The log carrier Funing was departing port when its main engine failed. Drifting in the current, its propeller and rudder tangled in a buoy mooring chain. A fuel injection unit had seized due to coking debris caused by low-viscosity low-sulphur fuel. Ship’s crew unaware of latest maintenance guidance about effect of low-sulphur fuel on engine. Key issues: engine maintenance, tug assistance, crew resource management.
Executive summary Tuhinga whakarāpopoto

What happened
- On 5 July 2020, the log carrier Funing finished loading its cargo at the Port of Tauranga and began preparations for departure. At about 2200 the officer of the watch contacted the engineers and informed them that departure was planned for midnight.
- When the main engine was tested in the astern direction, the main engine fault log indicated there was a fuel injection quantity piston failure.
- The engineering team attempted to rectify the fault but were unable to before the vessel departed its berth at about 0018, when the fault reoccurred again on the main engine.
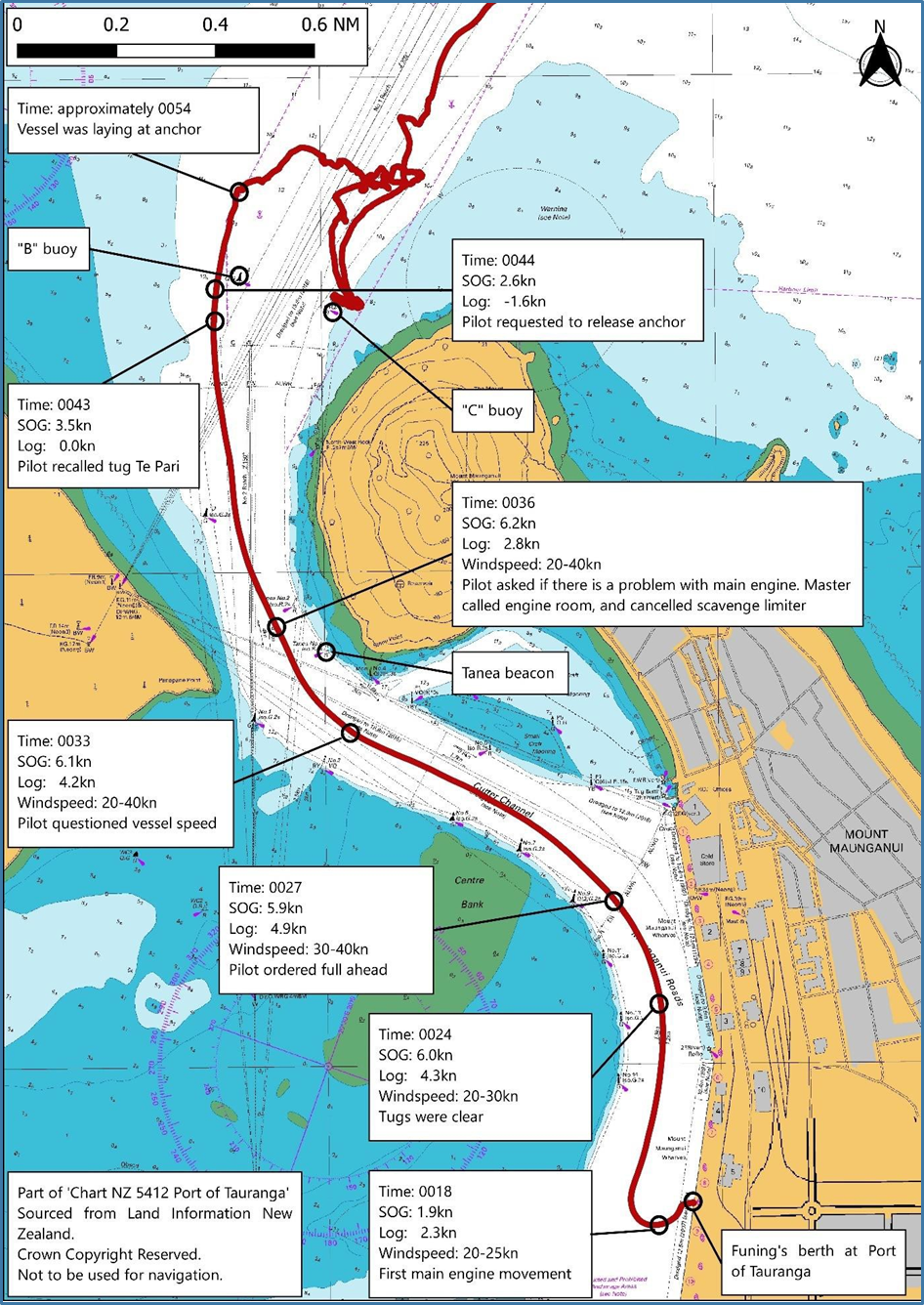
- At 0024 the tugs were let go, and at 0027 the Port of Tauranga harbour pilot ordered full ahead. The vessel’s speed through the water was about 4.3 knots.
- By 0043 the vessel’s speed through the water was about 0 knots, and its speed over the ground was about the same as the ebbing tidal stream of 3.5 knots. The vessel was effectively drifting with the current and moving out of the channel.
- Shortly afterwards the vessel drifted over channel marker ‘B’ buoy and the buoy’s mooring chain became entangled in the Funing’s rudder and propeller.
Why it happened
- The engineers identified a fault with the main engine during pre-departure testing, but they did not confirm it was rectified before departure.
- Ineffective communication between the master and chief engineer meant the bridge team were not fully aware of the problem with the main engine, nor its implications in respect of vessel manoeuvrability.
- The main engine defect was not accounted for during the bridge team’s preparation
- for departure, and therefore the harbour pilot was also unaware of the defect.
- The main engine fault was very likely due to the effect of low-sulphur fuel on the injection control unit.
What we can learn
- The role that bridge resource management and engine room resource management play in respect of the safety of a vessel cannot be overstated. Good communication between departments is a core principle that may, had it been implemented on this occasion, have caused the master to reconsider the planned departure time.
Who may benefit
- Vessel owners, operators, maintenance teams and crew. Port operators and marine pilots.
Factual information Pārongo pono
Narrative
- On the afternoon of 5 July 2020, the log carrier Funing finished loading its cargo of logs and began preparations for departure. At about 2200 the officer of the watch (OOW) on the bridge called the engine room and gave the engineers notice of departure at midnight.
- The second and third engineers began conducting pre-departure checks. The chief engineer arrived in the engine room at about 2215.
- At about 2225 the duty engineer officer called the bridge and asked permission to blow through the main engine (air is blown through the engine before starting it to remove any residual exhaust gas or combustion product trapped after the engine was shut down) using air.
- At about 2228, as part of pre-departure testing, the main engine was tested in the ahead and astern directions from the engine room. When it was tested in the astern direction, the main engine fault log indicated there was a fuel injection quantity piston failure on number two cylinder.
- Engineers removed the quantity piston cover, cleaned the piston rod and sensor with lubricant and reset the main engine slowdown alarm.
- At 2240 an engineer called the bridge to transfer control of the main engine to bridge control, allowing the OOW to test the engine ahead and astern of the bridge. The bridge logbook noted at 2241, “engine tested ahead and astern ok”. Shortly afterwards, at the chief engineer’s instruction, control of the main engine reverted to the engine room. At 2247 the main engine electronic fault log indicated an injection quantity piston failure on number two cylinder.
- At 2300 the main engine control was transferred to the bridge so that the OOW could test the main engine both ahead and astern. The OOW informed the master of a fault with the main engine, and the master in turn spoke to the chief engineer on the telephone. Details of the fault were not discussed, but the master did ask if it would be repaired in time for departure and was reassured by the chief engineer that it would.
- At about 2304 the engine was tested from the bridge, but the fault with the quantity piston was still present. At that time the engineers believed the problem to be the sensor on the injection quantity piston. At about 2330 the sensor was replaced, and the piston rod was lubricated.
- The chief engineer telephoned the OOW on the bridge and advised that there was a problem with the main engine. The chief engineer asked when the harbour pilot was due to arrive on board for departure and was told midnight.
- At about 2345 the chief engineer telephoned the master on the bridge. During the conversation the chief engineer told the master to press the ‘cancel slowdown button’ situated on the main engine control panel, which the master did. The cancel slowdown button cancelled the automatic engine slowdown. The master did not ask the chief engineer why it was necessary to press the cancel slowdown button. This point is discussed further in section 3.
- At about 2359 the engineer on watch telephoned the bridge and asked for the main engine to be placed in bridge control.
- At about midnight the pilot arrived on the bridge and the master-pilot exchange of information took place. During the exchange the master confirmed to the pilot that there had been no immobilisation of the main engine and that the engine was free of any defects. They also discussed the passage plan for departure.
- Forecast environmental conditions at the time of departure were:
- northerly wind 35 knots (one knot is equal to 1.852 kilometre per hour) gusting 45 knots and then easing
- tidal stream at the entrance to the port 2.5 knots ebb (ebb tide is an outgoing tide).
- Tugs were secured at about 0006, and all mooring lines were let go and clear at about 0018.
- As shown in Figure 3, the first main engine movement was at 0018, and the quantity piston failure alarm for number two cylinder was triggered immediately.
- Over the next three minutes the pilot ordered dead slow ahead, slow ahead and half ahead.
- At 0024 the tugs were let go, and at 0027 the pilot ordered full ahead and the telegraph (a telegraph is a communications device used by a bridge team to give main-engine orders to a vessel’s main engine) was set to full ahead (68 rpm [revolutions per minute]). The chief engineer noted that the main engine speed was not increasing above 48 rpm (this point is discussed further in section 3). The vessel’s speed through the water was about 4.3 knots.
- At 0028 an exhaust gas deviation alarm activated in the engine room because the number two cylinder was not firing.
- At about 0033 the pilot asked the master why the vessel’s speed was so slow, and requested more speed. In the next few minutes, the pilot repeatedly told the master the vessel was not going fast enough and asked if there was a problem. When the pilot first questioned the vessel’s speed the master called the chief engineer in the engine room and told the chief engineer that they needed more speed. During the conversation the master asked the chief engineer if they could cancel the scavenge limiter, to which the chief engineer agreed.
- By 0043 the Funing’s speed through the water was about 0 knots, and its speed over the ground was about the same as the ebbing tidal stream of 3.5 knots. The vessel was effectively drifting in the tidal stream and starting to move out of the channel near ‘B’ buoy (Figure 3). At about 0044 the pilot recalled the harbour tug Tai Pari to assist, and the starboard anchor was let go.
- Shortly afterwards the Funing drifted over the top of the channel marker ‘B’ buoy, and the buoy’s mooring chain became entangled in the Funing’s rudder and propeller.
- At about 0048 the main engine automatically shut down on overload.
- By about 0054 the Funing was anchored outside the main channel with its stern pointing towards shallow water.
- By about 0054 the tug Tai Pari had arrived on scene and made fast with a line to the Funing’s starboard quarter (the side of the vessel between the stern and midship, typically at the aft end). The tug attempted to pull the stern into the main channel, but due to the force of the wind and tide it was unsuccessful, and the tow line parted.
- A second tug, the Sir Robert, had also made its way to the area. Both tugs remained on station nearby.
- At about 0115 the engineers began to replace the injection control unit (ICU) on number two cylinder with a new unit. By 0220 the new unit was in place and tested. No alarms or faults resulted.
- The port anchor was let go and the vessel lay to two anchors. As the tide turned the vessel pivoted around the anchors and lay aligned with the channel, with the bow pointing north-northeast.
- The Funing’s port quarter lay very close to ‘C’ buoy, so the tug Sir Robert was used to try to drag the stern into deeper water. Due to the environmental conditions the line parted. The pilot made the decision for the vessel to remain in position, lying to both anchors, and wait for the tide to turn.
- At about 0800, once the tide had begun to ebb, both tugs re-secured and towed the Funing outside the harbour limits and re-anchored it.
- On 14 July 2020 the Funing was towed back into Port of Tauranga for repairs. The hull was surveyed, and damage was found to the rudder stock and the tip of one propeller blade.
- On 6 September 2020 the Funing was taken under tow to Singapore by an ocean-going tug for repair.
Introduction to the Funing’s propulsion system
- The Funing’s main engine was a slow-speed, five-cylinder, two-stroke diesel, Wärtsilä RT-Flex model, connected to a fixed-pitch propeller.
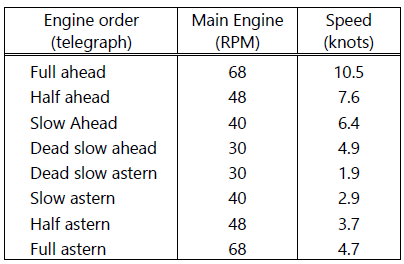
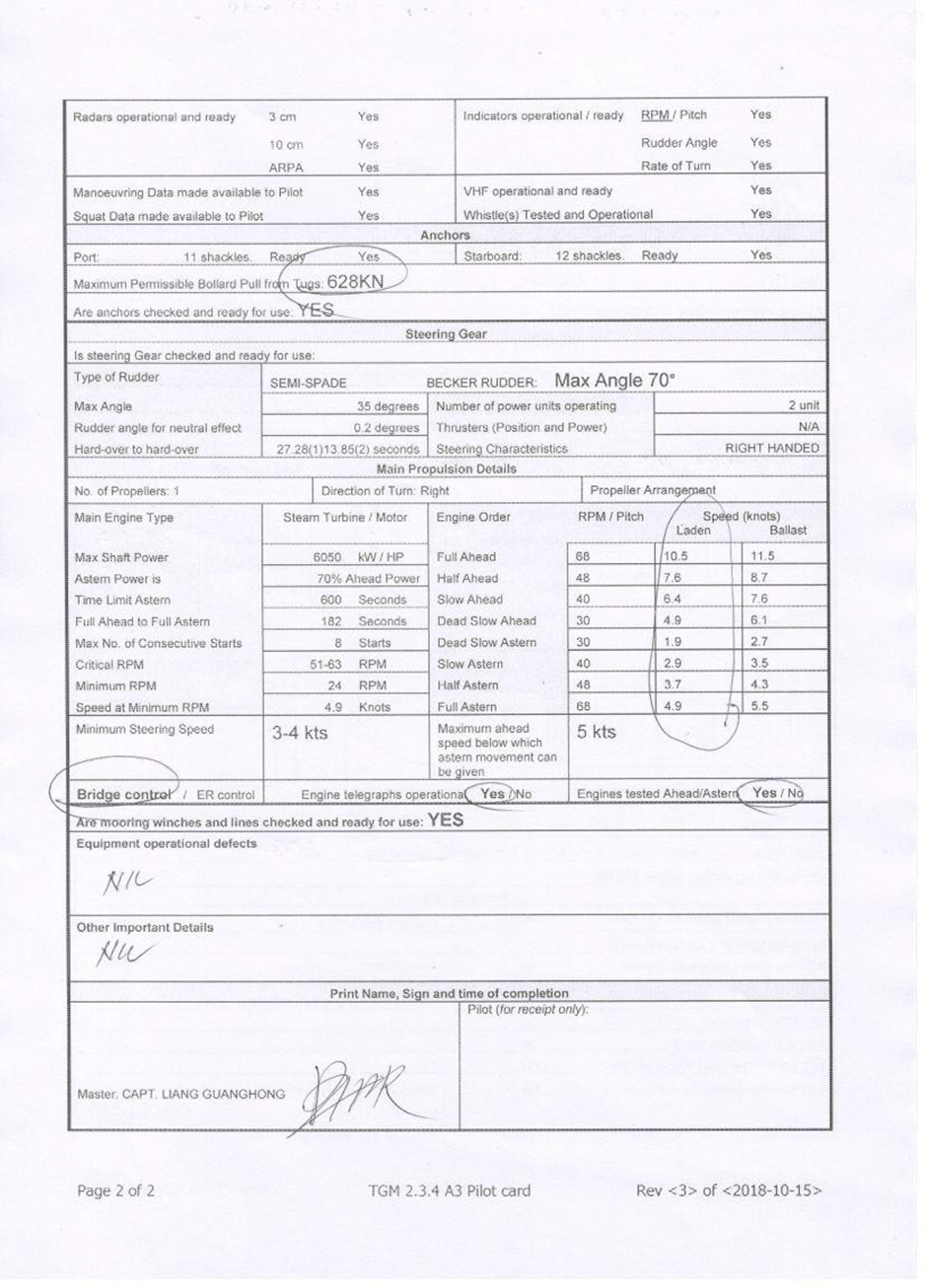
- The propulsion system did not include a gearbox, so the main engine rpm correlated to vessel speed through the water. The relationship between main engine rpm and design vessel speed is given in the Thome Ship Management pilot card (Appendix 1), and that excerpt is shown in Figure 4. Note the Funing was laden during its departure from Port of Tauranga.
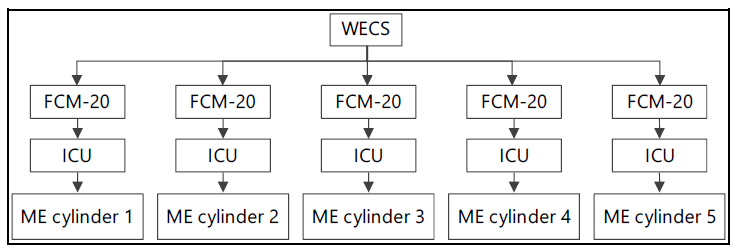
- The Funing’s main engine was controlled by a Wärtsilä engine control system (WECS) (Figure 5), which in turn controlled an electronic Flex Control Module (FCM-20) for each cylinder. The FCM-20 controlled electro-hydraulic valves for each ICU and is discussed in more detail later in the report.
- The function of the ICU was to supply a predetermined quantity of fuel to the engine cylinder fuel injectors. The quantity of fuel varied depended on the load on the engine, and was apportioned by a fuel injection quantity piston within the ICU. The quantity of fuel was measured by a sensor attached to the fuel injection quantity piston.
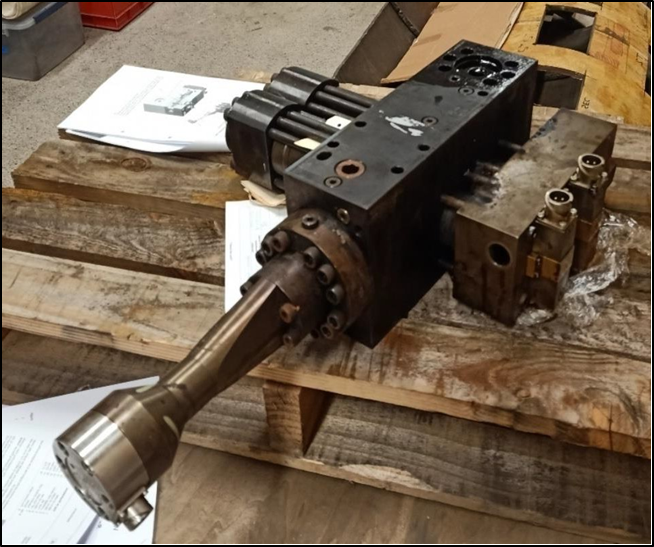
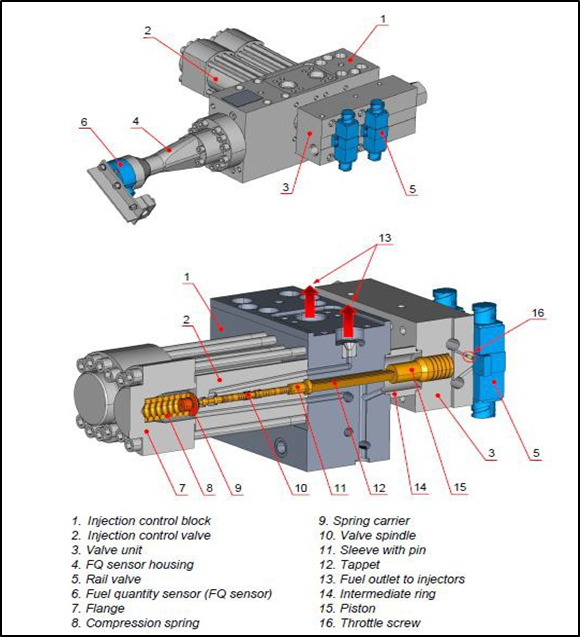
Injection control unit
- The ICU was a key component of the RT-Flex engine. Figure 5 shows a photograph of the ICU removed from the Funing after the accident, and Figure 6 shows a labelled image.
- The working principle of RT-Flex engines was that fuel injection timing was controlled by a computer via electro-hydraulic valves, rather than mechanical camshafts.
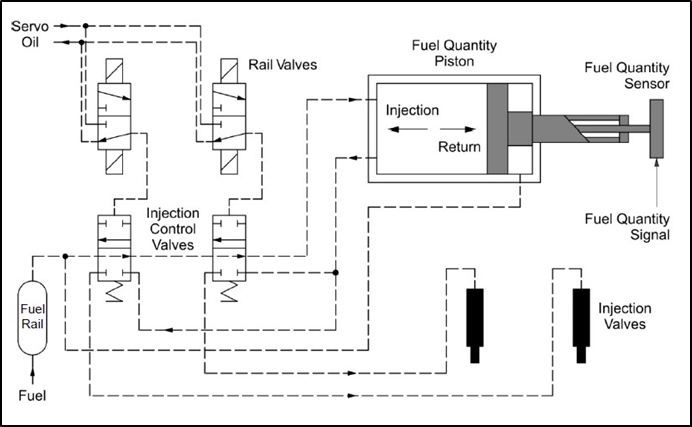
- The WECS controlled the functions of the main engine. For each combustion cycle of each cylinder, the WECS sent an ‘injection command’ to the FCM-20, which was relayed to the electro-hydraulic rail valves on the ICU (Figure 7).
- When the rail valve was actuated it opened the servo oil supply to a hydraulic piston within the rail valve, which in turn caused the injection control valve to open.
- Once the injection control valve had opened, the quantity piston started to move and fuel flowed to the fuel injector valves.
- Injection would continue until the WECS sent, via the FCM-20, a ‘return command’ to the electro-hydraulic rail valve, which would close that valve.
- When the rail valve closed the fuel injection control valve would close, ending the fuel supply to the fuel injector valves.
- The quantity piston would then slowly return to its initial position, ready for the next injection cycle.
Maintenance on the main engine ICU
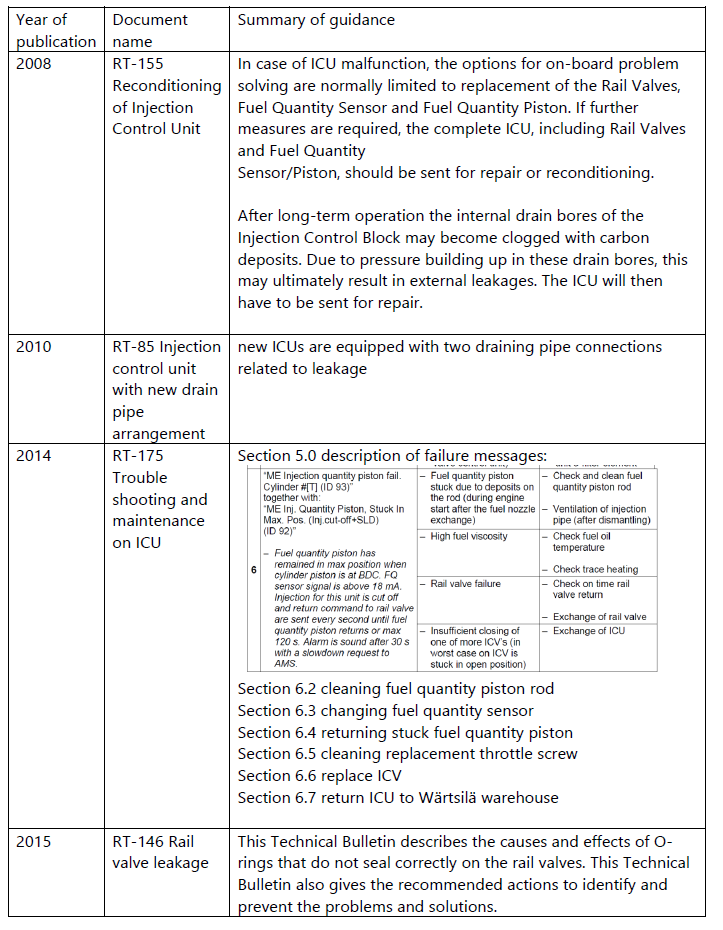
- Wärtsilä stated in its ICU maintenance guidance documentation: “The life expectancy of ICU components depends upon operational conditions.” In the case of ICU malfunction, the options for onboard problem-solving were normally limited to replacement of the rail valves, the fuel quantity sensor and the fuel injection quantity piston. If further measures were required, the complete ICU, including rail valves and fuel quantity sensor/piston, should be sent for repair or renewal.
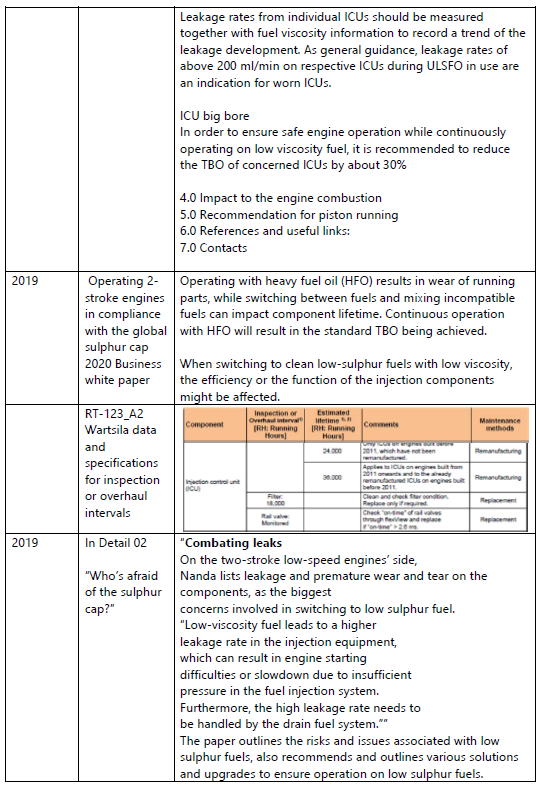
- Wärtsilä technical bulletins advised that the onboard maintenance of ICUs was limited to trouble shooting and “simple rectifying actions”. They stated that ICUs should be returned to a Wärtsilä service centre for remanufacture after they had reached their life-time service hours, which Wärtsilä estimated at 36,000 hours of service. The data and specification for overhauls of engine components are shown in Appendix They recommend the ICU lifetime service hours, checking a filter and checking the engine monitoring software for incorrect rail valve timing. Incorrect rail valve timing could indicate excessive leakage.
- The defective ICU removed from the Funing had accumulated 24,586.6 hours of service.
- One of the onboard maintenance tasks was to monitor any ‘leakage’ within the ICU. Leakage is a normal operating feature of an ICU.
- When mechanical components, such as a hydraulic piston or cylinder liner, slide against each other they are subject to wear. As the two components wear, the clearance between them increases. At some stage the clearance will be large enough for oil to leak between the components. Fuel quality can have a significant effect on engine wear, and can vary depending on where it is sourced.
- The viscosity of the fuel oil can also lead to leakage. Low-viscosity fuel can leak between components where high viscosity fuel would not.
- The leakage can result in fuel oil being present where it should not be. In the case of fuel leakage in an ICU, where the temperature is high enough, a coking process may occur and create coking deposits within the ICU.
- Recent maintenance of the ICUs had included measuring leakage each month. The most recent testing had been conducted on 11 May 2020, approximate two months before the accident. The test result had not indicated an issue with leakage. Records showed no test was conducted in June, hence it was one month overdue.
- Leaked oil can drain from the ICU and is collected in a drain tank; the drain tank is monitored daily. Changes in the rate of oil leakage to the drainage tank may indicate a problem with an ICU.
Low-sulphur fuel
- As part of reducing harmful emissions from shipping, the International Maritime Organization (IMO) had introduced a limit on sulphur in marine fuels; this had come into force in January 2020. Compliant fuel was referred to as ‘low-sulphur fuel’. The Funing was using low-sulphur fuel.
- Wärtsilä had provided guidance on “operating 2-stroke engines in compliance with the global sulphur cap 2020” as a business white paper in 2019.
- The paper had advised that: “continuous operation of the engine using high sulphur HFO (heavy fuel oil) would result in the standard lifetime service hours being achieved. When switching to clean low-sulphur fuels with low viscosity the efficiency or function of the engine’s fuel injection components might be affected”.
- Wärtsilä also noted in its technical journal, In Detail (issue 02 2019), that leakage and the premature wear and tear of components were the biggest concerns when switching to low-sulphur fuel.
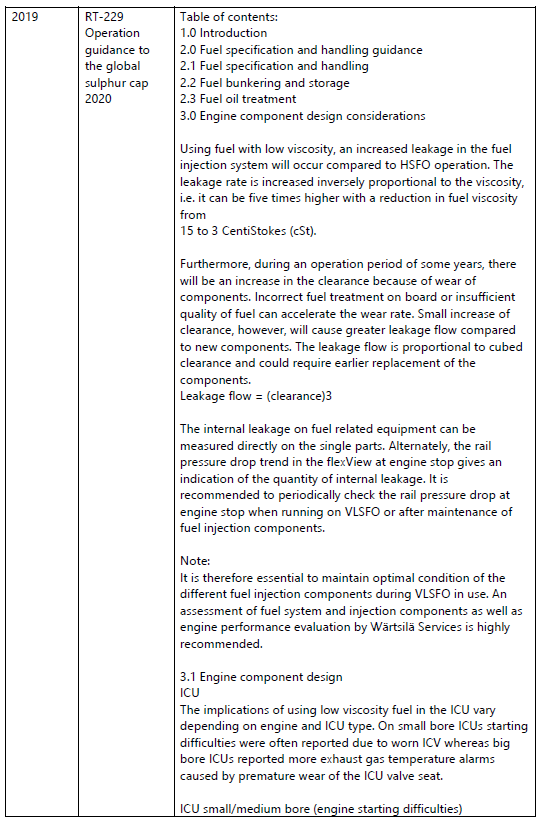
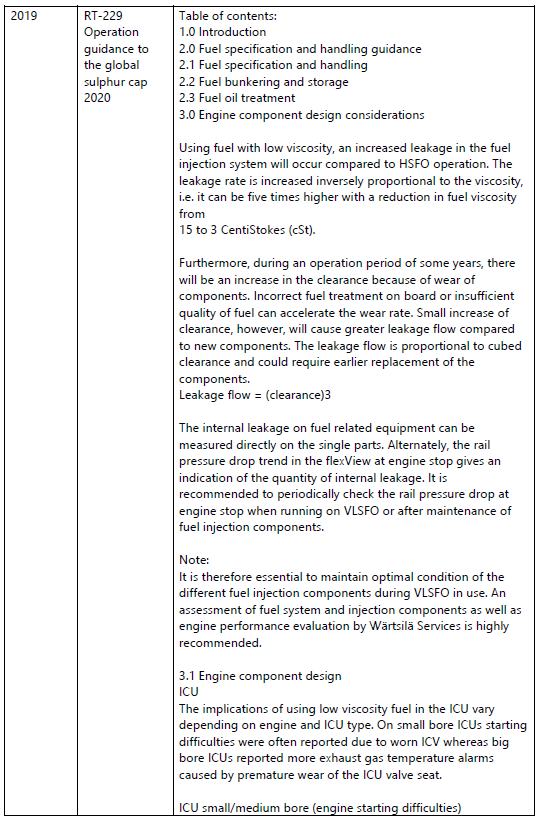
- Wärtsilä provided a technical bulletin, RT-229, titled Operation Guidance to the Sulphur Cap 2020, which targeted all owners and operators of Wärtsilä two-stroke engines.
- Section 3.1 of RT-229 discussed the implications of low-sulphur fuels for ICUs. The implications were outlined under two categories: small and medium bore engines, and big bore engines.
- With respect to small and medium bore engines, such as that fitted to the Funing, RT-229 stated, “Leakage rates from individual ICUs should be measured together with fuel viscosity information to record a trend of the leakage development. As general guidance, leakage rates… on respective ICUs during [low-sulphur fuel] use are an indication for worn ICUs.”
Thome Ship Management safety management system
- The IMO’s International Safety Management Code requires vessels to maintain a safety management system that:
- is managed and enforced by the master
- ensures the maintenance of the ship in safe condition
- ensures compliance with the relevant rules and regulations.
- The Funing was managed by Thome Ship Management Pte. Ltd. (Thome Ship Management). The vessel’s safety management system was contained within a safety management system manual. In respect of this accident the relevant sections of the Funing’s safety management system manual are outlined below.
The engine room
- The OOW provided the engineers with two hours’ notice for preparing and testing the main engine and auxiliary systems in accordance with their safety management system checklist. Under normal circumstances, two hours provided adequate time to work through the checklist and test the main engine ahead and astern from both the engine room and the bridge.
The bridge
- The bridge team were required to complete, and sign, a hard-copy checklist that covered bridge preparation for sea. One of the checklist items (shown in Figure 9) was to confirm with the engineers that the main engine had been tested both ahead and astern. When the checklist was completed it was countersigned by the master. On the day of the accident the checkbox confirming that the main engine had been tested was ticked.

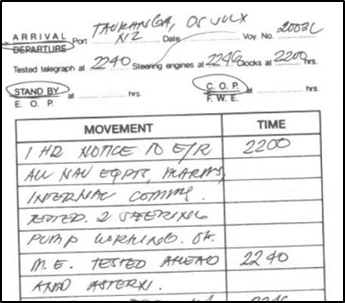
- The bridge manoeuvring logbook and bell book (a manoeuvring logbook and bell book is a document that records information significant to a vessel’s movements and the main engine) was a single logbook that was used to record vital information about the vessel’s movements. As shown in Figure 10, the manoeuvring logbook and bell book recorded that the main engine had been tested ahead and astern at 2240. The bridge logbook recorded the same.
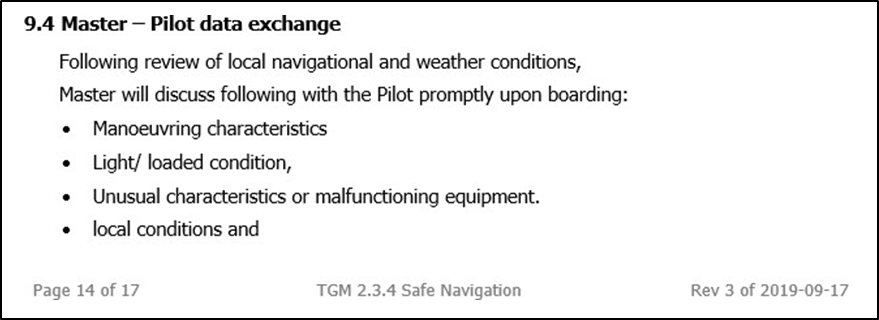
- When a pilot boards a vessel, a formal meeting takes place between the master and the pilot, known as the master-pilot exchange of information (Appendix 1). The purpose of the meeting is to ensure that the pilot and the bridge team have, among other things, a shared mental model of the intended passage plan, the vessel manoeuvring characteristics and any operational defects.
- The Funing’s safety management system manual included a section regarding the master-pilot exchange (shown in Figure 11) that, in part, required the master to discuss “unusual characteristics, or malfunctioning equipment”.
- A pilot card (Appendix 1) was completed by the master to provide the pilot with critical information in an easily accessible format upon their boarding the ship. It included whether the main engine had been tested ahead and astern (excerpt shown in Figure 12). Although the checkbox had been circled ambiguously, it was likely that it showed the main engine had been tested as already noted in the bridge logbook, manoeuvring logbook and bell book.
- The pilot stated at interview that they had not been made aware of any defects or issues with the main engine prior to sailing.

Roles of the master and chief engineer
- The Funing’s safety management system manual included sections defining the responsibilities of each of the vessel’s crew.
- The master of the Funing was responsible for, in part:
- the safety of life, ship and cargo
- ascertaining seaworthiness of the vessel in all respects (stores, navigation equipment, machinery etc) prior to sailing.
- The chief engineer of the Funing was responsible for, in part:
- the maintenance and operation of all machinery on board
- the safe running, management and maintenance of all engine and machinery related items
- keeping the master informed of all matters related to the vessel’s machinery and electrical installations.
Standards of training, certification and watchkeeping
- The IMO adopted the International Convention on Standards of Training, Certification and Watchkeeping for Seafarers (the STCW Convention) in 1978, and the most recent major revision came into force in 2010. In 1995 the Seafarers’ Training, Certification and Watchkeeping Code (STCW Code) was adopted and gave effect to the STCW Convention.
- Part A of the STCW Code – Mandatory Standards, Chapter II (Standards regarding the master and deck department) and Chapter III (Standards regarding the engine department), required that officers in charge of a watch “demonstrate the competence to undertake, at the operational level, the tasks, duties and responsibilities listed”, which included:
- maintain a safe watch using the principles and methods of BRM (bridge resource management) or ERM (engine room resource management).
- One principle of BRM and ERM was ‘effective communication’. The criteria for effective communication were listed as:
-
communication is clearly and unambiguously given and received
For example, when the control of the main engine is transferred to the bridge prior to departure, the chief engineer must clearly state whether the main engine is ready for manoeuvring, or describe any issues that might limit the ability to manoeuvre the vessel safely
-
questionable decisions and/or actions result in appropriate challenge and response
For example, if a master were made aware of a potential issue with the main engine prior to departure, and the chief engineer requested the master to activate a button that cancelled the main engine’s automatic slowdown, the master should challenge that request.
Funing crew
- The master held a master mariner certificate of competency issued in 2008. The accident voyage was part of their second tour of duty as master on board the Funing.
- The chief engineer had been promoted to the position of chief engineer in 2011. This tour of duty was the first time they had sailed on board the Funing.
- At the time of the accident the master and the chief engineer had been on board the Funing for about 10 months and six months respectively.
Port of Tauranga
- Port of Tauranga provides a pilotage service to vessels over 250 gross registered tons unless the master holds a pilot exemption certificate; the Funing was over 250 gross registered tons and required a pilot.
- The Port of Tauranga safety management system manual provided pilots with standard operating procedures to support their operations and ensure safe pilotage. The safety management system included the environmental conditions suitable for conducting pilotage operations.
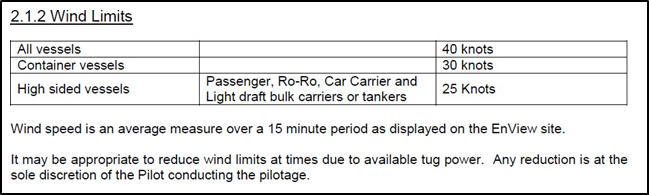
- The standard operating procedures prescribed an upper wind limit for pilotage based on the type of vessel involved (Figure 13). The prescribed upper wind limit for the Funing, a fully laden, deep-draught bulk carrier, was 40 knots.
- Further, the wind limit could be extended or restricted by the pilot, in which case the master should be fully informed on and agree to the intended movement.
- Pilots were also to consider the impacts of sea and swell conditions on vessels’ speeds.
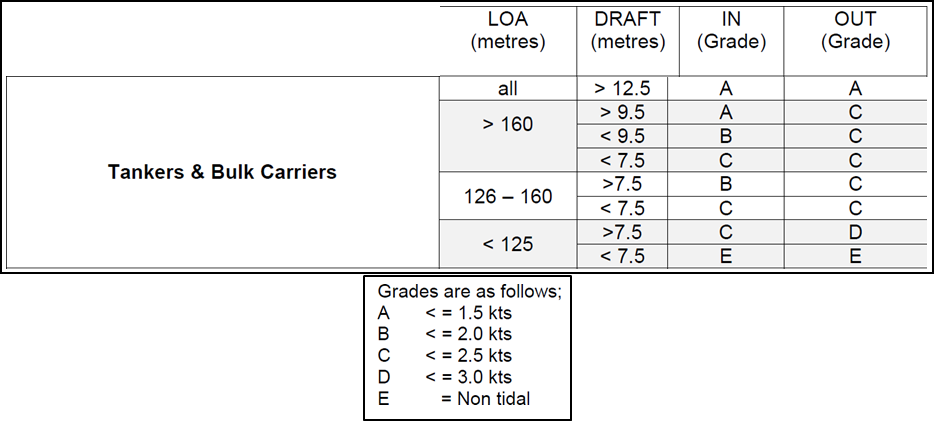
- The tidal stream can significantly affect the manoeuvring characteristics of large vessels. The standard operating procedures prescribed upper limits for the rate of tidal stream by using the vessel’s length and draught as key factors.
- The length of the Funing was greater than 160 metres and it had a draught greater than 9.5 metres and less than 12.5 metres. The corresponding prescribed upper limit for the rate of tide was less than or equal to 2.5 knots (see Figure 14).
- The Port of Tauranga provided a comprehensive passage plan for the port. Included as part of the plan were:
- a check of whether there were any deficiencies that might influence the passage plan
- a check of whether any main engine maintenance had been carried out while in the Port of Tauranga
- the environmental conditions expected for the pilotage passage.
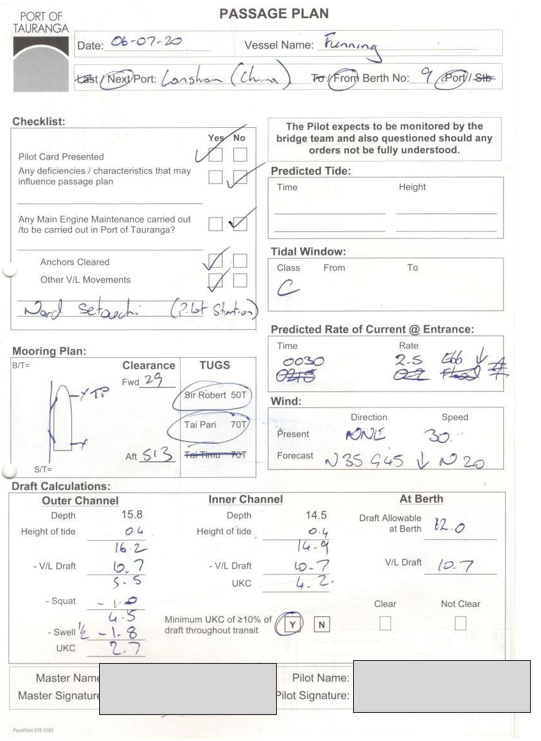
- Appendix 2 shows the Port of Tauranga passage plan completed for the departure of the Funing on the day of the accident. The pilot was expecting a wind of 35 knots gusting to 40 knots, and an ebb tide of 2.5 knots.
Testing the ICU
- During pre-departure checks of the main engine, a fault was identified on the injection quantity piston for number two engine cylinder, which had failed. It is very likely that the injection control valve was unable to move because it had become seized with coking debris that had entered the system and interfered with the operation of the valves.
- The same failure occurred again while the vessel was departing Tauranga.
- After the accident, when the vessel was laying at anchor, engineers replaced the ICU with a new unit. Replacing the ICU resolved the fault.
- The malfunctioning ICU was secured by the Transport Accident Investigation Commission (Commission), which then subjected it to forensic examination to determine the cause of failure.
- The Commission engaged two independent experts to conduct the forensic examinations of the ICU: Quest Integrity Ltd, which had expertise in metallurgy and forensic examination; and Det Norske Veritas, which had expertise in the Wärtsilä RT-Flex engine.
- The examination of the ICU was conducted at the Quest Integrity laboratory in Wellington, New Zealand. The draft report and its findings were discussed with a technical representative from Wärtsilä.
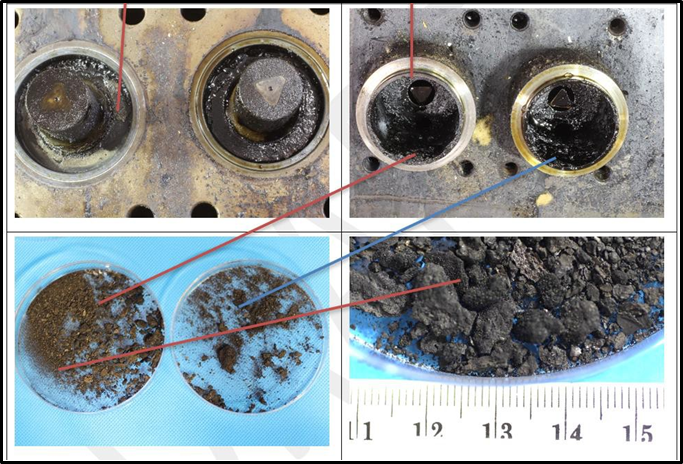
- The examination found that in the ICU the rail valves (see Figure 7, Item 5) were operational, and one of the two injection control valves had seized, very likely due to coking debris entering the system. Figure 15 shows the coking debris found in the cavity on the fuel oil side of the servo piston (see Figure 7, Item 15 labelled on the cross-sectional view of the ICU).
Analysis Tātaritanga
Introduction
- The Funing was a bulk carrier that could not generate enough propulsive power to overcome the prevailing adverse environmental conditions while under pilotage. As a result, the vessel lost control, deviated from the channel and became entangled in a channel marker buoy.
- It is virtually certain that the Funing’s main engine was unable to generate full power because a fuel ICU for number two engine cylinder was malfunctioning, and the cylinder was not firing.
- The environmental conditions were at the upper end of the allowable limits, which meant optimal engine power was required for the vessel to navigate the channel safely.
- Three safety issues were identified:
- ineffective communication between the master and chief engineer meant the master was not fully aware of the malfunctioning main engine prior to the vessel departing its berth
- the vessel’s main engine malfunction, combined with the prevailing environmental conditions, exceeded the safety considerations in the pilotage plan, and the vessel’s navigational control was rendered ineffective
- the introduction of low-sulphur fuel has had a significant effect on the performance of marine diesel engines. Although Wärtsilä had provided, in various documents, guidance on the effects of using low-sulphur fuels in its ICUs, this had not been fully integrated into the vessel’s safety management and planned maintenance systems.
Vessel departed the berth with a malfunctioning main engine
Safety issue: Ineffective communication between the master and chief engineer meant the master was not fully aware of the malfunctioning main engine prior to the vessel departing its berth.
- The chief engineer’s role on board the Funing included responsibility for the “maintenance and operation of all machinery on board”. In practice the chief engineer was responsible for managing all aspects of the engine room, and in particular ensuring that the main engine was fully operational before handing over control to the bridge.
- The bridge team had notified the engine room approximately two hours before the intended departure time, which was sufficient for them to complete all their pre-departure preparations and testing.
- About 28 minutes after commencing their preparations, the engineers tested the main engine ahead and astern and became aware of a malfunction with the ICU on the number two cylinder.
- They followed the trouble-shooting guidance provided by the engine manufacturer and attempted to rectify the problem four times. Each time the ICU on number two cylinder failed.
- The fourth test failed at 2342, which was 18 minutes before the planned departure. The engine room team had tried to rectify the fault using the information they had available to them on board the vessel. Although the chief engineer had already tried rebooting the number two cylinder control module and resetting the alarms, it was decided to try one more time.
- However, the engine was not tested again to confirm that it was functioning properly. The most recent test had shown that the main engine was malfunctioning.
- Given the safety management system requirement for the chief engineer to keep “the master informed of all matters related to the vessel’s machinery” (Funing’s safety management system manual), this was probably the last opportunity before departure to discuss the issue with the master.
- A few minutes later, at 2345, the chief engineer called the master on the bridge. During what was a brief conversation, the chief engineer told the master to cancel the automatic slowdown, but did not explain the reason for or the implications of doing so, specifically a likely reduction in propulsive power.
- The automatic slowdown feature of the main engine was designed to protect it from damage if it malfunctioned. If there were a risk of the main engine malfunctioning during a safety-critical passage or manoeuvre, the feature could be cancelled.
- It was rare to cancel the automatic slowdown, and the master had never used the feature previously. The request to cancel it was an indication that the chief engineer believed the main engine might malfunction. That the master had never used the function before was an opportunity to question the chief engineer’s request. By ascertaining the reason for cancelling the automatic slowdown the master may have discovered that the main engine was malfunctioning and the potential effects on the vessel’s manoeuvrability.
- However, the master complied with the chief engineer’s instruction to cancel the automatic slowdown without discussing the reason or the implications.
- As a result, the bridge team were unaware of the defect with the main engine and its implications, and consequently were unable to brief the pilot accordingly.
- The Commission identified two likely reasons for the bridge team being unaware of the main engine malfunction:
- the OOW observed the main engine turning ahead and astern during the pre-departure test
- the main engine defect and its implications were not clearly communicated between the engine room and bridge teams.
Crew resource management
- The key principle of BRM and ERM is that they use all available resources, including people, procedures and equipment, to provide safeguards against accidents created by human performance. The master and chief engineer had both been trained in BRM and ERM respectively.
- Although the bridge team demonstrated an effective use of closed-loop communication with respect to helm and engine orders during pilotage, there was a lack of departmental communication between the engine room and the bridge – specifically that the master and chief engineer did not maintain a clear and unambiguous line of communication. The requirements and benefits of good departmental communication had not been addressed in the safety management system.
- Had the master been made aware of the engine defect and its implications, the pilot could have been briefed accordingly. As a result both master and pilot would have been better able to make informed decisions on whether it was safe to depart as planned. The reality was that the master, unaware of the defect, believed his vessel would perform as designed in what were marginal environmental conditions.
- The Commission would have recommended to Thome Ship Management that it review the safety management system used on board the Funing to ensure that it incorporated the requirement for crews to communicate safety-critical information.
- However, as a result of the accident Thome Ship Management has already implemented changes to the safety management system to ensure that the master and chief engineer maintained full and clear communication. As a result, no recommendation had been made.
Vessel embarked on a pilotage passage in marginal environmental conditions
Safety issue: The vessel’s main engine malfunction, combined with the prevailing environmental conditions, exceeded the safety considerations in the pilotage plan, and the vessel’s navigational control was rendered ineffective.
- The manoeuvring characteristics of a vessel, and hence the control of the vessel are, in part, dependent on the rate of water flow past the rudder.
- The speed of the vessel is dependent on the main engine producing enough power to overcome the drag (a mechanical force that results from the interaction of a solid body with a fluid. Drag acts in opposition to the direction of the propelling force) of the vessel. The drag of a vessel is a combination of the characteristics of the hull in the water and the environmental conditions acting on the entire vessel, for example wind acting on the superstructure. An increase in wind speed and wave action will increase the drag of a vessel.
- The main engine was connected directly to the propeller, which in turn produced the water flow past the rudder. The relatively low power output produced by the main engine meant the propeller shaft revolutions could only increase as the vessel accelerated through the water. When the environmental conditions were adverse, it would take longer for the vessel to accelerate, and therefore the manoeuvring characteristics during this period would be reduced.
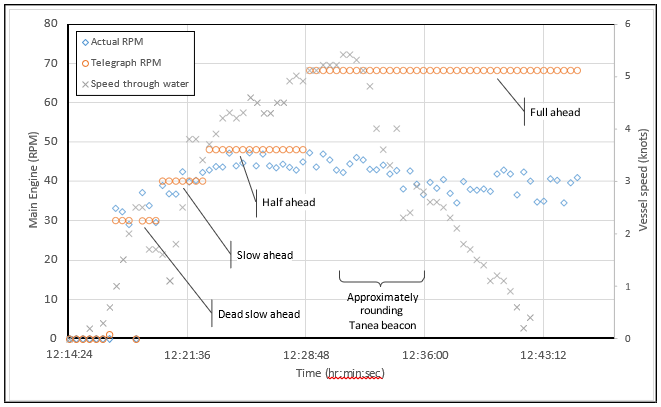
- Figure 16 shows the main engine rpm and vessel speed as the Funing departed Port of Tauranga. The X-axis shows the time. The left-hand Y-axis shows the engine rpm commanded by the telegraph, and the engine rpm as measured on the engine itself. The right-hand Y-axis shows the Funing’s speed through the water.
- It can be seen in Figure 16 that the telegraph showed the sequential bridge team commands from dead slow ahead to full ahead, but the actual rpm never consistently reached half ahead (48 rpm).
- Due to the reduced power of the malfunctioning main engine, the increased drag due to vessel speed and the adverse environmental conditions, the Funing did not consistently reach half ahead rpm when commanded by the telegraph.
- When the Funing rounded Tanea beacon it was more exposed to the head sea and wind. The combination of reduced main engine power and adverse environmental conditions further reduced the vessel’s rate of acceleration and its ability to increase speed. As a result, its manoeuvring characteristics were significantly diminished and ultimately overcome by the increasing environmental effect, and the vessel’s speed through the water was reduced to near zero knots.
Port of Tauranga safe operating procedures
- Port of Tauranga’s safe operating procedures (SOPs) included both preventive risk mitigation and recovery risk mitigation with respect to the pilotage service it offered.
- Preventive risk mitigation for safe pilotage included, but was not limited to, identifying risks to navigation and the vessel size- and type-specific upper limits for environmental conditions such as wind, tidal currents, wave and swell.
- Recovery risk mitigation included, but was not limited to, the use of tugs for vessels’ loss of power, and taking account of environmental conditions.
Port pilotage passage plan environmental conditions
- The environmental conditions at the time of the Funing’s departure, and described in the pilotage passage plan, were at the upper end of the allowable environmental limits described in Port of Tauranga’s safety management plan.
- Had the Funing’s main engine been able to produce full power, it is very likely the vessel would have completed the outbound pilotage without issue.
- In this case the unexpected lack of propulsive power due to the main engine malfunction had not been relayed to the pilot prior to departure.
- Although the risk mitigations in place did not seem unreasonable, the Commission would have made a recommendation to Port of Tauranga that it assess the allowable weather windows for pilotage and the ability of its tugs to mitigate the risk of a vessel losing power while under pilotage. However, it has already instituted changes to its SOPs that address both issues.
- The changes are:
- a reduction in upper wind limits for all vessels, from 40 knots to 30 knots
- a new SOP that mitigates the risk of high swell in the port’s outer channels
- the provision of vessel-type risk profiles regarding propulsion failure and the requirement for regular tug escorts for outgoing vessels.
Injection control unit malfunction
Safety issue: The introduction of low-sulphur fuel has had a significant effect on the performance of marine diesel engines. Although Wärtsilä had provided guidance, in various documents, on the effects of using low-sulphur fuels in its ICUs, this has not always been fully understood by end-users.
- The vessel was unable to increase speed because the power produced by the main engine was unable to overcome the vessel’s drag induced by environmental conditions.
- The primary reason for the vessel being unable to develop sufficient propulsive power was that number two cylinder of the main engine was not firing as a result of a malfunction of number two cylinder’s injection control unit. It is possible that other factors, such as hull fouling, propeller fouling (Hull/Propeller fouling can cause an engine to reach its maximum continuous rating before it reaches full RPMs. This condition is called heavy running of the fixed pitch propeller) and changes in the normal operating conditions of the vessel, further contributed to the main engine’s inability to generate sufficient propulsive power to manoeuvre the vessel safely.
- The malfunction of the ICU occurred prior to the vessel leaving the safety of its berth.
- Number two cylinder was malfunctioning because an injection control valve within the ICU was unable to move. This meant that the quantity piston was also unable to move properly, resulting in fuel not being properly injected into the cylinder, and the cylinder not firing.
- It is very likely that the injection control valve was unable to move because it had become seized with coking debris that had entered the system and interfered with the operation of the valves.
- As discussed in sections 2 and 3 of this report, the coking deposits within the ICU occurred because of fuel leakage. The leakage was likely a result of two things associated with low-sulphur fuels:
- increased wear of the ICU components
- low-viscosity fuel.
- There was evidence to indicate the engineers had been monitoring the condition of the ICU; for example, they had conducted monthly leakage measurements of each ICU. The magnitude of the leakage for number two ICU was recorded as between 1.74 and 2.07 litres per hour in a five-month period, as shown in Figure 17. These recorded leakage values can be considered minimal, representing values unlikely to lead to coking.
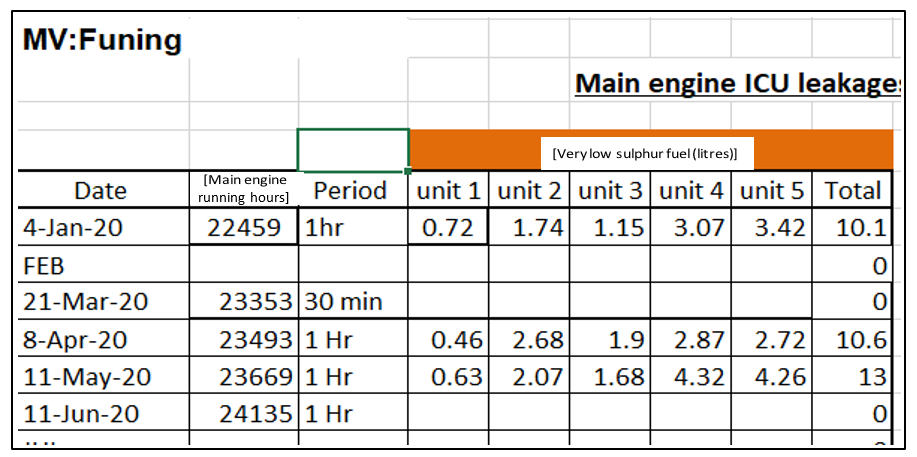
- As general guidance, Wärtsilä states that leakage rates of above 12 litres per hour while using low-sulphur fuel are an indication that the ICU is worn. When the Commission inspected the ICU, coking debris was found, which indicated excessive leakage. However, it is not clear why there was a disparity between the daily and monthly leakage measurements recorded on board and the coking found in the ICU.
- The ICU was a critical component of the vessel’s main engine, and its malfunction directly affected the safety of the vessel. Wärtsilä provided preventive risk-mitigation methods and recovery risk-mitigation methods. Preventive risk mitigation was provided by preventive maintenance, and recovery risk mitigation was provided by malfunction alarms and troubleshooting guidance.
- The engineers knew of the malfunction after being alerted by the various alarms and fault codes provided by the main engine monitoring system. They exhausted their understanding of the ICU troubleshooting guidance but were still unable to rectify the malfunctioning ICU.
Preventive maintenance
- Planned maintenance programmes are intended to rectify defects before they arise. By design, the onboard planned maintenance programme for the ICU was limited to basic lubrication and cleaning and monitoring certain performance metrics, in this case fuel leakage within the ICU.
- Wärtsilä required the ICU to be remanufactured at its service centre when the ICU had reached its lifetime running hours. The inspection and overhaul specification provided by Wärtsilä estimated the lifetime of the ICU at 36,000 service hours.
- Because the ICU had been designed to run effectively without significant onboard maintenance, the engineers relied on the estimated lifetime service hours and monitoring performance metrics to ensure the full function of the ICU.
- Although the ICU service lifetime was estimated at 36,000 hours, the ICU on number two cylinder had accumulated less than 25,000 hours before it malfunctioned.
Low-sulphur fuel
- The IMO had introduced a low-sulphur fuel cap in January 2020 for reasons of environmental protection. The change in fuel types and profile meant significant uncertainty for the maritime industry around the performance of ships’ engines.
- Wärtsilä had provided various documents, information and optional upgrades to end-users of its engines regarding the effects of low-sulphur fuel on Wärtsilä engines.
- In Wärtsilä’s business white paper of 2019 it stated that using high-sulphur fuels would result in engine components achieving estimated lifetime service hours, but that the efficiency or function of the engines’ fuel-injection components might be affected by using low-sulphur fuel. It also noted in its technical journal that, “Leakage and premature wear and tear on components are the biggest concerns when switching to low-sulphur fuel.”
- In this case the ICU malfunctioned far short of its estimated lifetime service hours, and this was very likely due to coking caused by oil leakage.
- During a meeting with the engine manufacturer and another meeting with ship managers to discuss the ICU malfunction, the Commission noted that Wärtsilä had produced a number of guidance notes on the subject of ICU performance and maintenance. However, on the vessel there was no single, comprehensive document available to the vessel’s engineers to address the effects of low-sulphur fuel on ICU maintenance. The guidance that had been provided by Wärtsilä to the vessel manager had not been fully integrated with the vessel’s safety management and planned maintenance systems.
- The switch to low-sulphur fuels across the marine industry brought significant uncertainty on how the new fuels would affect engine performance, maintenance and longevity. Wärtsilä has provided guidance on monitoring fuel leakage, analysing engine monitoring software, the potential effects of using low-sulphur fuels, and upgrading ICU parts. However, the information is located in various documents and is not always available to, or fully understood by, end-users. See Appendix 3 for a list of those documents.
- The Commission has made a recommendation to Wärtsilä that it take further steps to ensure that users of its RT-Flex engines can easily locate and assimilate all information regarding the effects of the IMO sulphur cap on ICU performance, maintenance and lifetime service.
Appendix 1. Thome Ship Management Pte. Ltd. pilot card
Appendix 2. Port of Tauranga passage plan
Appendix 3. Summary of Wärtsilä documents providing guidance on ICU maintenance that were available to the Commission