Bulk carrier & commercial fishing boat collided in good visibility night conditions. No substantial damage, no serious injuries or fatalities. Those operating each vessel, aware of the other, acted too late. Neither made best use of radar. Bulk carrier bridge team distracted by passengers. Fishing boat watchkeeper should have known more about collision-prevention rules.
Executive summary Tuhinga whakarāpopoto


What happened
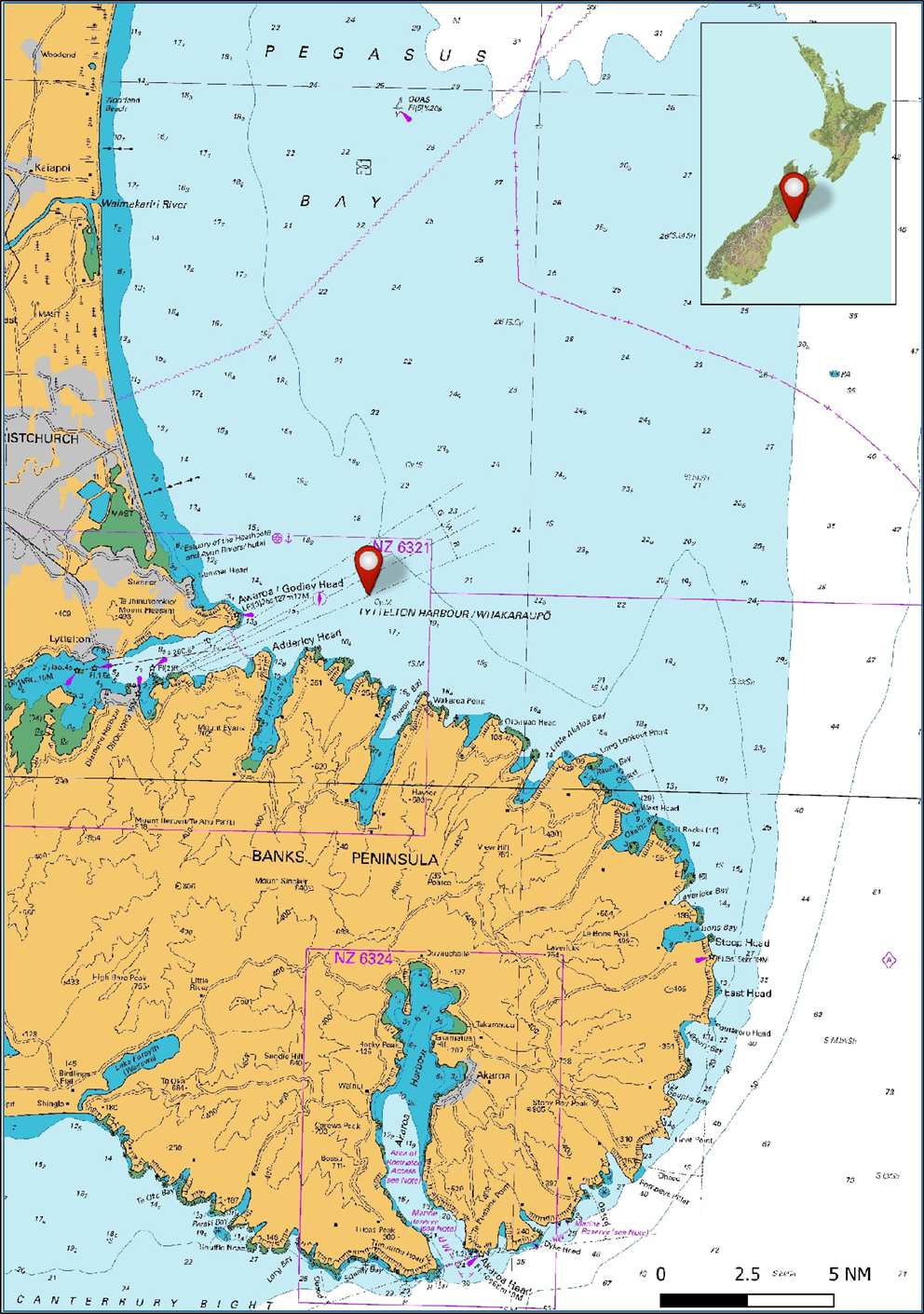
- On the evening of 12 January 2020 the visibility in Whakaraupō/Lyttelton Harbour was good, there was a light south-westerly wind of just under 10 knots and the tidal stream was negligible. The sun had set at 2112 hours. The bulk carrier Rose Harmony was outbound from Lyttelton. It had just disembarked a pilot and was coming up to speed for its intended passage to Dunedin. The Rose Harmony was carrying passengers from the vessel’s charterer; they were on the bridge at the time of the accident.
- The fishing vessel Leila Jo was heading to its home port of Lyttelton after fishing in Pegasus Bay. The skipper was resting at the time of the accident and a deckhand was keeping the navigational watch.
- The vessels were in a head-on situation, which required both to alter course to starboard to avoid a collision. The third officer on the Rose Harmony observed the Leila Jo when it was more than three nautical miles (5.6 kilometres) away. The deckhand on the Leila Jo had sighted a vessel leaving Lyttelton on the vessel’s radar but had not tracked the target or observed it with binoculars.
- Neither vessel took early and substantial action to avoid a collision, and at 2259 they collided.
- Neither vessel was substantially damaged. One person on the Leila Jo received minor injuries.
Why it happened
- The bridge team on board the Rose Harmony, both during and immediately after the pilotage ended, had a low situational awareness of other marine traffic in the vicinity.
- Distraction due to passengers being on the Rose Harmony bridge, the crew not making best use of radar equipment, and the absence of long-range scanning to obtain early warning of the risk of collision, were significant factors.
- The sole watchkeeper on board the Leila Jo had low situational awareness as to the risk of collision with the Rose Harmony because the radar equipment was not used to plot the track of the Rose Harmony.
- The watchkeeper on board the Leila Jo was not sufficiently familiar with the collision-prevention rules to undertake a sole watch.
What we can learn
- The collision-prevention rules provide the mandated standard to be followed by all vessels at sea to prevent collisions of two or more vessels. The risk of collisions will inevitably be high if the rules are not adhered to by one or more vessels.
- Navigating in pilotage waters is a safety-critical phase of a voyage. It is important that all unnecessary distractions are mitigated during these times, particularly the presence of people on the bridge who are not essential to its operation.
-
If collisions between vessels are to be avoided, anyone undertaking a sole bridge watch must be sufficiently trained in the collision-prevention rules and be fully familiar with the bridge equipment at their disposal. The collision-prevention rule 7, Risk of Collision (the rule is given effect in New Zealand by Maritime Rules Part 22.7: Risk of Collison) states:
(1) Every vessel must use all available means appropriate to the prevailing circumstances and conditions to determine if the risk of collision exists. If there is any doubt, such risk must be considered to exist.
Who may benefit
- Vessel owners and operators, owners and operators of fishing vessels, and watchkeepers on board any type of vessel may all benefit from the information in this report.
Factual information Pārongo pono
Background
- The 23.89-metre fishing trawler Leila Jo was built in Australia in 2000 as a fish-farm support vessel. The Leila Jo was purchased by Pegasus Fishing Limited, a Lyttelton-based fishing company, in 2017, and converted to a stern trawler. The vessel entered Part B (Part B registration is mainly for recreational and fishing vessels that require nationality for overseas voyages) of the New Zealand vessel registry in December 2017.
- The Rose Harmony was a 179.99-metre geared (capable of loading and discharging using the vessel’s own cargo-handling equipment) bulk carrier time chartered to import fertilizer from China to New Zealand and export logs to China on return voyages. The Liberian-registered vessel was operated by Union Marine Management Services Pte. Limited, based in Singapore.
Narrative
- On the evening of 12 January 2020 the visibility in Whakaraupō/Lyttelton Harbour was good (more than five nautical miles [NM]). There was a light south-westerly wind of just under 10 knots. The tidal stream was negligible. The significant wave height (the mean wave height of the highest third of waves) timed for 2200 near the area of the accident was 1.34 metres and the moon was in its waning crescent phase (20% of the moon was visible).
- The Leila Jo had left Lyttelton around 0300 on 11 January 2020 with four crew and the skipper on board.
- The Leila Jo had been fishing in Pegasus Bay, 23 NM off the North Canterbury coast. At about 2030 on 12 January 2020, the crew of the Leila Jo had hauled in their final catch of the day and set a course for Lyttelton. The deckhand was keeping the watch alone in the wheelhouse. The watchkeeping alarm was switched on.
- On the same evening, 12 January 2020, the Rose Harmony had completed discharging 10,500 metric tonnes of fertilizer in Lyttelton. At about 2205 the vessel departed from its berth with a harbour pilot on board. The bridge team comprised the pilot, master, third officer and helmsman. The pilot had the conduct (controlling the speed and direction of the vessel) of the vessel and the third officer was the officer of the watch.
- Also on the bridge were three passengers who were representatives of the charterer of the vessel. They were making an observation trip to the next port of Dunedin.
On board the Leila Jo
Times for the Leila Jo were gathered from interviews of the Leila Jo crew and positions gained from downloads of the boat’s chart-plotting systems.
- The skipper of the Leila Jo had set a waypoint in the vessel’s chart plotter for just off the harbour entrance, and told the deckhand to keep a watch and wake the skipper when the vessel was 10 minutes from the waypoint.
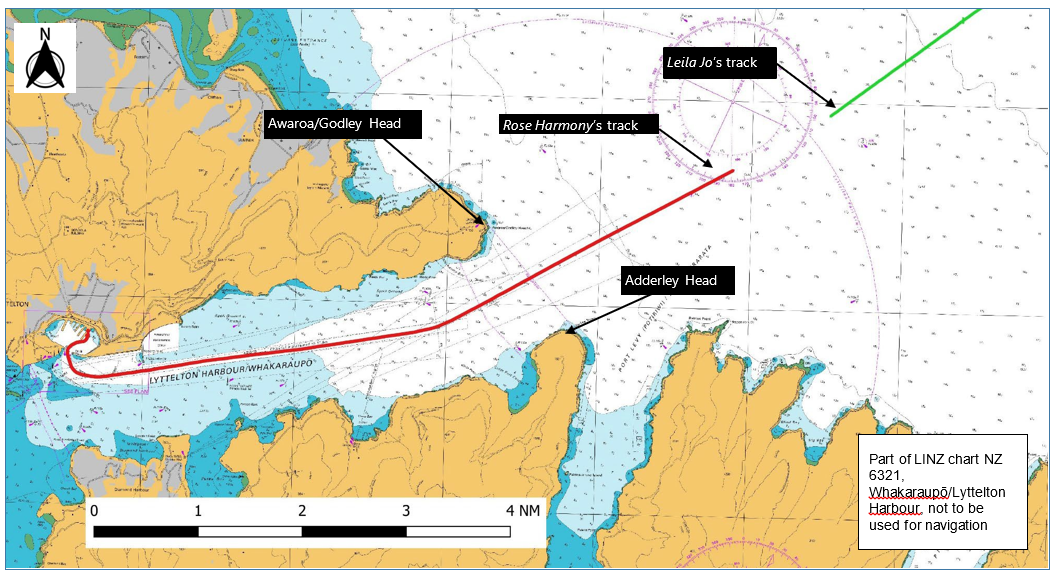
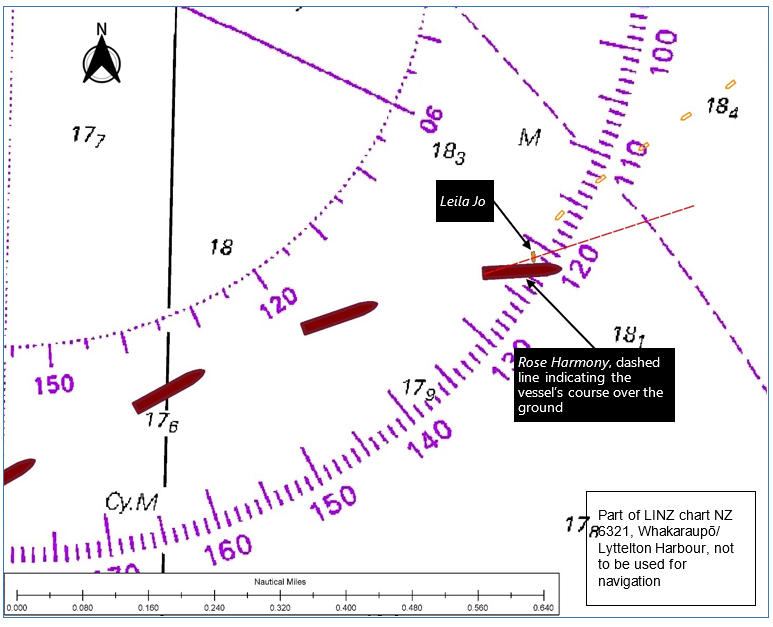
- The deckhand remembered seeing a radar target between Awaroa/Godley Head and Adderley Head at the entrance to Whakaraupō/Lyttelton Harbour (see Figure 3) at about 2240. The deckhand had not observed the target visually and had not identified the direction in which it was heading. This radar target was almost certainly the Rose Harmony leaving Whakaraupō/Lyttelton Harbour and may have been visually detectable.
- At about 2248 the deckhand left the wheelhouse to wake-up the skipper, he then stopped to make some food before returning to the wheelhouse with the skipper.
- As the skipper and deckhand were climbing the steps to the wheelhouse they heard the Rose Harmony’s whistle and rushed to the door on the port side of the wheelhouse. Looking up, the skipper saw the Rose Harmony’s port navigation light close above them. The skipper of the Leila Jo attempted to steer the vessel to starboard using the controls nearest to the port side door, but the autopilot was still engaged. The skipper called for the deckhand to take the autopilot out of automatic mode. Shortly afterwards the Leila Jo turned to port and the two vessels collided (see Figure 6).
On board the Rose Harmony
All times and positions reported for the Rose Harmony were gained from the Rose Harmony’s voyage data recorder.
- The pilot boarded the Rose Harmony at 2143 and exchanged information with the master. The vessel departed Lyttelton Port at about 2205 and proceeded outbound along the Whakaraupō/Lyttelton Harbour channel. The pilot had the conduct of the vessel. The vessel’s two radars (The Rose Harmony was fitted with a voyage data recorder, which recorded the status of the radars and other navigation equipment and provided an audio recording of events and conversations on the bridge) were set to 3 NM and 0.75 NM ranges respectively and remained so for the entire pilotage (the process of directing the movements of a ship by visual and/or electronic observations of recognisable landmarks and navigation marks).
- As the vessel was transiting Whakaraupō/Lyttelton Harbour, the pilot had the conuct of the vessel and was at times conversing with the three passengers on the bridge.
- The third officer and the master were monitoring the progress of the ship and the status of the various ship systems.
- At about 2240 in the vicinity of Awaroa/Godley Head, in preparation for their disembarking onto the pilot boat, the pilot handed the conduct of the vessel to the master. The radars remained on their respective three and 0.75 NM range scales. The pilot informed the master of the vessel’s current speed and course in a brief handover, During the handover there was no discussion about traffic in the area, as the bridge team had not noticed the presence of the Leila Jo some 5 NM ahead of the vessel.
- The third officer accompanied the pilot down onto the main deck and watched as the pilot descended the pilot ladder onto the pilot launch. The third officer then returned to the bridge at 2245.
- The master was in discussion with the three passengers, so the third officer began familiarising themselves with the vessel’s situation.
- At about 2248 the third officer observed a small vessel fine on the port bow of the Rose Harmony. When the third officer viewed the vessel through binoculars, both the port and the starboard navigation lights were visible. The third officer informed the master of the small vessel’s presence.
- At this point the Leila Jo was approximately 3.5 NM away, but it was not yet visible on the radars because they were still set on the three and 0.75 NM range scales. The speed of the Leila Jo was about 7.8 knots over the ground and the speed of the Rose Harmony was 8.2 knots over the ground, giving a closing speed of about 16 knots.
- As the Rose Harmony was by then clear of the channel, the master ordered the engine speed to be increased, giving a new speed of about 11.8 knots over the ground. The helmsman was still steering the vessel manually.
- At 2251 the third officer interrupted the discussion between the master and the passengers to inform the master of the developing situation with the Leila Jo. The master acknowledged the third officer and continued the conversation with the passengers.
- At 2254 the passengers and the master were discussing the electronic chart display information system. The Leila Jo was 1.5 NM away; neither vessel had altered course.
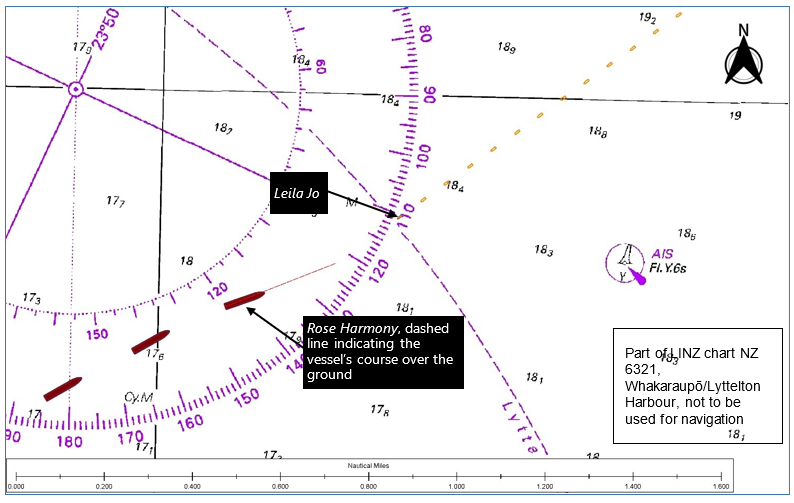
- At 2256 the third officer informed the master that the Leila Jo’s closest point of approach would be 0.047 NM.
- At 2258 the third officer informed the master that the fishing vessel’s course over the ground was 230°. The master first confirmed with the helmsman that the Rose Harmony was on a course of 060°, then ordered the helmsman to alter course 10° to starboard to avoid a collision.
- At 2258.30 the third officer informed the master that the bow crossing range was 0.089 NM. At this point the master ordered hard starboard and sounded one continuous long blast on the vessel’s whistle.
- At 2259 the Leila Jo and the Rose Harmony collided.
Post-collision actions
- The Leila Jo’s crew mustered and gathered lifejackets and started to prepare their life raft. The crew then carried out a damage assessment. The crew found there was no significant damage to the boat. The bow of the Leila Jo was damaged, but the crew found no ingress of water or fuel egress.
- The crew of the Rose Harmony contacted the Leila Jo via very high frequency (VHF) radio. They asked if there were any injuries to people on board the fishing vessel and offered assistance.
- Meanwhile the pilot launch had just returned the Rose Harmony’s pilot to the port. The pilot launch crew overheard the VHF conversation. The skipper of the pilot launch set out to offer assistance to the Leila Jo.
- At about 2333 the pilot launch arrived at the scene of the collision. The skipper of the Leila Jo confirmed they needed no assistance. The pilot launch stayed with the Leila Jo as it resumed its voyage to Lyttelton until about 2243, when the pilot launch left the Leila Jo to proceed to return to the port.
- The Rose Harmony remained off the port until receiving confirmation that the Leila Jo had reached Lyttelton safely. After consulting Lyttelton Port Radio, the Rose Harmony resumed its passage to Dunedin.
Post-collision consequences
- Following the collision the Leila Jo was surveyed by a marine engineer, who assessed the vessel as “having cosmetic damage and had not lost watertight integrity” (capable of preventing the passage of water through the structure under a head of water for which the surrounding structure is designed). The engineer also stated there was no need to take the vessel out of service.

- The Rose Harmony’s hull was surveyed by a classification society surveyor, who found some indentations to a ballast tank on the port side of the vessel. The surveyor recommended that the indentations be repaired before April 2020. The surveyor did not impose any conditions that would prevent the Rose Harmony sailing from Dunedin.
- Nobody on board the Rose Harmony was injured. The skipper of the Leila Jo received minor injuries resulting from a fall when the two vessels collided. The skipper spent a night in hospital under observation.
Navigation equipment
- The Leila Jo was fitted with a Furuno 1945 radar, which was equipped with an automatic radar plotting aid (ARPA). This feature meant the radar could acquire targets and provide tracking and anti-collision information. The Furuno unit was interfaced with a desktop computer that was running SeaPlotPro, a chart plotting software designed specifically for fishing vessels.
- The Leila Jo was fitted with a Robertson AP35 autopilot, which could maintain a course by automatically making alterations to the rudder. Course alterations under autopilot mode could be made either incrementally, by repeatedly pushing port or starboard buttons, or more rapidly by rotating a course command knob (see Figure 8). A disengagement of the autopilot (as performed by the standby button) transferred the control to manual steering.

- The Rose Harmony was equipped with two Furuno ARPAs, one S band (three gigahertz) and one X band (10 gigahertz). Both radars were fitted with the ARPA function. The vessel was also equipped with two TOKYO KEIKI electronic chart display information systems, one planning and one monitoring unit.
Analysis Tātaritanga
Introduction
- Notwithstanding the relatively minor damage and injuries resulting from this accident, collisions between large vessels and smaller fishing vessels can be catastrophic. Worldwide over many years there have been many fatalities resulting from such collisions. The Transport Accident Investigation Commission (Commission) has investigated one such case, a collision in 1996 between the container vessel Sydney Express and the fishing vessel Maria Luisa at the entrance to Wellington Harbour.
- The Sydney Express was outbound from Wellington and the Maria Luisa was inbound when the two vessels collided, with a loss of five lives (Transport Accident Investigation Commission Report 96-214, Collision between the container vessel Sydney Express and the fishing trawler Maria Luisa, Wellington Heads, 29 December 1996)
The collision regulations
- The International Regulations for Preventing Collisions at Sea, known as the COLREGs, were introduced by the International Maritime Organization in 1972. The COLREGs set out, among other things, the ‘rules of the road’ or navigation rules to be followed by vessels and other vessels at sea to prevent collisions between two or more vessels. The COLREGs are derived from a multilateral treaty called the Convention on the International Regulations for Preventing Collisions at Sea.
- The COLREGs have been given effect in New Zealand through Maritime Rules Part 22: Collision Prevention.
- This collision occurred in open waters where no other special rules applied. Fishing vessels that are engaged in fishing have special considerations under Maritime Rules Part 22. However, the Leila Jo was not engaged in fishing. Therefore, both the Rose Harmony and the Leila Jo were defined as power-driven vessels under way. Neither had right of way over the other based on size or manoeuvrability alone.
- The COLREGs required both vessels to “use all available means appropriate to the prevailing circumstances and conditions to determine if the risk of collision exists. If there is any doubt, such risk must be considered to exist” (Maritime Rules Part 22.7(1)).
- The COLREGs also required that, for both vessels, “proper use must be made of radar equipment, if fitted and operational, including long-range scanning to obtain early warning of the risk of collision and radar plotting or equivalent systematic observation of detected objects” (Maritime Rules Part 22.7(2)).
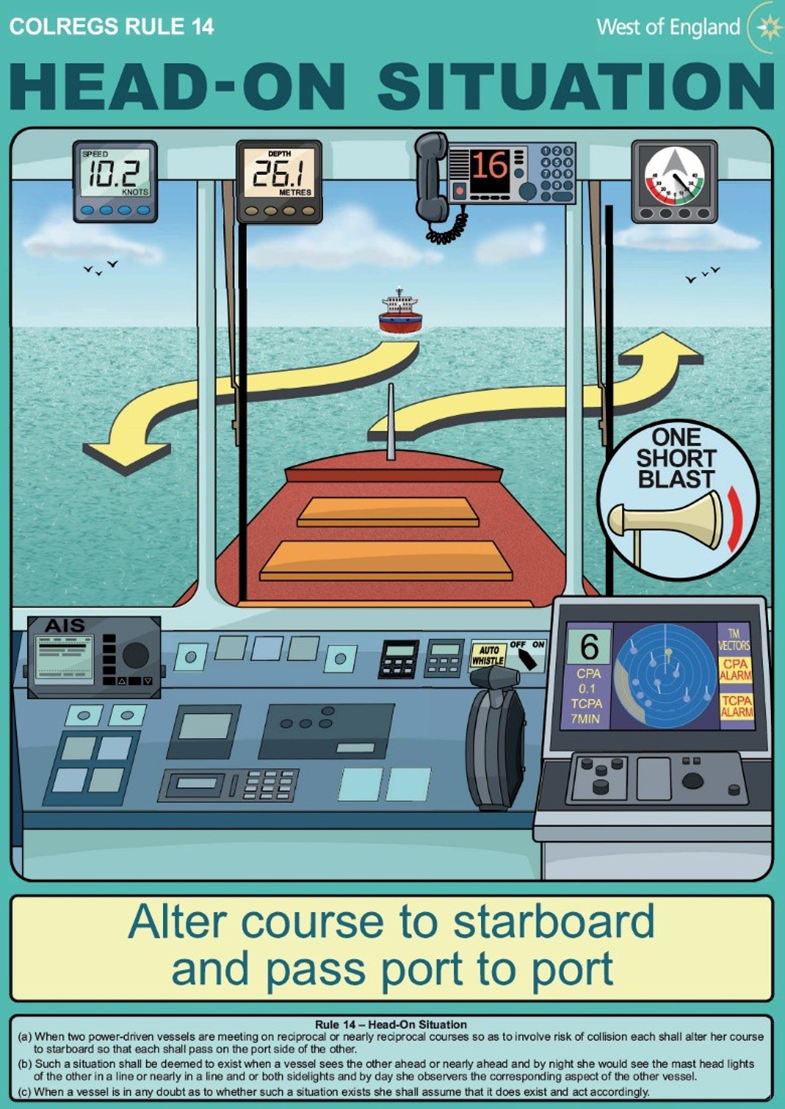
- The Leila Jo and the Rose Harmony were in what is described in COLREGs Rule 14 as a “head-on situation” (such a situation will be considered to exist when a vessel sees the other ahead or nearly ahead and by night, the masthead lights of the other vessel are in line or nearly in line and/or both sidelights are visible (Maritime Rules Part 22.14.2(a))), and because they were two power-driven vessels meeting on reciprocal or nearly reciprocal courses so as to involve a risk of collision, each had to alter course to starboard so that each passed on the port side of the other (Maritime Rules Part 22.14(1)) (see Figure 9).
- The meeting of these two vessels was not a complex situation. Each vessel was equipped with appropriate radar equipment capable of detecting the other and there was ample sea room for each to manoeuvre as required by the rules.
- If the collision regulations had been followed, each would have detected the other in sufficient time to have recognised that a risk of collision was developing or existed and altered their course to starboard early enough to pass safely on each other’s port side. The following analysis considers why the crew of each vessel did not take appropriate action.
The Rose Harmony
Safety issue: The situational awareness of the bridge team on the Rose Harmony was adversely affected by poor bridge resource management, exacerbated by the presence and distracting influence of passengers on the bridge in pilotage waters.
- The fundamental aspects of watchkeeping – position monitoring, collision avoidance and maintaining situational awareness – apply as much to vessels under pilotage as they do to keeping watch on a coastal route. Situational awareness is more than just knowing where a vessel is. It involves the entire bridge team (crew and pilot) working together to ensure all are aware of all factors that are affecting the vessel or are likely to affect it in the immediate future, including the presence of other traffic.
- The bridge team in this case appeared to have been caught up in the ‘moment of time’ rather than looking ahead at the emerging threats to the vessel. It is about as likely as not that distraction occurred to some degree through their engaging in conversation with the passengers.
- Both radars were set on short range for the entire pilotage. It is very likely that the Leila Jo would have been visible by radar much earlier had the range scale been cycled out to 6 NM or more. The pilot was not aware of the fishing vessel’s presence. Consequently, there was no mention of it when the pilot handed the conduct of the vessel to the master. At that time the Leila Jo was an emerging collision risk, less than 5 NM ahead with a closing speed of about 16 knots and rising as the vessel’s speed increased after disembarking the pilot.
- With the pilot gone and the master having accepted the conduct of the vessel, it would have been good practice for the master to be assessing the vessel’s position and monitoring for other traffic in preparation for handing the conduct to the third officer once the pilot had disembarked. Instead, the master was almost certainly distracted by the presence of the passengers on the bridge.
- When the third officer returned to the bridge and began to look ahead, they saw the lights of the Leila Jo, yet it was not until the Leila Jo appeared on the 3 NM radar range that the third officer began plotting its progress. Once plotting started the third officer realised the threat, and was heard on the voyage data recorder audio recording attempting to engage the master on five occasions.
- The master’s action of altering the Rose Harmony’s course 10 degrees to starboard likely put the two vessels on a collision course. Prior to that the Leila Jo had been tracking to pass marginally down the vessel’s starboard side at its closest point of approach, as described by the third officer.
- When the master ordered the helm to be put hard over to starboard, the correct sound signal to have made on the vessel’s whistle was one short blast, which would have been the signal for letting the Leila Jo know that “I am altering my course to starboard” (Maritime Rules Part 22.34(a)). However, the master made one long continuous blast.
- The International Chamber of Shipping’s Bridge Procedures Guide describes an effective bridge team as one that “will manage efficiently all the resources that are available and promote good communication and teamwork”. This is particularly important during an emergency situation when an effective response will depend on good communication and co-ordinated actions.
- Good communication is a cornerstone of bridge resource management. One known barrier to good communication is what is commonly referred to as a power-distance relationship, typically when a subordinate is required to challenge a superior, in this case the third officer challenging the master.
- One technique to overcome a power-distance relationship is the use of graded assertiveness communication. Communication escalates from probing to alerting to challenging, and eventually to emergency. The third officer was heard probing and alerting the master to the situation on the voyage data recorder’s audio recording, but did not take it to the next level of challenge or emergency. When it was obvious to the third officer that the master was not engaged with the threat, the correct thing for the third officer to have done would have been to suggest that they, or ask permission to, take earlier and more substantial action to avoid the collision. Finally, the third officer could have overridden the master’s conduct of the vessel and taken the required action.
-
The passengers being on the bridge during the pilotage was problematic. Their presence affected the bridge team’s ability to manage the conduct of the vessel effectively. The operator of the Rose Harmony had included guidance in its safety management system to mitigate the risk of distraction to the bridge team. The guidance included this paragraph:
Entry of personnel to the bridge shall be controlled so that no person who is not directly related to the operation on the bridge & its equipment, navigational duties, command centre duties in case of emergencies or to address urgent matters related to vessel operations can affect the alertness or focus of the bridge team.
- This statement did not prevent passengers being on the bridge, but it was clear in its intent that passengers’ presence should not adversely affect the bridge team performance at times of critical navigation.
- Distraction by non-essential personnel on the bridge of a vessel is not a new problem. The International Maritime Organization conducted a review of passenger vessel operations following the capsize of the cruise ship Costa Concordia. It published the document Maritime Safety Committee 92/6 (MSC 92/6) Review of Operational Safety Measures to Enhance the Safety of Passenger Ships (submitted by the International Chamber of Shipping). This document includes a section defined as “Access of Personnel to the Navigating Bridge and Avoiding Distraction” (see Appendix 1).
- The Commission raised distraction as a concern in its report on the near grounding in 2004 of the Cook Strait passenger ferry Aratere while transiting the entrance to Tory Channel (Transport Accident Investigation Commission Report 04-214, Passenger freight ferry Aratere, loss of mode awareness leading to near grounding, Tory Channel, 29 September 2004). The presence of passengers on the bridge leading up to the critical turn may have distracted the master and the officer of the watch.
The Leila Jo
Safety issue: The deckhand keeping watch on board the Leila Jo was not sufficiently familiar with the collision-prevention rules to be left in sole charge of the watch.
- The deckhand who was keeping a navigational watch had been recruited and trained by the Leila Jo’s skipper. Previously they had both been working on another fishing vessel in the fleet in similar capacities, and had been working for Pegasus Fishing for a total of 12 years.
- The deck crews usually kept two-hour watches while the skipper was resting, with instructions to wake the skipper when needed.
- The operator had a fatigue-management plan that included advice such as considering having two crew on watch, shortening the watch periods and using the wheelhouse watchkeeping alarm.
- It is unlikely that the deckhand fell asleep during the watch or that fatigue was a factor. The wheelhouse watchkeeping alarm was active and would have alarmed if the deckhand were not moving. The deckhand was sufficiently alert to notice the presence of the Rose Harmony on the radar.
- However, the deckhand did not take the actions required by Maritime Rules Part 22. Having detected the presence of the Rose Harmony, they made no attempt to plot the vessel to determine if there was a risk of collision. The deckhand, unaware of the developing close quarter situation, left the wheelhouse to wake up the master and prepare food, thereby leaving the wheelhouse unmanned.
- It was not until the skipper and deckhand arrived in the wheelhouse moments before the collision that some kind of action was attempted. Data from the Leila Jo’s chart plotter showed the vessel turned to port just before the collision occurred. The skipper’s intention was to turn to starboard. Why the fishing vessel turned to port could not be established with any certainty. The Leila Jo was in automatic steering at the time, which the skipper had asked the deckhand to disengage.
Crew training and certification on board the Leila Jo
- The Leila Jo was under 24 metres in length. Under Maritime Rules Part 31: Crewing and Watchkeeping the minimum manning requirement was a certified skipper and an engineer. In this case the skipper was certified as both skipper and engineer. The skipper was the only person on the vessel who had received formal training from an approved training provider for keeping a navigational watch.
- Maritime Rules Part 31 (Maritime Rules Part 31.85 : Fishing vessels within the inshore fishing limits or fishing vessels <24m in length beyond inshore fishing limits but within coastal or offshore limits) states that the “owner and master of the ship and any person engaged in navigational watch keeping duties on the ship must take account of the standards for navigational watch keeping”, which are defined in the International Convention on Standards of Training, Certification and Watchkeeping for Fishing Vessel Personnel (STCW-F) (Chapter IV of STCW-F describes the suitable arrangements of a navigational watch and states that a lookout must be maintained in compliance with the COLREGs).
- The owner of the Leila Jo (Pegasus Fishing) also operated four other fishing vessels. It was common practice for skippers to be the only certified watchkeepers when the vessels were going on trips for multiple days. When it was necessary for the skipper of a vessel to rest, a deckhand was required to keep the navigation watch.
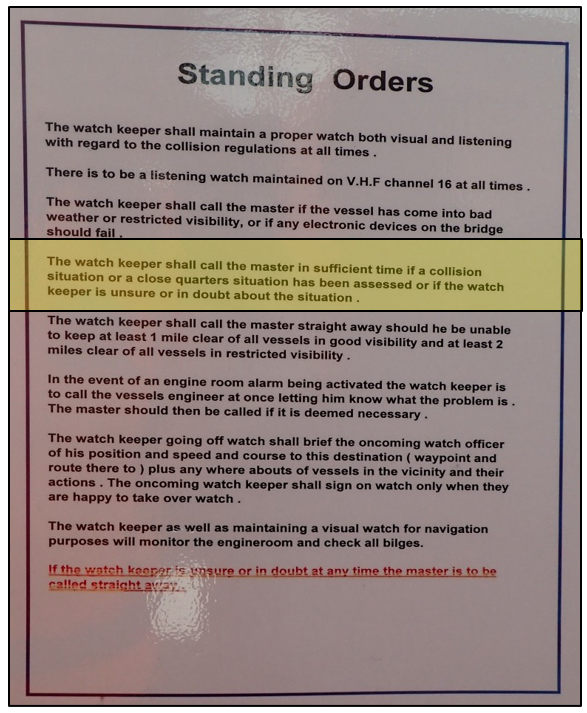
- On board the Leila Jo the deckhands knew that if they were unsure about anything when they were keeping a navigational watch, they were to wake the skipper immediately. This was defined in the vessel’s Standing Orders, which were posted in the wheelhouse (see Figure 10).
- The training and recruitment of deckhands on the vessels in the Pegasus Fishing fleet was the responsibility of the skipper. The training for working as a deckhand was overseen by an experienced deckhand. New recruits would also spend time working alongside the skipper in the wheelhouse, learning how to keep a navigational watch and how to handle the boat.
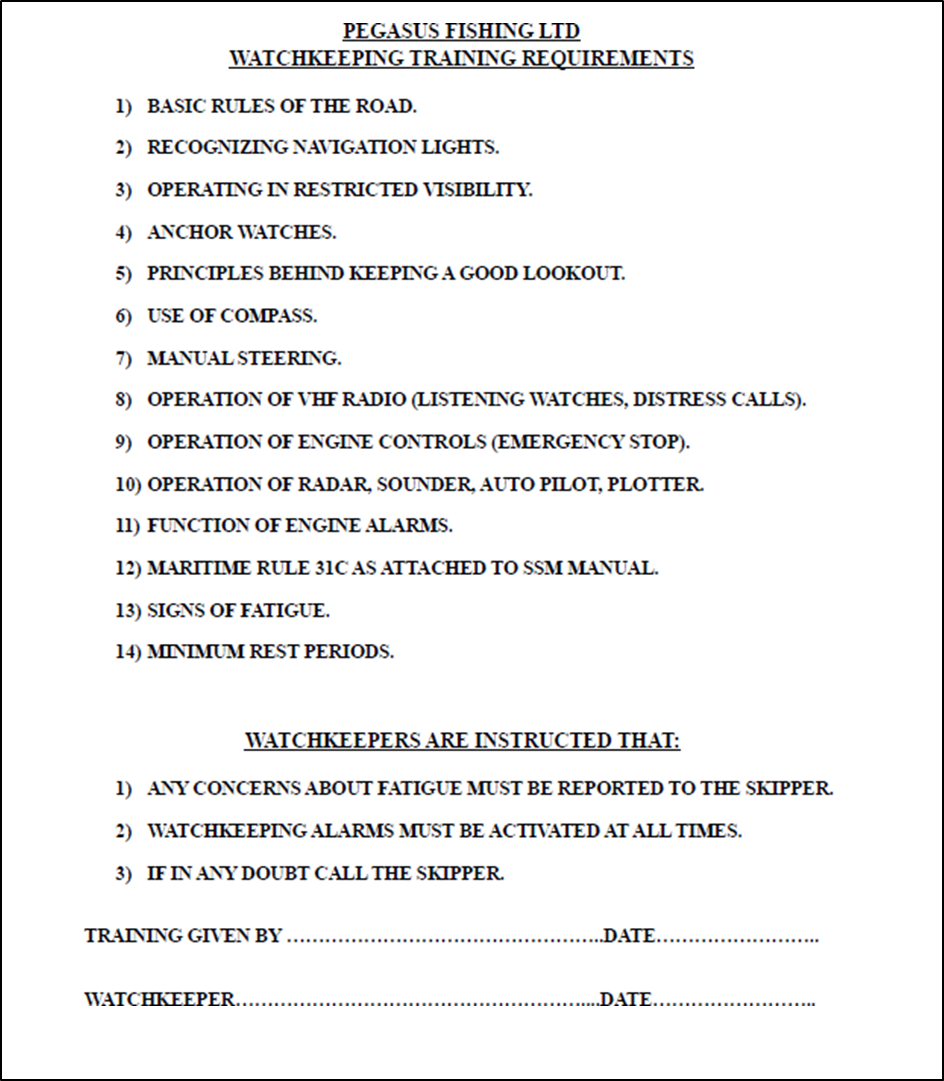
- Pegasus Fishing had a ‘Watchkeeping Training Requirements’ checklist that deckhands had to complete. The checklist was signed off by the skipper after they were satisfied that a deckhand was sufficiently trained to keep navigational watch (see Appendix 2 for a copy of the ‘watch keeping training requirements’ checklist). This on-the-job training usually lasted about one week. After a deckhand completed watchkeeping training, they would be rostered on with the other deckhands to keep watch when the skipper was resting.
- The deckhand who was in the wheelhouse at the time of the accident had completed the watchkeeping training requirements set out in the company checklist and had been signed off by the skipper. However, they were not completely familiar with the COLREGs and did not appreciate the risk that the Rose Harmony posed.
- A system whereby deckhands are only trained in watchkeeping to a level where the skipper is called in sufficient time when a collision or close-quarters situation exists is not consistent with the requirements of Maritime Rules Part 31, which requires owners, skippers and watchkeepers to take account of the standards of STCW-F. This training system was designed to allow skippers to rest; however, watchkeepers would have to wake skippers whenever they were uncertain, limiting the amount of rest the skippers could get.
- The Commission has recommended that the owner enhance its training system so as to upskill deckhands in watchkeeping practices that meets the minimum requirements of Maritime Rules Part 31 and adequately reduces the risk of accidents and incidents resulting from poor watchkeeping practices.
- The Commission has also recommended that Maritime New Zealand, when assessing or auditing Maritime Operator Safety Systems for fishing vessels, review the adequacy of watchkeeping training programmes for upskilling unqualified deckhands to a level that meets good industry practice and complies with the requirements of Maritime Rules Part 31.
Appendix 1. International Maritime Organization MO MSC 92/6/XX2013
PASSENGER SHIP SAFETY
Review of Operational Safety Measures to Enhance the Safety of Passenger Ships Submitted by ICS
Introduction
1. In response to the outcomes of MSC 90 and MSC 91 ICS recommended that member passenger ship operating companies conduct a review of operational safety measures. The recommendations provided at annex to MSC.1/Circ.1446 and the further recommendations within MSC.1/Circ.1446/Rev.1 were used as a basis for the review, however, additional aspects of passenger ship vessel operations were also considered and enhancements and best practice reported.
2. Recognising that the SOLAS definition of a passenger ship is “a ship which carries more than twelve passengers”, this submission reports on reviews by companies operating different types of passenger ships, including Ro-Ro Passenger ships and High Speed Craft and is not part of the Cruise Industry Operational Safety Review reported by CLIA in MSC 92/6/1.
3. The results of the reviews conducted by companies are summarised below and recommendations are made in some cases as a direct result of findings from the reviews. In addition, companies reported on other policies and procedures that they reviewed after the Costa Concordia accident.
Lifejackets on board Passenger Ships, except Ro-Ro Passenger Ships
4. Taking into account that the recommendation in MSC.1/Circ.1446 for companies to consider additional lifejackets was explicitly not applicable to Ro-Ro Passenger ships, these operators conducted a review to ensure that the location and accessibility of the additional lifejackets required by SOLAS were appropriate.
5. One issue identified, now rectified, was the absence of suitable signage for oversized lifejackets or lifejacket accessories to ensure compliance with the requirements of SOLAS Chapter III Regulation 7.2.1.5.
6. The distribution of lifejacket sizes was also considered for each assembly station to ensure accessibility, and that an appropriate number of oversized lifejackets or accessories to ensure compliance with SOLAS III/7.2.1.5, adult, child and infant lifejackets were available at each assembly station.
Recommendations
7. SOLAS specifies carriage requirements for lifejackets, however, there is no existing requirement or guidance for the location and distribution ratios for the different types of lifejackets. It is therefore recommended that guidance is developed on issues to consider when determining the distribution of lifejackets in each assembly station. Consideration of these issues could take place when conducting evacuation analysis.
8. It is also recommended that consideration should be given to ensure that there should only be one style of lifejacket that can be donned in a similar manner (irrespective of the manufacturer) on board for passengers. The goal of this recommendation is to avoid confusion amongst passengers and crew when donning lifejackets.
Emergency Instructions to Passengers
9. Companies identified that emergency instruction language provision was sufficient for their ships and noted that the extent of information provided in different languages is determined on a case by case basis. Planning based on passenger demographics was seen as important.
10. It was reported that in recent incidents where passengers were mustered as a precaution, passengers had confirmed their understanding of emergency information and instructions.
11. It has been highlighted that some vessel types, and in particular High Speed Craft utilise videos to supplement the provision of emergency instructions. In addition some companies use emergency information cards to complement information required by SOLAS. It is noted that the High Speed Craft Code requires such information to be provided “near each seat”.
12. It was also noted that emergency information is reinforced by announcement and by trained crew during an emergency and at passenger assembly.
Recommendations
13. It is recommended that companies consider extending the use of an accompanying video for passenger emergency instruction notices, where appropriate. It is also recommended that emergency information cards are made available for passengers, on request, that complement the information required by SOLAS.
Common Elements of Musters and Emergency Instructions
14. Companies reported that they had increased their focus on training and drills to ensure crew are able to provide assistance to disabled persons and persons with reduced mobility.
Passenger Muster Policy
15. Companies reported that the policy within MSC.1/Circ.1446/Rev.1 was in place, when required on voyages over 24 hours.
Access of Personnel to the Navigating Bridge and Avoiding Distraction
16. Companies provided information on established bridge access policies which were in place before the Costa Concordia accident. Identified best practice policies included the designation of Red, Amber and Green Conditions for the Bridge and Engine Control Room.
17. Such conditions are designed not only to ensure control of bridge access but to heighten alertness and minimise distractions, as navigational risk varies due to changing circumstances.
18. Companies also reported that they prohibit the use of mobile phones and other media or music devices on the bridge at any time, except as may be necessary for an emergency situation.
19. Typically such policies require the master and OOW to ensure that bridge organisation supports the increasing levels of team alertness and control of risks to safe navigation as conditions change from Green to Amber, Amber to Red or Green to Red.
20. The conditions and requirements for each condition, referred to above, are dependent on company policies and the ship’s trade and area of operation, however, in general:
1. Green is a condition for routine operations when the vessel is clear of pilotage waters and clear of any navigational situation requiring enhanced bridge organisation;
2. Amber is a condition requiring enhanced bridge organisation due to environmental, meteorological, operational or traffic risks, but clear of navigational danger; and
3. Red is a condition where a hazardous navigational situation exists due to meteorological conditions, technical deficiency or navigation in pilotage waters and in close proximity to other vessels or shore.
21. During Red and Amber conditions, procedures are in place to ensure that bridge access is restricted and distractions avoided such as phone calls to the bridge, not related to the immediate operation of the vessel.
Recommendations
22. It is recommended that bridge access control and bridge organisation policies are developed and harmonised to ensure that unnecessary distractions are avoided and that enhanced vigilance is in place and not disrupted during hazardous navigational situations.
Voyage Planning
23. Companies confirmed compliance with the Guidelines for Voyage Planning (Resolution A.893(21)). Company procedures for areas covering voyage planning, the conduct of a passage and bridge watchkeeping were evaluated. It was clear that any deviation from a passage plan is required to be planned in accordance with the Guidelines.
24. An example policy included the guidance that “Despite the master’s/OOW’s experience, qualifications and authority, the situation must never arise, even in pilotage waters, where the plan only exists in the master’s/OOW’s head.”
Recommendations
25. The requirements of A.893(21) should be fully complied with and in addition the further guidance in the ICS Bridge Procedures Guide should be taken into account:
“If the OOW has to leave the passage plan…the OOW should prepare and proceed along a new temporary track clear of any danger. At the first opportunity, the OOW should advise the master of the actions taken. The plan will need to be formally amended and a briefing made to the other members of the bridge team.”
Bridge Team Management and Maritime Resource Management
26. Companies reported on established and implemented bridge team management principles and techniques. One example of best practice is an effective ‘Challenge and Response’ environment on the Bridge and in the Engine Control Room. Effective Maritime Resource Management ensures that individual errors can be identified and corrected by team management of the Bridge or Engine Room.
27. It is noted that the STCW Convention, as amended, now includes requirements for leadership and teamwork skills, as well as resource management.
Auditing of Operations
28. It was reported that Bridge Team audits are conducted periodically and also at random intervals by operational management and by external parties contracted by companies. This ensures that the company’s shore operational management monitors the effectiveness of their bridge operations and that there is also an independent assessment provided. These audits focus on leadership, teamwork and management for all stages of the voyage plan.
Command Development
29. Many companies have established ‘Command Development’ policies that are undertaken prior to a competitive promotion process for command positions. These policies provide trainee masters and potential masters with professional development, support and guidance to prepare them for the role of master on company vessels.
Command Assessment
30. In addition to preparing and selecting masters, companies also regularly assess their masters’ performance at fixed and random periodic intervals. The assessments ensure that procedures are followed and that professional development continues following a command appointment.
Damage Control Drills
31. Since the Costa Concordia accident, companies have assessed the adequacy of and in some cases increased the frequency of, damage control drills.
Distress and Urgency Messages
32. Companies have reviewed their procedures to ensure that if a situation develops on board with the potential to require external assistance there should be no hesitation in requesting such assistance (including the issuing of an Urgency or Distress call) or in increasing on board states of readiness.
Shore Crisis Management
33. Companies reviewed their procedures for the management of an incident ashore and in particular the procedures for shore support and contact provided by a company during and after an incident.
ICS Bridge Procedures Guide
34. The ICS Bridge Procedures Guide is acknowledged as the principal industry guidance on the subject, it is used by ships worldwide and is referred to in the footnotes of several IMO Conventions. The Guide attempts to bring together the good practice of seafarers with the aim of improving navigational safety and protection of the marine environment. The need to ensure a safe navigational watch at all times, is a fundamental principle of the Guide. It is also clear that to ensure the safety of the vessel an essential part of bridge organisation is adherence to correct procedures.
35. ICS advised MSC 91 that the Bridge Procedures Guide is currently under review with the fifth edition anticipated for publication in early 2014. The outcomes of the Costa Concordia investigation will be taken into account during the review process, as appropriate.
Action requested of the Committee
The Committee is requested to note the information provided and in particular the recommendations in paragraphs 7, 8, 13, 22 and 25 and take action as appropriate.
Appendix 2. Watchkeeping Training Requirements