A tourist jet boat impacted a rock face when its steering and propulsion failed. 9 injuries. Fatigue cracking broke bolts holding steering nozzle and tailpipe together. Operator's hazard focus was more on operating conditions and driver training than mechanical matters. Regulatory practice should address the need for every jet boat operator to have a regime to maintain safety-critical components.
Executive summary

What happened
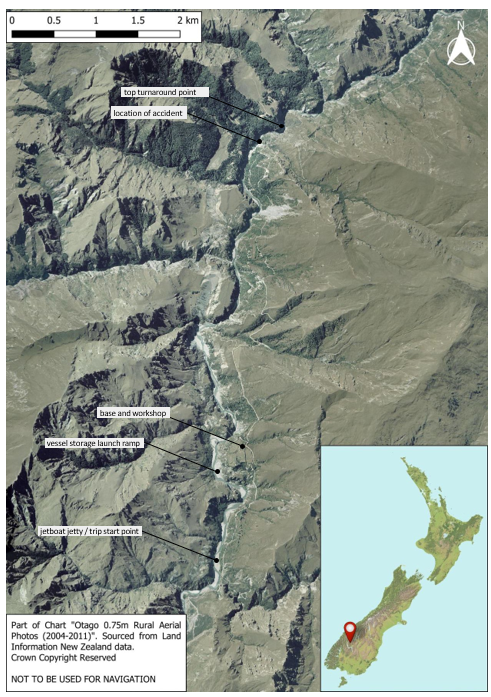
- On 23 February 2019, the commercial jet boat Discovery 2 was operating on the Shotover River in the vicinity of Skippers Canyon with nine passengers on board.
- The boat was on its return leg when the driver was required to negotiate a series of bends in a section of the river about 10 metres wide. Approaching a left-hand bend, the driver tried to turn the wheel over to the left but it would not move. The driver then tried to reduce speed by operating the reverse bucket, which also wouldn’t move.
- As a result the jet boat continued on its heading across to the opposite side of the river where it made contact with a rock face. The speed of impact was estimated to be between 20 and 30 kilometres per hour.
- On impact, one passenger was thrown partially overboard and suffered a broken leg, while the remaining passengers suffered minor lacerations and bruising. A rescue helicopter was on the scene about 20 minutes later and evacuated the passengers.
Why it happened
- Jet boating is a high-risk activity that leaves very little margin for error when navigating at high speeds in narrow channels and rivers. On this occasion the driver lost control of the jet boat due to a mechanical failure of the jet unit steering and propulsion system.
- An inspection of the jet unit showed that three of the four stud-bolts securing the tailpipe assembly to the steering nozzle had suffered fatigue cracking, rendering the unit ineffective.
- It is highly likely that the fatigue cracking was because the nuts on the stud-bolts were not tightened to the manufacturer’s recommended torque. As a result there was insufficient pre-tension in the stud-bolts.
- The operator’s hazard identification system had not identified the failure of the steering and propulsion system as a hazard, focusing more on operating conditions and driver training.
What we can learn
- An analysis of the evidence identified a number of key lessons:
- when a manufacturer provides detailed instructions and guidance on how to maintain its equipment, the onus is on the maintainer of the equipment to follow those instructions and ensure that it has an appropriate maintenance regime in place
- historically, investigations of jet boat accidents have mainly attributed the causes to operational conditions and driver training, but it is essential that operators pay equal attention to mechanical equipment and identify critical parts that, if defective, can have significant impacts on the safety of the operation.
Who may benefit
- In the interests of improving safety in the adventure tourism sector, the Transport Accident Investigation Commission has made a recommendation to the Director of Maritime New Zealand to address the requirement for operators to identify systems that are critical to the safe operation of a jet boat and ensure appropriate maintenance schedules are in place.
Factual information Pārongo pono
Narrative
-
On the morning of 23 February 2019, the jet boat Discovery 2 was parked on a trailer at its overnight storage facility in Skippers Canyon on the Shotover River. At about 0830 (times in this report are in New Zealand Standard Time (Co-ordinated Universal Time +12 hours) and are expressed in the 24-hour format) the Discovery 2’s driver commenced preparing the boat for the day.
-
The driver conducted various pre-start checks, which included a visual inspection of the jet unit, before starting the engine and reversing the boat off the trailer and into the water. The driver then took the boat for a short trip downriver to check that all systems were operating as expected, including the steering and control systems. The driver then berthed the Discovery 2 at the jetty ready for the first passengers to arrive (see Figure 3).

- When the passengers arrived, the driver provided each of them with a life jacket before they were allowed to board the Discovery 2. There was a total of nine passengers for the first trip of the day.
- When all the passengers were seated, the driver delivered a safety briefing. It included a demonstration of driver hand signals, for example when the driver intended to ‘spin’ the boat, and instructions to remain seated and hold on to the handrail in front of the seats, to not smoke, and to keep hands and arms within the confines of the boat at all times.
- The driver then took the boat away from the jetty and carried out a spin manoeuvre to demonstrate the jet boat movements and to check if any passengers wished to disembark.
- Trips were usually conducted using two jet boats, one following the other. Once the Discovery 2 had departed the jetty, a second jet boat berthed and embarked its passengers and followed behind the Discovery 2.
- The Discovery 2 set off up the river and arrived at the top turnaround point about 15 minutes later. It then departed and began the trip downriver.
- After about one minute travelling downstream the Discovery 2 came to a section of river with a series of quick, sharp turns (see Figure 4). This section of the river was about 10 metres wide and 30 metres long and the boat speed through the section was typically about 75 kilometres per hour.
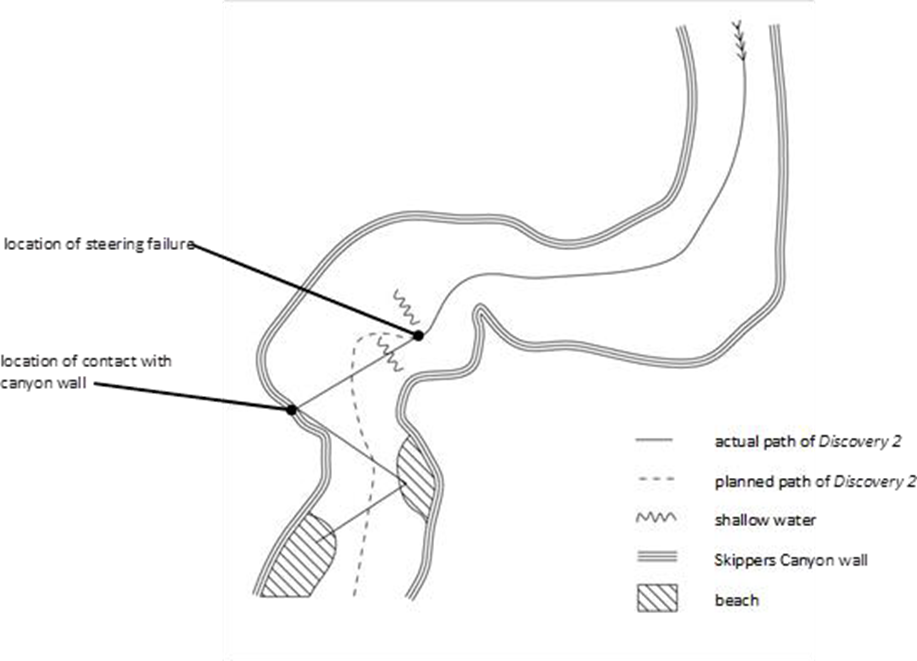
- As the Discovery 2 approached the first left-hand turn the driver steered to the left, but on the right-hand turn the driver tried turning to the right but the steering wheel would not move. The driver tried ‘shaking’ the wheel from left to right but it remained jammed. The driver then tried lowering the reverse bucket to stop the boat, but it wouldn’t move.
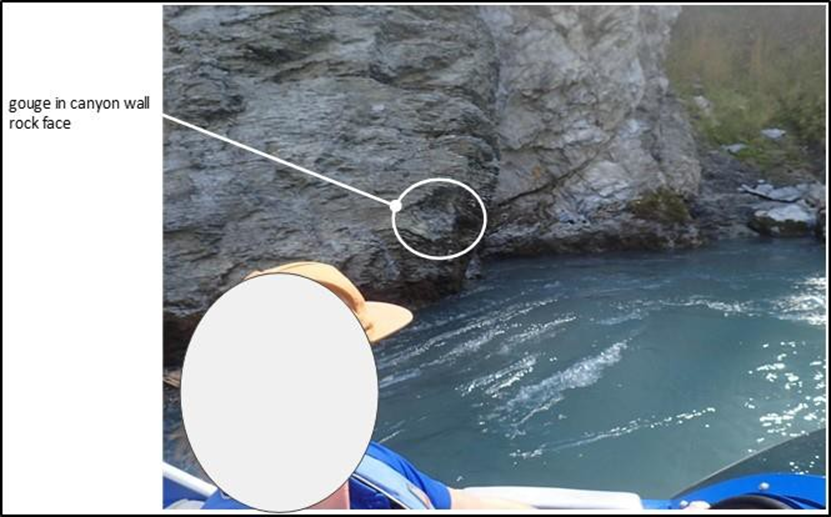
- The Discovery 2 skimmed across the water and collided with a rock face on the right-hand side of the river. The driver estimated that the collision speed was between 20 and 30 kilometres per hour. Figure 5 shows the gouge left in the rock face after the impact of the boat.
- The driver immediately broadcast a mayday distress call using the very-high-frequency radio.
-
As a result of the impact, one passenger was thrown partially overboard. The driver immediately helped them back on board, but the passenger was later diagnosed as having suffered a broken leg.
-
The Discovery 2 drifted with its bow pointing towards a river beach a few metres away. The driver applied some thrust using the jet unit and put the bow onto the beach.
- The driver confirmed the mayday distress call with the operators base and gave a situation report. The driver then began assessing the passengers for injuries, of which the majority were minor lacerations and bruising.
- As passengers moved around the boat, the weight distribution changed and the action of the river acting on the stern of the Discovery 2 moved the boat off the beach and back into the river. The driver saw it was pointing at another beach on the other side of the river and beached it again.
- The estimated time between starting the return trip and beaching for the second time was about three or four minutes.
- A few minutes later the second jet boat arrived at the scene. Together the two drivers helped move the passengers from the Discovery 2 to the river beach.
- A rescue helicopter arrived at the scene about 20 minutes later and evacuated all the passengers through multiple trips. They were all discharged from hospital that day except for the passenger who had suffered a broken leg.
The operator
- At the time of the accident the operator, Skippers Canyon Jet Limited, was a privately owned adventure tourism business based in Queenstown, New Zealand. It offered jet boat rides of about 25 minutes’ duration on a stretch of the Shotover River.
- The operator ran a bus service, picking passengers up in Queenstown and delivering them to the operator’s base at Skippers Canyon. Passengers embarked on a jet boat for a return trip upriver before being returned to Queenstown by bus.
- Skippers Canyon Jet Limited operated five commercial jet boats.
How a jet boat works
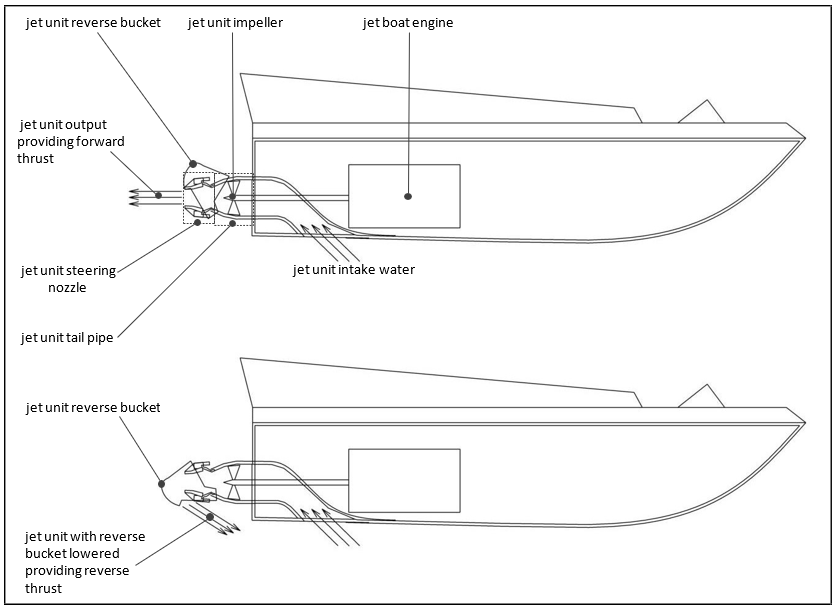
- A jet boat is propelled and steered through the water by a jet unit (see Figure 6). The jet unit is an impeller water pump powered by the jet boat’s internal combustion engine. The pump sucks water in through an intake under the hull, and forces it out through a pipe and steering nozzle mounted on the transom, thereby providing thrust to the boat. The steering nozzle can be rotated either side using the driver’s steering wheel to direct the thrust and provide steering.
- A bucket-shaped deflector is attached to the unit, which can be lowered down over the end of the steering nozzle. The deflector redirects the water jet forwards, which provides reverse thrust. The deflector is named the ‘reverse bucket’, and is lowered using a lever located beside the driver’s seat.
- The tailpipe, steering nozzle and reverse bucket installed on the Discovery 2 are shown in Figure 7.

The jet unit
- Hamilton Jet Limited is a jet unit manufacturing company based in Christchurch, New Zealand. The Discovery 2 was fitted with a HamiltonJet Limited unit model HJ212. The HJ212 is designed principally for a jet boat intended to be transported by a road trailer. The model was introduced in 1992 and about 12,000 units have been produced. The HJ212 is the prevalent jet unit used by commercial jet boat operators in New Zealand.
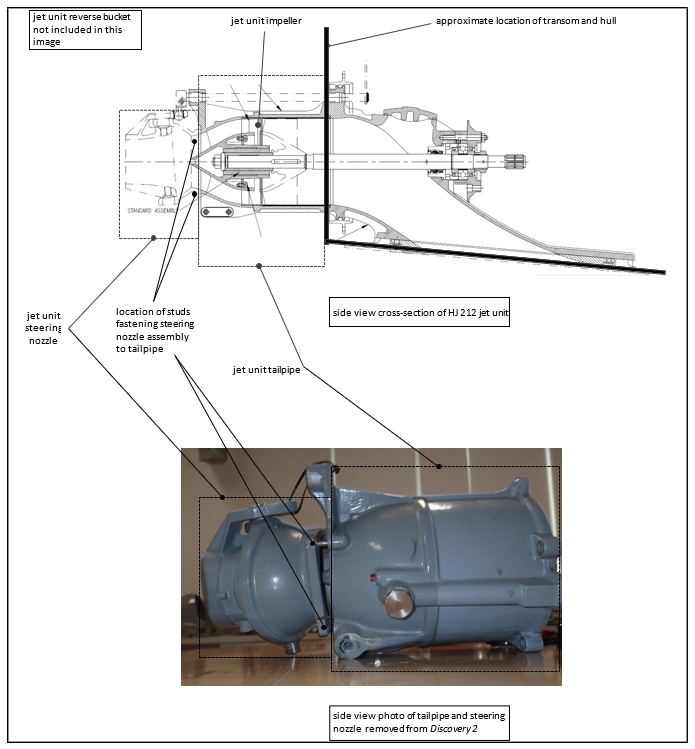
- Figure 8 shows a side-view cross-section design drawing of the HJ212 jet unit, together with a photograph of the HJ212 jet unit removed from the Discovery 2 after the accident. It can be seen in the photograph that the steering nozzle had become partially detached from the tailpipe, and at least one of the stud-bolts4 fastening the steering nozzle assembly to the tailpipe had parted.
Maintenance requirements for the Discovery 2
- The planned maintenance programme for the Discovery 2 was based on the accrued operating hours of the boat, which were measured by recording the engine operating hours displayed on the jet boat’s dashboard. The maintenance programme had been developed by the operator based on its previous experience and various manufacturers’ guidelines and recommendations. There were four levels of maintenance check:
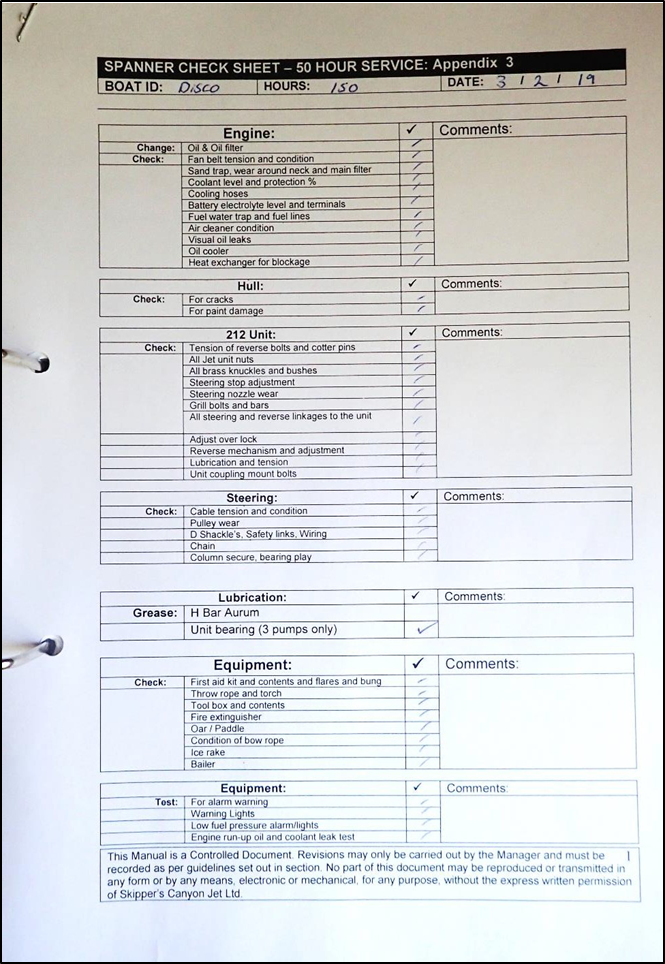
- 50-hour checklist – recurring every 50 hours of engine operation. Various parts of the boat were checked and maintained in accordance with the 50-hour checklist (see Appendix 1)
- 100 and 200 hours – additional maintenance items were added to the 50-hour check
- 1,000 hours – the boat was given a major refit, which included removing, re-installing or replacing all the systems of the boat. During a refit the jet unit nozzle was not usually removed from the jet unit tailpipe. Subsequent to the 1,000-hour maintenance check the hours started again from zero.
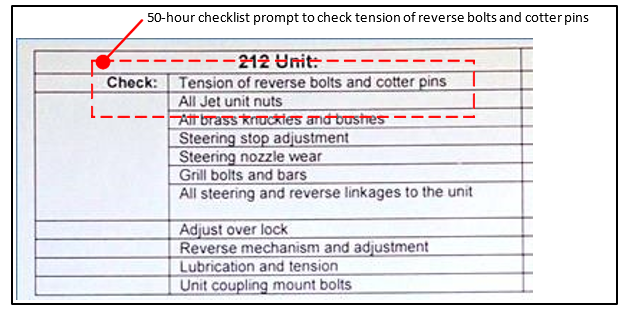
- The 50-hour checklist included an assessment of the HJ212 unit. The assessment required that the tension of the cotter pins and the bolts holding the reverse bucket be checked, and similarly that all jet unit nuts be checked (see Figure 9).
- The maintenance mechanic used a torque wrench6 to check the tension on the bolts holding the reverse bucket and cotter pins, and a spanner for all other nuts.
Recent maintenance history of the Discovery 2’s jet unit
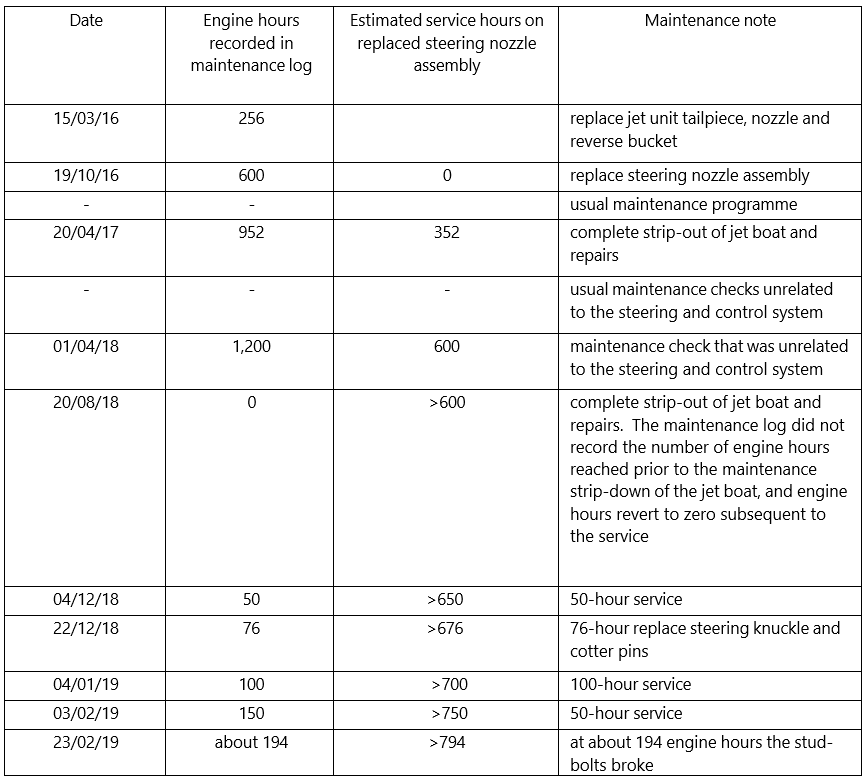
- The jet unit fitted to the Discovery 2 at the time of the accident had been installed in March 2016. In October 2016 the operator had replaced the steering nozzle assembly of the jet unit with an upgraded model; this was consistent across all the operator’s jet boats. The upgraded model used a different bearing system, but this change did not contribute to the accident. The Discovery 2’s recent maintenance history relative to the jet unit is shown in Table 1. The estimated number of service hours for the steering nozzle assembly is based on accumulated engine hours recorded in the maintenance log after the new steering nozzle assembly had been installed on 19 October 2016.
How the steering nozzle was fastened to the tailpipe
- Figure 10 shows a schematic drawing of a stud-bolt used to clamp the jet unit steering nozzle to the tailpipe. The stud-bolt is permanently screwed into the tailpipe, and the steering nozzle is clamped on to the tailpipe with the force of the nut screwed on to the stud-bolt.
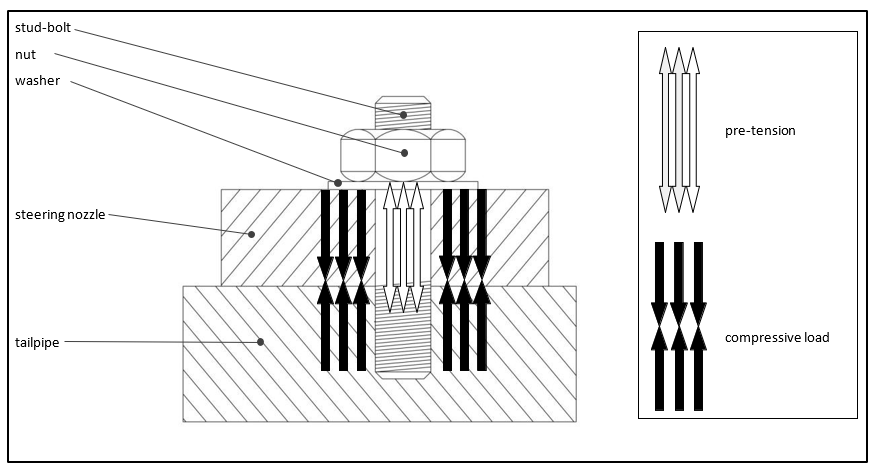
- The integrity of the engineering joint between the steering nozzle and the tailpipe is dependent on the stud-bolts being protected from the operational loads. The job of a stud-bolt is to hold the components together tightly to transfer loads directly between the two components rather than the stud-bolt. This is achieved by applying pre-tension to the stud-bolt.
- As the nut is tightened on to the stud-bolt, it creates tension within the bolt known as ‘pre-tension’, which is effectively trying to stretch the stud-bolt. The pre-tension within the bolt forces the two components together and creates an equal but opposite compressive load within and between the two components. As long as the compressive load is greater than the operational load the stud-bolt will be protected. Maintaining the compressive load is dependent on the two clamping faces being incompressible.
- The pre-tension of a bolt or stud is generated by tightening the nut, hence pre-tension is measured by the magnitude of torque used to tighten the nut.
- It is important to protect the stud-bolt from experiencing operational loads when the joint is subject to cyclic loading, as it was on the Discovery 2’s stud-bolts fastening the steering nozzle to the tailpipe. Cyclic loading on a stud-bolt causes fatigue, which can lead to fatigue cracking.
Steering nozzle insert and liquid sealant
- Figure 11 shows part of a design drawing of the steering nozzle assembly. The assembly includes three main components: the steering nozzle, the steering nozzle housing, and the steering nozzle insert. The steering nozzle assembly faces up against the tailpipe clamping face.
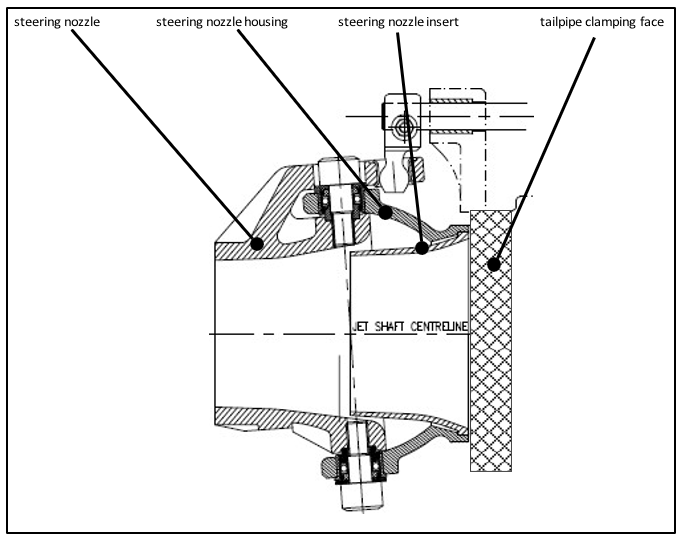
- It can be seen in Figure 11 that the steering nozzle insert must fit flush with the steering nozzle housing in order to achieve a good ‘flat’ and incompressible clamping face between the steering nozzle assembly and the tailpipe.
- It is a common practice in marine engineering to include some form of sealant between two components that are bolted together. The manufacturer’s specifications for the HJ212 did not specify that a sealant be used between the steering nozzle assembly and the tailpipe. However, a liquid sealant had been applied between the steering nozzle assembly and the tailpipe when it was fitted. Remnants of the sealant material can be seen on the bearing face of the tailpipe in Figure 12.
Engineering failure analysis of the jet unit
- An observation of the steering nozzle showed that it had become partially detached from the jet unit tailpipe. The entire tail assembly of the jet unit (Figure 12) was removed from the boat for the purpose of analysis.
- A failure analysis of the jet unit was conducted by an independent engineering consultancy (Quest Integrity NZL Limited report, ‘Assessment of failed water jet unit’ dated 6 June 2019). The consultancy provided a report, which is referenced by the Transport Accident Investigation Commission (Commission). A brief summary of the examination and findings is given below.
- The examination included the stud-bolts and fracture surface, the locations of the stud-bolts, the condition of the bearing surfaces between the tailpipe and the steering nozzle assembly, and the steering nozzle-housing surface under the stud-bolt nuts/washers (shown in Figures 12 and 13).
- The consultant’s report found, in part:
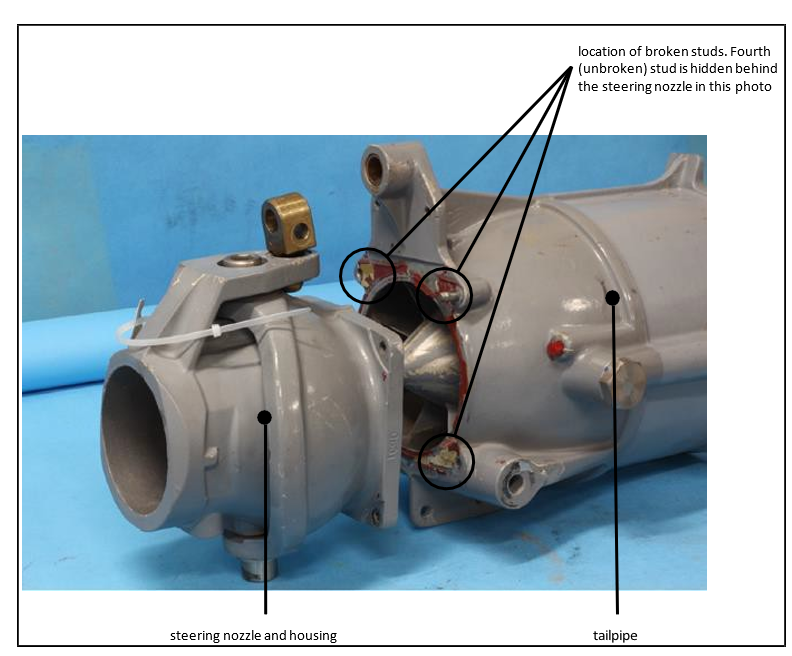
- the jet nozzle failed on the Discovery 2 as a result of fatigue cracking of three of the four stud-bolts holding the nozzle housing on to the tailpipe (shown in Figure 12)
- the fatigue cracking had begun within about the previous 200 hours of operation
- the major cause of the fatigue cracking is considered to be a lack of adequate torque when the nuts were last tightened on the stud-bolts
- this led to insufficient pre-tension on one or more of the stud-bolts, in turn resulting in excessive cyclic loads being applied to the stud-bolts, resulting in the observed fatigue failures
- on the Discovery 2’s jet unit, the steering nozzle insert was slightly proud of the steering nozzle housing; it protruded in places up to 0.23 millimetres, which could have affected the integrity of the joint.
- a liquid sealant had been applied to the joint, and was found to be up to 0.1 millimeters thick. If the stud-bolts had been tightened to specification the sealant should have been extruded from the contact face.

Industry regulation
Maritime Rules Part 80
- Maritime Rules Part 80: Marine Craft Involved in Adventure Tourism came into force in August 1998 and was superseded by Part 82: Commercial Jet Boat Operations – River in August 2012. Part 80 incorporated codes of practice for various types of marine craft used in the adventure tourism industry. For example, initially it provided codes of practice for commercial jet boats on rivers, and commercial rafting.
- Part 80 required, in part, that the operator “draw a safe operational plan that is related to the specific operations of that owner’s boat or boats”. It laid out requirements that the safe operational plan must meet, including a planned maintenance schedule and operational checks of the boat.
-
Two jet boat accidents occurred in 1999 (MO-1999-213 Jet boat Shotover 15 collision with canyon wall, Shotover River, Queenstown, 12 November 1999 and MO-1999-212 Jet boats Shotover 14 and Shotover 15 separate collisions with canyon wall Shotover River, Queenstown, 21 October and 12 November 1999) and the respective reports were combined. The Commission made 25 recommendations with respect to the two accidents. One of those recommendations was directed at Part 80. The Commission recommended:
a change to Rule Part 80 that will require:
Commercial jet boat operators to identify on each jet boat all components that are critical to the safe operation of the boat, and to have a documented inspection and maintenance system in place that covers those critical components. The inspection and maintenance system should complement rather than replace any system of daily checks. (104/99)
-
The recommendation was closed in 2005 without changing Part 80. Instead there was an expectation from the Maritime Safety Authority (Maritime Safety Authority was the predessor to Maritime New Zealand) that operators would address this issue in their own Safe Operational Plan. Maritime Rules Part 80 was subsequently superseded in 2012 when Part 82: Commercial Jet Boat Operations – River came into force.
Maritime Rules Part 82
-
Part 82 does not explicitly address the intent of recommendation 104/99, but includes a section ‘Managing hazards’ (Appendix 2), which refers the jet boat operator to ‘its health and safety responsibilities under the Health and Safety in Employment Act 1992, by including, without being limited to, the following [in part]:’
(a) the process used by the operator to identify the operational hazards that may cause harm to a person; and
(b) the process used by the operator to review operational hazards and how they are to be controlled, including how drivers are made aware of new hazards before drivers and passengers are exposed to them (for example, the day-to-day changes in river conditions); and…
(c) the process for reporting significant hazards, accidents, incidents, and mishaps; and…”
The operator’s hazard identification and mitigation system
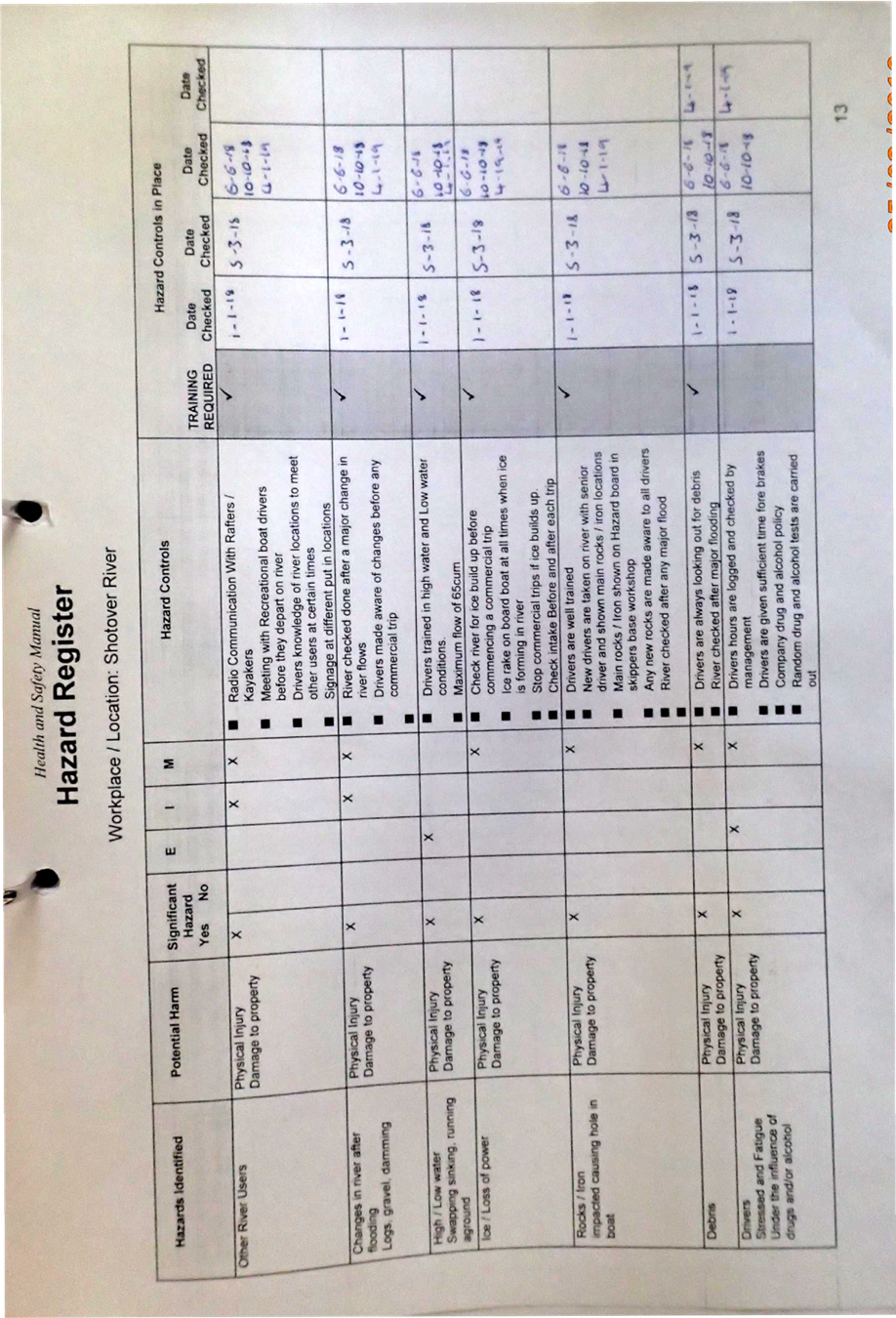
- The operator’s Safe Operating Plan incorporated a Health and Safety Manual. The Health and Safety Manual procedures for hazard identification and control included a Hazard Register.
- The operator’s Hazard Register was divided into four workplace locations: Queenstown Base, Skippers Canyon Base, Skippers Road and Shotover River.
- The operator’s Hazard Register and hazard identification process included using its response to incidents and its previous experience in operating commercial jet boats, monitoring industry publications (including the Commission’s reports), daily safety meetings and periodic reviews.
- Relevant to this accident was the Hazard Register section ‘Shotover River’. The Hazard Register noted several hazards specifically related to on-water operations, which are shown in Appendix 3.
Analysis Tātaritanga
Introduction
- The jet boat Discovery 2 was operating on the Shotover River with nine passengers on board when it made contact with a rock face in Skippers Canyon, resulting in a serious injury to one passenger and minor injuries to the remainder. The boat suffered moderate damage to the bow area.
- Jet boating is a high-risk activity that leaves very little margin for error when navigating at high speed in narrow channels and rivers. The consequence of an accident can be catastrophic when passengers are being carried. It therefore is essential that safety systems are in place and being followed to help reduce the risk of an accident occurring.
- The Discovery 2 was travelling at high speed through a section of the river in the canyon when a mechanical failure within the jet unit steering system caused a loss of control. This resulted in the bow of the boat making heavy contact with the canyon wall. The Commission found that the actions of the jet boat driver were not contributory.
- The following analysis examines the mechanical failure that caused the loss of control. It also considers the maintenance system that allowed the mechanical failure to occur, and the operator’s hazard identification and mitigation system.
Loss of control
- The jet boat driver lost control of the Discovery 2 because the stud-bolts fastening the steering nozzle assembly to the tailpipe of the jet unit broke and rendered the steering nozzle and reverse bucket ineffective (see Figure 12). As a result the boat lost steerage and could not be stopped before it hit the canyon wall.
- As discussed in section 2, the integrity of the bolted joint is dependent the stud-bolt being protected from experiencing cyclic loading by generating enough pre-tension within it. The pre-tension in the stud-bolt is achieved by tightening the nut with the required amount of torque. If the pre-tension is inadequate, the stud-bolt will experience fatigue.
- The failure analysis conducted on the broken stud-bolts found they had failed due to fatigue cracking. A close examination of the fracture faces (Figure 13) showed that the fatigue cracking was consistent with low pre-tension in the stud-bolt.
- The failure analysis report concluded that the stud-bolts had fractured due to fatigue cracking caused by insufficient torque being applied to the nuts and therefore inadequate pre-tension in the stud-bolts.
- The jet unit tailpipe and steering nozzle, including stud-bolts, washers and nuts, were all part of the HJ212 jet unit model. The manual for the HJ212 jet unit assembly contained prescriptive specifications, including the required torque for the various nuts and bolts fitted to the jet unit.
Maintenance
Safety issue: the operator’s planned maintenance programme did not ensure that the manufacturers’ specifications were met for the jet boat’s steering and control system
- The operator was subject to the requirements of Maritime Rules Part 82: Commercial Jet Boat Operations – River. Part 82 stated that “a commercial jet boat operator must have, and apply, a maintenance programme for every jet boat and propulsion unit”.
- The maintenance programme applied by the operator included maintenance checks and assurances that were prescribed based on the boat operating hours. For example, every 50 hours recorded on the engine would trigger the ’50-hour’ maintenance check, which was guided by the ’50-hour checklist’ (Appendix 1). The 50-hour checklist included a section of items to check on the HJ212 jet unit (shown in Figure 9).
- In accordance with the operator’s checklist, a torque wrench should have been used to check the tension on the bolts which fasten the reverse bucket, and the cotter pins. A torque wrench was not used to check other nuts in the jet unit assembly, including the stud-bolts that broke. The Commission was unable to establish when the torque on the broken stud-bolts had last been checked.
- The stud-bolts fastening the steering nozzle to the tailpipe were size M8 (a bolt that has a diameter of eight millimetres). The torque specified in the HJ212 manual for the M8 stud-bolts used on the jet unit was 12Nm (Newton metres). M8 nuts and bolts were used in various applications throughout the boat. However, they were not subjected to tightening using a torque wrench as they were generally considered to be ‘hand-tight’, an approach that the Commission found from interviews was not uncommon across the industry.
- A recommendation would have been made to Skippers Canyon Jet Limited to ensure that its maintenance system complied with all manufacturers’ instructions and guidance. However, since the accident the company has taken action to improve its Safe Operating Plan to ensure that all jet unit components are maintained to manufacturers’ specifications, which includes checking the torque on all nuts and bolts.
Hazard identification
Safety issue: the operator’s hazard identification system had not identified the risk that a system critical to the safety of the jet boat could fail
-
Maritime Rules Part 82, Section 1.20 – Managing Hazards (see Appendix 2) lays down the requirements for an operator’s hazard management system. It states, in part, that:
A commercial jet boat operator must meet its health and safety responsibilities under the Health and Safety in Employment Act 1992, by including, without being limited to, the following:
(a) the process used by the operator to identify the operational hazards that may cause harm to a person; and
(b) the process used by the operator to review operational hazards and how they are to be controlled, including how drivers are made aware of new hazards before drivers and passengers are exposed to them (for example, the day-to-day changes in river conditions); and …
- Section 1.20 of Part 82 primarily refers to hazards in the context they can be identified or controlled by jet boat drivers. That is to say, the hazards related to operating conditions faced by the jet boat driver on the day of operation.
- The hazards identified by the operator in the Hazard Register (Appendix 3) reflected the context of Section 1.20. Generally they related to river conditions and the drivers’ performance. For example, identified hazards included, but were not limited to, high and low water, ice, other river users and driver fatigue and training.
- The history of commercial jet boating accidents in New Zealand, especially the nature of those accidents in the late 1990s, resulted in a regulatory focus on jet boat operating conditions and driver performance and training.
- However, this accident demonstrates that the safety of a jet boat and its crew and passengers is also subject to significant hazards and risks not related to operating conditions or driver performance.
- The operator’s maintenance programme explicitly recognised that certain components were critical to the safe operation of the boat. This can be seen in the 50-hour checklist prompt that required a check of the torque of specified components. Also included in the maintenance programme was a Critical Parts Log, which listed the parts to be replaced at certain operating-hour-based milestones. Six of the 13 critical parts related to the steering and control of the boat.
- The proximate cause of this accident was a loss of steering and control due to a mechanical failure of the jet unit. Individual steering and control components were identified for increased scrutiny in the maintenance system, indicating that the steering and control system had been recognised as critical to the safe operation of the boat. Unfortunately, the mechanical failure of the steering and control system had not been identified as a hazard and therefore specific risk mitigation in the case of such an event was absent.
Risk control
- There are two categories of risk control: preventive risk control and recovery risk control.
- Preventive risk controls are put in place to prevent a negative consequence. For example, the operator had identified that ice in the river could cause a loss of power through the jet unit. The preventive risk controls put in place included checking the river for ice build-up, suspending commercial trips, and checking the jet unit intake before and after each trip.
- Recovery risk controls minimise the negative consequences of a realised hazard. Adventure tourism jet boating is a high-speed activity, often being undertaken in confined rivers with passengers on board. There is a very narrow margin of error, little scope for recovery when something goes wrong, and high consequences in the event of failure. Recovery risk controls include jet boat driver training in respect of accidents and emergencies, and the operator’s emergency response system.
- In this accident, the actions of the jet boat driver and the operator’s response to the accident were both efficient and effective, providing timely and appropriate aid to the driver and passengers.
- The safe operation of jet boats is heavily dependent on preventive risk controls, particularly driver training and the active analysis of river conditions. However, as noted above, the safety of a jet boat is subject to hazards and risks that are not related to operational conditions or driver training.
- Had mechanical failure of the steering and control system been identified as a hazard, the preventive risk controls may have led to increased scrutiny of the entire system, particularly critical parts relevant to the system.
- Although Part 82 does require an operator to carry out hazard identification and mitigation its context does not specifically prompt hazard identification of maintenance and safety critical systems.
- This accident was due to the mechanical failure of a system crucial to the safe operation of the boat. Hence the essential lesson of recommendation 104/99 remains pertinent, and therefore the Commission has made a recommendation to the Director of Maritime New Zealand that is applicable to Part 82.
Other potential safety factors considered
Liquid sealant and nozzle insert proud of bearing face contributing to fatigue of the stud-bolts
- As described in section 2, using a nut and bolt to clamp two components together is dependent on the two components bearing the compressive force imparted by the pre-tension in the bolt. This requires that the contact area between the two faces be maximised and incompressible, and the load transfer be uniform. The bearing should cover the entire bearing surface and not simply one small protrusion.
- The nozzle assembly described in section 2 included an insert into the nozzle. The failure analysis found that the insert was not fitting flush with the bearing face of the nozzle housing and was proud by up to 0.23 millimetres. The clamping arrangement between the steering nozzle and the tailpipe was therefore not optimal and may have contributed to fatigue in the stud-bolts.
- The manufacturers specifications for the HJ212 did not include a sealant being applied between the steering nozzle assembly and the tailpipe, but a liquid sealant had been applied within the joint.
- The nozzle assembly had been installed on the Discovery 2 in 2016 and had accumulated in excess of about 800 hours of cyclic loading before the stud-bolts broke. The engineering failure analysis found that the stud-bolts broke after about 200 hours of operation. Although possible, it seems unlikely that the sub-optimal bearing surfaces and liquid sealant contributed to the stud-bolts’ fatigue failure.
Survivability of the boat
- A significant recovery risk control available to jet boat operators is the survivability of the boats. Survivability is the capability of a boat to continue its mission and minimise injury to its occupants in the event of an accident or failure of some kind.
- The injuries sustained in this accident were due to passengers being thrown forward from their seats when the boat struck the canyon wall. The injuries included a broken leg for a passenger who was partially ejected from the boat. Other passengers had bruising and minor lacerations.
- Because the injuries were due to the occupants of the boat being thrown forward, one risk control would have been to install seatbelts to restrain them. The jet boat industry had considered the use of seatbelts, and in one case even trialled them. However, seatbelts were found to increase the risk to passenger safety in the event that passengers became trapped in a high-sided boat, it rolled over or it was subjected to a stern wave.
- The risk of being ejected from a boat is addressed in Maritime Rules Part 82, which requires that a boat’s side deck be a certain height above the seat. The Discovery 2 complied with that requirement, which likely prevented one passenger being completely ejected from the boat into the water.
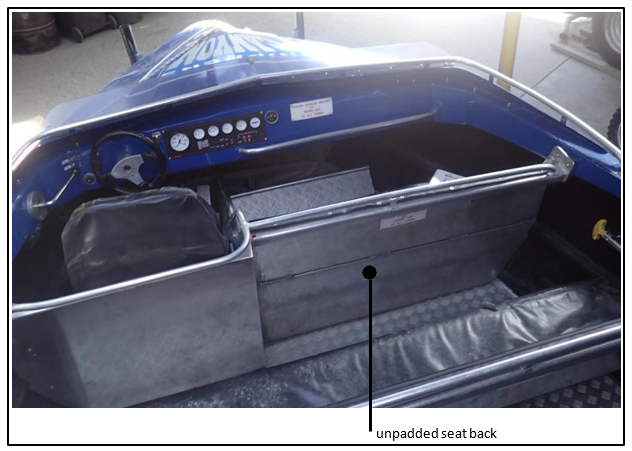
- Other recovery risk controls laid out in Part 82 are handholds for passengers, padding to cushion contact between them and the boat, and no “projections and sharp edges” that could harm passengers. The Discovery 2 was free of projections and sharp edges. However, it is likely that some injuries were aggravated when passengers were thrown into the unpadded seat backs in front of them, as shown in Figure 14.
- Although the Discovery 2 had been built in about 2000 and Part 82 had not been introduced until 2012, the boat had current certification, which found it complied with the rules. However, while the Maritime Rules provide a minimum safe standard, operators are still responsible for identifying and mitigating risks and hazards specific to their own operations and should endeavour to use that process to improve their safety standards over and above the minimum required.
Appendix 1. The operator’s 50-hour checklist
Appendix 2. Maritime Rules Part 82, Section 1.20
Appendix 3. The operator’s Hazard Register