On 27 April 2022, the Minister of Transport directed the Transport Accident Investigation Commission to investigate two fatal stevedoring accidents under section 13(2) of the Transport Accident Investigation Commission Act 1990. Although the accidents occurred separately, the Commission identified common systemic safety issues and has therefore presented both inquiries in a single report, noting their relevance to the wider stevedoring industry. The first accident occurred on 19 April 2022 at the Port of Auckland, where a stevedore employed by Wallace Investments Limited was fatally crushed after moving beneath a suspended container onboard the Capitaine Tasman. The second occurred on 25 April 2022 at Lyttelton Port, where a stevedore employed by Lyttelton Port Company Limited was found deceased on the ETG Aquarius, buried under coal during loading operations.
Executive summary Tuhinga whakarāpopoto



What happened
- On 27 April 2022, the Minister of Transport directed the Transport Accident Investigation Commission to open two inquiries under section 13(2) of the Transport Accident Investigation Commission Act 1990. The inquiries were in response to two fatal stevedoring accidents that occurred at two New Zealand ports.
- Separate investigations were conducted into each accident. There were common systemic safety issues identified in the two accidents and the Commission has therefore published the two inquiries in a single report. These systemic issues are relevant to the wider stevedoring industry.
- The first accident occurred on 19 April 2022 at the Port of Auckland. A stevedore, working onboard the container vessel Capitaine Tasman, moved underneath a suspended 40-foot container and suffered crush injuries as a result of the container being lowered onto them. The stevedore was employed by Wallace Investments Limited (WIL), an independent stevedoring company operating at the Port of Auckland.
- The second accident occurred at Lyttelton Port on 25 April 2022. A stevedore, involved in the process of loading coal onto the bulk carrier ETG Aquarius, was discovered, deceased, on the deck of the vessel, buried under a quantity of coal. The stevedore was employed by the Lyttelton Port Company Limited (LPC).
Why it happened
- The Commission found that both WIL and LPC were in the process of improving their respective safety systems. However, at the time of the accidents there were deficiencies common to both organisations. The risks associated with work activity were primarily managed with administrative risk controls, yet robust safety assurance processes to ensure that these controls remained effective were lacking. As a result, neither LPC nor WIL adequately understood how the day-to-day behaviour of their employees was negating the effectiveness of already vulnerable control measures.
- While both organisations were attempting to improve their safety management systems, a lack of cohesiveness within the stevedoring community meant there was little ability to benchmark comprehensively with others in the industry. With no best practice guidelines, no minimum training requirements and few safety-related information-sharing platforms, leadership from within the sector was found lacking.
- Historically, stevedoring has a poor safety record (International Labour Office, 2018), yet it is not regulated with the degree of rigour afforded to other high-risk industries. From a regulatory perspective, neither organisation received a satisfactory level of proactive oversight of their stevedoring operations. Most regulatory interactions were limited to LPC and WIL reporting notifiable events under the Health and Safety at Work Act 2015, and to any subsequent follow-up by Maritime New Zealand (MNZ) and WorkSafe New Zealand (WorkSafe) as a result of those notifications. Reactionary reporting and associated regulatory sanctions provide little insight into the health of an organisation’s safety system or assurance of future safety performance. Nor do they encourage information sharing within the industry to encourage safety growth across the sector.
- The Commission has made five safety recommendations as a result of these two inquiries.
What we can learn
- Those who work in high-risk industries are not necessarily exposed to adverse events on a regular basis. This can lead to a desensitisation to risk, which itself becomes a hazard.
- When risk is not fully understood or appreciated, a variety of factors can lead to employees taking shortcuts or drifting away from rules (see footnote 16 for explanation of human behaviour within organisations). Passive safety messages and reminding people to follow procedures are not effective means by which to change risk perceptions or modify behaviours.
- The way in which tasks are designed and procedures are written is often incongruent with how day-to-day work activity is conducted. A critical component of any safety system is the ability to identify, understand and resolve the reasons for the disparity.
- Where administrative risk controls are necessary to manage hazards associated with high-risk activity, appropriate supervision and a culture of strong safety leadership is required to ensure their effectiveness.
- Industry collaboration and benchmarking is one of the most effective ways to improve safety standards and support continuous improvement.
- Reactive interventions are not a substitute for proactive regulatory oversight of high-risk industries, particularly those with a poor safety record.
Who may benefit
- Regulatory bodies, port organisations, stevedoring organisations, stevedores, vessel operators, anyone designing safety standards, and anyone working in a high-risk industry may benefit from this report and the Commission’s recommendations.
Factual information Pārongo pono
- On 27 April 2022, the Minister of Transport directed the Commission to open two inquiries under section 13(2) of the Transport Accident Investigation Act 1990. The inquiries were in response to two fatal stevedoring accidents that occurred at New Zealand ports. The first accident occurred at the Port of Auckland on 19 April 2022, when a stevedore employed by Wallace Investments Limited (WIL) was crushed by a container during loading operations onboard the Capitaine Tasman. The second accident occurred at Lyttelton Port on 25 April 2022, when a stevedore employed by Lyttelton Port Company Limited (LPC) was buried under a quantity of coal onboard the ETG Aquarius.
- During its two inquiries, the Commission identified commonalities between the two accidents, including several systemic safety issues that are relevant to the wider stevedoring industry. For this reason, the two investigations have been published within a single report.
- This section of the report sets out the context for the investigations, specifically an overview of the stevedoring industry within New Zealand. This includes the hazards associated with stevedoring activities and the importance of having an effective safety management system (SMS). Commonalities between the two accidents are also noted. Section 3 discusses the wider safety issues the Commission identified for the New Zealand stevedoring industry. Section 4 outlines the safety actions that have been taken since the two accidents. Section 5 contains the Commission’s recommendations arising from its two inquiries.
- Appendix A of this report covers the investigation into the accident at the Port of Auckland, MO-2022-203. Appendix B covers the investigation into the accident at Lyttelton Port, MO-2022-202.
Introduction to port operations
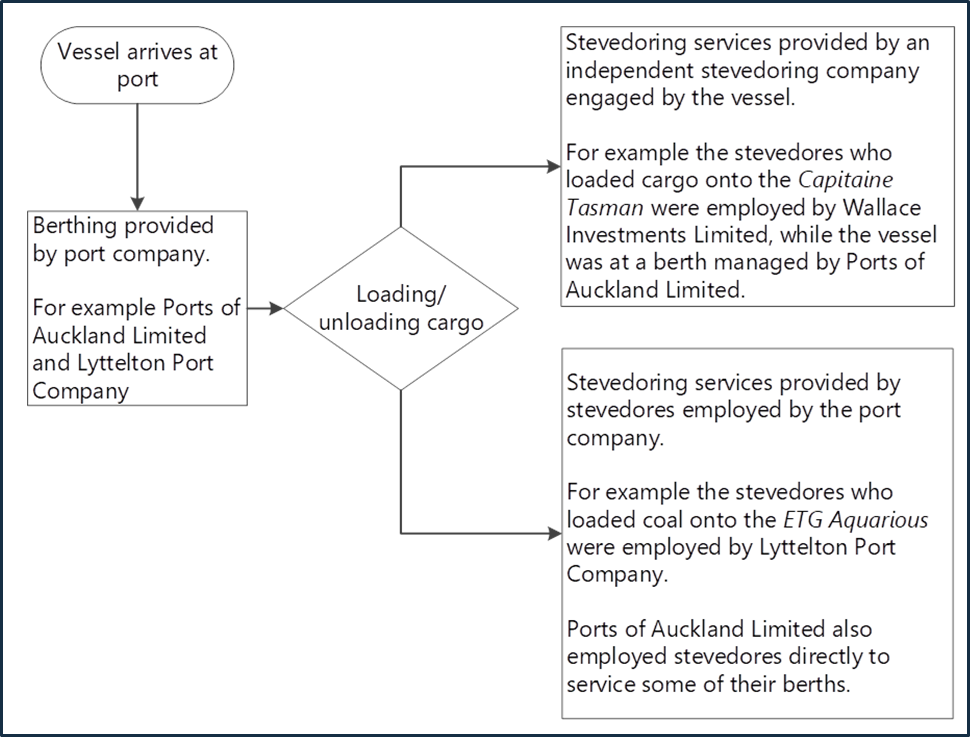
- A port is a location where goods are loaded and unloaded from ships. The two locations where these accidents took place are the Port of Auckland and Lyttelton Port (see Figure 3). Port companies, such as Ports of Auckland Limited (POAL) and Lyttelton Port Company Limited (LPC), operate and manage the infrastructure and facilities at these ports, such as berthing ships, loading and unloading cargo, and providing storage and transportation.
- Stevedoring activity includes loading and unloading of the cargo carried on vessels, stacking and storing cargo on the wharf, and receiving and delivering cargo within the terminal or port facility. Stevedores may be employed directly by the port company, or by a privately owned stevedoring company that is independent of the port company (see Figure 4). Stevedores usually operate in teams, known as gangs. Often, several gangs will be supervised by a foreman. The stevedoring roles within the gangs involved in these two accidents are described in the factual information for each inquiry (see Appendices A and B).
- Shipping companies operate the ships that transport the cargo. Depending on their needs, they can use stevedores from the port company or stevedores from an independent stevedoring company to handle the loading and unloading of cargo at port.
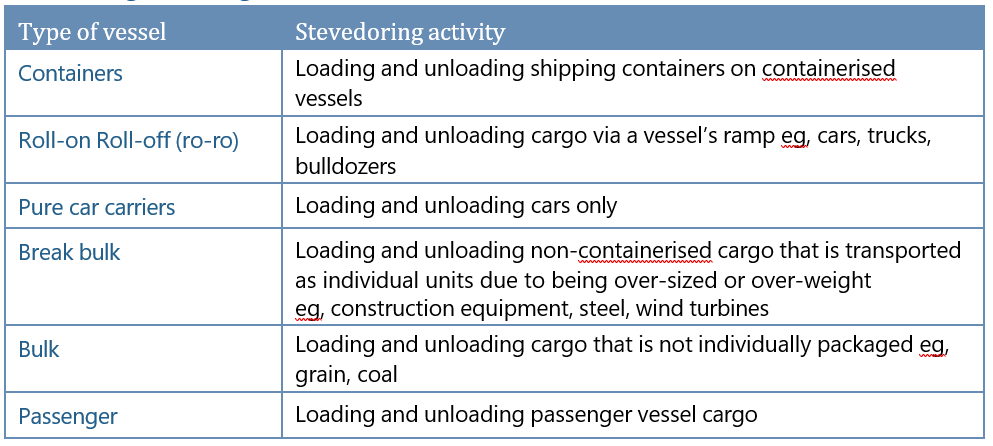
- Stevedores undertake various types of cargo handling (see Table 1):
Regulation of stevedoring in New Zealand
- The Waterfront Industry Act 1953 (WIA) was passed in New Zealand to regulate the operations and conditions of the country's waterfront industry. The WIA was intended to protect the rights of workers and employers in the industry and focused on the efficiency and costs of operations on the waterfront.
- The WIA established the Waterfront Industry Tribunal (judicial functions) and the Waterfront Industry Commission (administrative functions).
- However, it was not until the WIA was reconsolidated and amended in 1976 that the Tribunal and Commission could explicitly consider the safety of the waterfront industry (the Waterfront Industry Act 1976 is sometimes referred to as the Waterfront Industry Commission Act 1976).
- Throughout the 1970s and 1980s several legislative changes ultimately saw the dissolution of both the Tribunal and Commission (the Waterfront Industry Commission Amendment Act 1987 dissolved the Tribunal, and the Waterfront Industry Reform Act 1989 dissolved the Commission).
- These amendments meant that:
- ports were required to employ their own workforces and function under the Labour Relations Act 1987 in the same manner as any other employer
- the common standard of stevedoring labour administration and regulation was removed.
- These changes effectively resulted in deregulation of the stevedoring workforce, and individual ports and shipping agencies became free to set their own rates and practices for the services they provided.
- It was not until the early 1990s that stevedoring attracted safety regulation again, with health and safety on ports falling under the Health and Safety in Employment Act 1992 (HSE) (administered and enforced by the Department of Labour) and on vessels, falling under the Maritime Transport Act 1994 (MTA) (administered and enforced by the Maritime Safety Authority (MSA), which was renamed Maritime New Zealand (MNZ) in July 2005).
- In 2002, safety for work onboard vessels was moved from the MTA into the HSE. At the same time, a provision for designation was also introduced that allowed the Prime Minister to designate an agency to be the health and safety regulator for an industry, sector or type of work.
- In 2003, MSA was given a designation and new appropriation for activity associated with health and safety regulation onboard vessels. Operational agreements to support the designation were developed between the Department of Labour and MSA.
- In 2015, the HSE was repealed and replaced by the Health and Safety at Work Act 2015 (HSWA), administered by the Ministry of Business, Innovation and Employment (MBIE). WorkSafe New Zealand (WorkSafe) was established as the primary regulator for New Zealand’s workplace health and safety, with MNZ retaining their designated role for health and safety onboard vessels.
- HSWA places the responsibility for securing the health and safety of workers and workplaces on the person conducting a business or undertaking (referred to as a PCBU). Port companies and stevedoring companies are PCBUs under HSWA, as are operators of New Zealand-flagged vessels. HSWA does not generally apply to foreign-flagged vessels operating in New Zealand waters. However, it does apply when stevedoring companies are undertaking work onboard foreign-flagged vessels at a New Zealand port.
- Given the designation held by MNZ, in a port environment there are two regulators: WorkSafe is the regulator for any shore-based operations and MNZ is the regulator for operations onboard the vessel. The boundaries between shore-based and vessel-based operations can be ambiguous, for example when a vessel’s crane is being used to lift cargo from the wharf onto the vessel.
- To facilitate cooperation, the two regulators agreed a memorandum of understanding in 2018. Where jurisdictions or interests overlap, joint work programmes are undertaken. If an incident occurs and it is initially unclear who has jurisdiction, both WorkSafe and MNZ will attend.
- HSWA has 16 pieces of secondary legislation that further define the responsibilities of PCBUs, including those that might apply to specified persons or circumstances. One of those is the Health and Safety at Work (General Risk and Workplace Management) Regulations 2016 (HSWA-GRWM), which prescribe a risk management process for certain working conditions. Those working conditions include raised and falling objects and substances hazardous to health – both of which are inherent in some stevedoring activities.
- HSWA-GRWM requires PCBUs, so far as it applies to specific hazards and/or risks as prescribed in regulation, to identify hazards that could give rise to reasonably foreseeable risks, manage them using a hierarchy of control measures, maintain effective control measures, and review and revise control measures to make sure they are effective (see the Managing the risk of harm in stevedoring operations subsection below). The regulations also require the PCBU to ensure that the supervision and training provided to a worker is suitable and adequate. Exactly how the PCBU complies with the regulations is left to the discretion of the PCBU.
- HSWA duties for managing health and safety risks will overlap in shared workspaces such as a port, or when services are being contracted or sub-contracted, such as when a shipping company requires the use of stevedoring services at a port. Organisations are not expected to operate in isolation and HSWA requires that PCBUs must, as far as is reasonably practicable, consult, cooperate and coordinate activities with all other PCBUs with whom they share overlapping duties (HSWA, s 34(1)). Which PCBU is best placed to manage a particular risk depends upon the degree of influence and control the PCBU has in the circumstances. For example, if stevedores are working on a vessel, the stevedoring company may be best placed to manage the worksite itself, but the shipping company would likely have a duty to ensure that equipment such as the vessel’s cranes were maintained to the required standard and were safe to operate.
- Beyond the responsibilities required of a PCBU, there are no additional or specific requirements for stevedoring activity within HSWA. This was also the case under the previous HSE.
- Since the regulation of safety for work onboard vessels was removed from the MTA in 2002, the MTA has no regulations specific to stevedoring organisations. However, there are several rules relating to port activities that are relevant to stevedoring activity.
- The MTA lays out the responsibilities of port operators for maritime safety, including that port operators must not allow the port to be operated in a manner that causes unnecessary danger or risk to vessels, or people and property on vessels.
- There are no existing Maritime Rules specifically regulating stevedores or stevedoring, although some parts contain provisions that apply to stevedoring.
- Regulatory requirements regarding training for stevedoring activity do not extend beyond the primary duty of care laid out in HSWA, to provide information, training, instruction or supervision that is necessary to protect all people from risks to their health and safety arising from work.
- Non-compulsory qualifications for stevedoring exist within the NZQA framework. The New Zealand Certificate in Port Operations offers three options of study: port administration, cargo handling, and heavy machinery.
Managing the risk of harm in stevedoring operations
- Globally, the modernisation of stevedoring has seen increasingly sophisticated technology within port environments. The introduction of containerised shipping and roll-on roll-off (ro-ro) vessels in the 1960s marked a significant change in cargo-handling, which had until then largely remained unchanged. While many of these developments have reduced the level of human-intensive operations, there has not been a comparative reduction in injury risk (Fabiano et al., 2010). Historically, port work had a poor safety record and it is still regarded as an occupation with very high accident rates (Ronza et al., 2005; International Labour Office, 2018). International data from 2022 shows that approximately 34 per cent of incidents involving vessels occurred when docked in port (Rightship, 2023) (where report data identified location).
- Domestically, there have been 18 deaths amongst port workers since 2012. A recent examination of port safety within New Zealand (Port Health and Safety Leadership Group, 2022) shows that the number of fatalities across a 10-year period has remained consistent, averaging 1.8 deaths per annum. As a proportion of the workforce, stevedore fatalities occur at a rate of approximately 20 deaths per 100,000 workers, which is the second highest rate of any sector within New Zealand.
- When compared internationally, New Zealand ports do not move high volumes of cargo (Lloyds List One Hundred Ports, 2022). For example, in terms of container movements per year, most New Zealand ports would be considered ‘small’ (less than 0.5 million TEUs (Twenty-foot Equivalent Units) per year, as defined by Container Port Performance Index 2021). However, New Zealand’s port-worker fatality rate is higher than other countries that move significantly more cargo, such as the United States. In terms of the number of deaths, considering the amount of cargo moved, New Zealand’s fatality rate is two- to three-times higher than both the UK and Hong Kong. The fatality rate for New Zealand stevedores is comparable to Australia, despite the amount of cargo handled being considerably less.
- Falls from height and crushing by machinery or vehicles were the two most common causes of fatalities within New Zealand ports, followed by vehicle crashes and being hit or crushed by cargo.
- The Port Sector Insights Picture and Action Plan (Port Health and Safety Leadership Group, 2022) reported that there were 397 reported notifiable injuries at New Zealand ports between 2012 and 2022, the most common causes being slips, trips and falls, followed by workers being caught between objects. Information provided by sector participants and analysed as part of this work (see paragraphs 4.9 to 4.12 of this report for further information on the Port Sector Insights Picture and Action Plan) suggests a correlation between increasing volumes of cargo and rising rates of harm. In the previous five to six years, MNZ has conducted 39 investigations into PCBUs that were undertaking stevedoring activity at New Zealand ports. Four investigations resulted in prosecution. MNZ also issued five prohibition notices and 19 improvement notices.
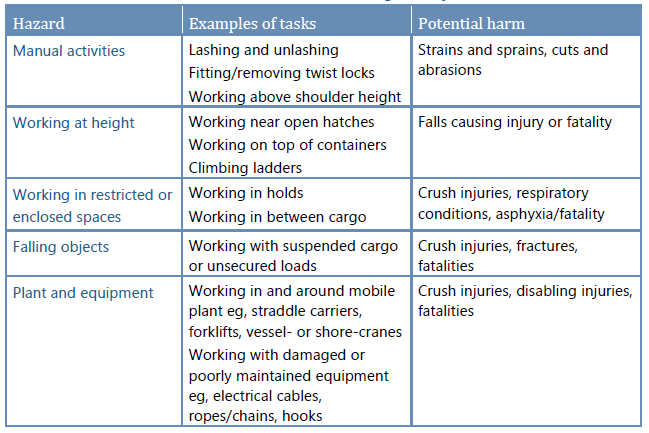
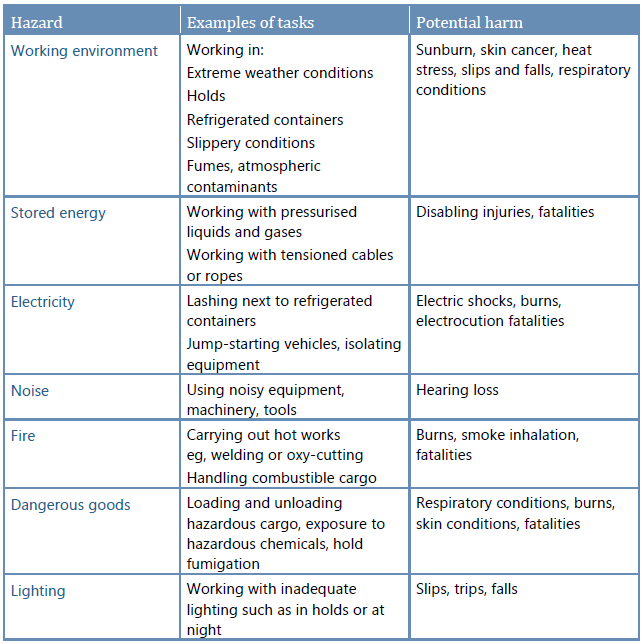
- Hazard refers to anything that has the potential to cause harm. Some activities have an inherently high risk of causing harm because of the nature of the hazards that are associated with the activity. Stevedoring fits into this category because it puts workers near heavy machinery, significant stored energy hazards and dangerous materials, often whilst working at heights (see Table 2).
- Risk management refers to the systematic process of hazard identification, risk assessment and treatment of the risk using risk controls. Risk controls are mechanisms designed to either eliminate, mitigate or reduce to as low as reasonably possible, the unwanted outcomes posed by exposure to hazards.
- Risk controls can be classified according to where on the potential hazard-to-risk trajectory they are employed. Preventative risk controls are put in place to prevent the risk associated with the hazard from occurring. For example, a guard cover over a switch to prevent inadvertent selection of the switch is a preventative risk control. Recovery risk controls are designed to reduce the consequences of the negative outcome should the risk associated with the hazard eventuate. The use of personal protective equipment (PPE) is a common recovery risk control, such as a harness protecting a worker from injury should a fall from height occur.
- There are multiple ways to control risk and the mechanisms to do so can be grouped depending on their level of effectiveness. This is commonly known as the hierarchy of controls (see Figure 5).
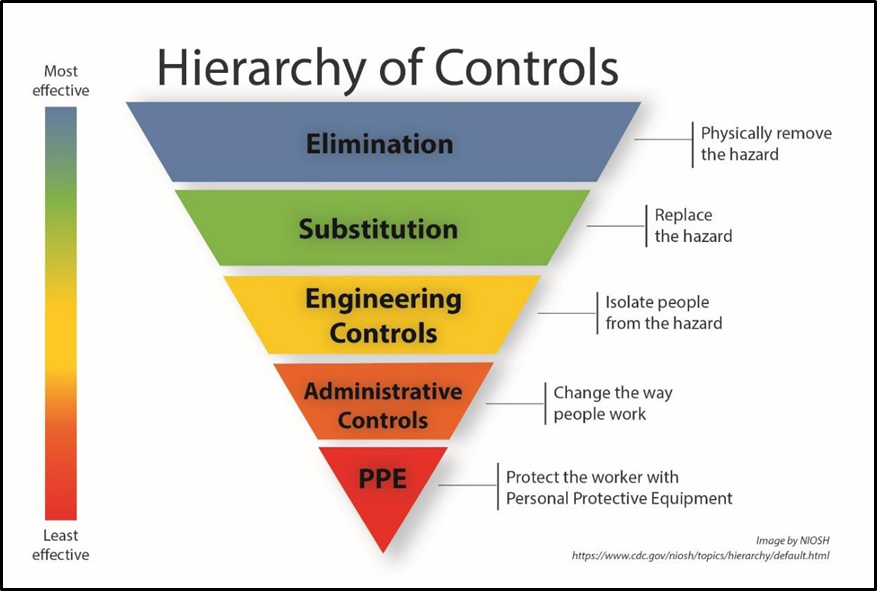
- The most effective way to manage a risk is to eliminate its source by removing the hazard altogether; if the hazard does not exist, no risk is posed. If it is not possible to remove the hazard, then the next most efficient control is reduction of any potential risk. This can be achieved in several different ways; however, some methods are more effective than others.
- Firstly, substitution of the hazard should be considered. This involves replacing the hazard source with something that creates less risk. If this is not reasonably practicable, an engineering control will provide the best defence. Engineering controls are physical in nature and can be designed into a system to protect an individual from the hazard. Guard switches and protective barriers are examples of engineering controls where there is some degree of isolation between the worker and the hazard.
- Less effective than engineering controls are administrative risk controls. These consist of measures such as providing workers with information about the hazard through training and having documented procedures or work instructions in place. Safety messaging is an example of an administrative control. Finally, PPE should be used to protect against any remaining risk.
- HSWA-GRWM requires PCBUs to implement risk control measures, so far as they apply to certain working conditions, in accordance with this hierarchy of controls. If it is not reasonably practicable to eliminate a risk (HSWA-GRWM, r 6(1)), then PCBUs must, so far as reasonably practicable, use substitution, isolation or engineering controls in the first instance (HSWA-GRWM, r 6(3)) followed then by the less effective administrative risk controls and PPE (HSWA-GRWM, rr 6(4) and 6(5)).
- Once risk controls have been established, they must be reviewed and, as necessary, revised to ensure that their effectiveness is maintained (HSWA-GRWM, rr 7 and 8).
Effectiveness of administrative risk controls
- Currently, many of the inherent hazards in stevedoring activities are managed with administrative risk controls. While technological innovation has increased the engineering solutions, most stevedoring operations remain human-centric. As of 2021, there were only 53 container terminals (ports of Auckland’s Ferguson Terminal has since reverted to manual saddle cranes) around the world that utilised some degree of automation, which represents 4 per cent of the total global container terminal capacity (International Transport Forum, 2021). Moreover, while some stevedoring activities could be automated, some of the most dangerous aspects of container handling (such as lashing, and fitting twist locks) are considered more problematic in terms of automation (International Transport Forum, 2021). The degree to which automation will increase port-workers’ health and safety is still uncertain and, with the ability to fully automate ports still some time away, the requirement for stevedores to work in hazardous environments remains. (The argument that increased automation will rapidly lead to a reduction in harm by reducing human involvement in the system, is not straightforward. Automated processes still require supervision and appropriate management. Within the port environment, there is currently little empirical data to support the assumption that the health and safety of container terminal workers has improved in the ports that have introduced automated processes. Several automated ports have had accidents with equipment, including the Ports of Auckland’s Freyberg Terminal, which experienced two separate incidents involving automatic straddle cranes. See International Transport Forum (2021)).
- The primary reason that administrative risk controls are not as effective as other types of risk control is that they rely heavily on compliance. For administrative risk controls to work, employees must always follow instructions, never make mistakes and never put themselves in harm’s way – a concept that is at odds with human behavioural science. (In addition to being susceptible to human error, people rarely always follow rules or instructions precisely. Individuals tend to drift away from rules and procedures as they gain familiarity with the tasks they are performing. While policies and procedures are prescribed to set boundaries for safe operations, workers may experiment with these boundaries to become more productive or obtain some benefit. This experimentation can lead to adaptations of procedures and a shift beyond the prescribed boundaries toward unsafe practices. Without intervention, this can lead to other employees observing what appears to be a successful adaptation of procedures and a spread of such behaviour takes place throughout the workforce. In the absence of any negative repercussions such adaptations are unlikely to be recognised as deviations as often these behaviours result in successful outcomes. Over time, adaptation of procedures slowly becomes the normal behaviour and any risk associated with short-cuts or workarounds is unlikely to be recognised. This is commonly described as ‘normalisation of deviance’, a phrase first used when examining the 1986 Challenger disaster (see Vaughan, (1996)). For an overview of normalisation of deviance in high-risk industries, see Sedlar et al. (2023)).
- There are multiple organisational factors that influence employees and can contribute to engaging in at-risk behaviour. At-risk behaviour is a term used to describe behavioural choices that increase risk, specifically where the risk is not recognised or is mistakenly believed to be justified (Marx, 2009). Common motivators (factors that can encourage people to break rules or not follow procedures (Santiago, 2007)) of at-risk behaviour within organisations are:
- financial gain
- saving time/making life easier
- impractical safety procedures
- unrealistic operating instructions
- unrealistic operating schedules
- demonstrating skill/enhancing self-esteem
- real or perceived pressure from management to cut corners
- real or perceived pressure from the workforce (peers) to break rules.
Common modifiers (factors that tend to increase the probability that people will break rules or not follow procedures (Santiago, 2007)) of at-risk behaviour within organisations are:
- poor perception of safety risks
- enhanced perception of benefits
- low perception of potential injury/damage event
- inappropriate management/supervisory attitudes
- low chance of detection due to inadequate supervision
- insufficient accountability
- complacency caused by accident-free environments
- ineffective performance management/disciplinary procedures.
- Where administrative risk controls are necessary, they require significant and ongoing effort by workers and their supervisors (United States National Institute for Occupational Safety and Health, 2022). Workers must remain appreciative of and alert to the potential risks within their environment. However, the absence or irregularity of adverse events such as accidents or incidents can lead to a desensitisation to hazards. Passive safety messages and reminding people to follow procedures are not effective risk controls when used in isolation. Procedural adherence is more likely when societal norms dictate the desired behaviour eg, everybody else is following the rules in the workplace. How successfully an organisation manages risks depends on the maturity of their safety management system (SMS) and culture.
Safety management systems and safety culture
- Many international transport regulators require industry participants to implement and maintain a formal SMS that is periodically reviewed as part of regulatory monitoring. Within New Zealand, MNZ requires SOLAS (The International Convention for the Safety of Life at Sea (SOLAS) is an international treaty. SOLAS’s main objective is to specify minimum standards for the construction, equipment and operation of ships, compatible with their safety. Flag States are responsible for ensuring that ships under their flag comply with its requirements) vessels to have an International Safety Management System in place (as required by the International Safety Management Code, the International Maritime Organization’s standard for the safe management and operation of ships at sea) and non-SOLAS vessels to have a certified SMS as part of the Maritime Operator Safety System (MOSS).
- An SMS is an established set of systematic processes to identify hazards and manage safety risks. A common framework for an SMS consists of four independent but interrelated components: safety policy and objectives, safety risk management, safety assurance, and safety promotion.
- An effective SMS will have a tightly coupled relationship between safety risk management and safety assurance (Demming, 2023). The risk management process will provide for hazard identification, risk assessment and treatment of the risk using risk controls. The safety assurance function is vital to ensure that risk controls are achieving their intended objectives of managing risk to an acceptable level.
- One of the primary elements of safety assurance includes the ability to measure and monitor safety performance. To do so effectively requires the collection of a wide variety of both relevant and reliable data to determine whether an organisation’s desired safety outcomes are being met. Data sources include employee hazard and safety reports, findings from safety investigations and audits, safety climate surveys, and operational performance metrics.
- Given much of this information is captured from frontline employees, it is essential that organisations not only have suitable reporting mechanisms in place, but also foster a culture in which employees feel comfortable to raise and report on safety issues. Organisational culture is acknowledged as being the most important factor for shaping safety reporting practices; a healthy safety culture underpins a successful SMS (Maurino, 2017; International Civil Aviation Organization, 2018).
- The safety maturity of an organisation encompasses both its SMS processes and its safety culture. While different models of safety maturity exist, the majority bear a distinct resemblance to the original model, which depicts the various levels of an organisation’s journey from safety naivety to safety maturity (see Figure 6) (Westrum, 1993; Reason, 1997; Hudson, 1999).
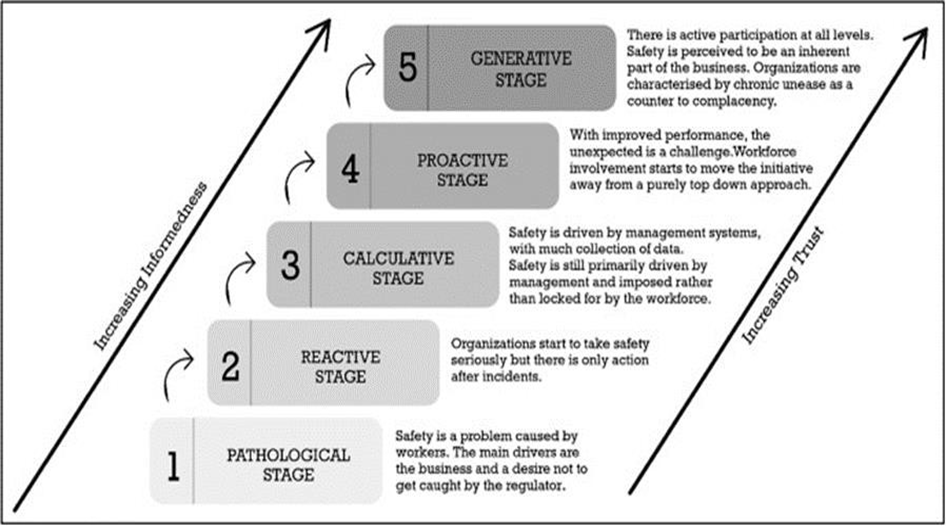
- Safety maturity can be measured by examining different elements across each level of an organisation, considering both the tangible components, such as SMS processes, as well as the more abstract qualities of the system, such as safety culture. An example of the former is how an organisation measures its safety performance. Primarily focusing on Lost Time Injury rates (LTIs) – which do not provide a valid or reliable measure of risk, risk drivers or the effectiveness of risk controls – indicates a less mature safety system (Safe Work Australia, 2013). In contrast, utilising a wide variety of appropriate measures, including leading- or predictive-performance indicators across multiple aspects of an organisation’s activity, would reflect a more mature safety system (Kaassis and Badri, 2018).
- A less tangible aspect of organisational safety maturity is related to culture, including the concept of ‘who causes accidents in the eyes of management’ (Parker et al., 2006) At a pathological stage, accidents are either viewed as ‘bad luck’ or as an accepted part of the job. Management sees responsibility as belonging to the individuals directly involved with the accident and employees are blamed and punished when events occur. As safety maturity increases, so does an understanding of the complexities of human behaviour. Management begins to accept a shared responsibility for accidents and blame is replaced with philosophies such as an organisational ‘just culture’. The generative stage of maturity reflects a true comprehension of the nature of human behaviour and a recognition that safety is an emergent property of a complex sociotechnical system.
- The positive correlation between organisational safety culture and safety outcomes is well documented (Zohar, 2010; Bjornskau and Naevestad, 2013). This has led to regulatory authorities in some sectors evaluating an organisation’s safety culture as part of their monitoring and oversight of industry participants (internationally, commercial aviation is a recognised example where this occurs. Within New Zealand this is a requirement for aviation certificate holders).
Summary
- Stevedores work in an environment with numerous and significant hazards. These hazards require effective management to reduce the risk of harm associated with stevedoring activity. The degree to which this can be successfully achieved is largely dependent on the maturity of an organisation’s safety system. Whether an individual organisation can create, maintain and continually improve its safety system will depend on many factors. Two significant factors are the extent of leadership and cohesion within the wider industry, and the way the sector is regulated. These factors are discussed in Section 3 of this report.
Overview of the two accidents
Maritime inquiry MO-2022-203, Port of Auckland
- On 19 April 2022, a stevedore employed by the independent stevedoring company Wallace Investments Limited (WIL) was working as a hold operator onboard the container vessel the Capitaine Tasman, which was berthed at the Port of Auckland’s Jellicoe Wharf. As a hold operator, the stevedore’s job was to help guide the containers into the vessel’s hold and into their correct positions as they were being lowered by the vessel’s crane.
- At the time of the accident, the stevedore was not in sight of either the crane operator or the second hold operator, who was positioned on a different level of the container stack. As the crane operator was manoeuvring a 40-foot container, the stevedore unexpectedly moved under the suspended load and suffered crush injuries followed by a fall from height when the container was lowered.
- WIL had recognised suspended loads as a hazard. The risk controls used were administrative in nature; employees were given training, procedures to follow, and regularly reminded not to position themselves under a suspended load. However, the procedures did not clearly allocate safety responsibilities before giving direction to the crane operator. The presence of at-risk behaviour in the form of non-adherence to procedures also indicated a desensitisation to workplace hazards and a lack of effective supervisory oversight.
- WIL’s SMS was still in development and had not reached the level of maturity required to provide assurance that risk controls were adequate or that all hazards were being identified. The regulatory framework did little to support the ongoing development of WIL’s SMS, nor was the level of regulatory oversight sufficient to provide assurance of WIL’s future safety performance.
- See Appendix A for details of the Commission’s inquiry MO-2022-203.
Maritime inquiry MO-2022-202, Lyttelton Port
- On the morning of 25 April 2022, a stevedore employed by the Lyttelton Port Company Limited (LPC) was working onboard the bulk carrier ETG Aquarius, which was berthed at the Lyttelton Port coal-loading berth. The stevedore was part of a gang that was loading coal into the number one hold of the vessel. As the coal signalman, the stevedore’s job was to monitor the flow of coal from a conveyor belt into the hold.
- At the time of the accident, the coal signalman was not in sight of any of the other gang members, including the stevedore who was operating the machine delivering the coal to the hold. During the final stages of loading coal into the hold, radio communication was lost between the coal signalman and the stevedore operating the coal-loading machine. The coal signalman was subsequently found buried under coal that was accumulating on the vessel’s deck.
- LPC had taken significant steps to improve safety of its port operations before the accident occurred. It was in the first year of a three-year programme to improve its SMS in regard to risk identification and management. At the time of the accident, LPC had not identified all the critical risks of the coal signalman’s role, which meant that the associated risks, such as medical fitness or working in physical isolation, were not explicitly addressed. The risk mitigation strategies that were in place for the associated risks tended to rely upon informal administrative risk controls, which were not always well articulated within the SMS.
- The training system did not ensure that all staff had a thorough understanding of the associated risks and their mitigation measures, reducing the effectiveness of those risk controls. This was compounded by passive supervision of the coal signalman, which did not ensure compliance with risk controls and safety-critical procedures.
- The regulatory framework did not encourage proactive support, monitoring or assessment, via review or otherwise, of LPC’s SMS to ensure its effectiveness.
- See Appendix B for details of the Commission’s inquiry MO-2022-202.
Commonalities between the two accidents
- Despite the difference in the type of stevedoring activity taking place when the accidents occurred, each of the Commission’s inquiries found notable similarities regarding how safety was being managed at an organisational, industry and regulatory level.
- At an organisational level, the risks associated with work activity were primarily being managed with administrative risk controls, yet robust safety assurance processes to ensure that these controls remained effective over time were lacking. As a result, neither LPC nor WIL adequately understood how the day-to-day behaviour of their employees reduced the effectiveness of the already vulnerable administrative risk controls.
- Both organisations were attempting to improve their SMSs. However, a lack of industry cohesion meant there was little ability to benchmark with others in the industry. With no best practice guidelines, no minimum training requirements, and few safety-related information-sharing platforms, leadership from within the sector was found lacking.
- Neither organisation received a satisfactory level of proactive regulatory oversight of their stevedoring operations. Most regulatory interactions were limited to LPC and WIL reporting their notifiable events under HSWA legislation, and to any subsequent follow up by MNZ and WorkSafe because of those notifications. Reactionary reporting and associated regulatory sanctions provide little insight into the health of an organisation’s safety system or assurance of future safety performance. Nor does it encourage the sharing of information within the industry to support safety across the sector.
- Section 3 considers common safety issues for the New Zealand stevedoring industry.
A1. Appendix A: MO-2022-203 Fatal accident at Port of Auckland, 19 April 2022
A1. Factual information
Pārongo pono
Narrative
A1.1. On 17 April 2022, the container vessel Capitaine Tasman was berthed alongside Jellicoe Wharf at the Port of Auckland, New Zealand, with its starboard side to the quay. The vessel had arrived from Tauranga as part of a routine cargo voyage servicing New Zealand, Australia and the South Pacific islands.
A1.2. Stevedores employed by the private stevedoring company Wallace Investments Limited (WIL) carried out loading and discharging of containers. The stevedores used the vessel’s three deck cranes to transfer the cargo between the vessel and the wharf.
A1.3. On 18 April 2022 the discharge of containers was complete and loading had started. Loading operations continued until the evening of 18 April when work stopped for the night.
A1.4. On the morning of 19 April 2022, two stevedore supervisors were rostered to oversee the cargo operation. The supervisors both arrived on site at approximately 0700 to discuss the plan for the day and to check that the wharf area and vessel were ready for cargo operations to start.
A1.5. At approximately 0730, the day-shift stevedores assembled at the vessel’s gangway for a pre-start briefing given by the two supervisors. The briefing covered details of the loading plan for the cargo as well as safety-related information pertaining to the work activity (see paragraph A1.61).
A1.6. The stevedores were pre-organised to work in three gangs: one gang assigned to each of the vessel’s three cranes. The stevedore involved in the accident was assigned to gang number three. Gang three was to load 47 containers using crane number three. The roles of the stevedores within the gang are described in Table 3.
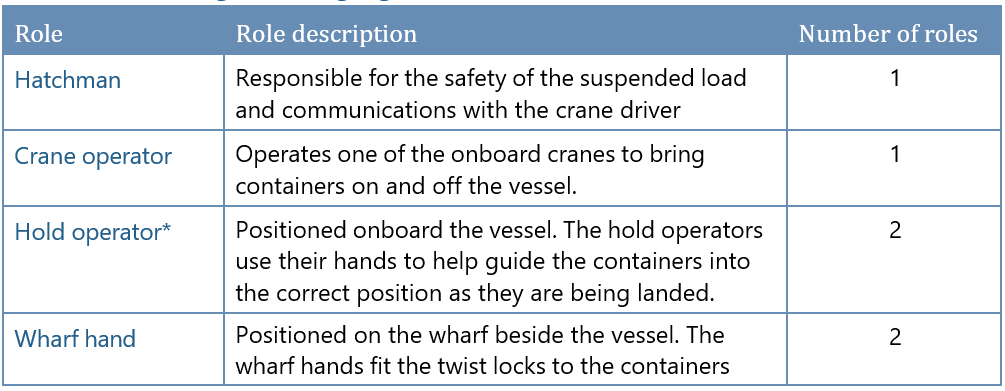
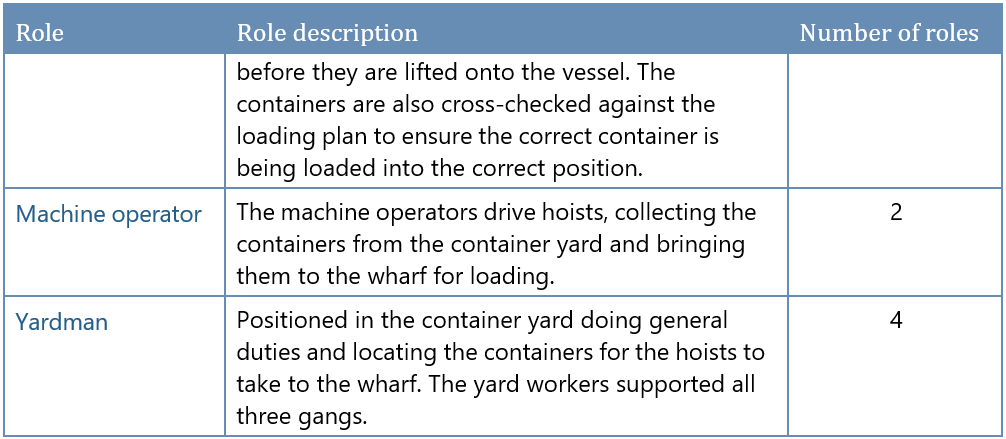
*The deceased stevedore had been working as one of the two hold operators.
A 1.7. As loading was about to begin, the number one crane would not start. The issue was rectified, but the crane subsequently lost power again for approximately half an hour. To accommodate for the lost time, the supervisors redistributed some of the containers from gang one to gang two. One of the supervisors then left the port and went to the company office to query what was thought to be some missing cargo.
A1.8. By about 0850, gang three had loaded twenty 20-foot containers onto the main deck of the vessel in bay 32 (See Figure 7) (location numbers used to describe a containers longitudinal position on the deck of the vessel from forward). The crane’s spreader was then changed to accommodate the loading of 40-foot containers, which were to be stacked on top of the previously loaded 20-foot containers.
A1.9. At about 0910, the fifth 40-foot container was delivered from the container yard to the wharf for gang three to load. Two wharf hands from gang three fitted twist locks to each of the four bottom corner castings of the container. They attached the spreader onto the container and signalled to the number three crane operator that the container was ready to be lifted onto the vessel.

A1.10. At 0912 the crane operator lifted the 40-foot container from the wharf. The stevedores on the wharf observed it had an uneven weight distribution, resulting in the container being on an incline when suspended so that the forward end (reference to the orientation of the containers is in relation to the forward end of the vessel) of the container was lower than the aft end.
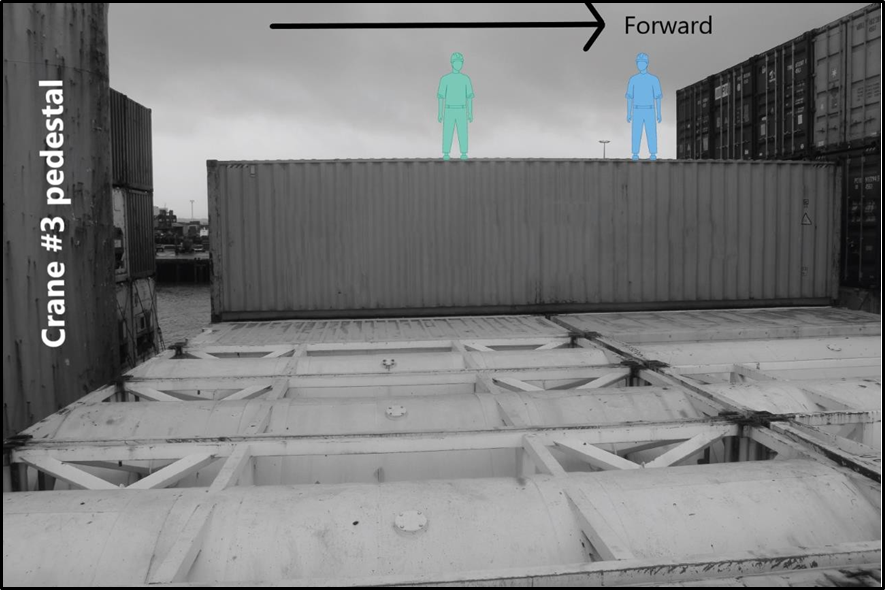
A1.11. Two stevedores in gang three (hold operators A and B) were positioned on the second tier (refers to the number of containers stacked on top of each other) of containers (see Figure 8). The hold operators’ task was to guide the containers into the correct position as the crane lowered them. At the time the container was being lifted from the wharf, the hatchman had left the vessel to collect a rain jacket.
A1.12. As the crane operator manoeuvred the container from the wharf onto the vessel, the forward port-side twist lock of the container made contact with a container on the bottom tier, resulting in the twist lock moving slightly within its casting.
A1.13. At 0913, the crane operator attempted to land the 40-foot container onto the vessel. However, the misalignment of the forward port-side twist lock prevented it from locking into the 20-foot container below. When the crane operator lifted the container back up to attempt to re-land it, the twist lock dropped out of its casting and fell onto the container below, obstructing the corner casting of the 20-foot container on which it was to rest.
A1.14. To rectify the issue, hold operator A (the deceased) descended onto the tier of containers below. To enable them to access the lock once they were down, the crane operator manoeuvred the 40-foot container so that its aft end was resting against the turret of the crane. Hold operator A then lowered themselves down onto the first tier of containers using the spreader wire for assistance (when the chains and wire of the spreader are slack, a stevedore can lower themselves down a level of containers by hanging onto the wire for support, much like an abseiling movement).
A1.15. Once down on the first tier, hold operator A repositioned the displaced twist lock into the top corner casting of the 20-foot container (placing the twist lock upside down into the top of the 20-foot container achieved the same result as placing it the correct way up into the bottom casting of the 40-foot container in that the containers would still lock together in the correct fashion). Hold operator A remained on the first tier of containers and hand-signalled to the crane operator that the landing could be re-attempted (see Figure 9).
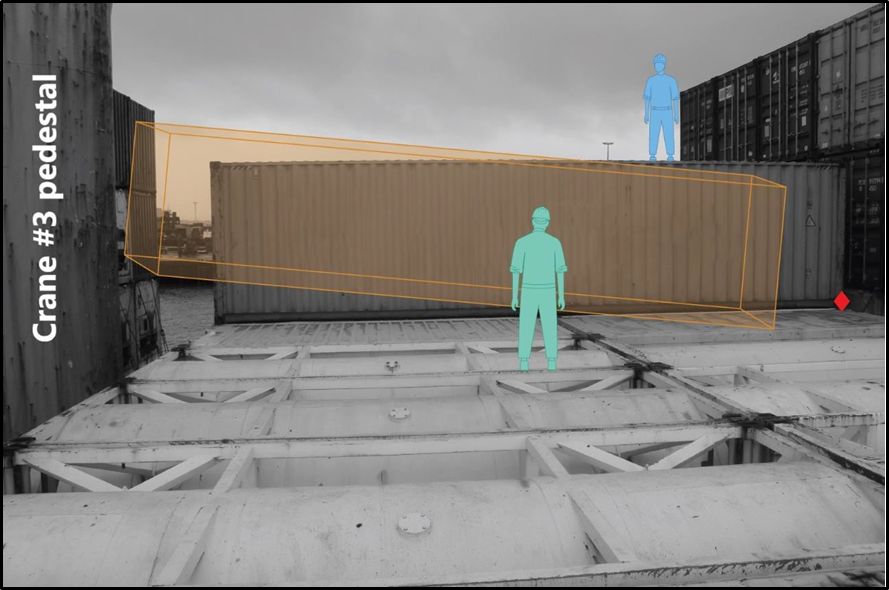
A1.16. At about 0916, the crane operator raised the 40-foot container and began to reposition it for landing. The crane operator was taking signals from hold operator B, who had remained on top of the second container tier (blue figure in Figure 9). Due to the unequal weight distribution within the container, the crane operator landed the forward, heavier end of the container first and then lowered the aft end.
A1.17. As the container was being repositioned, one of the vessel’s crew members was positioning lashing equipment (rods and turnbuckles used to secure the first two container layers to the deck) on the main deck. As they neared the turret of the number three crane, the crew member observed hold operator A standing on the edge of the row of 20-foot containers. They appeared to be in position to guide the aft end of the container as it was being landed (see Figure 10).

A1.18. At the time the crew member observed hold operator A, the 40-foot container was suspended approximately 1.5 metres above the first tier. The crew member then saw the hold operator bend down and move underneath the suspended container, reaching with their arm toward the aft port side of the container.
A1.19. Almost immediately after observing this, the crew member saw the container lower, resulting in hold operator A being pinned under the container and crushed by its weight.
A1.20. The crew member attempted to alert the crane operator by shouting but, due to the proximity of bay 32 to the number three crane, could not signal the crane operator visually. The crew member then observed the container rise a small amount and hold operator A fell from the 20-foot container onto the main deck (see Figure 11).
A1.21. The crew member, who could not see hold operator B from their position on the main deck, ran to the starboard side of the vessel and alerted the other stevedores, who were working on the wharf.
A1.22. The crane operator, unaware of what had happened below, was having difficulty locking the aft end of the container in place, so stood up at the crane controls and looked down through the forward window of the crane cab (see Figure 12). The crane operator observed the victim lying face down on the vessel’s main deck and shouted to alert hold operator B on the second tier of containers. The crane operator then used their cell phone and attempted to call the hatchman (See Table 3 for description of stevedore roles). However, the call went unanswered.

A1.23. Upon being informed of the accident by the crew member, the stevedores who were on the wharf boarded the vessel and attempted to render assistance. One of the supervisors who had been talking with gang three’s hatchman at the vessel’s gangway when the accident occurred, called emergency services on their cell phone.
A1.24. Within 10 minutes emergency assistance had arrived. The stevedore was pronounced deceased at the scene.
Personnel information
A1.25. Hold operator A was an employee of the Wallace Investments Limited (WIL) stevedoring company. They had joined WIL in 2018 and began by working in general duties (general duties typically involve non-specialised tasks such as operating machines in the container yard, unlashing cars and containers) before moving up to work as a hold operator on containerised vessels. During their time at WIL, the stevedore had completed the New Zealand NZQA Level 3 Certificate in Port Operations (Cargo Handling).
A1.26. Hold operator B had also joined WIL in 2018. They also held a New Zealand NZQA Level 3 Certificate in Port Operations (Cargo Handling).
A1.27. The hatchman, who had been working as a stevedore in Auckland for over 20 years, held NZQA Assessments 20048 Operate Ships Crane, and 18954 Drive a motor vehicle within a port environment. The hatchman also trained crane operators when required.
A1.28. The crane operator joined WIL in 1998 as a casual employee engaged in general duties. In 2004 they became a permanent employee and trained to operate cranes in 2005.
A1.29. Supervisor A had worked for WIL for approximately ten and a half years. They held a New Zealand NZQA Level 3 Certificate in Port Operations (Heavy Machinery).
A1.30. Supervisor B had previously been employed in an administration role at another stevedoring organisation before joining WIL in 1998.
Vessel information
A1.31. The Capitaine Tasman was a Singapore-flagged container vessel operated by the Neptune Pacific Agency Australia. The vessel had a capacity of 1,730 twenty-foot equivalent units (TEU) in its four holds and deck area.
Onboard lifting equipment
A1.32. The vessel’s cargo-handling equipment consisted of three onboard cranes. Each crane was operated from a cab that was accessed via internal ladders within the crane pedestals.
A1.33. Each crane had the ability to slew 360 degrees and had a safe lifting weight of 45 tonnes. Crane number three (see Figure 13) had a work radius of 3.5 metres to 29.0 metres and the maximum hoist speed with a load was 19 metres per minute.
A1.34. Routine maintenance for the cranes included an annual service of the cargo hooks and crane sheaves by the vessel crew. Every three months, the cranes were greased and the wires were inspected. Each month a visual inspection and test of the cranes was carried out. The most recent monthly visual inspection had occurred on 27 March 2022. A rocking test on all three cranes had been conducted on 26 March 2022.
Recorded data
A1.35. Ports of Auckland Limited provided CCTV footage of the accident to the Commission.
Medical and pathological information
A1.36. The hold operator sustained crush injuries as a result of the accident. The accident was fatal. Toxicology results were negative (clear) for any performance-impairing substances.
Organisational information
Ports of Auckland Limited
A1.37. Ports of Auckland Limited (POAL) is a public company, wholly owned by Auckland Council. The port’s multi-cargo facility encompasses five wharves, including Jellicoe Wharf where the Capitaine Tasman was berthed at the time of the accident. The multi-cargo division of POAL manages the berthage and wharf space for cargo vessels servicing Auckland. This includes container vessels, vehicle carriers and multi-purpose general-cargo vessels for bulk and breakbulk cargo.
A1.38. Many of the port’s activities are continuous over a 24-hour period, including some stevedoring activities. POAL’s multi-cargo operations staff were on site from 0700 to 2300 on weekdays and from 0700 to 1500 on weekends. Outside these hours an on-call function was provided.
A1.39. Cargo-handling services at the port were provided by either POAL or privately operated stevedoring companies. At the time of the accident there were two primary stevedoring companies, one being WIL. Procurement of WIL stevedore services involving vessels did not involve POAL; arrangements were made directly between the shipping companies or their shipping agents and WIL.
A1.40. When required to help separate different operations on the multi-cargo wharf area, POAL allocated workspaces using concrete blocks or cones. Within these workspaces, whoever was conducting the operations was responsible for all aspects of the activity including safety. Common areas of the port, such as roadways or shared container areas, required each operator to follow POAL’s Common User Safety Protocols (CUSP).
A1.41. POAL contracted WIL as their multi-cargo inter-wharf service provider. This service provided transportation and stacking of containers between the various wharves. When an operator contracted directly to POAL, such as WIL did when providing multi-cargo inter-wharf services, they were required to follow the CUSP.
A1.42. If an on-wharf operator had a contract with another organisation for services provided at the port (such as the contract between a stevedoring company and a shipping company), responsibility for worksite safety was managed between the two parties. In these cases, POAL staff would have some degree of oversight of the operations taking place on the wharf. If dangerous activity was observed, POAL could intervene or issue a stop-work notice to the operator.
A1.43. Operations taking place onboard the vessels were not monitored by POAL. Any work within a vessel’s hold was unable to be observed by the CCTV units on the wharf.
Wallace Investments Limited
A1.44. At the time of the accident, Wallace Investments Limited (WIL) was the largest private stevedoring company operating on the Port of Auckland. WIL was established in 1998 and specialised in conventional cargoes. WIL handled most containerised operations at the port as well as the multi-cargo inter-wharf services.
A1.45. WIL employed approximately 200 stevedores including twelve supervisors. WIL’s management structure consisted of a Managing Director and a General Manager. They were supported by an Environment, Health and Safety (EHS) Manager and two EHS Supervisors.
Staff training
A1.46. Stevedore training provided by WIL for the different roles was through on-the-job training and shadowing other stevedores.
A1.47. Crane operator, hold operator and hatchman duties required more formalised training and an assessment conducted by a training supervisor (WIL employed two training supervisors who assessed different types of stevedoring operations in accordance with NZQA standards). All employees were also able to enrol in the NZQA Certificate in Port Operations as part of their training and development.
A1.48. Safety training for new WIL stevedore employees consisted of a generic POAL induction video. Stevedores were also required to watch a WIL safety-induction video that covered evacuation procedures, how to report safety issues, hazard awareness, staff responsibilities for safety, the role of the health and safety committee, and general safety rules such as drug and alcohol use, PPE, vehicle safety and accident management.
A1.49. Following an accident onboard the Capitaine Tasman in 2021 (see paragraph A1.56), additional safety-related training had been developed around working at heights. This included use of the man-cage, the requirement to be harnessed when working less than two meters from an exposed edge, and the order in which to stack containers to maximise a safe work area for hold operators.
A1.50. Safety messaging, including the dangers of suspended loads, was also presented through a video feed in the lunchroom.
Stevedore gang structure
A1.51. When operating all three cranes on the Capitaine Tasman, the stevedores worked in three gangs, each gang working with one crane.
A1.52. At WIL, stevedores working in the hatchman role were also assigned the title of ‘foreman’. While there were no formal responsibilities associated with this title, those working in the hatchman position were typically the most experienced stevedores and the role of foreman was understood by the gang to hold an element of leadership within the gang.
Container loading procedures
A1.53. WIL’s operational procedures described the work activity required to load and discharge cargo on a container vessel (WIL-SWMS-002 Safe Work Method Statement – Discharge/Load Containers). The procedures were broken up into 12 subtasks. Subtask number eight described the off-load procedure in detail and stated that the process was to be reversed for loading of containers:
- Lashers unlash containers as per instruction of foreman
- Hatchman directs crane operator to container to be lifted
- Crane operator positions wire in correct position
- Hold operators attach spreaders, wires and hooks securely to container and signal when completed
- Hatchman directs crane operator to move container to position on wharf
- When container secure on wharf, general hands unhook wire (if used) from container
- General hand notes the container number in the appropriate log
- Directs mobile operator to move container to yard
A1.54. Roles and responsibilities during container loading operations were also documented in the procedures (WIL-SOP-068 Roles and Responsibilities – Container Vessels). The supervisor responsibilities included:
- Facilitate that the vessel is planned and worked in a safe way
- Communicate to all personnel working on or around the vessel regarding the operating and any hazards that may be encountered
- In the event you identify procedures not being followed, STOP and rectify
- Make regular observation of all personnel working under them and remedy any shortfalls
- Encourage employees to report all hazards they encounter. The foreman/hatchman responsibilities were listed as:
- Be clearly visible to the crane driver always. If this is not possible other means of communication shall be used eg, portable radio
- Give the crane driver clear and efficient signals using standardised signals
- Keep the hook in sight as much as possible
- Check that the load is fully hooked on or unhooked and the load does not exceed the SWL of the gear before giving the signal to hoist
- Do not walk away from hatch when a load is on the way up – Foreman should follow units until they (units) are at rest ie, on vessel/wharf. Not to lose contact visually with unit until unit at rest
- Do not allow any improperly slung load to be lifted
- In the event you identify procedures not being followed, STOP and rectify.
- The crane operator responsibilities included:
- Follow all signals given by the Hatchman
- Follow stop signals given by any person as it may be an emergency. The hold operator responsibilities included:
- Be clearly visible to the crane driver always. If this is not possible other means of communication shall be used eg, portable radio
- If required give the crane driver clear and efficient signals using standardised signals.
- If you observe personnel venture within 2m of an unprotected edge with no fall protection, STOP operation till procedure is adhered to
- Avoid personnel standing or passing under suspended loads by either directing personnel away from working an area or not directing movement of the load until area is clear One person shall be in sight of the foreman to give emergency signals
- Keep the hook in sight as much as possible
-
Get into a safe position when a load is on the way up or down.
A1.55. Other, more general procedures included the following instructions:
For the hatchman (WIL-SOP-05 Standard Operating Procedure – Hatchmen):
- The hatchman is responsible for any suspended load at all times
- Ensure that the hook is in sight at all times
-
Do not leave position until crane driver is safely on deck.
For the crane operator: (WIL-SOP-027 Standard Operating Procedure – Crane Operator)
- Follow instructions of hatchman and staff at all times
-
Obey all signals given by the hatchman.
For the deck and hold operations (WIL-SOP-009 Standard Operating Procedure – Deck/Hold Cargo Operation):
- Don’t work under suspended loads.
Risk Management
A1.56. About 15 months before the accident, WIL initiated a review of their SMS. This was partly in response to an accident in February 2021, in which a stevedore suffered serious injuries when they fell from height while loading containers on the Capitaine Tasman. As a result of the review, WIL were taking steps to improve management of their workplace safety, including upgrading technology, an external quality accreditation, appointment of a new safety manager, and introduction of a critical risk management framework.
A1.57. In January 2021, WIL began transitioning to a new software platform, Mango, to manage their health and safety system and improve internal audit functionality and capability. At the time of this accident in 2022, WIL was not yet using all the safety management functionality that the Mango platform was able to provide, and further customisation was being developed.
A1.58. In May 2021, WIL conducted an internal gap analysis in preparation for ISO 45000 safety accreditation (ISO 45001 is an international standard for health and safety in the workplace). Certification was achieved in November 2021 following two Telarc (Telarc Limited is a Crown Entity Subsidiary owned by the Accreditation Council and recognised as a Certification/Registration Body by the Joint Accreditation System – Australia and New Zealand) audits across a period of three months.
A1.59. In August 2021, WIL appointed a new EHS manager. Following a series of internal audits, on-job observations and review of WIL’s health and safety data, the EHS manager developed a critical-risk-management framework. WIL was in the process of rolling out the framework at the time of the accident and new documentation on how critical risks were to be identified, managed and reviewed had been issued on 9 February 2022 (WIL-SOP-100 Critical Risk Management), two months before the accident.
A1.60. Ten critical risks had been identified by WIL across all stevedoring activities undertaken. These included falling from height, crushing and lifting operations. Critical risk controls were known as ‘lifesavers’. These were: equipment inspections, vehicle pre-start checks, safe zones, use of positive communication between personnel, following procedures, being trained and competent for the task, and working to the conditions.
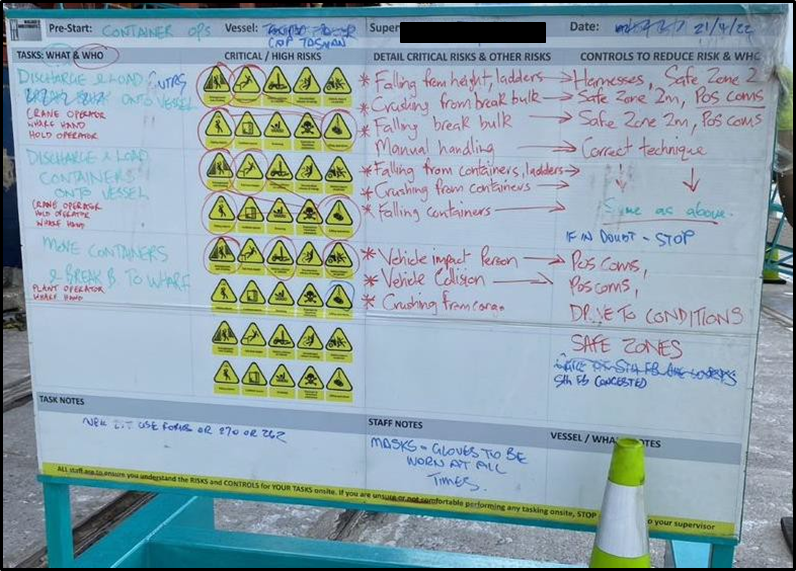
A1.61. The supervisors overseeing the gangs conducted pre-start meetings at the beginning of every shift on an operational worksite. Critical risks associated with each role within the gang were identified along with the applicable lifesaver controls. The briefings were recorded on a whiteboard and were photographed and uploaded to Mango for safety assurance purposes. The pre-start board for 19 April 2022 (the date on the board has been changed to reflect the pre-start briefing which took place when operations resumed following the accident, however, the content remains the same as it was on the morning of the event) is shown in Figure 14.
Safety Assurance
A1.62. Following their ISO accreditation in November 2021, WIL had undertaken work to further develop their internal safety-assurance processes. This included expansion of their internal audits as well as improvements in their incident and hazard reporting.
A1.63. At the time of the accident, WIL had procedures in place for Safe Act Observation (SAO). This was a move to encompass more proactive safety assurance, whereby any employee could report an example of work conducted safely. Introduction of SAO allowed for Key Performance Indicators (KPIs) to be established to measure safe working practices and employee reporting rates within the safety system. Previously, only incidents or non-compliances had been recorded, and training competencies had not been assessed against a regular schedule and were only conducted in response to safety-related incidents.
A1.64. Other recent safety-assurance measures included: verification that any corrective actions raised from an internal safety investigation were appropriately addressed and closed (VERA); verification that any newly established procedure had been appropriately implemented (VIP); and quarterly internal audits of high-risk environments. These processes were supported by regular safety meetings, which included the daily pre-start meetings. Quarterly EHS meetings were established and these informed WIL Management Review meetings. As a major on-wharf operator, WIL also attended regular multi-cargo health and safety meetings chaired by POAL.
A1.65. Employees of WIL were encouraged by management to raise any safety concerns with their supervisors on site. This included hazards, near misses, incidents or accidents, as well as any unsafe behaviours that were observed. Paper-based forms were also available in the gear store and lunchroom. The introduction of the new Mango safety software, in 2021, allowed reporting to be done via an electronic app. At the time of the accident, this function was primarily used by supervisors to capture issues raised verbally with them by the stevedores. Reports submitted into the system were reviewed by the EHS team to determine whether any further follow-up by way of an internal investigation was required.
Regulatory oversight
A1.66. As a stevedoring company undertaking work onboard a foreign-flagged vessel, WIL had a duty of care for the health and safety of its employees whilst operating on the Capitaine Tasman. The HSWA-GRWM regulations (HSWA-GRWM Part 1 General duties rr (5), (6), (7), (8)) required WIL to demonstrate that they were identifying hazards and managing risk regarding specific situations. This meant WIL had to eliminate risk as far as reasonably practicable, and then to minimise any relevant remaining risk as far as reasonably practicable.
A1.67. WIL reported any notifiable events under HSWA to Maritime New Zealand (MNZ).
Depending upon the severity of the event, MNZ could investigate and impose sanctions. Following the accident on 19 April 2022, MNZ issued WIL with a Prohibition Notice (instruction to stop workplace activity until further notice). MNZ inspected WIL’s container operation on 23 April 2022 and subsequently lifted the prohibition.
A1.68. Aside from the high-level joint HSWA assessments of the major commercial ports by MNZ and WorkSafe, action taken by the regulators was largely because of an accident or incident. There was little proactive safety interaction between either WorkSafe or MNZ and WIL. There were no requirements for either regulator to inspect or review WIL’s safety management system.
A2. Analysis Tātaritanga
A2.1. This section analyses the circumstances surrounding the event to identify those factors that increased the likelihood of the event occurring or increased the severity of its outcome. It also examines any safety issues that have the potential to adversely affect future operations.
A2.2. During container loading onboard the Capitaine Tasman, a stevedore working as a hold operator moved under a suspended 40-foot container that was subsequently lowered. The stevedore’s movement was unobserved by any of the other stevedores working in the gang.
A2.3. WIL was continually improving its SMS. However, safety processes were not adequate to provide assurance that all hazards were being effectively controlled.
Rectification of the displaced twist lock
A2.4. Loading operations had been uneventful for gang three until the movement of the fifth 40-foot container, which was being stacked as part of the second tier in bay 32. The container had an uneven weight distribution, resulting in the forward end hanging lower than the aft end. The crane operator became aware of the imbalance as they lifted the container from the wharf but did not consider the load to be unsafe or difficult to manoeuvre.
A2.5. The crane operator attempted to compensate for the imbalance as they slewed the container across the first tier of the stack. However, in not raising it high enough to compensate for the imbalance, the proximity of the lower hanging forward end to the first tier of containers was such that the port-side twist lock made contact with one of the containers and caused it to dislodge in its casting. As the container was being landed, the twist lock fell out and became stuck in the corner casting of the container below.
A2.6. Twist locks falling out of their castings is not uncommon, particularly in the case of the automatic twist locks that were being used on the Capitaine Tasman. In this case the lock had to be physically removed for the container to be landed properly. To get down from the second tier of containers to the first tier, the hold operator could either have used the man-cage or the spreader wire.
A2.7. Using the man-cage would have required the crane operator to transport the container back to the wharf for the wharf hands to disconnect the container from the spreader and enable the spreader to return to the vessel. A hold operator could then have stood in the spreader’s man-cage and been lowered by the crane operator onto the first tier of containers. After repositioning the twist lock the hold operator could have ridden back in the man-cage up to the second layer of containers. The crane operator would have then returned the spreader to the wharf and had the container reconnected ready for loading.
A2.8. The second option was to use the wire technique, using the spreader wire. This involved a crane operator resting the container down until the chains and wire of the spreader were slack. A hold operator could lower themselves down the container by hanging onto the wire for support. This was the technique hold operator A used on the day of the accident.
A2.9. As part of their safety improvements around working at heights, WIL had elected to discontinue using the wire technique approximately a year before the accident. Personnel were to stand in the spreader man-cage when being transported to and from a container (WIL-SOP-026 PPE) and were instructed not to ride wires or chains (WIL Safe Work Pack, Accessing and working at height on containers - Vessels v. 3.0). However, using the spreader wires was a quicker means of moving between container tiers, as it did not require time for the container to be removed ashore. Information provided to the Commission during interviews indicated that some employees still regularly used this method despite the change in procedures.
Findings
1. The wire technique used by hold operator A to descend from one tier of containers to another was no longer an approved practice, but was still being used by stevedores at the time of the accident.
Unseen movement under the suspended load
A2.10. After the twist lock had been refitted, hold operator A moved into a position where the crane operator was able to see them and signalled to the crane operator for the container to be re-landed. It was the last time the crane operator saw hold operator A, whom they expected to remain in the same position until the container had landed. Hold operator A was also out of sight of hold operator B, who remained on the second-tier containers. From this point on, the crane operator was focused exclusively on hold operator B on top of the second tier as they needed to follow their signals to land the container.
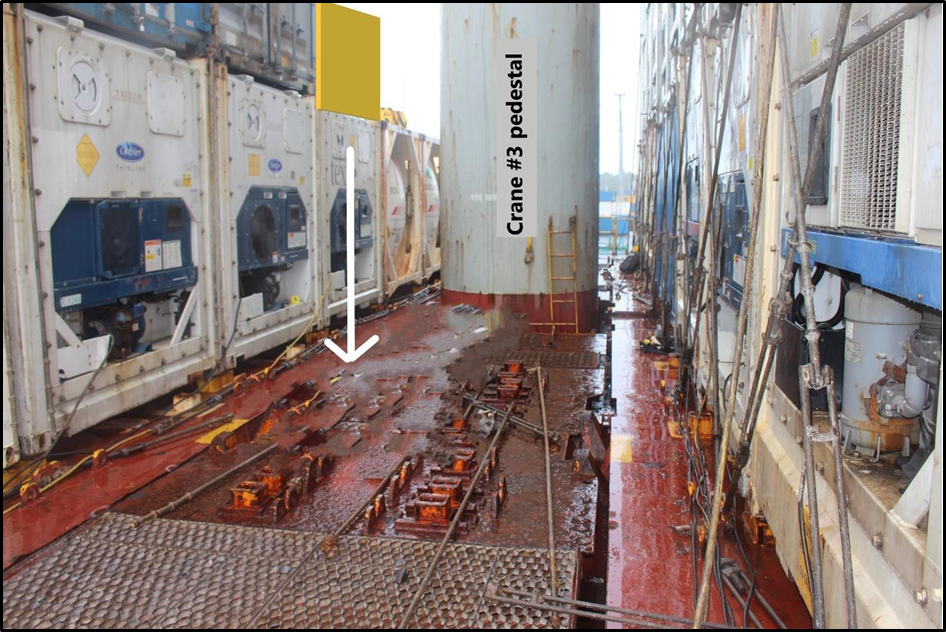
A2.11. Because the heavier (forward) end of the container needed to be landed first, hold operator B had moved to the forward end of the container stack. The result of this was that the crane operator’s attention was now being directed away from hold operator A on the first tier. Exacerbating this was the proximity of bay 32 to the pedestal of the crane; when the crane operator was seated in the cab, the final movements of hold operator A on the first container tier could only have been observed by looking through the floor grating (see Figure 15).
A2.12. At the time of the accident, the floor grating was partially covered by the crane operator’s bag and by a loading plan that had been left on the floor by a previous operator. These items restricted visibility through the floor grating and reduced any opportunity to observe hold operator A moving into an unsafe position. However, the Commission believes it is unlikely that the crane operator would have noticed the hold operator’s movement even if they had unrestricted visibility (Changes in the environment are less likely to be noticed during tasks demanding increased attention, as the visual angle between the location of the change and the fovea increases, and the more that an event is unexpected to occur (Wickens et al., 2021)).

A2.13 Why hold operator A moved under the container while it was suspended is unknown, but it is likely they became aware of an issue with the twist lock fitted to the aft end of the container. The vessel’s crew member saw the hold operator quickly ducking under the load and appearing to stretch out their hand toward the port side of the container. Further, following the accident when the container was returned to the wharf, only the two starboard twist locks were found in their castings. The port-side forward twist lock had remained in the top of the 20-foot container’s casting, where hold operator A had repositioned it after it had become displaced, however the aft port side twist lock was missing from its corner casting on the 40-foot container.
A2.14. A twist lock was subsequently found on the vessel’s main deck in the immediate vicinity of where hold operator A fell. It did not belong to the vessel (container vessels carry their own supplies of lashing gear. Each ship will have different types of locks for different areas of stowage. However, these locks will all be produced by a particular manufacturer. In the case of the Capitaine Tasman, all the lashing equipment was manufactured by German Lashing. Locks are not to be mixed between vessels and the Capitaine Tasman’s Cargo Securing Manual explicitly stated ‘Mixing of smart locks with other types of locks or other maker’s locks is not allowed’) and was different from those being used on the Capitaine Tasman (the correct lock for the 40-foot container was a SL-1 Smartlock manufactured by German Lashing. The lock found by where the stevedore fell was a TL-FA Smartlock made by a different manufacturer). It is considered likely that this lock had been fitted by the wharf hands before the container coming on-board the vessel. The lock was similar in design to the twist locks being used on the Capitaine Tasman and may not have been recognised as being different from the others being fitted. As container corner castings are manufactured to a universal standard, the lock would fit normally when inserted. Had hold operator A noticed the presence of a different lock while the container was still suspended, or if the lock appeared misaligned in some way because of the different design, it may explain why they moved underneath the load.
A2.15. The dangers posed by suspended loads and the potential for crush injuries to occur was communicated to stevedores during their training and as part of the daily pre-start meetings. It is virtually certain that hold operator A was aware of this risk. However, familiarity with a task can lead to more automated behaviour and an increased vulnerability to error (Rasmussan, 1982; Reason, 1990).
Findings
2. Hold operator A suffered crush injuries when they moved underneath a suspended 40-foot container that was subsequently lowered.
3. It is likely that hold operator A moved underneath the container to rectify an issue with the aft port-side twist lock.
4. Hold operator B was unaware of the position of hold operator A when they signalled to the crane operator to lower the container.
5. Although visibility from the crane operator’s cab was limited by objects covering the grating, it is unlikely that the crane operator would have noticed hold operator A moving underneath the container.
Risk management for container loading operations
A2.16. A central tenet of risk management is to ensure there are appropriate controls in place to guard against harm. This includes harm that may occur because of human error or an unsafe behaviour or act. While it is not known for certain why hold operator A moved under the suspended load, a situation where they were able to do so without being observed by the other gang members should not have been able to occur.
A2.17. Working at the same level of the container stack allowed the two hold operators to remain in sight of each other and observe any unsafe behaviours should they occur. However, once hold operator A had refitted the displaced twist lock, they elected to remain on the lower level of containers rather than return to the second tier. This increased risk by creating a situation whereby neither of the two hold operators could see the other.
A2.18. WIL had no specific policy to prohibit working on separate levels of the container stack and this had not been considered as part of the risk-assessment process. As a result, there were no additional control measures identified that may have better protected those working in a heightened-risk environment. This permitted a situation whereby hold operator B could signal the crane driver to lower the container without requiring visual confirmation that hold operator A was in a safe position.
A2.19. Although a ‘lack of understanding of responsibilities’ had been identified by WIL as a potential risk, at the time of the accident there were ambiguous procedures for signalling the crane operator.
A2.20. WIL’s procedures stated that the hatchman was responsible for signalling, but that the hold operators could signal the crane operator if required. Similarly, the crane operator was instructed to obey the signals of the hatchman, but could also take signals from staff. There was no requirement for the hold operators to have one another in sight before signalling, nor was there any requirement for the crane operator to have both hold operators in sight before manoeuvring a load (in circumstances where the crane operator could not see either hold operator to receive signals, such as loading into a vessel’s hold or when the crane operator was operating ‘blind’ (loading/unloading over a container stack), they were required to use a radio for communication). As to the hatchman responsibilities, in one piece of documentation, the hatchman was instructed to keep the crane’s hook in sight ‘at all times’, yet in another, it was only to keep the hook in sight ‘as much as possible’.
A2.21. At the time of the accident, the hatchman had left the vessel to find a rain jacket and then talked with a supervisor at the gangway for around 10 to 15 minutes. While this was not unusual behaviour for a hatchman, who typically moved between the vessel and the wharf at various times, it did not conform with the duties outlined in the operational documentation.
A2.22. The gang three hatchman considered their role was to oversee all aspects of the gang’s work, including making sure people were operating safely, as well as checking the wharf hands were tallying the containers correctly and cross-checking that the containers were going to the correct places onboard. These activities were not documented by WIL as part of the hatchman’s role for container operations.
A2.23. Formal oversight of the vessel-loading operation was the supervisors’ responsibility. The ‘foreman’ title assigned to the hatchman role had no specific tasks associated with it but implied they had a leadership position within the gang. This likely created a situation in which those working in the hatchman role with the additional title of foreman felt a sense of responsibility to oversee other aspects of their gang’s work.
A2.24. WIL had recognised that a lack of understanding between roles within a gang was a potential risk when loading container vessels (WIL-SOP-068 Roles and Responsibilities – Container Vessels), but their procedures were ambiguous and contradictory. One of the hazards that had been identified for container vessel operations was ‘Not understanding the responsibilities, leading to harm’. However, a documented control measure for this hazard was listed as ‘Responsibilities get shared to ensure personnel stay safe’, a concept that is counterintuitive to having clearly defined responsibilities.
A2.25. At the time of this accident, neither the hatchman, the crane operator nor hold operator B had sight of hold operator A before the container was lowered, nor was this an explicit requirement as part of signalling procedures. A lack of procedural clarity led to a diffusion of responsibility within the gang and there was only one risk-control measure preventing a crushing accident, being a reliance on stevedores not putting themselves in an unsafe position.
Findings
6. The hold operators were working on different levels and did not have sight of one another, increasing the risk of a crush injury.
7. The procedures for container loading included unclear, contradictory and ambiguous descriptions of role responsibilities.
Supervisory oversight
A2.26. While many of the inherent risks associated with stevedoring can be difficult to eliminate, the majority of WIL’s risk controls were administrative in nature (see Figure 5 for hierarchy of risk controls). Administrative risk controls refer to interventions such as training, procedures and warnings as a means of mitigating risk. Administrative risk controls and PPE are often applied to existing processes where hazards are not well controlled (United States National Institute for Occupational Safety and Health, 2022).
A2.27. Administrative risk controls can provide a defence against hazards but as they are human-centric by design, their effectiveness relies heavily on workers conforming to expectations, despite the many factors known to influence human behaviour. The use of administrative risk controls, such as documented safety procedures, requires considerable effort by front-line workers and an effective level of supervisory oversight (United States National Institute for Occupational Safety and Health, 2022).
A2.28. WIL required the use of an arrestor system (consisting of a harness and the ability to be tethered to an anchor point) when a worker was positioned less than two metres from an exposed edge. Whilst hold operator A was wearing a harness, they did not tether themselves to anything before moving outside their safe zone.
A2.29. Motivation to follow procedures varies with an employee’s perception of risk. Even in hazardous situations, it is natural to become desensitised to risk over time, particularly when adverse consequences infrequently occur. In such situations, simply reminding people to follow procedures or not to put themselves in harm’s way, such as the discussion that took place at the daily pre-start meetings, is seldom effective and should not be overly relied upon for the assurance of safety.
A2.30. Supervisory oversight provides an additional layer of defence by detecting the presence of at-risk behaviour. The underlying reasons it is occurring can then be examined within the wider safety system. Choosing to use the wire technique instead of using the man-cage on the spreader to change between container levels was a shortcut. While employees often take shortcuts to achieve an outcome, the reasons for doing so vary (see ‘Effectiveness of administrative risk controls’ in Section 2 of this report). At WIL, stevedores were paid for a full shift of work, regardless of how many hours were worked. There is potential for such an arrangement to act as motivation to take shortcuts in order to leave work early. Regardless of whether that was a factor in this accident, the Commission considers it is important to explore sources of system-induced behavioural risk.
A2.31. Supervisors must be supported to be particularly focused on safety, not just on productivity or other business demands (Safe Work Australia, 2006) (emphasis as in original). Two supervisors were assigned to oversee the loading operation on the day of the accident. WIL had purposely designed the supervisor role to be one that was present at the vessel and could actively supervise loading operations. However, given the extent of the supervisor responsibilities, it was not possible for them to observe stevedore behaviours across three gangs. This reflects an insufficient understanding of the importance of supervision when relying on administrative risk controls.
A2.32. At the time the accident occurred, there was only one supervisor onboard the vessel. This was not unusual as the supervisor role included overseeing loading operations to check they were being conducted in accordance with the plan, which often required trips to and from WIL’s office.
A2.33. The presence of at-risk behaviours, such as not using a harness and using the wire technique that WIL no longer condoned, are indicators that supervisory oversight was not an effective risk control. There was a disconnect between the documented procedures and how operations were being conducted on a day-to-day basis (Situations such as this are described as ‘work done versus work imagined’ meaning that documented procedures that are written are often significantly different from how activities are conducted by those on the front line). It demonstrates how WIL’s administrative risk controls appeared robust on paper yet in practice proved to be ineffective.
Findings
8. Hold operator A was not using their fall arrestor system while positioned outside a safe zone (less than 2m from an exposed edge).
9. The presence of at-risk behaviour in the form of non-adherence to procedures indicated a desensitisation to risk and an insufficient understanding of the importance of effective supervisory oversight.
10. Many of WIL’s risk control measures were administrative in nature and required a high degree of compliance oversight to ensure they were effective.
WIL Safety Management System
Safety issue: At the time of the accident, WIL’s SMS was still in development and had not reached the level of maturity required to provide assurance that risk controls were adequate or that all hazards were identified.
A2.34. WIL was in the process of improving their SMS at the time of the accident. The introduction of new safety-reporting systems and the development of a critical-risk framework were examples of this. However, some operational activities fundamental to an SMS were not effective, specifically processes related to safety assurance.
A2.35. Safety assurance can be described as:
a continuous, ongoing activity aimed at ensuring that the initial identification of hazards and assumptions in relation to the assessment of the consequences of safety risks, and the defences that exist in the system as a means of control, remain valid and applicable as the system evolves over time (International Civil Aviation Organization, 2018).
For a safety system to be effective, a continuous cycle of monitoring and reviewing operations must be in place to provide assurance that hazards are being adequately controlled. Where there is a high dependency on administrative risk controls, such as at WIL, this should include verification of employee behaviour to ensure that procedures are reflective of the way work is being conducted. Any inconsistencies can be indicative of problems either with behaviour or with the procedures themselves.
A2.36. The risks associated with discharging and loading containers were detailed in WIL’s Safe Work Method Statement (WIL-SWMS-002 Safe Work Method Statement – Discharge/Load Containers), which had last been reviewed on 14 September 2020. Each of the 12 subtasks were assigned a primary risk score depending on the hazards associated with the task. Control measures were prescribed, which reduced the risk score.
A2.37. Moving containers to and from the wharf had five hazards identified, including crush injuries. The primary risk score for this subtask was Medium. Three control measures had been prescribed to address this risk:
1.Containers only moved on instruction of hatchmen
2.Good hand signals and radio communication between foreman, hatchmen, crane operator and hold operators
3.Careful manoeuvring of spreaders, wires and hooks onto the load by the hold operators.
As a result of these measures, the risk score was reduced to Low. However, the procedures did not reflect how container operations were being conducted and therefore negated the risk control. Had an effective safety-assurance system been in place it is likely that these discrepancies would have been captured.
A2.38. At the time of the accident, WIL’s mechanisms for safety assurance were limited. The primary method for employees to report safety-related issues was to inform a supervisor. Escalation of issues was then reliant on supervisors submitting reports on their behalf. Feedback from stevedores during the investigation revealed that if they saw unsafe behaviour they would often ‘just deal with it at the time’ and not necessarily inform a supervisor unless the event involved an incident or accident.
Together with the fact that supervisors could not observe all the stevedores across multiple gangs, this meant that the true number of unsafe acts or non-conformances that were taking place on the front line were almost certainly much higher than was formally captured by the EHS team (data provided to the Commission for the purposes of this investigation).
A2.39. In the months leading up to the accident, WIL had identified the need to increase safety reporting and had set operational objectives for hazard identification, near-miss reports and employee improvement suggestions. There was also a recognition that more rigour and quality control was required for internal auditing processes and training competencies.
A2.40. At the last Management Review meeting before the accident, WIL had assessed the risk of a serious health and safety incident occurring within the company as High. The management of risks was to be supported through ongoing improvements of their safety processes. It would therefore be expected that an accident occurring would act as a mechanism to trigger safety improvements beyond those arising from a normal continuous improvement cycle.
A2.41. However, the Commission found that WIL’s safety improvements had been limited to reminding stevedores not to position themselves under suspended loads and to stop work if they observed any unsafe behaviour. During a visit to the worksite two months after the accident, the Commission observed the pre-start briefing board, and noted that it was substantively unchanged from the day of the accident (the date, name of vessel and supervisors’ names were updated). This suggests that the passive safety messaging was ineffective in causing change. The Commission was also concerned that some staff within WIL believed that nothing could have prevented such an event from happening.
A2.42. The Commission does not consider that WIL’s safety system was operating at the standard required to provide rigorous safety assurance. The Commission has therefore made a recommendation in Section 5 of this report to address this safety issue.
A2.43. The regulatory framework did little to encourage the ongoing development and continuous improvement of WIL’s SMS. There were no requirements for proactive oversight in the form of regular reviews by WorkSafe or MNZ, nor was there any requirement to proactively demonstrate ongoing safety assurance to the regulators.
A2.44. Interaction between WIL and the regulators was primarily limited to reporting notifiable events and any subsequent interventions that were triggered as a result. The Commission does not consider that this level of regulatory oversight was sufficient to provide assurance of WIL’s future safety performance. The Commission has therefore made a recommendation in Section 5 of this report to address this safety issue.
Finding
11. The regulatory framework and oversight provided little support to the ongoing development of WIL’s safety management system.
B1. Appendix B: MO-2022-202 Fatal accident at Lyttelton Port, 25 April 2022
B1. Factual Information
Pārongo pono
Background
B1.1. On the morning of 23 April 2022, the bulk carrier ETG Aquarius berthed at Lyttelton Port to load a cargo of coal.
B1.2. The loading of coal at Lyttelton Port was carried out by stevedores employed directly by the Lyttelton Port Company Limited (LPC). Table 4 explains the roles of the stevedores involved.
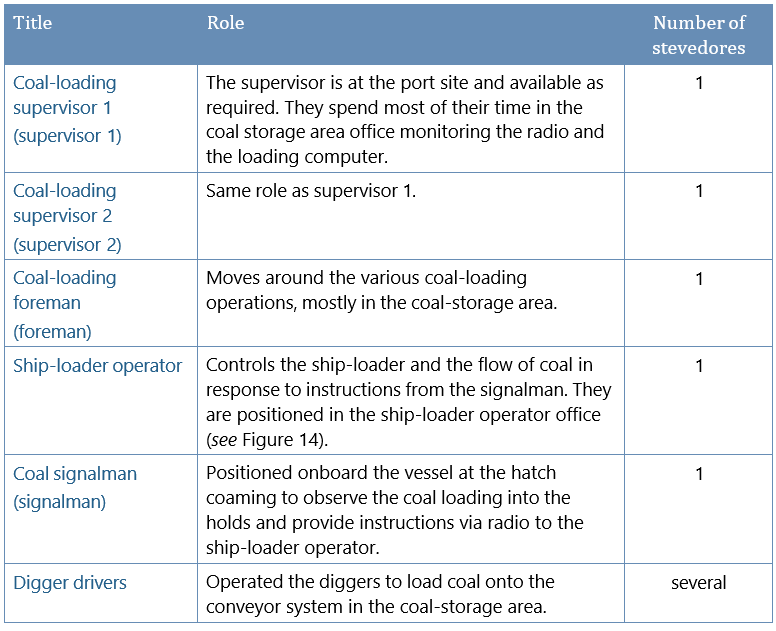
Introduction to loading coal at Lyttelton Port
B1.3. The coal loading operation at Lyttelton Port was unique compared to more generalised stevedoring operations at other ports. However there remain many common features and hazards of stevedoring such as safety management, stevedoring gang structures, communications, leadership, hazardous environment, and risk-mitigation strategies.
B1.4. Lyttelton Port has a coal stockpile facility and coal loading operation. The coal was moved from the stockpile to the vessel via conveyor belts. The final stage of the process, loading coal into the vessel’s hold, used specialist equipment known as a ship-loader.
B1.5. The ship-loader travelled on rails parallel to the edge of the wharf. The wharf conveyor belt fed coal onto the ship-loader lower conveyor belt, which then fed the coal onto the boom conveyor belt, which in turn fed it into the loader chute, from which it passed out through the jetslinger and into the ship’s hold (see Figure 16 and Figure 17).
B1.6. The jetslinger incorporated a short conveyor belt moving at high speed to direct the coal in the direction and elevation required.
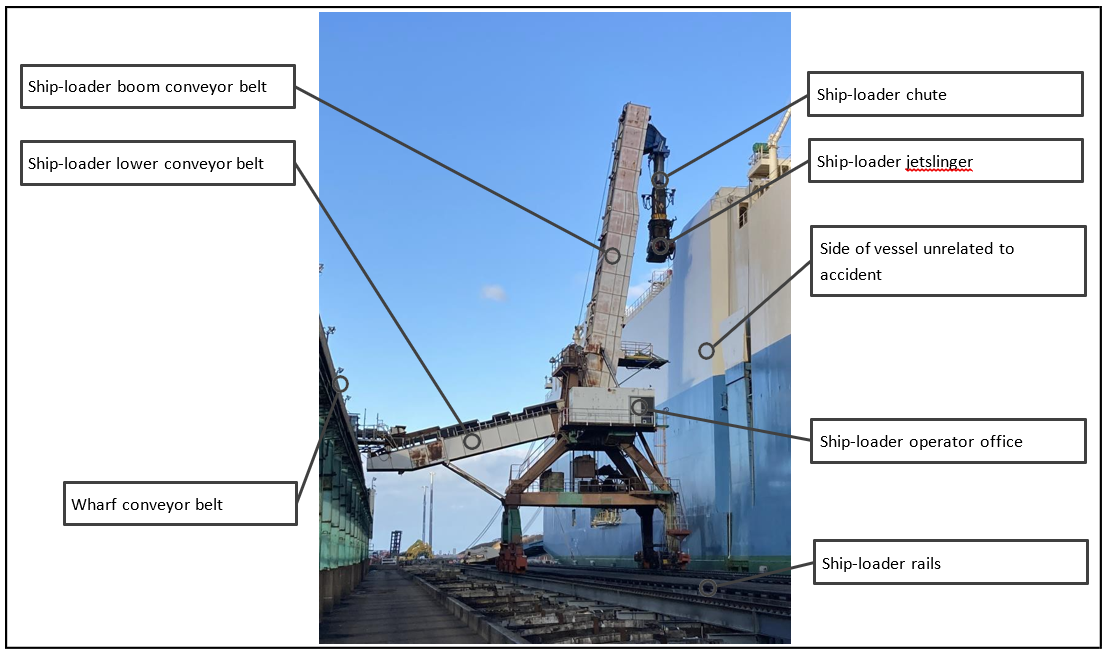
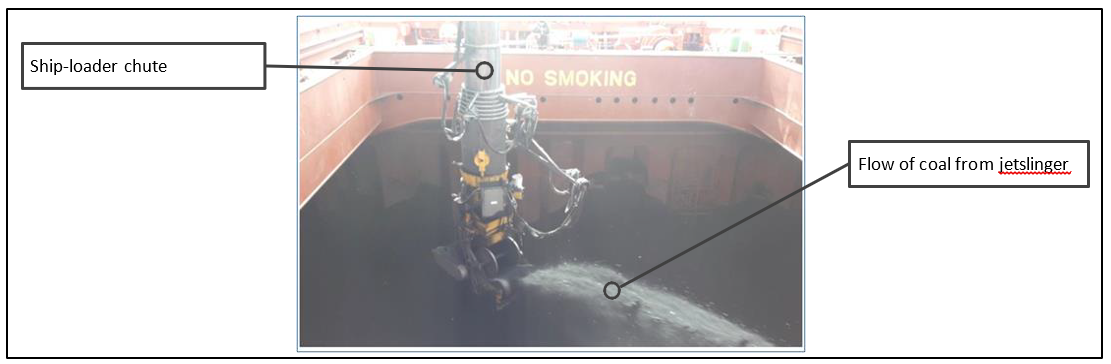
B1.7. During loading operations, the ship-loader operator had limited visibility of the jetslinger, the hold, or the area around the hatch coaming. There was no closed-circuit television (CCTV) system installed on the ship-loader to assist the ship-loader operator in directing the flow of coal from the jetslinger. The ship-loader operator relied upon instructions transmitted over radio from the signalman, who was positioned at the hatch coaming to observe the progress of coal loading. The signalman was responsible for giving instructions to the ship-loader operator by radio to adjust the direction, elevation and flow of coal from the jetslinger to ensure the hold was loaded appropriately.
B1.8. One radio channel was used for coal loading operations. This channel was used by the digger operators, the ship-loader operator and signalman. The supervisors and the foreman monitored both digger operations and ship-loading.
Narrative
B1.9. After the vessel’s arrival on 23 April 2022, supervisor 1, supervisor 2 and the foreman went onboard the vessel to discuss the loading plan with the vessel’s master, and coal loading started at about 0715 that day.
B1.10. On 25 April, between about 0600 and 0630 the ship-loader operator and signalman both arrived at the port in preparation for the start of their shift at 0700.
B1.11. At about 0635, loading of the vessel was nearly completed by the previous shift but was paused while an independent cargo surveyor, supervisor 1, supervisor 2 and the vessel’s chief officer conducted a draft survey.94 They calculated that about 1,000 tonnes of coal still had to be loaded into the number seven and number one holds.
B1.12. The ship-loader operator made their way to the ship-loader operator office within the ship-loader (see Figure 16) and at about 0700, after a limited handover from the ship-loader operator going off-shift, they assumed control of the ship-loader. The signalman had made his way onboard the vessel and began their shift at about 0700.
B1.13. The ship-loader operator moved the ship-loader from its location beside the vessel’s number one hold to locate it beside the number seven hold. Working with the signalman’s radio instructions they began to load the number seven hold, finishing at about 0825. The ship-loader was then moved to the number one hold and began loading.
B1.14. Based on instructions from the signalman, the ship-loader operator directed the flow of coal towards the port aft corner of the hold (see arrow 1 in Figure 18). When the area was full, the signalman instructed the ship-loader operator to ‘come around clockwise’, which meant to slew the jetslinger in a clockwise direction ‘a few degrees’ (see arrow 2 in Figure 18).
B1.15. The coal continued flowing until the signalman again instructed the ship-loader operator to ‘come around clockwise’ (see arrow 3 in Figure 18). The signalman continued to give instructions to the ship-loader operator, and the jetslinger continued to incrementally rotate in a clockwise direction to load the hold. Most movements were within about 15 seconds of the previous movement.
B1.16. Throughout the loading process, coal was flowing from the jetslinger (see Figure 17) continuously. Usually, the flow of coal was only stopped by the ship-loader operator when it was necessary to move the ship-loader between cargo holds.
B1.17. While the coal was being loaded, the foreman, who was not onboard the vessel, used a hand-held radio to check in with the ship-loader operator to determine how much coal was still to be loaded.
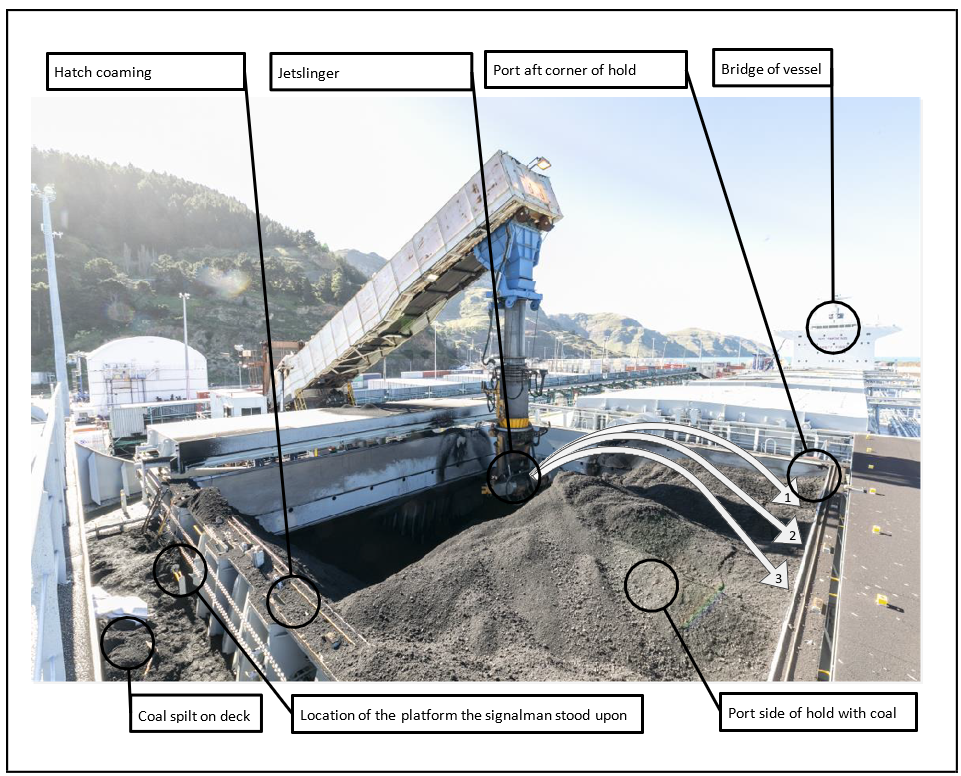
B1.18. At about 0900 the port side of the hold was nearly full and the signalman positioned himself at the hatch coaming by the platform to observe the progress of loading in the hold (see Figure 18). They periodically climbed onto the platform to see into the hold. The jetslinger continued to rotate in a clockwise direction towards the signalman who was standing on the platform.
B1.19. As the coal started to reach the top of the hold, the angle and height of the jetslinger caused some of the stream of coal to spill over the top of the hatch coaming (see Figure 18).
B1.20. At 0903:38 the signalman instructed the ship-loader operator to ‘come around clockwise’. Then at 0903:47 said, ‘that’s good’, before saying at 0903:50 ‘back, two clicks’ (a ‘click’ referred to a click of the slew button on the ship-loader controls).
B1.21. At 0904:01 the ship-loader operator heard some muffled noises on the radio. A few seconds later the jetslinger finished rotating from the ship-loader operator’s most recent command, and some of the coal began to spill over the coaming at the approximate location of the signalman.
B1.22. About this time the signalman almost certainly fell off the platform they were standing upon, and as they fell their helmet came off and they hit their head on the deck.
B1.23. After 23 seconds of radio silence the ship-loader operator asked if the signalman was alright but received no reply. The ship-loader operator asked again a few seconds later, and again received no reply.
B1.24. Supervisor 2 (who was on the wharf) had been listening to the exchange over the radio and asked the ship-loader operator if they could see the signalman. The ship-loader operator replied that he could not. Supervisor 2 then said he would go onboard to look for the signalman.
B1.25. The ship-loader operator noticed that coal was spilling over the coaming and at about 0906 asked the foreman if he should hit the stop sequence (the stop sequence was the process to stop the conveyors. It ran the conveyors until they were empty before stopping movement – this took about 1:30 minutes), which the foreman approved. At about 0907, the foreman noted the coal had stopped.
B1.26. Supervisor 2 arrived onboard the vessel at the number one hatch just after 0907 but was unable to locate the signalman. At about 0910, they radioed for assistance (the request was made via radio and hence was heard by the rest of the coal-loading team) to search the spilt coal. By 0916, three stevedores and some of the vessel’s crew began searching the coal looking for the signalman.
B1.27. At about 0918 the foreman radioed to ask port security to call emergency services, but in response was told emergency services would require information and the foreman should call them. At 0928 someone confirmed over radio that emergency services had been called. The signalman was found at about 0930, unresponsive, near the base of the platform they had been standing upon. Emergency services arrived on the scene and the signalman was pronounced deceased at about 0950.
B1.28. The signalman was found near the base of the platform they had been standing upon. They had suffered a serious head injury, a medical event and possible asphyxiation, although there is uncertainty about the sequence of events.
Personnel information
B1.29. The signalman began working as a stevedore for LPC in 2013 and completed training as a coal signalman in January 2018.
B1.30. The ship-loader operator began working as a stevedore for LPC in 2012 and completed training as a ship-loader operator in October 2017, completing a refresher course in October 2020. They had also trained as a signalman in February 2015.
B1.31. Supervisor 1 had worked as a stevedore at Lyttelton Port since 1984 and was experienced in all stevedoring roles at the port. He was scheduled to retire in June 2022.
B1.32. Supervisor 2 began working at LPC in 2000 and completed training as a terminal signalman (terminal signalman refers to the role of signalman in the container terminal) in 2002 and as a ship-loader operator in 2004. They were acting as second in command to supervisor 1 while they finished their training and until the retirement of supervisor 1.
B1.33. The foreman began working at LPC in 2008 and was trained as a ship-loader operator in 2014. They were trained as a coal signalman in 2012, terminal signalman in 2015, and in 2019 completed a ship-loader operator refresher course. There is no record of formal training specific to the role of foreman.
B1.34. The training system at LPC was developed internally and did not result in NZQA qualifications.
Vessel information
B1.35. The ETG Aquarius was registered in Liberia and began operating in April 2022. It was a bulk carrier with a cargo capacity of 82,000 tonnes and was on its maiden voyage when it berthed to load coal at Lyttelton Port.
Recorded data
B1.36. Recorded data was used to help determine the timeline and actions of the accident:
- a CCTV was located on the bridge of the vessel. Its field of view included some of the number one hatch during the time leading up to the accident
- the port radio log captured the radio traffic of the stevedore team
- the ship-loader log captured some of the actions of the ship-loader.
Medical and pathological information
B1.37. There were two sources of medical information used in this investigation. The first was the historical employment records of the signalman, and the second was the medical records that related to the accident.
B1.38. Employment medical records included a pre-employment health assessment report, and ongoing health monitoring records.
B1.39. The pre-employment health assessment was conducted by an occupational health nursing service. The assessment included a questionnaire completed by the candidate and resulting discussion with the assessor, with some clinical assessments (see Figure 19 for the checklist).
B1.40. The ongoing health monitoring programme assessment was similar in scope to the pre-employment assessment.
B1.41. The signalman had an undiagnosed pre-existing medical condition. The condition was not identified during the pre-employment health assessment, nor was it identified by the ongoing health assessment.
Organisational information
Lyttelton Port
B1.42. Lyttelton Port was officially established in 1849. Port operations continued until the Port Companies Act of 1988, which led to the creation of Lyttelton Port Company Limited (LPC). LPC took over the port’s commercial role, including management of the land, assets and facilities. LPC manages the port itself and two inland cargo processing facilities. LPC is owned by Christchurch City Holdings Limited, which is owned by Christchurch City Council.
B1.43. LPC had an organisational structure that included a board of six directors led by a chairperson, and about 670 staff led by the chief executive officer.
B1.44. LPC employed a pool of stevedores, who spent most of their time working in the container terminal at the port. Stevedores who had been trained for coal operations were assigned to load coal as the need arose, which was approximately once per month.
LPC safety management system
B1.45. LPC’s safety management system (SMS) was evolving. Before 2017, the foundations of a health and safety management system were in place and were subject to an audit programme aligned to the ISO 18001 international standard for health and safety management systems.
B1.46. From 2017 to 2019, LPC introduced new safety management systems, including:
- documented descriptions of how to do a task safely, known as safe work method statements (SWMS)
- development of a document management and storage system using SharePoint
- some LPC standards (for example, risk management)
- identification of some critical risks
- a revised risk matrix
- a framework to meet their HSWA obligations.
B1.47. In 2020, LPC gained secondary-level Accident Compensation Corporation (ACC) Accredited Employers Programme (AEP) accreditation and began work to introduce an integrated SMS. The AEP enables employers to assume management of workplace injuries instead of ACC. Accreditation under AEP includes assessment of the health and safety system and annual audits once accredited.
B1.48. In 2021, LPC’s Critical Control Assurance Programme was in place, and had identified more critical risks. The 2021 AEP audit resulted in LPC gaining tertiary-level accreditation. The audit report noted that although LPC’s health and safety system was in a state of flux ‘Improvements are many. …The health and safety team has more than doubled in size this last year. There is a sense of getting to the starting line with work projects aimed at improving safety’.
B1.49. Also in 2021, recognising a need to improve health and safety led LPC senior leadership to commission an independent review of the SMS, (the Review). The Review report was delivered in July 2021 and described some findings and recommendations pertinent to the Commission’s investigation, which are summarised below:
- while all fundamental risk-management tools were in place, including a good understanding of ‘critical risks’, the understanding of when they should be used, and identification of ‘critical’ was lacking
- procedures and SWMSs related to several areas, including signalman operations, were not specific enough to minimise risk
- lack of compliance with risk controls was not monitored through visible leadership
- there was no radio-communication protocol (LPC’s marine operations operate using radio protocol as laid out by MNZ and according to international standards).
B1.50. The Review made recommendations, some of which are summarised below:
- produce visible leadership targets and tools for in-field critical control checks
- roll out education and training to all levels for hazard reporting, personal risk assessment, job safety analysis and formal risk assessment
- improve risk reporting
- review procedures for high-risk work with a focus on reducing risk
- define a radio protocol and monitor compliance
- develop trigger action responses for high-risk procedures to assist response to alarms and alerts.
B1.51. At the time of the accident, LPC had started a programme to address the AEP audit and the Review recommendations.
B1.52. Neither regulator (WorkSafe or MNZ) had undertaken monitoring or a detailed assessment of LPC’s stevedoring SMS.
Procedures and training
B1.53. The training system at LPC was based on role-specific modules, and the training was delivered in-house by LPC staff. The training material included module-specific training manuals, SWMSs and module-specific assessment forms.
B1.54. The training manuals provided wider context and guidelines around the role (for example, the training manual for the signalman included a description of loading terminology with respect to bulk carrier loading) and the SWMSs provided specific procedures and risk controls for the role.
B1.55. The training was developed and delivered by the LPC training coordinator, and was based on procedures, documentation (for example SWMSs) and some NZQA unit standards.
B1.56. LPC staff commented during interviews with the Commission that the training material and programme lacked adequate input from the people with experience in the roles.
B1.57. The AEP audit report 2021 found ‘limited evidence that the staff are involved in the review of relevant policies and procedures, measures of performance or the setting of objectives’.
Risk identification and mitigation
B1.58. As noted above, fundamental risk-management tools were in place, including a risk matrix and risk-control assurance.
B1.59. A ‘major hazard’ that had been identified for the signalman was the flow of coal from the jetslinger. The risk controls set out in the SWMS were administrative and some excerpts are quoted here:
- The signalman should always know movements of the jetslinger
- Keep jetslinger in sight at all times as it could potentially swing causing a change in the trajectory
- The signalman needs to give his full attention to the ship-loader and jetslinger for potential risks.
B1.60. The training manual highlighted the risk of ‘standing in front of the coal jetslinger flow’.
B1.61. The 2021 AEP audit report found ‘The controls applied in the risk registers are often lower-level administrative controls…’.
Another major hazard identified was working at heights while the signalman stood upon the pedestal to see into the hold. The photo accompanying that section of the SWMS shows the signalman standing on the pedestal onboard a different vessel (see Figure 20).

B1.62. None of the documentation identified that the signalman was working in physical isolation, nor that it was a hazard.
B1.63. LPC staff acknowledged that final loading of hatches increased risk, which they informed the Commission was controlled by reducing the feed rate and stopping as necessary. This process was not documented in the procedures, and it is unclear if it was implemented in practice. A potential need for ‘mentoring’ when hatches were loaded over 90% was noted in safety meeting minutes, however it is uncertain what was meant by that, nor to what extent it occurred.
B1.64. The Review found that:
While all Fundamental Risk Management Tools are in place, the understanding of when they should be used, and what is “critical”, are lacking. …Similarly, a review of jobs identified that many elements of the Safe System of Work are not in place.’
The Review also said:
…Procedures and SWMS related to a number of high-exposure Operational activities are not specific enough to minimise risk, including dozer operations, isolation of energy sources, lashing and signalman operations.
Risk controls monitoring
B1.65. A key performance indicator for the supervisor role was that ‘safe work practices and procedures are always followed.’ There was no mechanism to monitor or report on non-compliance with procedures and risk controls.
B1.66. The effectiveness of the risk controls was assessed against the reported incidents and accidents. Hazards and near-miss reporting had identified cases of non-compliance, but they mostly related to vehicle-traffic non-compliance with traffic signals and road markings within the port. The Commission was unable to find any records of non-compliance and actions taken related to coal operations.
B1.67. Monthly Coal Health and Safety meeting minutes did not discuss non-compliance or leadership around enforcing risk controls or adhering to procedures. The need to submit incident forms was, however, a regular agenda item. Compliance with procedures and risk controls was not a reporting item of senior leadership.
B1.68. The 2021 AEP audit report gives an ‘inexhaustive’ list of safety issues such as ‘PPE not in useable condition’, and says ‘This suggests the effectiveness of the [safety checking] programme is ineffective ... The checking of controls should be reviewed and an effective system that gives confidence implemented.’
B1.69. The Review makes recommendations around visible leadership and the need to monitor compliance with risk controls at a supervisory level through to senior leadership.
Radio communications
B1.70. The primary means of communication between team members was a two-way radio (a two-way radio can transmit and receive radio communications).
B1.71. Use of two-way radio as a resource was mentioned in the SWMS of both the signalman and the ship-loader operator. Some radio-communication guidelines were provided in the ship-loader operator’s training manual, which included the coal emergency radio communications protocol, radio channels, operating hints and a phonetic alphabet. It required that ‘All personnel shall keep radios switched on at all times.’
B1.72. In the two years before the accident, there were seven reported incidents related to poor radio communications across different port operations but not the coal operation. On 27 June 2023, LPC advised the Commission that a separate review of LPC Harbour Control (Harbour Control relates to LPC’s marine operations, not stevedoring) radio communications was undertaken during
November 2021 and subsequent work was completed to improve training and procedures. However, at the time of the accident this had not been extended to include the coal operation.
B1.73. The Review found there was no specific radio operations protocol, and that LPC should define them, communicate them, and monitor compliance.
Emergency response
B1.74. The ship-loader operator training manual described a coal emergency response procedure (see Figure 21), which included a description of the coal-loading team roles in an emergency, emergency communication radio channels, and protocols and location of emergency stops for the ship-loader itself.
B1.75. Although it does not provide explicit guidance on when to use the emergency stops, it does note ‘If at any stage, there are concerns or doubts of the safety of personnel or state of equipment or the vessel, cease loading and contact the Coal Foreman’. The emergency stop was not activated because the ship-loader operator initially didn’t realise there had been an accident; they thought the issue was a communication problem and so they used the normal stop sequence for the ship-loader.
B1.76. The 2021 AEP audit report found ‘Insufficient evidence is available to show that other relevant emergency scenarios are practised and that relevant persons know what to do in such an emergency’.