TAIC final report shows why equipment should be operated by people who understand how to use it safely, and why safety management systems should require ongoing monitoring and review of risk control effectiveness. A container ship crew member's leg was seriously injured when caught in a moving part of a telescopic ladder.
Executive summary Tuhinga whakarāpopoto


What happened
- On the morning of 10 December 2021, the container vessel Moana Chief was preparing to leave the Port of Auckland. The crew had started retrieving the telescopic accommodation ladder when a crew member’s lower leg got trapped between the fixed upper ladder and the moving lower ladder, resulting in serious injury to their leg.
Why it happened
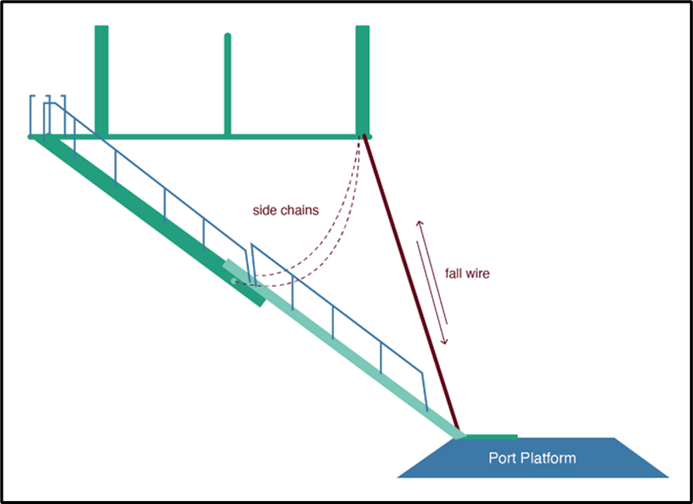
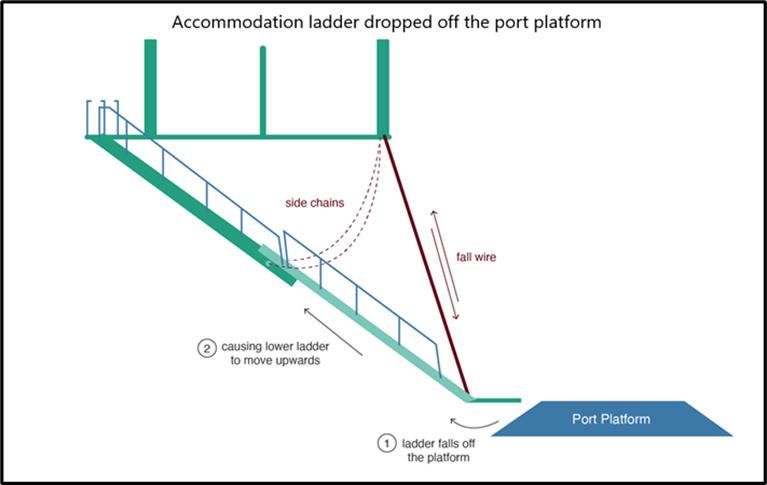
- As crew members were retrieving the accommodation ladder, it slipped off the Port platform on which it was resting. The slack side chains allowed the ladder to drop and the weight of the ladder was transferred to the fall wire, which caused the lower ladder to slide upwards. A crew member, who was standing in an area that had previously been identified and designated as a danger area, was seriously injured.
- Actions to retrieve the accommodation ladder were not consistent with the procedures documented in the vessel's Safety Management System. Several control measures listed in the risk assessment for deploying and retrieving the accommodation ladder were not implemented.
- It is very likely that the accident could have been prevented, if other crew members standing in the vicinity had intervened and alerted the winch operator to a crew member standing in the designated danger area.
What we can learn
- Deploying and retrieving accommodation ladders can be a dangerous operation, and often involves ships’ crews working over the side of the vessel. A telescopic accommodation ladder has several moving parts that further increase risk of injury. It is important that users understand how to operate the equipment safely in accordance with the manufacturer’s instructions.
- Risk assessment and management of a hazard does not end with the implementation of risk controls. Monitoring and reviewing the effectiveness of the risk controls is an ongoing process and should be formalised into the Safety Management System.
Who may benefit
- Operators of telescopic accommodation ladders, vessel owners and operators, maritime training facilities and shore-based emergency response agencies may all benefit from the findings in this report.
- Any organisation using a safety management system to assess risks and manage hazards, including monitoring the effectiveness of their processes which is essential for safe outcomes, may also benefit.
Factual information Pārongo pono
Telescopic accommodation ladder
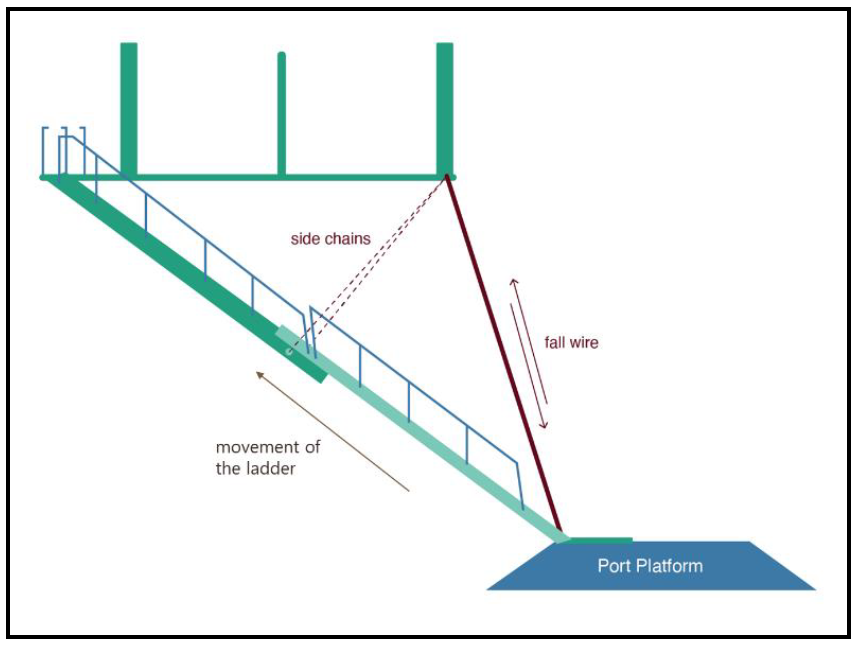
- Typically, a telescopic accommodation ladder (the ladder) is made up of two parts: a fixed upper ladder and a moving lower ladder.
- Onboard Moana Chief (the vessel) the top of the upper ladder was hinged on a turntable mounted onto a platform attached to the ship’s deck. The bottom of the upper ladder was supported by two side chains (see Figure 3).
- The lower ladder was telescopic and could be extended or retracted. It was secured to the upper ladder by an interlocking guide and rollers. There was an overlap between the two ladders of about 1.5 metres, which provided support and helped maintain rigidity and strength. turntable mounted onto a platform attached to the ship’s deck. The bottom of the upper ladder was supported by two side chains (see Figure 3).
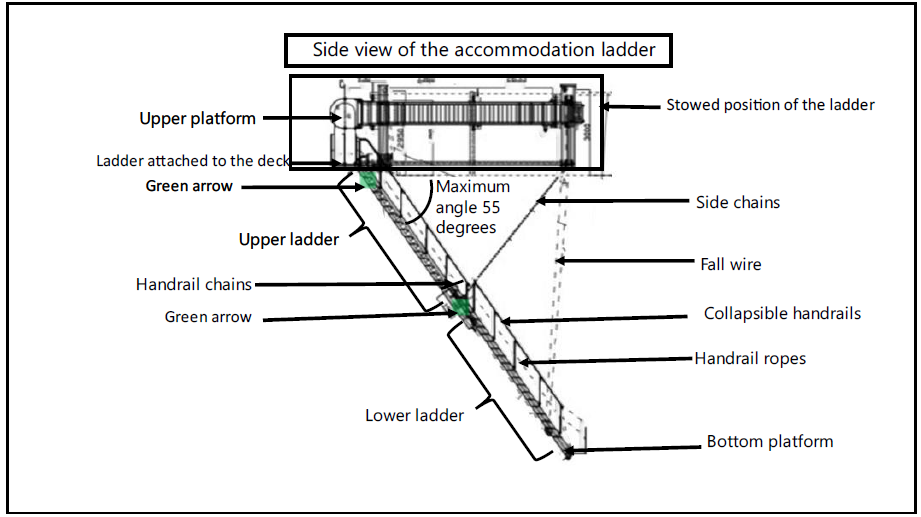
- The ladder was deployed and retrieved by a fall wire connected to a winch. The winch was operated by a remote-control unit on a wandering lead (see Figure 4).

Narrative
- On 10 December 2021 at approximately 0515 the container vessel Moana Chief completed cargo operations alongside Fergusson Wharf (a structure built alongside or perpendicular to the shore where ships berth for loading or discharging cargo) at the Port of Auckland.
- The vessel was due to depart at 0730. At approximately 0700 the duty Integrated Rating (IR) woke the majority of the crew in preparation for unmooring operations.
Events at the accommodation ladder
- The accommodation ladder team (the team) consisted of the Chief Integrated Rating (CIR), the Engine Room Watch Rating (EWR) and the Integrated Rating (IR). The team was responsible for retrieving and stowing the ladder in preparation for sailing.
- Two additional IRs helped to remove and stow the accommodation ladder safety net.
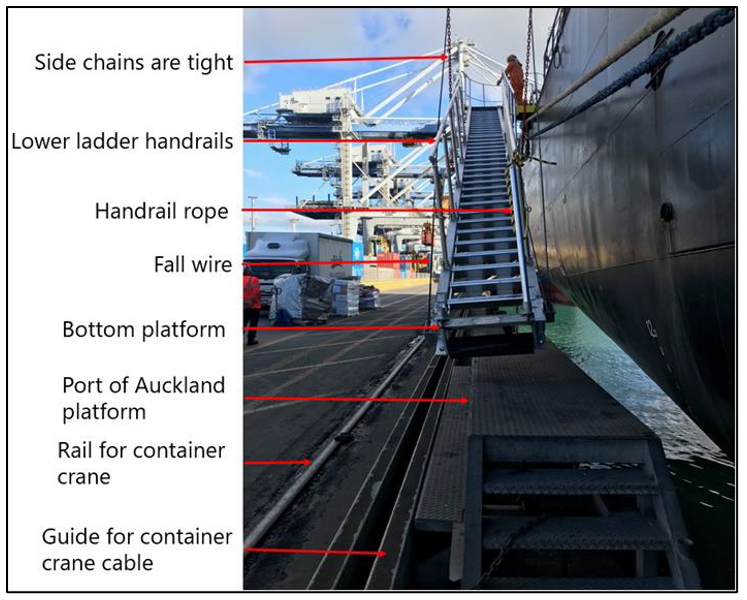
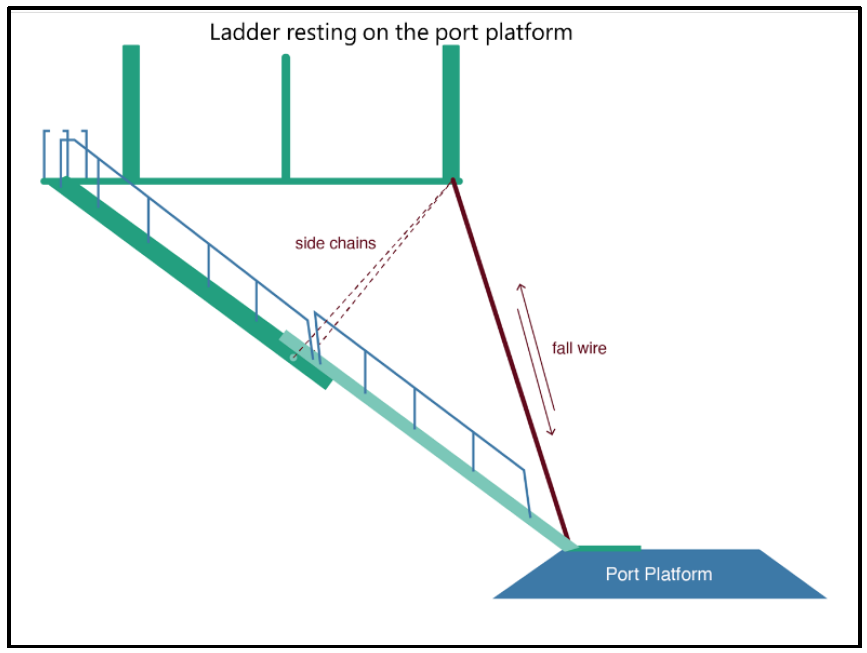
- The ladder was resting on top of a steel platform known as the Ports of Auckland Limited platform (the Port platform) (see Figure 5). The Port platform was designed to keep the ladder clear from obstructions on the wharf and prevent it from impeding the safe operation of the container cranes, which ran on dedicated rails close to the side of the vessel.
- The CIR was the winch operator and person in charge of rigging and stowing the ladder.
- The Chief Officer and the Third Officer were also standing in the vicinity of the ladder observing the operation.
- The team and the two additional IRs removed and stowed the accommodation ladder safety net before the Pilot boarded the vessel at about 0722.
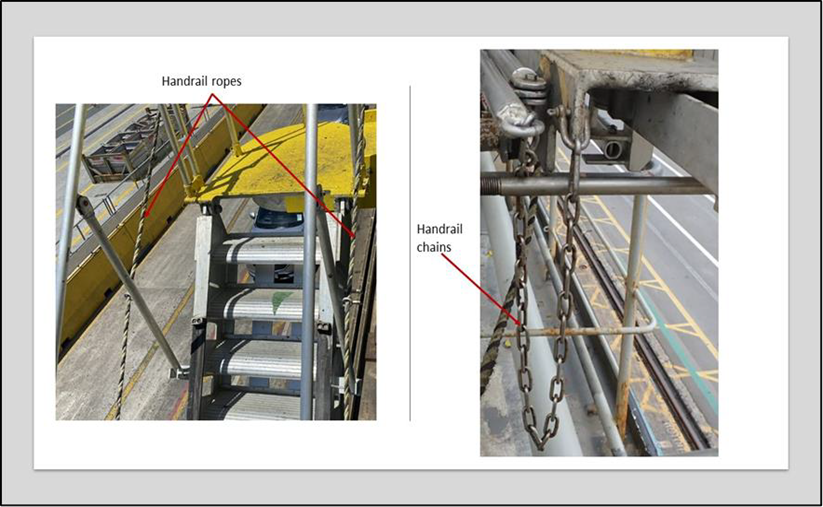
- After the Pilot had boarded the vessel, the team started retrieving the ladder. At approximately 0723, the CIR started the winch and started heaving on the fall wire, which in turn moved the lower ladder up by about one metre. The CIR stopped the winch and directed the EWR and the IR to untie the lower ladder handrail ropes (see Figure 6).
- The EWR walked down to the bottom platform and the IR walked down to the top of the lower ladder. They untied the handrail ropes but left the handrail chains in place, which was the normal procedure (see Figure 6).
- At approximately 0724 the CIR resumed retrieving the ladder, with the IR and the EWR standing on the moving lower ladder. Approximately 30 seconds later the CIR stopped the winch. The EWR and the IR lowered the handrails of the lower ladder.
- The IR then returned to the upper platform. The EWR stepped onto the upper ladder and walked up a few steps, turned around and placed the two handrail chains, clear of any obstructions, on the top step of the lower ladder.
- At approximately 0725 the Chief Officer (who was standing on the poop deck) and the two additional IRs (who had finished removing and stowing the ladder safety net) left to prepare for sailing.
- The CIR continued retrieving the ladder until the inboard (towards the centre of a ship) handrail chain got stuck between the sliding lower ladder and the fixed upper ladder. The CIR stopped the winch and the EWR freed the chain.
- The EWR cleared the inboard handrail chain, picked up the outboard (away from the centre of a ship) handrail chain, and held onto both chains to prevent them from getting caught again.
- The CIR resumed retrieving the ladder, while the EWR remained on the upper ladder and held onto the handrail chains.
- At approximately 0726, the lower ladder fell off the Port platform on which it was resting. As the ladder fell it tightened the fall wire and caused an uncontrolled upward movement of the lower ladder.
- The sudden upward movement of the lower ladder trapped the EWR's left leg between the top step of the lower ladder and the third step of the fixed upper ladder.
- All work stopped immediately and the Third Officer, who was standing on the poop deck nearby, informed the Master on the bridge14 that there had been an accident.
Events after the accident
- The Master saw that the EWR was sitting on the ladder with their left leg trapped between the steps and immediately advised the Pilot that there had been an accident and asked them to inform Harbour Control.
- The crew wedged timber between the steps to ease the weight on the EWR’s le and prevent further injury. The crew assured the EWR that they were doing everything possible to free them from the ladder. At approximately 0736 an ambulance was requested.
- The essel’s crew considered various options before deciding that the safest option to free the ERW’s leg was to cut the step. At approximately 0752 the ladder step was cut away (see Figure 7) and the EWR’s leg was freed. At about the same time the first responders boarded the vessel.

- An ambulance arrived at approximately 0805. A paramedic boarded the vessel to assess the condition of the injured EWR and administered medication. At approximately 0843 the ambulance left the wharf and took the EWR to hospital.
Personnel information
- The Master had held command (to have control of a ship and to be in charge) since 1989 and had over 43 years’ seagoing experience, including 19 years working on container vessels. The Master had worked for Swire Shipping (NZ) Limited (the operator) since 2013 and had command of Moana Chief since October 2019.
- The Chief Officer had a Master’s Certificate of Competency and had joined the vessel the previous day to start a four-week roster. The Chief Officer had worked for the operator since 2011 and had worked on the vessel since February 2020.
- The EWR had started their seagoing career in August 2010. They held an Able Seafarers Deck and Engine Room Watch Rating certificate issued by Maritime New Zealand in 2013. The EWR started working onboard Moana Chief on 25 March 2020, mostly relieving engine room crew members, but occasionally working on deck.
- The CIR had over fifty years’ maritime experience, working on a variety of vessels including bulk carriers and liquefied natural gas vessels. The CIR had previous experience working with the telescopic accommodation ladder on the Moana Chief.
- The IR had over twenty years’ experience working on offshore vessels. The IR had joined the vessel on 5 December 2021 for their second four-week term onboard.
Vessel information
- The Moana Chief was a container vessel. It was owned by John Swire & Sons Limited, a private company registered in the United Kingdom, and operated by Swire Shipping (NZ) Limited. The vessel was registered in New Zealand in September 2019, and its home port was Auckland, New Zealand.
- The vessel had operated on a fixed port rotation between Tauranga, Auckland, Lyttelton, Nelson and Marsden Point since September 2019.
- At the time of the accident, the vessel had a crew of sixteen that comprised the Master, three deck officers, the Chief Engineer, three engine officers, one CIR, four IRs, one EWR, a cook and a steward.
Poop deck telescopic accommodation ladder
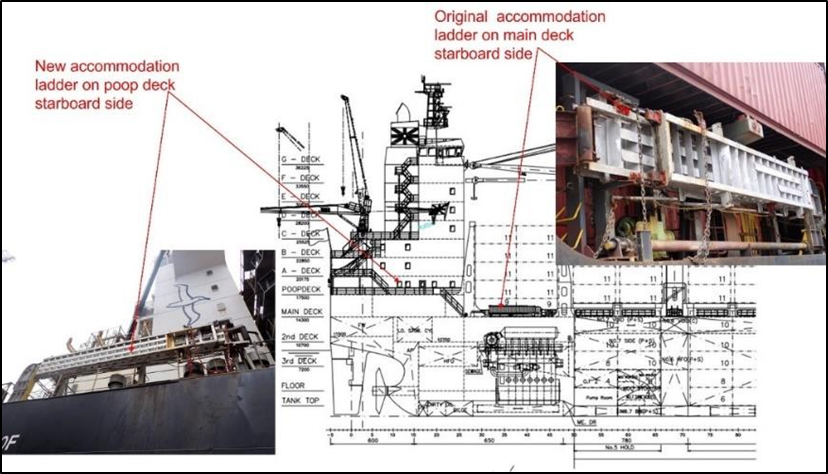
- The vessel was originally built with two telescopic accommodation ladders fitted on the main deck, one on each side. However, the vessel’s draught and the height of tide often resulted in the ladders becoming unsuitable for use at the ports of Auckland and Lyttelton.
- To overcome this challenge, the vessel operator fitted a new telescopic accommodation ladder to the vessel in August 2019. It was fitted on the starboard side of the poop deck, which was one deck higher than the main deck and allowed for contingencies should the main deck ladders become unsuitable (see Figure 8).
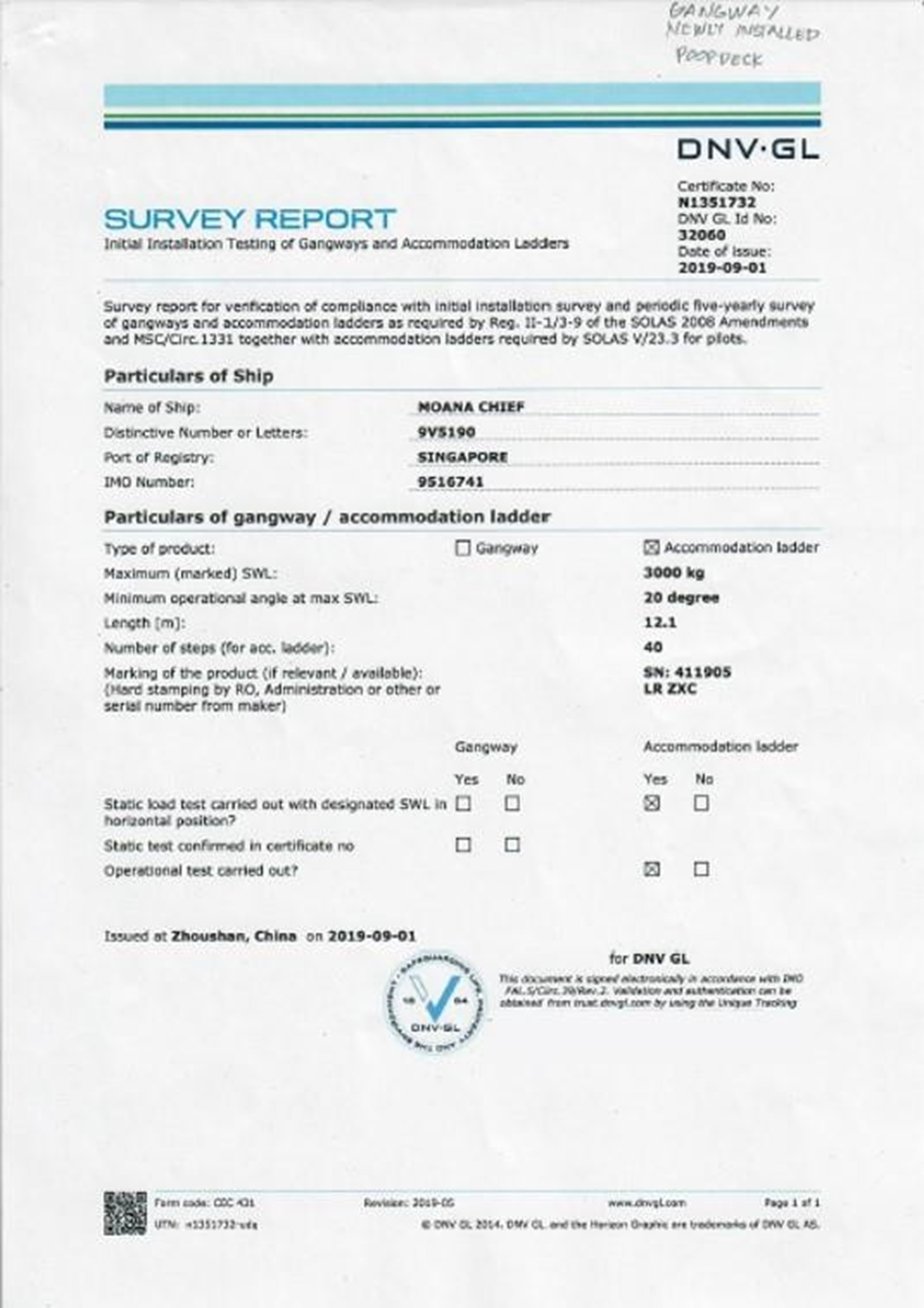
- The ladder met the requirements of the International Convention for the Safety Of Life At Sea (SOLAS) regulation II-I/3-9 Means of Embarkation and Disembarkation from Ships. The ladder was constructed and installed as per the guidance contained in Maritime Safety Committee circular (a statutory document issued by IMO’s Maritime Safety Committee) 1331 (11 June 2009).
- The installation was certified by classification society Det Norske Veritas and Germanischer Lloyd (DNV GL). See Appendix 1 for the DNV GL Survey Report.
Regulation
- SOLAS chapter II-1 (Construction), Part A-1 (Structure of Vessels), regulation 3-9 covers the Means of Embarkation22 on and Disembarkation23 from Ships, and states that they shall be inspected and maintained in suitable condition for their intended purpose. It also states that wires used to support the means of embarkation and disembarkation shall be maintained as specified in regulation III/20.4
- SOLAS chapter III (Life Saving Appliances and Arrangements), Part B-III (Additional requirements for cargo ships), regulation 20-4 states that fall wires shall be inspected periodically, with special regard to areas passing through sheaves, and renewed when necessary due to deterioration or at intervals of not more than five years.
- IMO Maritime Safety Committee circular 1331 provides guidelines on maintenance and examination of accommodation ladders. The circular states that during annual surveys required by SOLAS, the suspension points, davit structures, wire and sheaves of the accommodation ladder should be thoroughly examined. The circular also states that the winch, brake mechanism and remote-control systems should be examined.
Previous issues with the accommodation ladder
Fall wire
- Since its installation in September 2019, there had been ongoing challenges with the fall wire including:
- the wire coming off the winch drum and getting jammed between the drum and the winch
- the wire becoming jammed between the sheave and the cheek plates25 at the bottom platform, causing damage to the wire.
- The fall wire of the ladder had been replaced three times since its installation. The issues with the fall wire were resolved in April 2020.
The winch
- In April 2021, the accommodation ladder winch motor failed when the brake clutch sheared off. The winch continued to lower the ladder by gravity alone. The clutch failed again in May 2021.
The side chains
- The side chains were used to support the upper ladder. They were adjusted manually to alter the ladder’s an le of inclination. ome crew had reported that the side chains were too long and were cumbersome to adjust. It was unclear if this issue was resolved at the time of the accident.
Poop deck telescopic accommodation ladder operations
Deployment
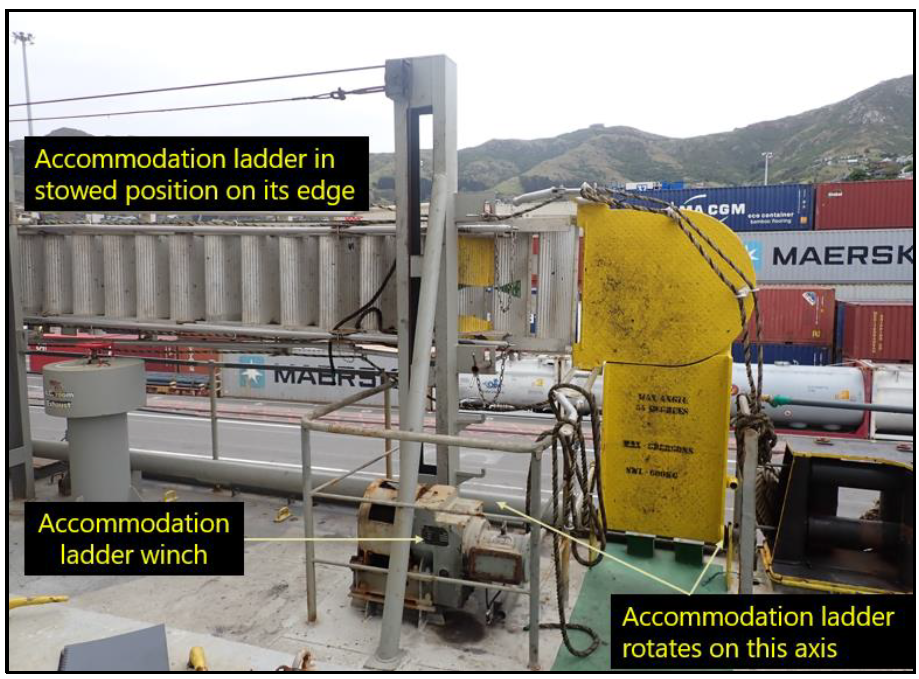
- In the stowed position the ladder rested on its edge along the ship’s side (see Figure 9). The ladder was designed to deploy using gravity. By slackening the fall wire the ladder rotated from its stowed position to a horizontal position outboard of the ship’s siderail.
- The ladder handrails were raised and secured manually. The side chains were then manually adjusted by a crew member to the desired length to facilitate the required angle of inclination.
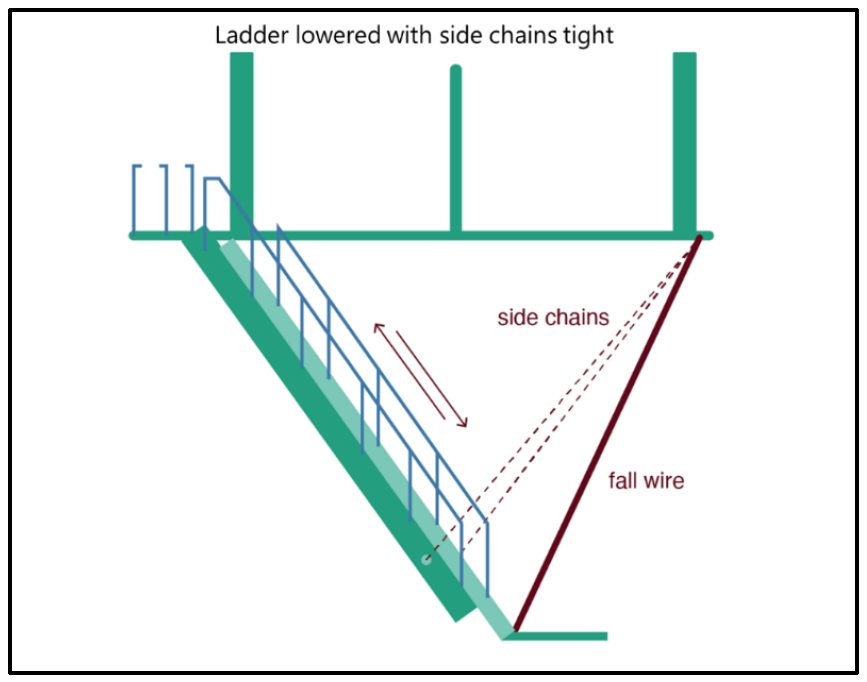
- Further slackening of the fall wires lowered the upper ladder until the side chains were tight and were supporting the weight of the upper ladder (see Figure 10).
- When the weight of the upper ladder was supported by the side chains, further slackening of the wire allowed the lower ladder to slide out (see Figure 11). The operation was complete when the lower ladder reached the desired target area (the Port platform) on the wharf.
Retrieval
-
The retrieval of the ladder was controlled by a winch used to heave in the fall wire. This resulted in the lower ladder sliding up an interlocking guide in the upper ladder until it reached the end point (see Figure 12).
Further heaving of the fall wire took the full weight of both the ladders and lifted them together until the side chains became slack.
When the ladder reached the horizontal the crew, wearing safety harnesses, stepped onto the ladder and lowered the handrails. Further heaving lifted the ladder inwards and into its stowed position at the side of the vessel.
In port, the ladder had to be closely monitored and adjusted to allow for changes in the vessel’s draught and the height of tide. Minor adjustments were made by using the fall wire only. If a large adjustment was required, the ladder was retracted and the side chains manually adjusted before redeploying the ladder back down to the wharf. During a four-hour watch period it was normal for the crew to make between three and ten minor adjustments and one or two major adjustments.
Safety management
- Under SOLAS, the International Safety Management (ISM) Code is mandatory for vessels such as the Moana Chief. The aim of the Code is to improve safety at sea and protect the marine environment.
Moana Chief Safety Management System
- The following section describes the relevant parts of the operator’s safety management system (SMS) that were applicable to this accident.
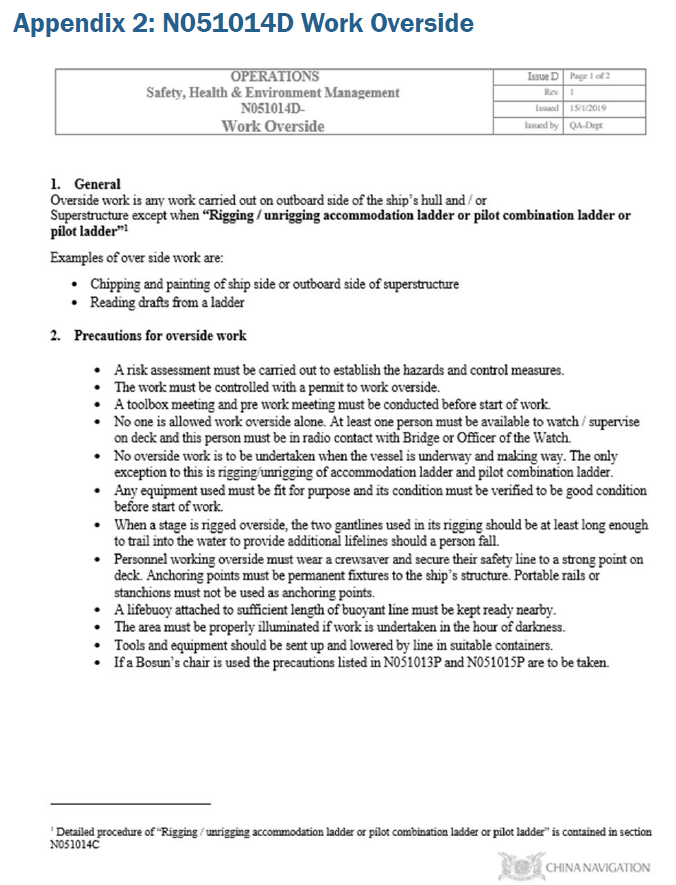
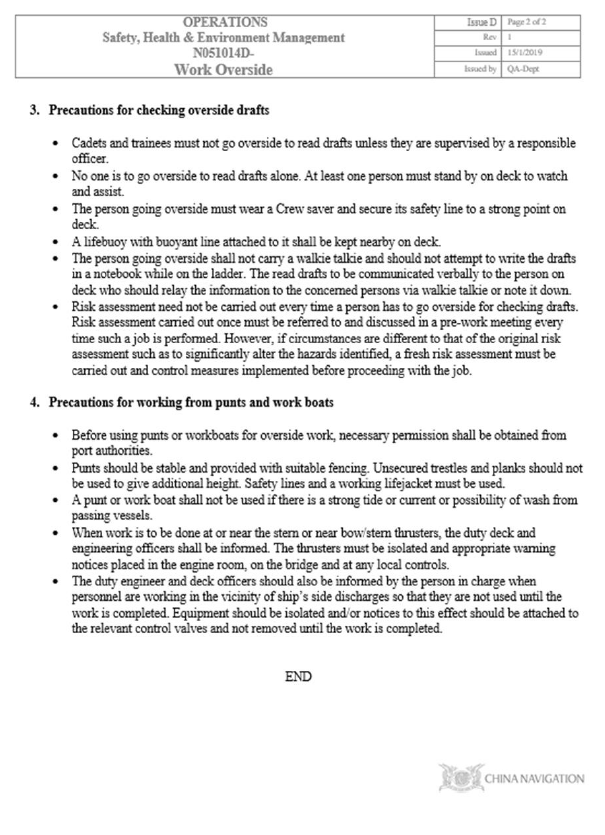
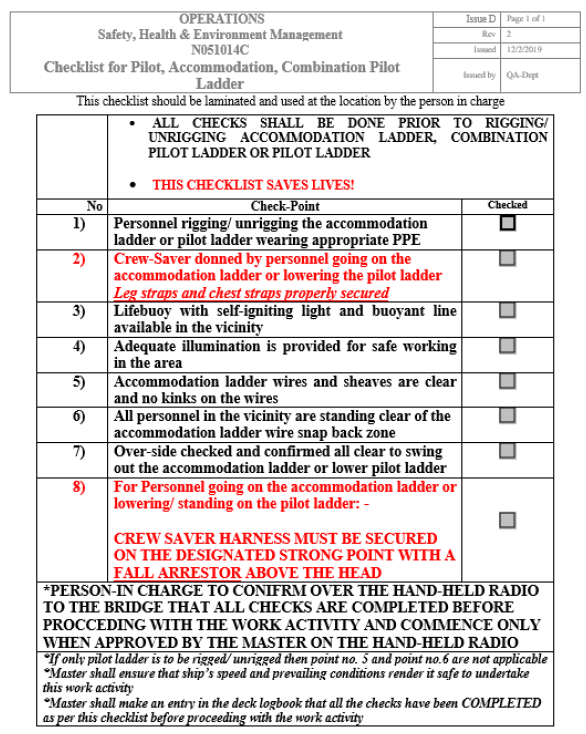
- Retrieving and deploying the ladder required the crew to work outside the ship’s rails, over the side of the vessel. The SMS document N051014D ‘Work Overside’ explained the need for a risk assessment, a toolbox meeting and pre-work meeting to be carried out (see Appendix 2) before starting work. When rigging and unrigging the accommodation ladder the crew was to use document N051014C ‘Checklist for Pilot, Accommodation, Combination Pilot Ladder’ instead (see Appendix 3).
- N051014C required crew working on the accommodation ladder to wear a crew-saver harness secured to a designated strong point. The checklist did not prompt the crew to conduct a toolbox meeting or a pre-work meeting before starting the work.
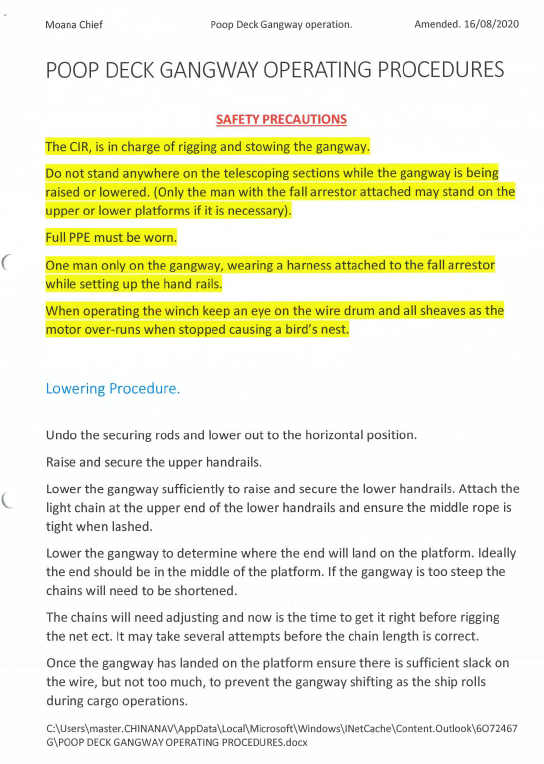
Poop deck gangway operating procedures
- The vessel-specific ‘Poop deck gangway operating procedures’ were amended in August 2020 following a similar accident (refer to paragraphs 2.71–2.75) that occurred on a Singaporean-registered ship not in the wire hippin (NZ) limited’s fleet but within the wire group structure.
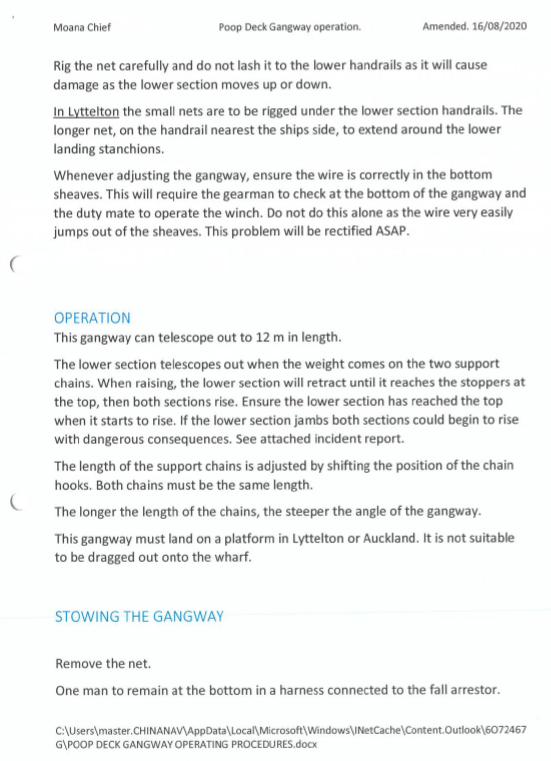
- The operating procedures had four sections (see Appendix 4). Section One ‘Safety Precautions’ stated that the CIR was in charge of rigging and stowing the accommodation ladder. It instructed the crew not to stand anywhere on the telescopic part while the accommodation ladder was being raised or lowered. When setting the handrails, only one person with a fall arrester was permitted to stand on the upper or lower platform.
- Section Three ‘Operation’ highlighted the need to adjust the side chains when the accommodation ladder was resting on a Port platform.
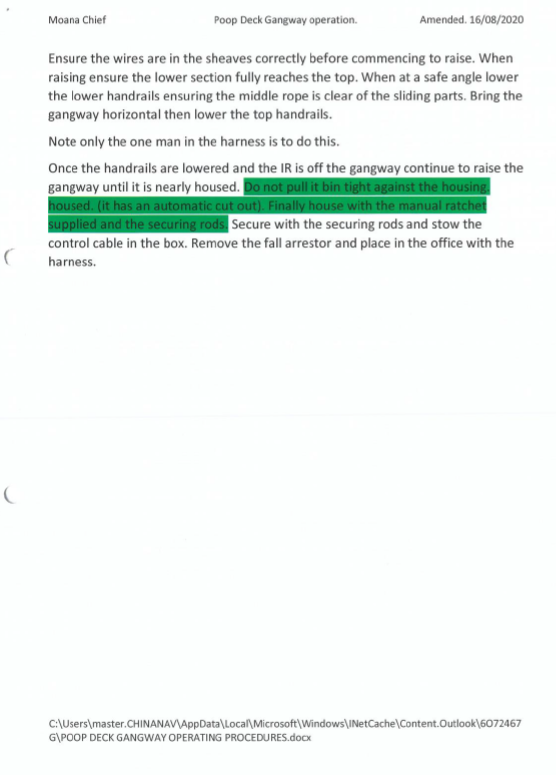
- Section Four ‘Stowing the Gangway’ covered retrieving and stowing the ladder. It instructed the operator to retrieve the lower ladder until it reached the end point before anyone was allowed to step onto it.
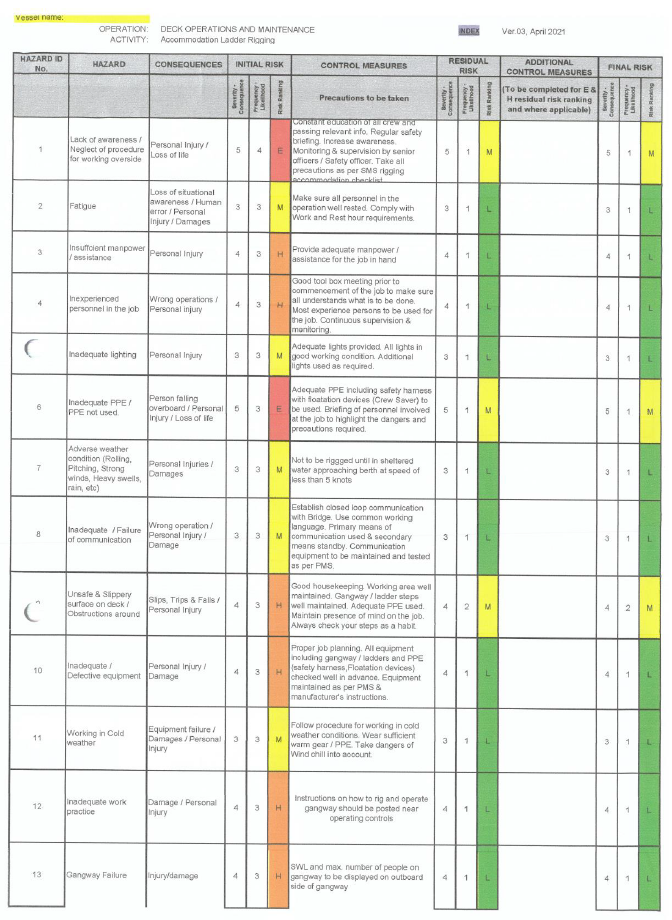
Risk Assessment
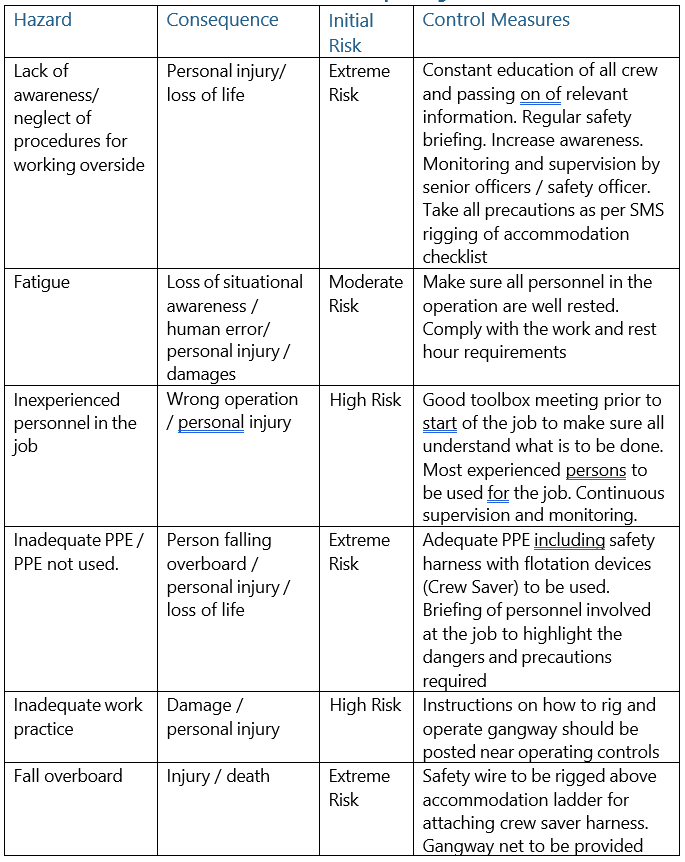
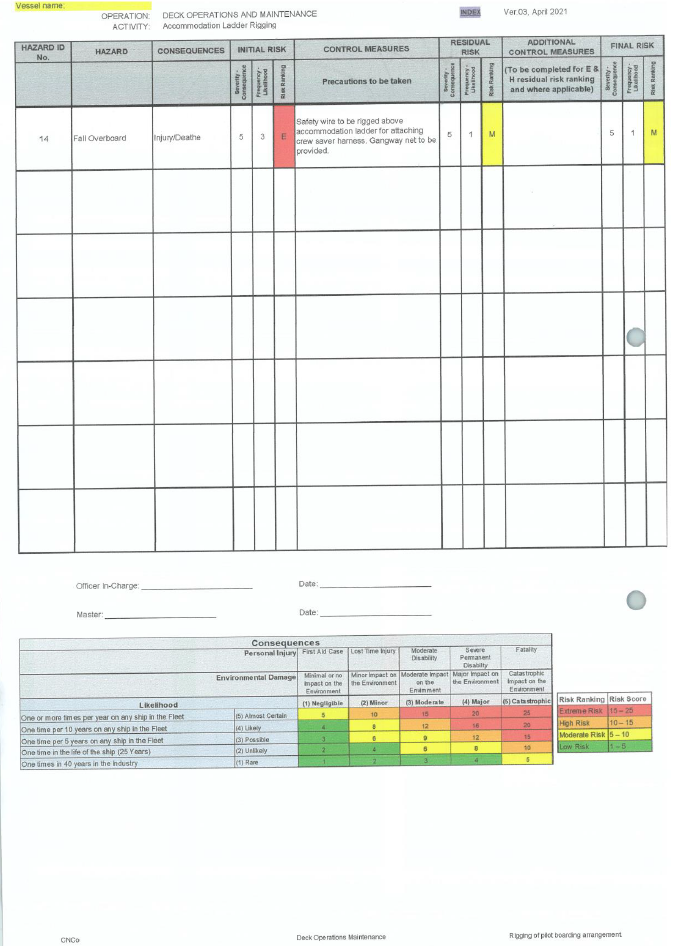
- The SMS required the crew to conduct a risk assessment for routine jobs. One such risk assessment was ‘Accommodation Ladder Rigging Ver 03’, dated April 2021. Table 1 highlights some of the hazards identified in the risk assessment and the corresponding control measures (see Appendix 5 for the full risk assessment).
Meteorological and ephemeralinformation
- The tidal data for Auckland on 10 December 2021 is shown in Table 2:
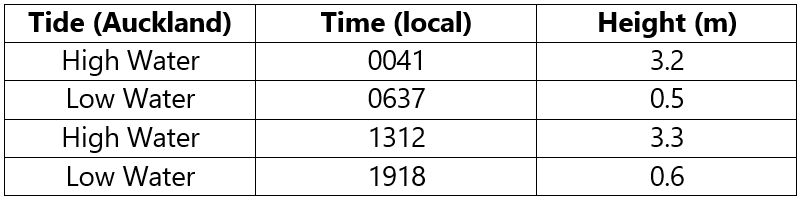
The accident occurred about one hour after low water in the morning.
- At the time of the accident the temperature was about 20C, it was mostly cloudy, with light winds of about 2 metres per second blowing from the southeast.
Recorded data
- A CCTV recording taken by a security camera fitted near the essel’s accommodation ladder was recovered following the accident. The recording allowed investigators to observe the incident as it unfolded.
- CCTV was also recovered from the Fergusson Wharf Camera 1. The recording helped investigators confirm the hypothesis of why the ladder fell off the Port platform.
Site and wreckage information
- Before the injured EWR was safely moved to the poop deck, the bottom platform of the ladder was crushed between the wharf and the essel’s side, when the mooring line was tightened. A Ports of Auckland CCTV camera recorded the occurrence (see Figure 13).
- The ladder was retrieved and stowed after the incident. The bottom platform was badly damaged, which made the ladder unsafe for any further use.

Previous accommodation ladder occurrence
- On 14 May 2020, a crew member from the Singapore registered container ship MV Szechuen, operated by another company within the Swire group structure, suffered serious crush and fracture injuries to both their legs (Company investigation report received from Swire Shipping (NZ) Ltd).
- The Transport Accident Investigation Commission (the Commission) was notified of the incident but chose not to investigate as New Zealand was in COVID-19 Alert Level 4 and travel restrictions were in place.
- The accident occurred while retrieving and securing the port side telescopic accommodation ladder at North Port, New Zealand. On this occasion, the lower ladder did not slide up to its end point, stopping approximately 1.5 metres short.
- A crew member stepped onto the fixed upper ladder to fold down the handrails. As soon as the handrail on the outboard side was lowered, the lower ladder recoiled and trapped the crew member’s lower le s between the steps of the two ladders. The crew member was subsequently removed from the ladder and, after initial first aid, was taken to a hospital in Auckland.
- The operator conducted an internal investigation with the following findings.
- The existing practice on the vessel was to untie the handrail rope from the non-shackled end, and leave it in place, before lowering the railings. In this instance, the slack handrail rope on the outboard side of the lower ladder got caught between the two ladders and prevented the lower ladder from sliding up to its ‘home’ position.
- The crew member was working in the line of recoil when they stepped onto the fixed upper ladder, with the safety stoppers removed and the taut lower ladder not yet home. When the fouled rope dislodged, the lower ladder sprung upwards and trapped the crew member’s le s.
- The officer in charge and the crew had not identified that even though the ladder was nearly horizontal the lower ladder had not reached its end stop. They had not considered the recoil hazard that the fouled lower ladder posed and continued to work in the line of fire.
- The design of the telescopic accommodation ladder made the rigging/securing process complicated. It required personnel to step on to the ladder more than once, to remove the stoppers and manually transfer the weight of the lower ladder to the bridle while rigging and vice-versa while securing.
- The officer in charge did not ensure that the process of securing the accommodation ladder was done safely. The officer was also operating the accommodation ladder winch control from the turntable, where they did not have an overview of the entire operation.
- There was an operating procedure for the accommodation ladder which was displayed near the location. These procedures were inadequate and did not address all the likely hazards involved with lowering and securing the accommodation ladder.
Analysis Tātaritanga
Introduction
- Deploying and retrieving an accommodation ladder can be dangerous and often involves crew members working over the side of the vessel. The risks associated with the operation are well known and need to be carefully managed. A telescopic accommodation ladder has several moving parts which can increase the risk of injury. It is important that operators understand the equipment and the hazards associated with it.
- The following section analyses the circumstances surrounding the accident to identify those factors which increased the likelihood of the event occurring or increased the severity of its outcome. It also examines any safety issues that have the potential to adversely affect future operations.
Why did the accident occur
- Whilst retrieving the telescopic accommodation ladder the crew untied the handrail ropes but left the handrail chains in place. When the inboard handrail chain became caught between the sliding lower ladder and the fixed upper ladder the ERW stepped onto the upper ladder to free it.
- Once the EWR had cleared the inboard handrail chain they picked up the outboard handrail chain and held onto both to prevent them from getting caught again. While holding the handrail chains the EWR stood on a ladder step close to the top of the fixed ladder.
- As the CIR resumed heaving on the fall wire to retract the lower section of accommodation ladder, the ladder dropped off the Port platform. Because the side chains were slack and not supporting the fixed upper ladder (see Figure 14) the weight was transferred from the Port platform and onto the fall wire. It resulted in an unexpected and uncontrolled upward movement of the lower ladder.
- The lower ladder slid upwards in its interlocking guides and before it reached the end point trapped the EWR’s le between the top step of the lower ladder and the third step of the fixed upper ladder (see Figure 15).
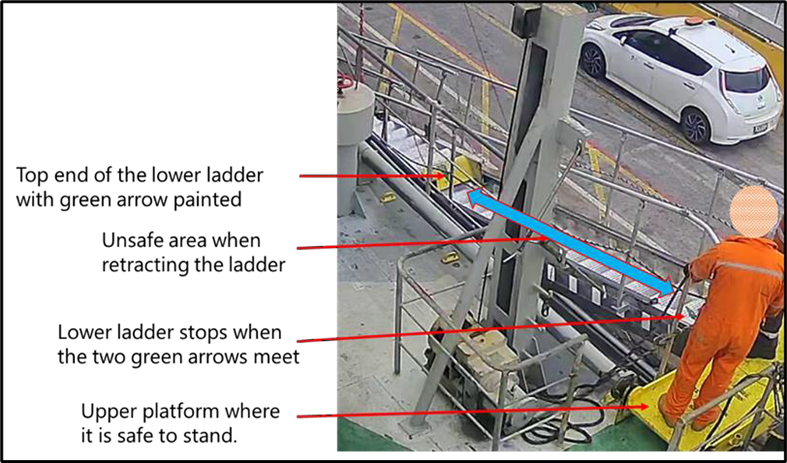
- The EWR had stood between the two green arrows marked on the steps of the upper ladder. As a result they were positioned, and working, in an area that had been identified as unsafe (see Figure 16). The arrows were a preventative safety action taken in response to a previous accident on another vessel.
- Had the state of the ladder been observed by the team before starting its retrieval, it is very likely that they would have noticed the slack side chains and, depending upon their knowled e and understandin of the ladder’s operation, adjusted them. This would have ensured that when the ladder fell off the Port platform the weight was taken immediately by the side chains and the retrieval operation was kept under safe control. Importantly, the lower ladder would not have been subjected to the force necessary for it to slide up the interlocking guide.
- The slack side chains were indicative of an accommodation ladder that had not been tended or adjusted to maintain it in a safe state. When cargo operations were completed, and the stevedores had left the vessel, the requirement to maintain safe access to and from the vessel became less significant.
- Had the accommodation ladder operating instructions been followed, specifically that no one was to step on the ladder until the green marks on the upper ladder and the lower ladder fully coincided, then the injury to the crew member could have been avoided.
Risk assessment for retrieving the accommodation ladder
Safety issue: The possibility of the accommodation ladder falling off the Port platform had not been identified as a hazard and risk mitigation control measures were not followed.
- The vessel operator had conducted in-house training for all crew in June 2021. It was therefore reasonable to expect that those crew members allocated to deploying and retrieving the ladder would be familiar with the hazards identified in the risk assessment (see Appendix 5).
- The operating procedures for the accommodation ladder were posted near the ladder and were referred to in the accommodation ladder risk assessment.
- Although the risk assessment had addressed the hazard of stored energy, it had not identified all the possible scenarios likely to cause the lower ladder to retract in an uncontrolled manner. The hazard associated with the ladder falling off the Port platform was a case in point. The consequence of retrieving the ladder whilst it was on a platform and the side chains were slack had also not been considered.
- A review by the Commission of the ship’s Accommodation Ladder Rigging Risk Assessment found that several hazards identified during the risk assessment process might have benefitted from more robust control measures. These hazards are discussed below.
Supervision
-
The risk assessment had identified that a lack of awareness and neglect of procedures for working overside was considered an extreme hazard associated with operating the accommodation ladder. The control measure in place to mitigate the risk and reduce it to a more manageable level was:
‘Constant education of all crew and passing relevant info. Regular safety briefing. Increase awareness. Monitoring & supervision by senior officers / Safety officer. Take all precautions as per SMS rigging accommodation checklist’
- Although there were several infringements of the accommodation ladder operating procedure, there was little supervision or intervention by the person in charge of the operation or by the officers observing. It is reasonable to expect a well-trained crew to exercise their judgement and call ‘stop work’ when they observe an unsafe condition or act that may result in an accident (refer to Part B of the form in Appendix 6).
- It is almost certain that the injury to the crew member could have been avoided had the person in charge, or the officers, called ‘stop work’ and ensured that the crew member moved to a safe position.
Assessing risk
-
'Inexperienced personnel in the job’ had been identified as a hazard and was considered to be a high risk. The control measure identified to mitigate the risk and reduce it to a more manageable level was:
‘Good toolbox meeting prior to commencement of the job to make sure all understands what is to be done. Most experience persons to be used for the job. Continuous supervision & monitoring’.
- At the time of the accident the EWR had about 44 weeks’ experience working on the vessel. Even though the EWR was not a permanent employee, they were regularly rostered as relieving crew on the vessel. They were the most experienced person at the scene in respect of working with the poop deck accommodation ladder. The CIR had recently been appointed as CIR and had not worked with telescopic accommodation ladders before. Similarly, the IR had not worked with telescopic accommodation ladders until sailing on this vessel.
- The EWR had been given a later wakeup call due their duties the previous evening. When they arrived at the work site, the operation to retrieve the ladder had already started. There was no evidence to show that a toolbox meeting had been conducted or that checklist N051014, ‘Checklist for Pilot, Accommodation, Combination Ladder’ (see Appendix 3) had been completed.
- The Commission found that the last pre-work meeting form31 for accommodation ladder operations that the ERW participated in was completed on 22 August 2021, (see Appendix 6) nearly four months before this accident. The vessel operator had a policy for completing pre-work meeting forms for routine tasks. However, for repetitive tasks the policy stated, “for certain work activities that may be repetitive over a relatively short period of time, pre-work meeting need not be conducted prior to each occasion that such a task is undertaken so long as the hazards remain unchanged”. The vessel operator told the Commission that for these repetitive work activities, there was an expectation that the toolbox meetings would still be required. An example of repetitive work activity was rigging / unrigging the accommodation ladder or pilot combination ladder.
- Had a toolbox meeting been completed and operating instructions consulted before starting to retrieve the accommodation ladder, the Commission considers it likely that the danger area marked on the accommodation ladder would have been discussed and the dangers associated with it highlighted.
- By not completing a toolbox meeting before starting work, the crew missed the opportunity to review the risks and mitigation strategies and familiarise themselves with their role and responsibilities before starting a routine high-risk activity.
Working overside and falling overboard
- Falling overboard had also been identified as a hazard and was considered high risk with a consequence of injury or death. The control measure to mitigate the risk and reduce it to a more manageable level was for a safety wire to be rigged above the accommodation ladder and used by the crew to clip on a safety harness or fall arrestor. A gangway net was also to be provided.
- At the time of the accident the gangway net had been removed and stored away, which substantially increased the consequence had someone falling overboard. It reinforced the need for crew working overside to wear a safety harness or fall arrestor connected to a designated anchor point.
- On this occasion the designated anchor point was a wire sling rigged above the ladder. The wire was manually spliced and connected across the ladder posts. There was no safe working load marked on the wire and nothing to show that the wire met any New Zealand or international standard to withstand a shock load caused by a person falling.
- New Zealand Maritime Rules Part 49.4 governs the maintenance and inspection of ships’ lifting appliance and loose lifting gear. The wire sling used at the accommodation ladder was not part of the ship’s liftin ear. The industry best practice is that all wire slings on board a ship have an identification number and a safe working load marked on them, and are inspected and maintained to a similar standard as lifting gear.
- While New Zealand has not formalised these best practises, the United States of America has, through implementing U S Department of Labor Occupational Safety and Health Administration (OSHA) standards 1910.184, which state:
- 1910.184(c)(11): shock loading is prohibited
- 1910.184(c)(13): employers must not load a sling in excess of its recommended safe working load as prescribed by the sling manufacturer on the identification markings permanently affixed to the sling
- 1910.184(c)(14): employers must not use slings without affixed and legible identification markings.
- The standard is accentuated by the United States Coast Guard, Marine Safety Alert, 04-2 ‘Verify Your Wire Rope Terminations32: Incorrect Terminations can Lead to Catastrophic Failure’. The safety alert focuses on the importance of verifying the condition and manufacturing of the wire sling terminations used in a load-handling or lifesaving capacity such as this one.
- Notwithstanding the need for certified anchor points, at the time of this accident the crew working overboard were not wearing either a safety harness or a fall arrestor.
- In respect of this accident neither a safety harness nor fall arrestor would have prevented the accident from occurring, but it demonstrates a gap between the operator’s risk mitigation requirements and the equipment and practices onboard the vessel.
- The vessel operator had developed a ship specific accommodation ladder procedure, supported by a risk assessment and the crew had been trained in its use.
- Safety procedures and instructions alone cannot guarantee that a particular operation is conducted safely; to be effective crew members must follow and comply with them.
- However, whilst the vessel continues to operate with the same telescopic accommodation ladders the risk assessment for the operation should be reviewed and procedures contained within the operator’s updated in light of this accident. The Commission has made a recommendation in section 6 of this report to address this safety issue.
Safety Culture and Leadership
Safety issue: Non-conformance to operating procedures and a diffusion of responsibility with respect to oversight and supervision are symptomatic of more systemic issues regarding the safety culture onboard.
- Following the operator’s own internal investigation into the MV Szechuen accident, the operator implemented several safety actions to help prevent a similar accident.
- To ensure fleet-wide awareness of the accident, the operator issued a safety alert that highlighted the root causes and specified the preventative actions to be implemented. One of the immediate causes identified was that the crew member was in an unsafe position for the task. When the lower section of the accommodation ladder recoiled, it trapped the crew member, causing a serious injury.
- The root causes identified in the safety alert are:
- inadequate hazard identification and risk perception
- lack of situational awareness
- design of the accommodation ladder with a complicated rigging/unrigging process.
- improper leadership
- inadequate procedures of rigging and securing the accommodation ladder.
- The vessel’s accommodation ladder operating procedures had been amended to take into consideration the root causes and preventative actions specified in the safety alert.
- As part of the risk mitigation process, the crew received in-house training and were given the opportunity to discuss the MV Szechuen accident. The in-house training was intended to reinforce their understanding of the risks involved when working with the accommodation ladder, and to appreciate the safety benefits of the protections Implementation is prescribed.
- The Moana Chief accident showed that the implementation of several safety measures identified from the previous accident was ineffective. This was demonstrated by the crew not following the revised procedures and the lack of intervention of other crew members who were observing the operation.
- Crew training was an important part of the risk mitigation process. However, there were no audits conducted to assess whether the training was successful and whether there had been a change in behaviour.
- Non-conformance to operating procedures, and a diffusion of responsibility are symptomatic (indicators) of more systemic issues. The Commission believes that more can be done by both the operator and the onboard management team to improve safety culture and leadership and reduce at-risk behaviour and non-conformance to operating procedures.
- The Commission has made a recommendation in section 6.3 of this report to address this safety issue.
Appendix 1. Survey report for new accommodation ladder
Appendix 2. N051014D Work Overside
Appendix 3. N051014C Checklist for Pilot, Accommodation, Combination Pilot Ladder
Appendix 4. Moana Chief Poop deck gangway operating procedures
Appendix 5. Risk Assessment Accommodation L adder R igging dated April 2021
Appendix 6. Pre Work Meeting Form