On a ship loading logs, crew were using a crane to tension a wire rope to secure the load. When a wire snapped, equipment recoiled. It struck and fatally injured a seaman. It snapped due to the load from the crane and configuration of pulleys. Crew lacked information and guidance on hazards and doing this work safely. Operator’s safety management system lacked a safety assessment for the work.
Executive summary Tuhinga whakarāpopoto

What happened
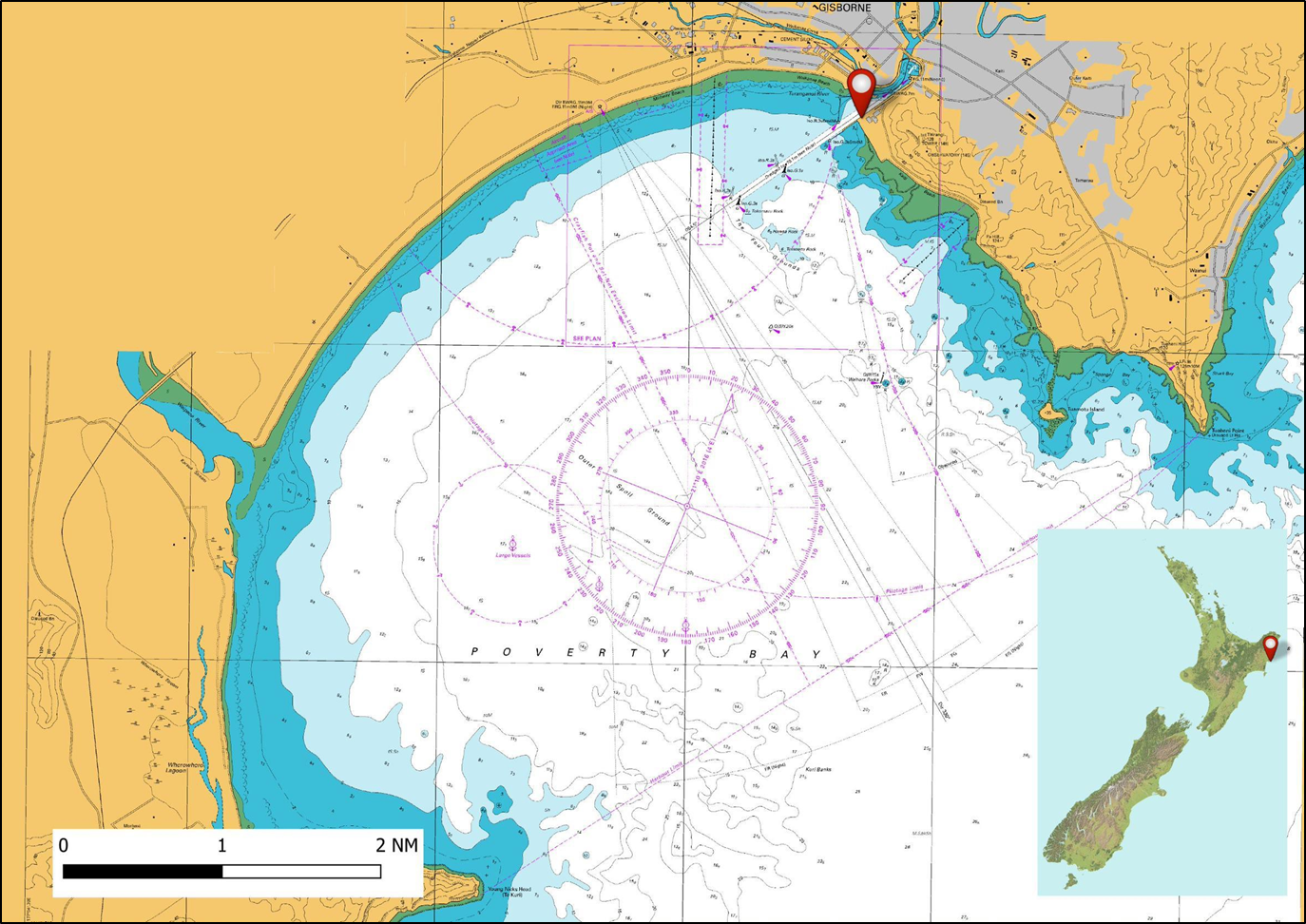
- At approximately 2130 on 2 April 2019, the bulk carrier Coresky OL completed loading logs in Eastland Port, Gisborne. Shortly afterwards the crew commenced securing the logs that were stowed on deck.
- At 2341 the chief officer, boatswain and two able-bodied seamen had just completed securing the logs stowed on top of number one hatch and were commencing to lash the logs stowed on top of number two hatch. It was dark but the deck was well lit by both the ship and shore floodlights.
- The chief officer was operating a crane, which was being used to tension the wiggle wire. Both able-bodied seamen were standing close to the wire to monitor its tension, when the boatswain signalled to the chief officer to stop heaving (to lift or to haul) on the crane’s lifting wire.
- As the heaving stopped, a wire parted and caused the securing equipment to recoil towards the able-bodied seamen. One of the able-bodied seamen was struck by part of the securing equipment and later died of their injuries.
Why it happened
- The crew did not identify the hazards associated with wires under tension and had not implemented mitigation measures prior to undertaking the operation.
- The load being applied by the crane, combined with the configuration of the blocks used to tension the securing wires, was sufficient to part the foot wire.
- Turnbuckles were not rigged between the wiggle wire and foot wires, which meant that the crane was used to tension the wiggle wire. This required both able-bodied seamen, whose role it was to monitor the tension being applied, to be in a hazardous area close to a wire under tension.
- The operator’s safety management system did not include a safety assessment of cargo-securing operations. As a result, no information on the hazards associated with wires under tension was available to the crew, and the cargo securing manual did not provide guidance on a safe system of work for cargo-securing operations on the vessel. As a result, the Transport Accident Investigation Commission made a recommendation that Shih Wei Navigation Company Limited (Taiwan) carry out a comprehensive safety assessment of vessels engaged in carrying and securing deck log cargo. The assessment should result in appropriate procedures and guidance being contained in the safety management system and ensure that a safe system of work is established.
What we can learn
- Securing logs can be a hazardous operation that should be fully risk assessed. Only then will comprehensive procedures and instructions be developed to help create a safe system of work.
- Those involved in a securing operation need to be aware of the likely loads involved and the potential dangers to which they may become exposed. In addition, relevant information needs to be recorded in the cargo securing manual for future reference.
Who may benefit
- Flag administrations, classification societies, ship operators and crew members may all benefit from the information in this report.
Factual information Pārongo pono
Narrative
- The Coresky OL was a Panamanian registered geared (capable of loading and discharging using the vessel’s own cargo-handling equipment) bulk carrier engaged in shipping logs from New Zealand to South Korea.
- At about 1950 on 30 March 2019, the vessel was made fast (secured) alongside the number eight berth in Eastland Port, Gisborne. Shortly afterwards the loading of logs began. The intention was for the vessel to sail on the high tide on the morning of 3 April.
- Prior to entering the port, the crew had carried out a visual inspection of the loose-cargo-securing gear (off-the-shelf equipment including, but not limited to, shackles, chain, hooks, connecting links, turnbuckles, binders, sheave blocks, and swivels used in an assembly to suspend, secure or lift a load) and then made it ready for securing the logs that were to be stowed on top of the ship’s hatches.
- At 2030 on 2 April 2019, the loading of the logs was complete. A total of 34,000 tonnes of logs had been loaded into all five holds of the vessel and onto the tops of the hatches.
- At 2341 the chief officer, boatswain and two able-bodied seamen (ABs) had just completed securing the logs on the number one hatch and were about to start securing the logs on top of the number two hatch.
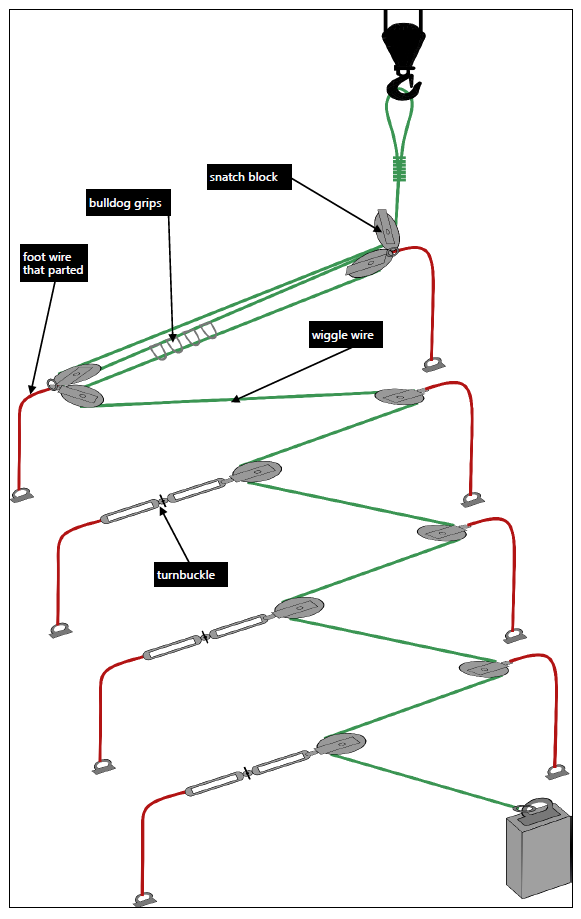
- Figure 3 shows the system the crew were using to secure the cargo. The securing system involved the use of foot wires, snatch blocks and a wiggle wire.
- There was a very light wind and it had just stopped raining. Although it was dark, the deck was well lit by the ship’s own floodlights and the floodlights on the wharf. The crew were wearing personal protective equipment, which included boot spikes to reduce the risk of slipping on top of the wet logs, and safety helmets.
- The chief officer was operating the number one crane, which was being used to tension the wiggle wire, and the two ABs were standing close by, checking the tension. The boatswain who was in charge of the securing operation (see Figure 3) was communicating with the chief officer using hand signals. This was due to the boatswain’s hand-held very high frequency radio having been lost overboard earlier while securing the logs on number two hatch.

- At about 0140 the chief officer commenced heaving (lifting or hauling) on the wiggle wire. At this time the boatswain was walking away from the number one crane and had their back to the chief officer. The boatswain then turned around and signalled to the chief officer to stop heaving.
-
The chief officer stopped heaving on the wiggle wire almost immediately. The boatswain started to walk back towards the two ABs in preparation for attaching bulldog grips to secure the tensioned wire.
- As the boatswain walked back in the direction of the number one crane, a foot wire directly in front of the two ABs parted (to separate or break a rope or wire). The rapid release of tension allowed a block, which was secured to the foot wire, and the wiggle wire to recoil toward the two ABs.
- One of the ABs was struck by part of the securing equipment and later died in Gisborne Hospital. The other AB was hit on the legs by the wiggle wire and sustained minor injuries.
Site examination
- An inspection of the vessel showed a parted foot wire on the port side and a wiggle wire complete with snatch block, shackle and wire eye just to starboard of the vessel’s centreline.
- The crane and securing equipment that were in use at the time of the accident were inspected by a specialist crane engineer, whose report was obtained by the Transport Accident Investigation Commission (Commission). The engineer was requested to attend the accident scene by Maritime New Zealand, and the subsequent report identified that the crane and its rigging were in good working order.
- Both sections of the parted foot wire were removed from the vessel for further testing.
Tests and research
- An expert metallurgist engaged by the Commission examined the parted wire and provided a report. Part of this report can be found in Appendix 1.
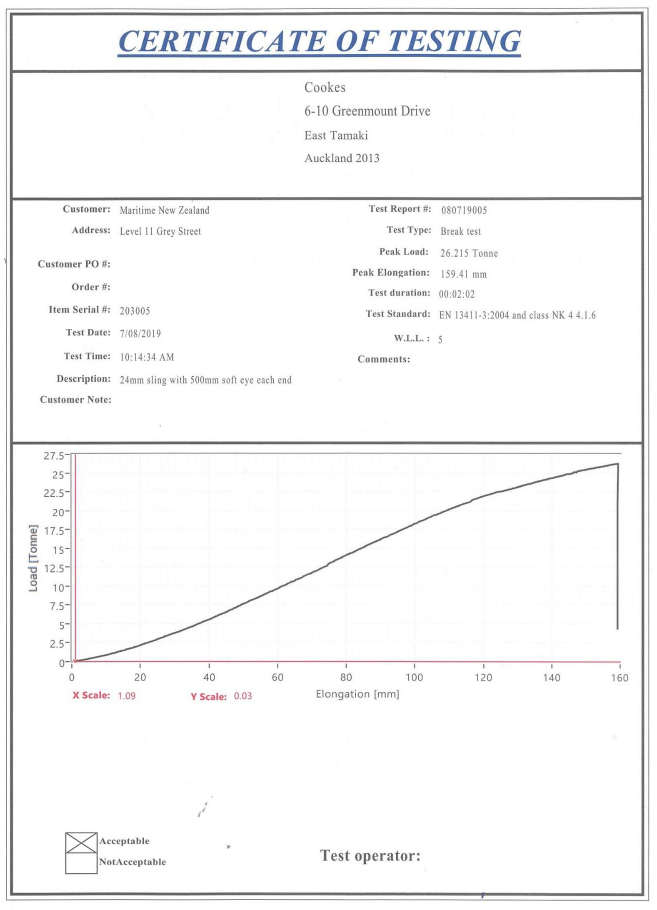
- The parted wire was also tested to breaking point on 7 August 2019 at Cookes New Zealand Limited, in accordance with the Japanese classification society Nippon Kaiji Kyokai’s (NKK).‘Rules and Guidance for the Survey and Construction of Steel Ships (Part L: Equipment)’. A copy of the test certificate can be found in Appendix 2.
Cargo-securing documentation
- The International Convention for the Safety of Life at Sea requires each vessel engaged in the carriage of bulk cargo to carry a cargo securing manual on board. The manual should cover all relevant aspects of cargo stowage and securing.
- An important function of the manual is to provide officers with an awareness of the magnitude and direction of the forces involved in securing cargo and the limitations of securing devices and equipment. It should also show the correct application of securing devices and equipment and provide advice to the ship’s crew for securing cargo.
- The cargo securing manual should also contain, in part, identification markings and certification showing test results and the maximum securing loads of all cargo-securing equipment.
- The cargo securing manual supplied to the Coresky OL had been approved on behalf of its flag administration by Nippon Kaiji Kyokai.
- In addition to the cargo securing manual, the International Maritime Organization (IMO) produces a Code of Safe Practice for Ships Carrying Timber Deck Cargoes. The code provides:
- guidance for safe transportation
- methodologies for safe stowage
- design principles for securing systems
- guidance for developing procedures to be included in the vessels’ cargo securing manual.
- The code is non-mandatory and applies to ships of 24 metres or more in length carrying timber deck cargoes. A copy of the code was contained in Coresky OL’s cargo securing manual.
Documented method for securing deck log cargo on the Coresky OL
- The documented method for securing deck log cargo on board the Coresky OL was laid down in the vessel’s cargo securing manual and supplemented by the guidance provided in the IMO Code of Safe Practice for Ships Carrying Timber Deck Cargoes, 1991. The method can be seen in the simplified diagram in Figure 4. It required a combination of wiggle wires, foot wires and turnbuckles to secure the deck logs in position.
- A wiggle wire, secured at one end to a deck fitting, was required to be run through a series of snatch blocks, which were secured to foot wires on one side of the vessel and to turnbuckles on the other side (see Figure 4).
- Although there was no specific guidance on how to tighten the wiggle wires, once the appropriate tension was achieved the wiggle wires were secured in position using bulldog grips.
- When the vessel was on passage, the turnbuckles were to be used to tighten the wiggle wires further if movement of the deck logs had created slack.
The foot wire specification
- The foot wire that parted was constructed from a coil of wire manufactured by Nantong Steel Wire Rope Group, China in May 2014.
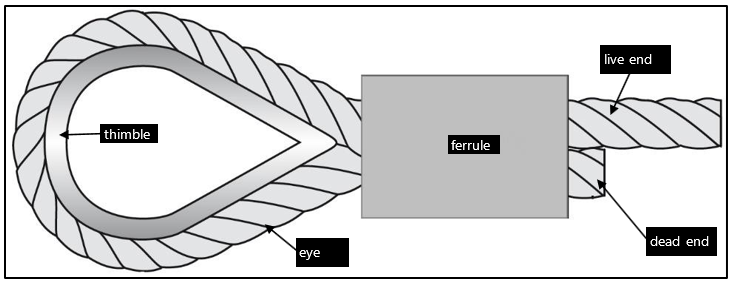
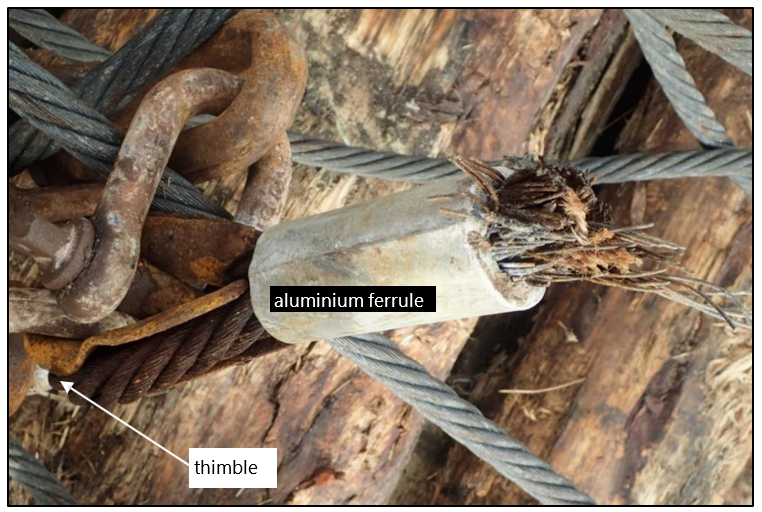
- The wire was 24 millimetres in diameter and made from hot galvanised steel, with six strands of 24 wires containing fibre cores. It was certified as having a minimum breaking load of at least 269 kilonewtons, equivalent to 27.4 tonnes. The foot wire was 15.5 metres long and had an eye constructed using a steel thimble and an aluminium ferrule15 at each end (see Figure 5).
- The vessel’s cargo securing manual defined the maximum securing load of re-usable wire ropes, such as foot wires, to be 30% of their breaking strength. By calculation, the maximum securing load of the foot wire that parted was 8.22 tonnes.
Inspection and maintenance of wire ropes
- The cargo securing manual required regular routine visual examinations to be carried out on all portable cargo-securing devices, and periodic examinations/re-testing as required by the flag administration.
- If a visual inspection identified a permanent deformation or break, the device was to be removed from service.
- The cargo securing manual also required that all inspections be recorded and kept with the manual.
- The cargo securing manual on the vessel showed that the crew routinely visually inspected all loose-cargo-securing devices for any obvious defects before entering a port and preparing the securing equipment for use.
- Prior to entering Gisborne on 31 March 2019, the crew visually inspected all the loose-cargo-securing equipment and recorded that all equipment was “sound”.
Drug and alcohol
- The Commission received evidence showing that after the accident the crew underwent testing for alcohol using an onboard breath analyser. The results were negative (clear) for all crew members.
- A toxicology test carried out by the Institute of Environmental Science and Research (New Zealand) on the deceased AB showed a negative (clear) result for alcohol and drugs.
Analysis Tātaritanga
Introduction
- Securing logs on the deck of a ship can be a hazardous task that requires good communication and co-ordination of skills between the people involved.
- At the time of the accident, the chief officer and the boatswain were being assisted by two ABs to secure the deck log cargo above number two hatch.
- The team securing the deck logs had all completed the task numerous times before. Both the chief officer and the boatswain were charged with overseeing the operation and had considerable experience.
- The two ABs who were struck by the securing equipment had been tasked with checking when the tension in the wiggle wire was sufficient.
- The following section analyses the failure of the foot wire and the subsequent fatality of the AB. It also examines the conduct of the cargo-securing operation and associated procedures.
Failure of the foot wire
- Both sections of the foot wire that parted were removed by the Commission from the vessel. Experts were appointed to conduct a thorough metallurgic examination of the parted wire (see Figure 6) and to carry out a destructive load test on the remaining section of the foot wire.
Metallurgical examination
-
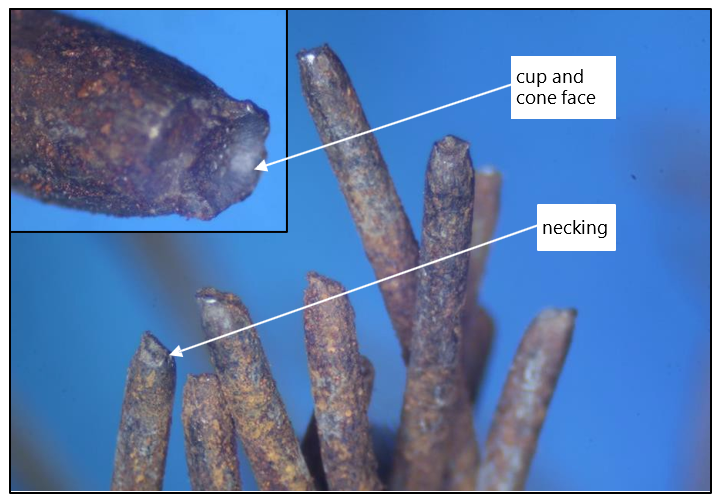
The foot wire was inspected by a metallurgic engineer, who concluded in part:
The failure of the rope most likely occurred as a result of overload. The failed wires exhibited necking and a cup and cone fracture face that is typical of this type of failure.
Although some corrosion had occurred it is considered unlikely that corrosion of the rope was the primary cause of the failure.
- The elements of the failure mechanism described by the engineer can be seen in Figure 7, and the relevant section of the report is contained in Appendix 1.
Destructive test
- On completion of the visual examination, the foot wire was tested to destruction (parted under controlled conditions) to determine its breaking load at the time of the accident. This test concluded that the load required to part the wire was 26.21 tonnes. The certificate of testing can be found in Appendix 2.
- The Commission found that the breaking strength of the parted foot wire at the time of the accident had not been significantly reduced since its manufacture in 2014.
- In the absence of any defect being identified in the foot wire, it was likely that the crane was applying a load that resulted in the foot wire being overloaded and parting.
Why the foot wire was overloaded
- An overload of a wire occurs when the axial load exceeds the breaking load (Verreet, R. and Ridge, I., 2005. Wire rope forensics). The vessel’s cargo securing manual stated that to minimise the likelihood of wire overload occurring, re-useable wires were considered to have a maximum securing load of 30% of their certified breaking load. In the case of the foot wire this was 8.2 tonnes, which allowed a margin of safety of 19.2 tonnes. The maximum securing load of the foot wire was not recorded in the vessel’s cargo securing manual and the crew were unaware of the value when interviewed. This increased the risk of the crew inadvertently exceeding the breaking load of the foot wire.
- The cargo securing manual on the Coresky OL also showed how the securing equipment (see Figure 4) was to be configured to apply a binding effect on the logs.
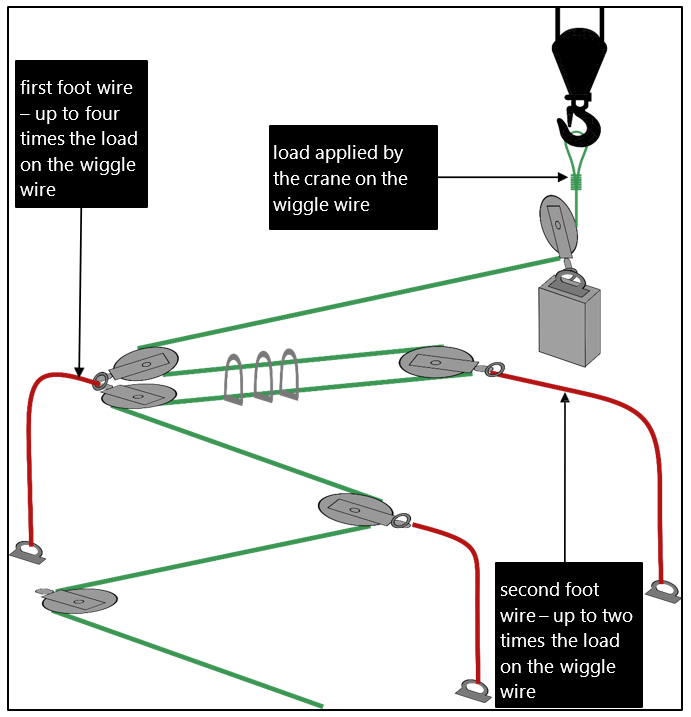
- At the time of the accident, the securing equipment was configured to allow the crew to attach bulldog grips and secure the tensioned wiggle wire between the first and second foot wires (see Figure 8). The first foot wire had two blocks attached to it. This resulted in the first foot wire having a load of three to four times the load being applied by the crane to the wiggle wire (see Figure 8). Therefore, the crane needed to apply between
- 6.55 and 8.7 tonnes to the wiggle wire to overload the foot wire. The crew were unaware that the foot wire was experiencing a load three to four times greater than the load being applied by the crane. This increased the risk of the crew inadvertently exceeding the breaking load of the foot wire.
- The diagram in the guidance material also showed turnbuckles (see Figure 4) between the wiggle wire and the foot wires. Turnbuckles allow tension to be increased or decreased manually in a controlled manner. However, at the time of the accident turnbuckles had not been rigged between the wiggle wire and the foot wires. Instead, blocks had been attached directly to the foot wires. As a result, it was not possible to increase the tension in the wiggle wire manually after the initial tension had been applied. If turnbuckles had been rigged, it would have been unnecessary for the crane to apply more than just the initial tension and reduced the likelihood of a foot wire becoming overloaded.
- By not rigging turnbuckles on the day of the accident, it was necessary for the crew to use the ship’s crane to apply sufficient tension in the wiggle wire to bind the logs securely. The ABs, whose role was to monitor the tension, had no way of determining how much tension was in the wire other than by feel. This required them to ‘step’ on the wiggle wire. For the two ABs to be able to ‘step’ on the wiggle wire, it was necessary for them to stand in a hazardous area close to a wire under tension. This exposed them to considerable risk from the failure of any part of the securing equipment that was under tension.
- It is usual, before commencing work of this sort in a hazardous environment, for the person in charge of the operation to hold a pre-work safety meeting or ‘toolbox talk’. Such meetings were not routinely held on board the Coresky OL. Had a meeting been held before this securing operation commenced, it would have provided an opportunity for the team to discuss the safety implications of crew standing in hazardous areas where wires and associated securing equipment were under tension. Although the crew had carried out this task many times before, a pre-work safety meeting might have prompted them to think of alternative solutions to standing in a hazardous place, including the recommended use of turnbuckles to reduce the amount of tension required in the wiggle wire.
Safety management
Safety issue: The operator’s safety management system was not supported by an effective safety assessment of log-cargo-securing operations, which should have identified the hazards present. This resulted in ineffective controls to mitigate the risks to crew when completing these tasks.
- A safety management system (SMS) is defined in the International Safety Management Code as “a structured and documented system enabling company personnel to implement effectively the company safety and environmental protection policy”. A mature SMS should include but not be limited to:
- operating procedures
- role responsibilities
- review and audit requirements
- training requirements
- identifying risks to personnel and establishing appropriate safeguards.
- Incorporated within the operator’s SMS was the vessel’s cargo securing manual, which contained technical instructions for the crew in respect of securing deck log cargo.
Operating procedures for securing cargo
- The cargo securing manual contained a copy of the IMO’s ‘Code of Safe Practice for Ships Carrying Timber Deck Cargoes – 1991’. However, the most current version of the code had been adopted on 30 November 2011.
- A number of changes had been made to the code between 1991 and 2011. Significantly, the 2011 version of the code explained:
- the need for turnbuckles to be rigged between wiggle wires and foot wires
- that a crane or winch was to be used only to apply the initial tension to wiggle wires.
- An extract from the 2011 edition of the code, explaining the arrangement for wiggle wires, is shown in Figure 9.
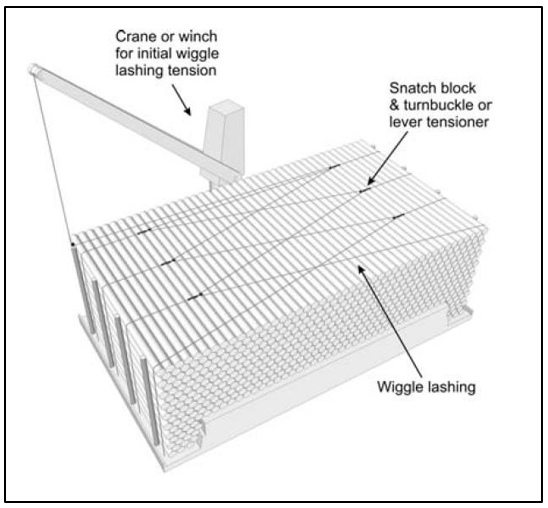
- The explicit reference to apply only the initial tension would have provided the crew with the guidance necessary to minimise the likelihood of inadvertent overload and reinforce the need to use turnbuckles, which would have allowed the crew to better assess the amount of tension throughout the securing system.
- The implementation of the 2011 version of the code, and the procedural changes contained within it, would have also prompted the operator to conduct a review of the log-securing operation and update procedures and instructions within the SMS.
- Although the vessel’s SMS had been audited by the classification society and by internal auditors, the audits had not identified that the vessel was using an out-of-date IMO Code of Safe Practice for Ships Carrying Timber Deck Cargoes. As a result, the amendments contained in the 2011 code, which would have made the operation safer, had not been incorporated into onboard procedures.
Risk-assessing the log-securing operation
- The operator’s SMS required the crew to undertake an initial risk assessment before securing the deck log cargo. The SMS instructed the crew to carry out a second, detailed risk assessment if the initial risk assessment identified any “significant risks”.
- Evidence showed that previous initial and detailed risk assessments carried out by the crew for deck log cargo operations had each identified the same hazards. The assessments carried out on the day of the accident were no different. The detailed risk assessment, of which an extract is shown in Table 1, did not identify any additional hazards.
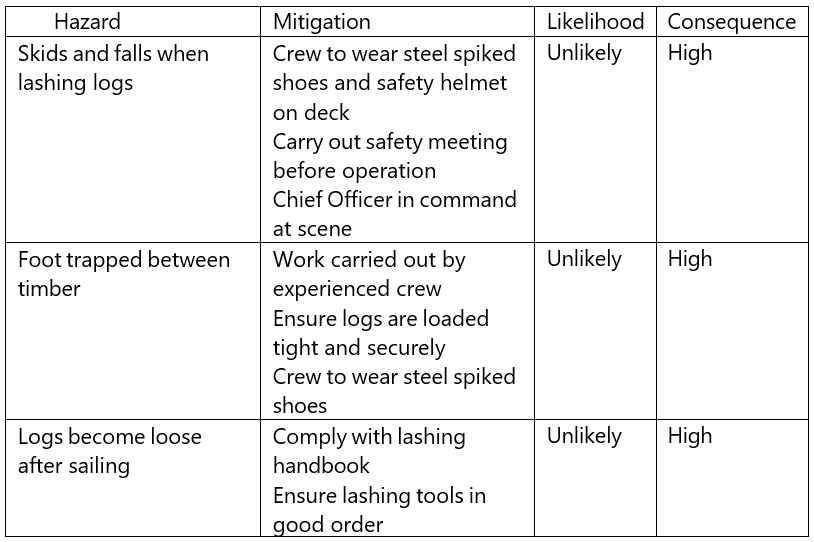
- There were more significant hazards present in the securing operation that were not identified, such as the potential hazard of wires under tension parting.
- Although the cargo securing manual provided technical guidance and drawings on how log cargo was to be secured on the deck, it did not provide a safe operating procedure for the crew to follow. The development of a safe operating procedure was the responsibility of the operator and should have involved a fulsome risk assessment. Because the operator had not undertaken such an assessment for log-securing operations, there was no guidance contained in the SMS about the dangers associated with wires under tension, the potential for load multiplication, snap back zones (the predicted trajectories of lengths of rope or wire from their points of failure) or safe areas to stand when a crane was being used to heave on the wiggle wire. This likely contributed to the crew involved in this accident not identifying this hazard during their risk assessments or implementing appropriate mitigations.
- A fulsome assessment by the operator would have likely provided it with the opportunity to implement more effective mitigation measures for the hazards of the log-cargo-securing operation. Doing so would have helped to ensure that a safer system of work was established and that the crew were exposed to fewer risks. The Commission has therefore made a recommendation to the operator to carry out such an assessment.
Provision of information to crew
- The cargo securing manual provided the crew with some of the information they required. However, the crew would still have had to calculate the safe working load of loose-cargo-securing gear calculate the load being applied to the foot wires through the configuration of the blocks, and then produce a risk-mitigation plan.
- This was a task more suited to being conducted by the operator, before the vessel commenced operations, using experts familiar with the methodology of the securing operation and the loads likely to be imparted.
Appendix 1. Quest Integrity visual and metallographic examination
Appendix 2. Cooke's destructive testing certificate