In November 2016, the bulk carrier New Legend Pearl was about 125km east of Coromandel. A crew member working on a crane jib was changing his safety harness securing point when he fell 8 metres to the deck below. Paramedics helicoptered to the ship but were unable to revive him and he died from his injuries. Working at height is risky, so all crew should use suitable safety harnesses correctly.
Executive summary Tuhinga whakarāpopoto

- On the morning of 3 November 2016, the bulk carrier New Legend Pearl was east of Coromandel Peninsula on passage between the New Zealand ports of Bluff and Marsden Point. The crew were attempting to change a hoisting wire on one of its cargo cranes. Part-way through the task the hoisting wire snagged on the crane jib that was resting in its cradle, about eight metres above the hatch cover.
- One of the crew donned a safety harness and climbed up onto the crane jib, secured the lanyard of his harness around a luffing wire and walked along the jib to unsnag the wire. However, the lanyard prevented him reaching the snag, and he was in the process of transferring the lanyard to a different securing point when he lost his balance or slipped and fell eight metres to the deck below. He died from his injuries.
- The Transport Accident Investigation Commission (the Commission) found that it was about as likely as not that the locking mechanism for the safety harness hook was not engaged, which allowed the lanyard to roll or burst out of the hook when the crew member fell, and that the safety harness was not suitable for the intended task.
- The Commission also found that:
- the risk assessment conducted prior to the crew starting the wire replacement on crane number 2 did not fulfil the requirements of the operator’s safety management system, because it did not adequately identify and manage the risks associated with the task
- the repeat failures of the crew to comply with safe working practices when working at height and the acceptance of using a substandard wire on a working crane are indications of a poor safety culture on board the New Legend Pearl.
- The Commission identified two safety issues: the operator’s risk assessment process did not prevent the crew member working at height with an inadequate fall-protection system; and both the safety management system and the underlying safety culture on board did not meet industry good practice.
- The Commission made one recommendation to the flag state for the New Legend Pearl to address these safety issues.
- The key lessons arising from the inquiry are:
- working at height is a risky activity and all crew should use suitable safety harnesses that are fit for the intended tasks
- working at height is a risky activity that must be properly managed using a formal risk assessment methodology
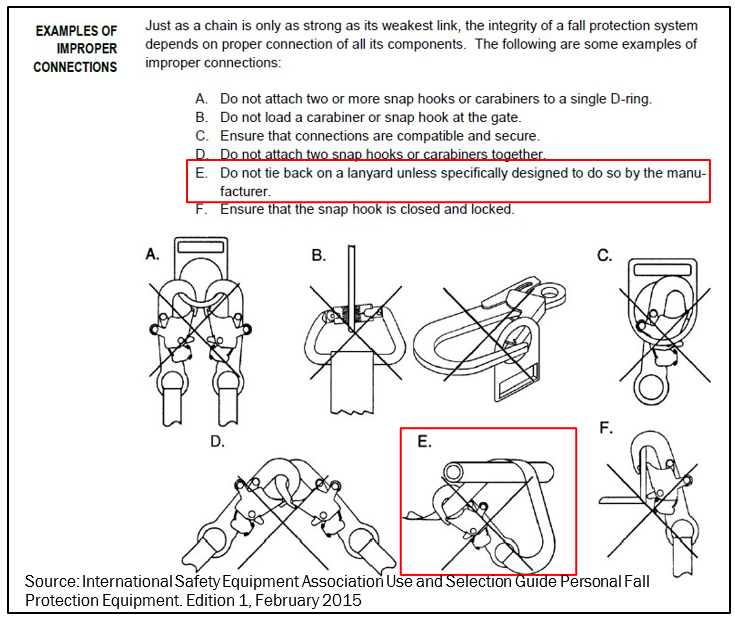
- attaching a safety harness by passing it through or around the securing point and back onto the lanyard is a dangerous practice that can result in inadvertent release unless the lanyard and hook are designed for that purpose.
Factual information Pārongo pono
Events leading up to the accident
- Prior to the accident the New Legend Pearl had called at the port of Bluff. The vessel had been delayed for several days; it was alongside the berth from 0100 on 26 October until 1454 on 31 October.
- At 0800 on 26 October, cargo operations commenced using the ship’s cranes, but after about two hours they were stopped because the stevedores observed what they thought was a crack in the structure of a crane.
- The crew went to check the crane and demonstrated that what appeared to be a crack was only grease. However, the port company had already reported their concerns about the condition of the cranes to MNZ. A maritime officer from MNZ issued a Notice of Imposition (Notice of Imposition of Conditions on the Use and Operation of a ship pursuant to sections 55 or 397 of the Maritime Transport Act 1994), dated 26 October 2016, which stated, ‘the four cargo cranes are not to be used for the lifting of any equipment or cargo’. Cargo operations were halted until the cranes could be inspected and declared structurally sound by a classification society surveyor.
- The vessel’s operator arranged with its classification society, BV, for a surveyor to attend the vessel and carry out an occasional cargo gear survey. There was a two-day delay waiting for the surveyor to arrive, during which time the crew took the opportunity to carry out rust removal and painting on the cranes.
- At about 1015 on 27 October, the port facility’s health and safety team were advised by stevedores that the crew on board the New Legend Pearl were not working safely. The health and safety officers boarded the vessel and witnessed the crew working at height, on the cranes, without full fall-protection equipment (see Figure 1). The ship’s duty officer was informed of their concerns and work on the cranes ceased.
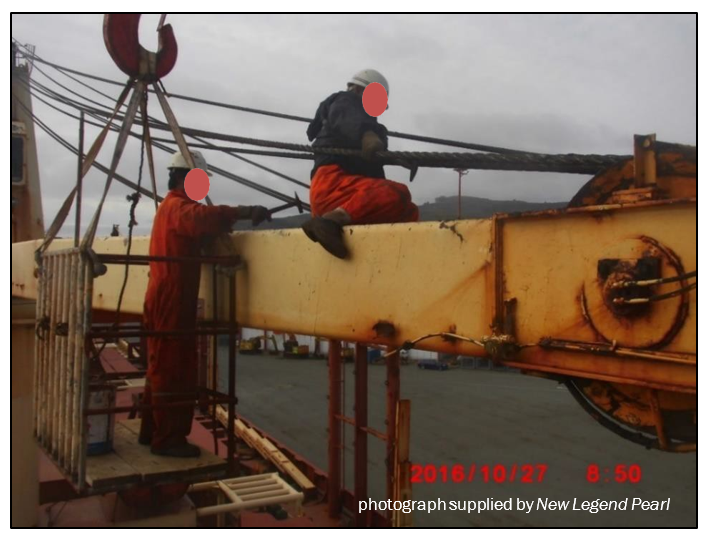
- At about 1730 on the same day, one of the port health and safety officers witnessed the crew once again working at height on the cranes without fall protection. The health and safety officer informed the master that under no circumstances should the crew be working without the proper personal protective equipment. The health and safety officer sent an online report on the unsafe work to MNZ.
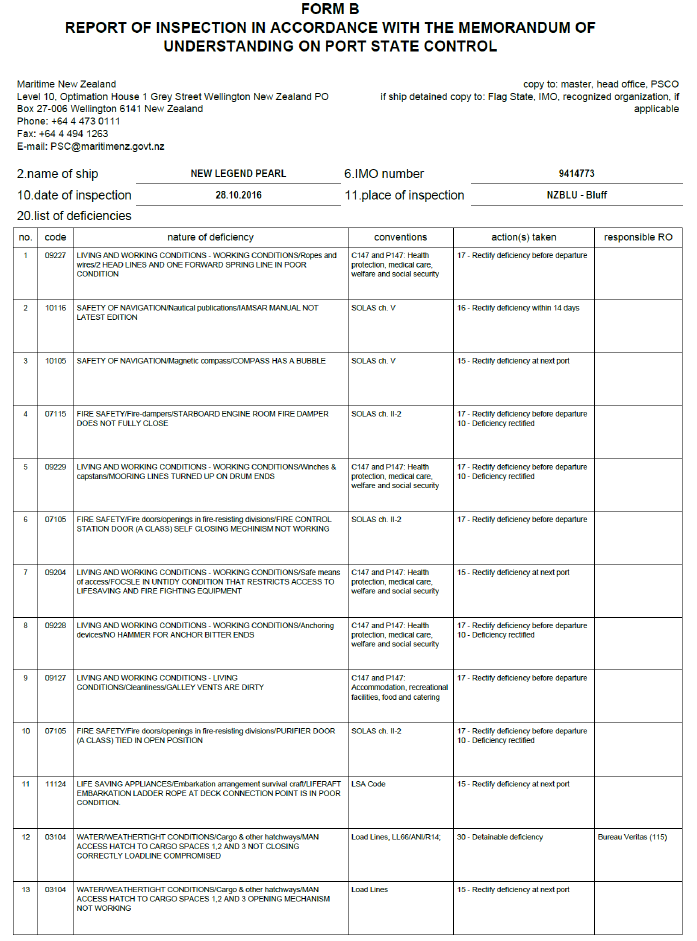
- On 28 October, an MNZ maritime officer conducted a Port State Control inspection (a Port State Control inspection is a safety inspection carried out on a foreign ship by an officer of the local regulator), and found several deficiencies that had to be rectified before the vessel could depart from Bluff.
- On 28 and 29 October, a surveyor from BV carried out an occasional cargo gear survey. Four recommendations were issued which had to be carried out by 15 December 2016.
- MNZ then issued a Notice of Withdrawal (Notice of Withdrawal of Impositions of Conditions on the Use and Operation of a Ship Pursuant to sections 55 or 397 of the Maritime Transport Act 1994) to remove the imposition. The deficiencies identified during the Port State Control inspection (see Appendix 2) had also been rectified, so MNZ released the vessel from detention.
- At about 1900 on 29 October, cargo operations resumed. However, the stevedores were unhappy with the condition of the hoisting wires on numbers 2 and 4 cranes (see Figure 2).
-
The following day the crew fitted a new hoisting wire onto number 4 crane, which was the only spare wire on board. This crane was prioritised because it was the only crane that could work cargo at number 5 hatch.
- Later that afternoon the master emailed the agent at Marsden Point, the vessel’s next port, to request a quotation for a new crane hoisting wire. The agent replied the following day, but no order was placed for a new wire. Cargo was still able to be loaded at Marsden Point with only three gangs (a gang is a group of stevedores working as a unit in handling cargo), and number 2 crane was not required.
- The master consulted the operator and a decision was made to replace the hoisting wire on number 2 crane with the old wire that had been removed from number 4 crane. The intention was to change the wire during the passage from Bluff to Marsden Point so that the cranes were fitted with the best available wires.
- At 1454 on 31 October, the New Legend Pearl departed Bluff for Marsden Point.

Narrative
- By the morning of 3 November 2016, the ship had endured three days of strong winds on its voyage to Marsden Point. The master and the chief officer discussed the weather forecast. Because the wind was still at Force 5 (Force 5 on the Beaufort wind scale is 17-21 knots), the master decided to not allow the crew to change the wire on number 2 crane that morning, but agreed that sea conditions might improve sufficiently by the afternoon. At the morning meeting the chief officer talked to the crew about the procedure for changing the wire.
- By the afternoon, the wind had decreased to Force 4 (Force 4 on the Beaufort wind scale is 11-16 knot) and conditions had improved sufficiently to allow the wire change to go ahead. The chief officer completed a risk assessment and the working-at-height checklist before the work commenced.
- At about 1330, the bosun, the ship’s carpenter and the deck crew assembled on deck to change the wire on number 2 crane. About half an hour later the chief officer joined the deck crew to supervise the work.
- The carpenter and two able seamen climbed onto the crane-house to release the old wire at its termination point. The wire was lowered to the deck, where the end was cut off neatly so that it could be connected to the new wire with a cable sock (see Figure 3).

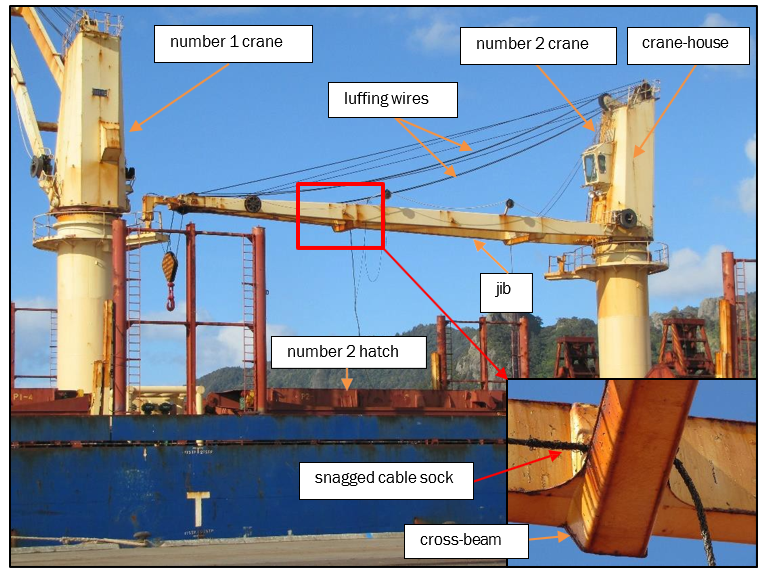
- The crew commenced heaving the connected wires through the hoisting-wire sheaves, but stopped when the cable sock snagged on the crane-jib cross-beam (see Figure 4).
- The bosun put on his safety harness and climbed up the ladder of number 1 crane and across to the end of number 2 crane’s jib (see Figure 4). He secured his safety harness lanyard around a luffing wire and walked along the jib to reach the point where the cable sock had snagged (see Figure 4).
- When the bosun reached the cross-beam, he could not reach the snag with his lanyard still secured around the luffing wire. He unhooked the lanyard to relocate it to a lower wire so that he could reach it.
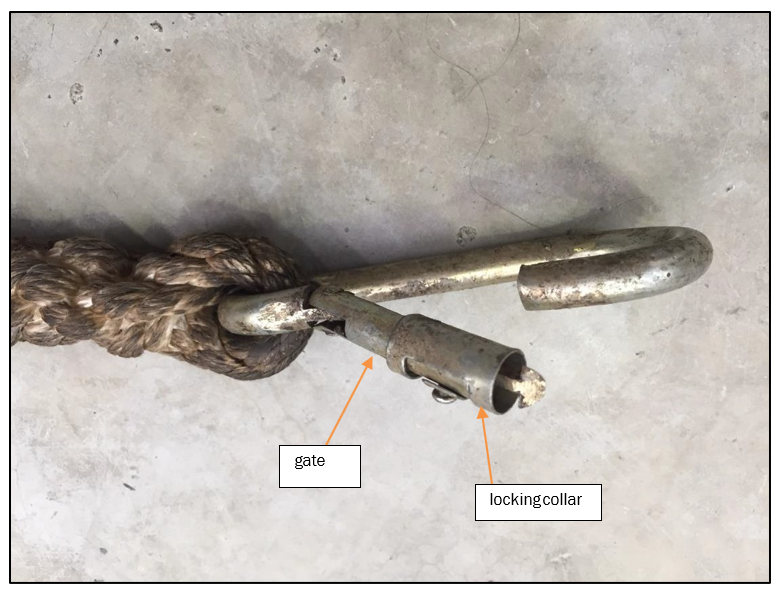
- At some point in the process of moving the lanyard between the luffing wires, he lost his balance and fell eight metres onto number 2 hatch cover. None of the crew could say for sure whether the bosun was clipped onto a luffing wire when he fell. The safety harness was intact but the gate (see Figure 8) of the securing hook was damaged.
- The bosun was unconscious and bleeding, so the chief officer immediately sent the crew to get first aid equipment. The ship’s carpenter remained with the bosun. The chief officer went to the ship’s office and called the master to report the accident and request a helicopter evacuation.
- At about 1730, the helicopter paramedic was winched on board and confirmed that the bosun was deceased. The New Legend Pearl continued on passage to Marsden Point.
The crew
- At the time of the accident there were 24 crew on board the New Legend Pearl. The minimum crew required by the safe manning certificate was 14. All of the crew originated from the People’s Republic of China.
- The master had commenced his seagoing career in 1993 and gained his master’s certificate of competency in 2008. This qualification was issued under the provisions of the International Convention on Standards of Training, Certification and Watchkeeping for Seafarers 1978, (STCW Convention), as amended. He had been sailing in the rank of master since 2009 and the New Legend Pearl was the first bulk carrier he had sailed on. Prior to joining the vessel he had spent one day at the company’s office being introduced to the company’s safety management system. A copy of the safety management system had been sent to him for reading before he joined the New Legend Pearl on 18 August 2016.
- The chief officer had been at sea since 2006 and had a chief mate’s certificate of competency issued under the provisions of the STCW Convention in September 2015. The contract on board the New Legend Pearl was his first appointment as chief officer. He had completed his previous contract as a chief officer under training and joined the New Legend Pearl on 2 March 2016.
- The bosun was 51 years old and had worked at sea for more than 30 years. He was the eldest crew member and he was well respected by the crew as an experienced seafarer. He had been found fully fit for sea service on 23 February 2016 and joined the New Legend Pearl on 26 February 2016.
The cranes
- The cranes were subject to an inspection regime carried out in accordance with the International Labour Organization’s Occupational Safety and Health (Dock Work) Convention, 1979 (No. 152), which requires specific tests and examinations of a ship’s lifting appliances. These requirements are written into New Zealand law through Maritime Rule Part 49, Ships’ Lifting Appliances. A foreign ship that is working cargo in New Zealand territorial waters must be able to produce evidence that the following tests and examinations have been carried out on every lifting appliance:
- tested by a competent person (‘Competent person’ means a person who is authorised to carry out testing and examination of ships’ lifting appliances and loose gear by the equipment manufacturers, a classification society, a testing establishment recognised by MNZ or another nation’s shipping administration) prior to first use and after any substantial repair or alteration, using proof loads at a specified factor of the safe working load of the lifting appliance
- re-testing of every lifting appliance at least once in every five-year period
-
thorough examination by a competent person at least once in every 12-month period.
These examination and test requirements are also reflected in the BV Rules for the Certification of Lifting Appliances Onboard Ships and Offshore Units (October 2011).
- The cranes on board the New Legend Pearl had been most recently tested in June 2015 and an annual thorough examination had been carried out in August 2016. The tests and examinations had been carried out or witnessed by the ship’s classification society, BV.
Risk identification and control
-
The Maritime Labour Convention 2006 (The Maritime Labour Convention 2006 is an international treaty adopted by the International Labour Organization. It sets internationally agreed minimum standards for the health, safety and welfare of seafarers and came into force in August 2013) was adopted by Panama and regulated by Executive Decree No. 86, 2013. The New Legend Pearl was subject to the requirements of this decree, which placed an obligation upon the owners:
… to adopt effective safety and health policies and programs of work, including an evaluation of risk, as well as training and education of seafarers, with the purpose of preventing work accidents, professional injuries or illnesses.
- The operator’s Risk Identification, Assessment and Control Programme established the methods of and requirements for risk identification, assessment and control.
- On board, the master was responsible for implementing the risk control plan, training relevant personnel on risk perception and control, and providing feedback to the operator about on-board risks.
- The operator’s risk control programme grouped risks into five categories ranging from unacceptable to ignorable.
- Working at height without safety controls presented an unacceptable risk and required the application of controls to reduce the risk to a tolerable level. A risk assessment plan was required, with special attention paid to specific work locations.
-
The operator expected the following factors to be taken into account when selecting risk control measures:
a) Where possible, elimination or complete elimination of the source risk;
b) If elimination is not possible, the risk should be actively reduced;
c) After all optional control measures have been considered, consideration may be given to personal protective equipment;
d) Consideration should be given to the establishment of contingency plans and crisis management, as well as the provision of appropriate emergency equipment.
- The operator also had specific instructions for working at height, which were applicable to any work performed at a point that could lead to a fall from two metres or more. The following steps were required to be completed prior to working at height:
- a detailed investigation of the work site
- developing a safe operation plan based on the weather conditions and operating environment
- explaining the safety procedures and precautions to the operating personnel
- designating a person or persons responsible for organisation and supervision.
Safety harnesses
- The safety harnesses provided to the crew were half-body harnesses that conformed with the Chinese mandatory national standard for full-body harnesses. This standard specified the requirements and inspection rules of personal fall-protection systems used in working at height for a total weight of no more than 100 kilograms. The harnesses were supplied to the vessel with lanyards and hooks already attached (see Figure 5).
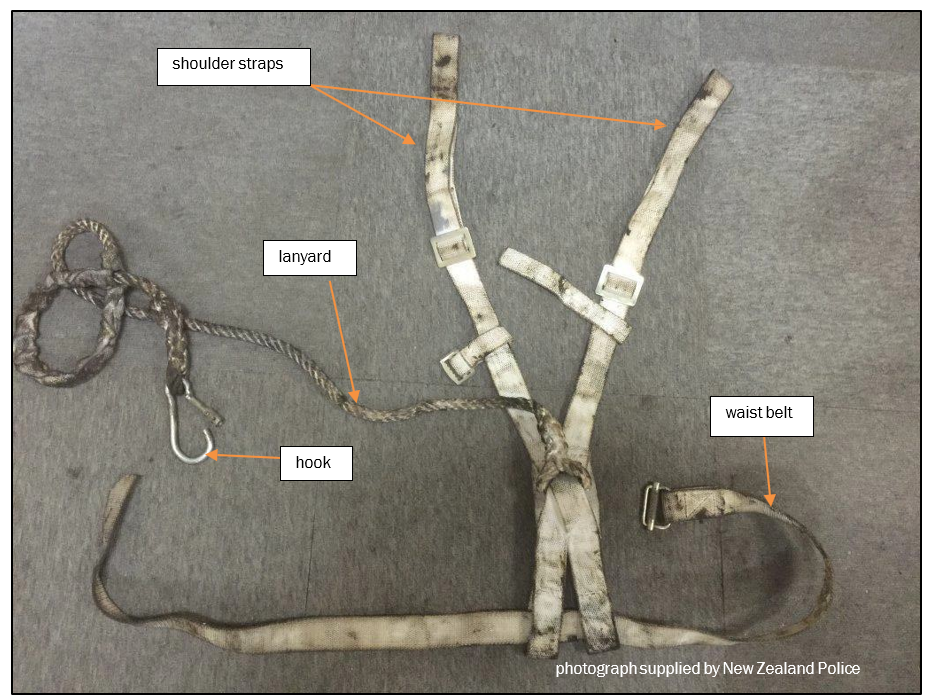
- The lanyards were made of 14-millimetre, soft polyester, three-strand, right-hand-lay rope, eye-spliced with three tucks. There was no marking to indicate that the lanyard met the mandatory Chinese standard for lanyards used in personal fall-protection systems.
- The hooks attached to the lanyards were mild-steel carbine hooks with manually lockable gates. The hooks were not stamped with any identification, safe working load or indication of meeting the recommended Chinese standard for connectors used in personal fall-protection systems.
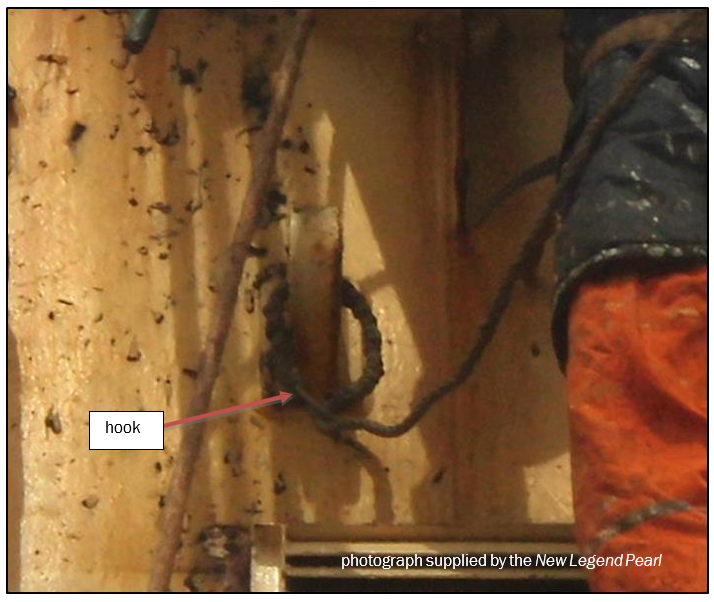
- The crew working on top of the crane-house were wearing safety harnesses as well as their normal personal protective equipment consisting of boiler suits, safety helmets and safety boots. They secured their safety harness lanyards to strong points by clipping each lanyard back onto itself (see Figure 6). There were no designated anchor points or safety wires specifically for the purpose of fall-protection.
Analysis Tātaritanga
General
- Working at height on a ship at sea can be dangerous, particularly on an open deck, due to unpredictable motion and slippery surfaces caused by salt deposits and sea spray.
- The following analysis discusses what happened and why, and the significance of two safety issues:
- the operator’s risk assessment process did not prevent the bosun working at height with an inadequate fall-protection system
- the safety management system and the underlying safety culture on board did not meet industry good practice.
The accident
- The bosun was working on top of number 2 crane’s jib when he fell eight metres onto number 2 hatch cover (see Figure 4) and suffered fatal injuries.
- He had climbed onto the jib to clear a snagged cable sock, but with the lanyard of his safety harness secured to a luffing wire he was unable to reach the snag below him.
- The bosun was seen to be in the process of moving the position of his safety harness lanyard hook when he lost his balance and fell. There were no designated fall-prevention anchor points on the cranes, so the crew regularly secured their lanyards to convenient fixings or wires (see Figure 6). The bosun had passed his lanyard around one of the crane’s luffing wires, then hooked it back onto itself.
- The practice of hooking a lanyard back onto itself is not recommended unless the lanyard and hook have been specifically designed for that purpose. This practice prevents the hook aligning with the force applied in the event of a fall, which means that it can also expose the gate of the hook to side-loading forces. The force required to roll out or burst out the gate of a hook is significantly less than the force the hook can withstand when pulled in direct alignment with the long axis of the hook.
- After the accident the gate on the bosun’s safety harness hook was found bent sideways and it no longer married up with the end of the hook (see Figure 8). The crew said that the safety equipment had been checked before they started changing the wire and had been found to be in a satisfactory condition. If this damage occurred during the fall, then the locking collar on the end of the gate should have been damaged as the gate was pulled sideways. However, the locking collar was not damaged. Therefore it is about as likely as not that when the bosun fell he had either removed the locking collar in preparation for removing the hook from the upper luffing wire, or had clipped onto the lower luffing wire but had yet to engage the locking collar. Any sideways force on the gate as the shock-load came onto the lanyard could have caused the gate to burst out and disconnect the harness from the anchor point.
Fall protection
Safety issue – The operator’s risk assessment process did not prevent the bosun working at height with an inadequate fall-protection system.
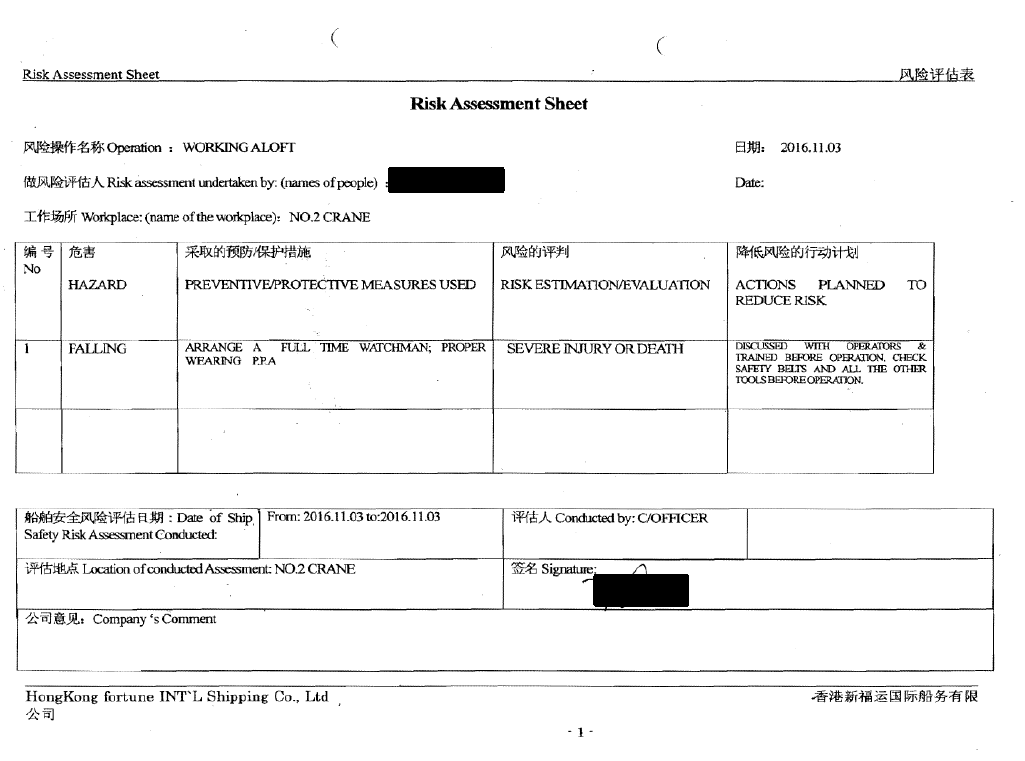
- The operator’s Risk Identification, Assessment and Control Programme required risks to be identified, categorised and controlled. On the day of the accident, a working-at-height risk assessment was carried out for working on number 2 crane (see Appendix 1) and a checklist was completed before the wire change commenced.
- The assessment sheet showed that the hazard of falling had been identified, the consequence of which was severe injury or death. The actions or control measures to reduce the risk were discussion, training, supervision and inspection of personal protective equipment before carrying out the wire change. A personal fall-protection system includes the harness, an anchor point and a lanyard and hook. All components must be fit for purpose and used correctly for it to be effective.
- The bosun’s actions to free the snagged wire were impromptu and not properly planned. The initial risk assessment had not distinguished between working at height on the crane-house and working out on the crane-jib. Both were high-risk activities. However, the chances of the bosun losing his balance and the need to transfer his securing point were greater out on the jib. A task-specific risk assessment should have identified that additional control measures were required.
- The location of the snag required an exposed traverse along the jib where there were fewer handholds, footholds and securing points. The jib was also more susceptible to the vibration and movement of the vessel. When the bosun lost his balance, the safety harness was the only thing preventing him falling to the deck, but it was not properly secured to a reliable strong point.
- The harness that the bosun was wearing had only one lanyard. The sample harness that the Commission removed from the vessel was fitted with two lanyards. The two-lanyard type was designed to provide security when the wearer is performing a task that requires them to move between anchor points.
- The operator’s instructions for working at height stated that, ‘the harness must be attached to a reliably secured device right above the worker’. However, there were no designated fall-arrest anchoring points on the crane-jibs. This meant that the bosun or any other crew member could only achieve an attachment by passing the lanyard around a luffing wire and back onto itself. The hooks on the harnesses provided on board were mild steel carbine hooks with manually lockable gates. The hooks were not stamped with any identification, safe working load or indication of meeting the recommended Chinese standard for connectors used in personal fall-protection systems. They were not of a type suitable for looping around an attachment point and back onto the lanyard. They were not therefore suitable for use when changing a wire or any other task requiring the crew to work out on the crane-jibs.
- A bulk carrier with its own cranes will, from time to time, require new crane wires to be fitted. This was not the first time that a wire and sock arrangement had become snagged on a cross-beam during this type of operation. A good risk assessment should have identified the need either to provide single securing points designed for the safety harnesses on board, or for the provision of harnesses with clips suitable for securing back onto themselves in the way the bosun rigged his harness. Equally, a good risk assessment should have identified the possible need to change securing points, and mitigated that risk by requiring a harness with dual securing lanyards. Either measure could have prevented the accident.
The decision to change the crane wire on passage
- The vessel’s schedule for testing and inspecting lifting appliances was up to date and the cranes had been surveyed by BV in order to confirm compliance with the International Labour Organization’s convention No. 152. When the stevedores at Bluff found numerous broken strands in the hoisting wires on numbers 2 and 4 cranes, they were right to question their condition and to not use the cranes.
- The crew agreed that the wires needed replacing, and the decision was made to change the hoisting wire on number 2 crane while the vessel was on passage from Bluff to Marsden Point. The intention was to have all of the vessel’s cranes rigged with the best wires available on board.
- However, there were no more new wires on board, so the crew used the damaged wire that had been removed from number 4 crane. The rules of BV required the crane to undergo a load test if a used wire was installed on the crane. Therefore, number 2 crane would have to have remained out of service at Marsden Point until an approved surveyor attended and witnessed a load test.
- It is of concern that the crew were considering placing a used wire that had previously been considered not fit for purpose onto a crane. There was no logical reason for doing so, except if they intended to use the crane with the old wire at subsequent ports outside New Zealand.
- Had a new wire been sourced and fitted, number 2 crane could have been operational before the New Legend Pearl left Marsden Point without the need for a load test. The wire change could have been carried out alongside using a personnel cage for working at height, and the risk substantially reduced.
Safety management and safety culture
Safety issue – The safety management system and the underlying safety culture on board did not meet industry good practice.
- The New Legend Pearl had a safety management system that fulfilled the occupational health and safety requirements of its flag state, Panama.
- However, a safety management system is only effective if it is being followed by the crew at all levels.
-
An effective safety management system must have operational procedures and instructions for high-risk work. Working at height in different areas of a vessel will present different risks not covered by standard procedures.
- The operator’s working-at-height instructions required a designated person to provide supervision and guidance to workers in ‘the correct use of harnesses, safety lanyards, helmets and other protective equipment’. The designated person was in this case the chief officer. However, there was also a duty of care imparted on every crew member, at every rank, to look out for their own safety and the safety of others.
- Working at height without wearing fall-protection equipment had been observed on board on two occasions when the vessel was in Bluff. The second occasion was in spite of the crew having been previously warned against the poor practice.
- The continued practice by the crew of working at height with so few safeguards suggests that they did not fully understand fall-prevention systems or the dangers associated with working at height. It is an indication that it was normal procedure to work at height in an unsafe manner. The unsafe practices for working at height, the failure to ensure that the safety equipment was fit for the proposed task of changing a crane wire at sea, and the acceptance of installing a used crane wire that had already been rejected as substandard by the stevedores in Bluff were all indications of a poor safety culture on board the New Legend Pearl.
-
The Code of Safe Working Practices for Merchant Seafarers, issued by the United Kingdom Maritime and Coastguard Agency, describes a good safety culture as:
… one where safety is an integral part of everything that is planned, discussed, done and documented. With good safety culture everyone in the company thinks about safety and new ways of improving it as a matter of course. They are constantly on the lookout for any unsafe acts or unsafe conditions, look out for each other, intervene to prevent accidents and incidents, actively share good ideas and always seek to improve.
- A recommendation has been made to the flag state Panama to seek improvements in the operator’s implementation of its safety management system on board its vessels, including the underlying safety culture.
Appendix 1. Risk assessment and risk control plan
Appendix 2. Port State Control Inspection