and prescription of generic risk controls. At an operational level the SMS required the crew to conduct a toolbox meeting before starting work. The purpose of the toolbox meeting was to ensure the crew conducting the work had a shared understanding of what was to be done.
- The SMS required that ‘Before commencement of work there should always be a toolbox meeting and [a] record [of it] in the log’. The log was a paper form, and included the following prompts:
- Hazard and risk controls for work activities are highlighted.
- Safe work procedures are communicated (SMS, SOPM, SI, etc)
- Recent incidents are shared
- Crew members are encouraged to ask questions and participate
- Wearing personal protective equipment (PPE)
- The meeting should take about 10 minutes and be recorded in the log.
- COSWP recommends that a toolbox talk should be conducted before any work being carried out that involves more than one person, and where there is significant risk to persons or assets. It recommends the following:
- Active involvement of those carrying out the work and who may be at risk
- Encouragement of full and active participation
- Discussion of any questions
- Consideration of any concerns raised
- Documenting the toolbox meeting any relevant risk assessments.
- The onboard toolbox meeting log identified three different areas of work that were to take place on 20 March 2025 (see Figure 12). Two of these tasks involved using powered machinery, including the recovery of the two lashing chains and the relocation of the mooring rope.
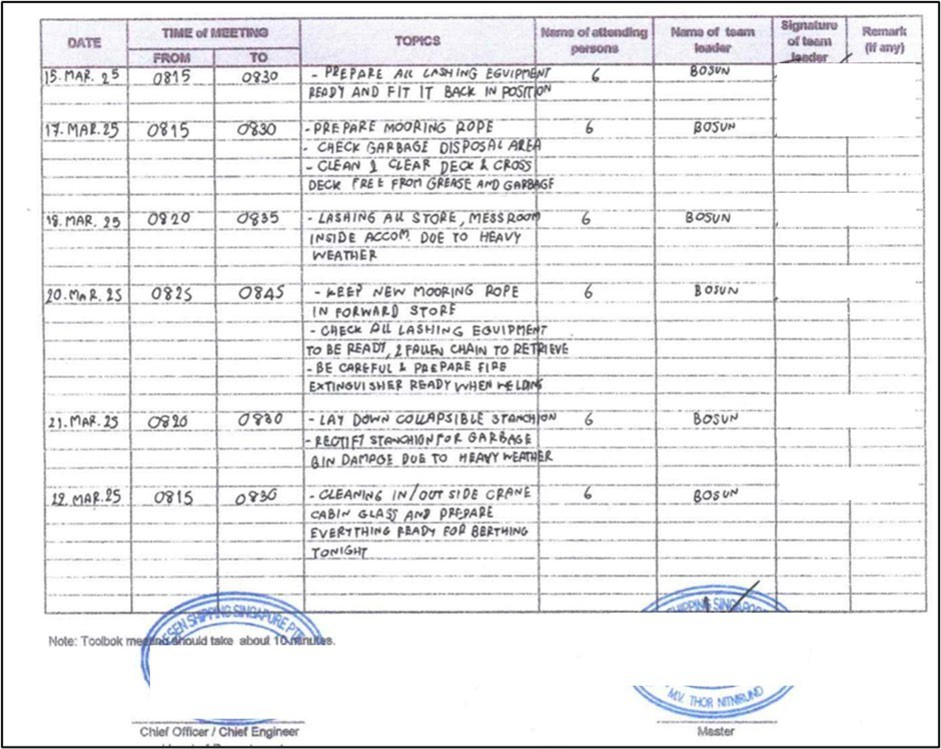
- Each task required crew to conduct a separate risk assessment that considered the powered deck equipment to be used and the associated increased risk levels. The toolbox meeting, which covered all three tasks, was recorded in the log as taking 20 minutes, with no remarks recorded.
- A risk assessment, dynamic or otherwise, was not mentioned in the toolbox meeting log as an area to cover in the meeting. Neither a task-based risk assessment nor formal risk assessment was conducted for lifting the lashing chains, which was a non-routine task. It was a missed opportunity for all crew involved to identify the equipment to be used, and possible hazards and risks associated with the task. Identifying the equipment intended to be utilised would have provided the opportunity to assess the condition of the synthetic web sling.
- Not conducting a toolbox meeting at the work site reduced the ability for the crew to:
- visualise how the lifting system would work and interact with the structures around it
- identify potential snags and pinch points, between the vessel’s structure and the lifting components, if the system were to come under strain
- identify the weakest points of the lifting system that would fail first and possibly be subject to recoil
- appreciate the potential to overload the lifting system by using a high-powered mooring winch to perform the lifting work
- determine safe areas to stand that were either sheltered or appropriately distant from recoil
- reassert good practices, like not standing next to a line under tension
- identify challenges to line-of-sight communication where obstructions between operating areas made handheld radios more appropriate than communicating by hand signals.
- A supervisor was not assigned for this task because the bosun was part of the team conducting the work. As a result, there was no single point of control with complete overview of the work. None of the crew members involved identified or challenged the decision to stand in the bight of a line used in a lifting system under tension.
-
Daily work planning meetings and toolbox meetings should be separate tasks. At the time of the accident, these meetings were amalgamated into one and did not involve all concerned or cover risk assessments for separate tasks.
Personal protective equipment
- The ship’s SMS contained a personal protective equipment (PPE) policy. It required all crew members to wear industrial safety helmets when working on deck. The consequences of this accident were significantly reduced because the work crew were wearing head protection.
- When a person falls and their feet and lower body are suddenly displaced, their head becomes the leading point of contact with the ground. The AB was wearing a basic general-purpose safety helmet, worn properly with the chinstrap secure. This played a crucial role in absorbing some of the impact when the AB’s head hit the deck, increasing the survivability of the accident.
- Safety helmets protect the head by distributing external pressure over a large area. The helmet’s hard shell deflects and absorbs energy while resisting deformation and damage. The harness secures the helmet and reduces the impact of a strike by maintaining clearance between the helmet shell and the user’s skull. During the accident sequence, the AB’s helmet shell became detached from the harness after impact. Despite this, the helmet’s shell absorbed some of the impact and forces involved in this accident.
- No single type of helmet is the ideal form of protection for all tasks and eventualities. PPE is considered the very last order of safety control when higher-order safety actions, such as elimination, engineering and administrative safety controls, have been applied. Operators should consider the most appropriate type of helmet for their operation to maximise their effectiveness.
Onboard implementation of the SMS
- During the investigation, Commission investigators reviewed relevant parts of the SMS and concluded that the prescribed maintenance procedures and expected work practices were sufficient to safely carry out the intended job. However, the work was not planned or executed in accordance with best seafaring practice. The COSWP advises that all lifting operations should be:
- risk-assessed
- properly planned
- supervised
- carried out in a safe manner
- The onboard familiarisation training required sign-off that officers were familiar with all relevant codes, conventions and guidelines relevant to their job.
- The operator conducted internal ISM audits at intervals not exceeding 12 months. The audit carried out in February 2025 identified seven observations where the root cause was a lack of understanding or awareness of the SMS and its importance. Senior officers, who were vital in the implementation of the SMS on board, did not fully understand the importance of elements of the SMS. However, only one of these audit observations resulted in long-term preventative action that included education of the crew in respect of the relevant SMS requirements.
- Several safety indicators showed that the SMS was not deeply entrenched in the onboard safety culture. These included the standard of housekeeping in the deck store, the confusion about lifting gear identification, inspection and storage, and the use of the toolbox talk log as a job list. A completed checklist did not guarantee that a job was carried out as prescribed in a procedure. Audit observations were addressed by rectifying the fault and assigning responsibility to the senior officer already responsible for that item, rather than ensuring that senior officers had a deep understanding of the SMS and their role in implementing the SMS in the day-to-day running of the ship.
- On the day of the accident, the components used to make up the improvised lifting system were not inspected to ensure they were fit for the lifting job. Potential hazards, especially those likely when the system came under tension, were not identified or controlled. A risk assessment should have identified the risk of the system failing at its weakest point. This risk was enhanced because the mooring winch was significantly overpowered for use with an improvised lifting system, should part of the lift become snagged. Often, a mooring winch is used to move ropes with a safe working load 30 times greater than that of a 1-tonne sling.
- Inspection and control of the accessories for lifting and loose gear, as required by the SMS, would have removed damaged slings from circulation, preventing their use as part of a lifting system. Implementation of the SMS toolbox meeting and risk assessment requirements would have increased the opportunity for crew to recognise the risk involved with carrying out the job as planned and take steps to make it safer.
- Risk assessment, planning and supervision of the work, as recommended in COSWP, increase the likelihood of the work being carried out in a safe manner, and provide the crew with a deeper appreciation of the risks associated with the job.
Appendix 1. Part 1 Deck – Loose lifting gear inspection/maintenance report
Part 2 - Thorough examination of lifting appliances and loose gear