A pilot qualification, licence or aircraft-type rating does not in itself confer expertise. Pilots need to be familiar with the aircraft they are flying and their own capability as they gain experience. Pilots also need to ensure they are fully aware of the increased risks of flying at low level and monitor the performance of their aircraft accordingly.
Executive summary Tuhinga whakarāpopoto


What happened
- On Tuesday 15 December 2020, the pilot was using EC120-B helicopter ZK-HEK to fly their family and a friend from Rangiora to Kekerengu north of Kaikoura for lunch at a café. Flying towards the beach, the helicopter suddenly started yawing1 left and descending. The helicopter crashed on the beach.
- The two adults, including the pilot, were killed and the helicopter was destroyed. The three children were seriously or moderately injured but survived.
Why it happened
- The weather was suitable for the flight with a moderate northeasterly onshore breeze blowing. The pilot had not landed at the café before and was conducting a reconnaissance of the intended landing area. The helicopter slowed as it was turned towards the beach and downwind for a second pass at low level. The slow airspeed combined with increasing power caused the helicopter to suddenly yaw uncontrolled to the left, very likely startling the pilot.
- The rate of yaw increased, and the pilot was unable to regain control before the helicopter crashed onto the beach. The impact forces were determined to be non-survivable. However, the three children did survive, albeit with serious or moderate injuries, very likely because of their smaller physical size and mass.
- The investigation determined that the pilot did not pick up on the visual indications about the performance of the helicopter, resulting in it slowing at a critical phase of the flight. The pilot’s inexperience was a key factor.
- The Commission made no new recommendations.
What we can learn
-
A pilot qualification, licence or aircraft-type rating does not in itself confer expertise. Pilots need to be familiar with the aircraft they are flying and their own capability as they gain experience. Pilots also need to ensure they are fully aware of the increased risks of flying at low level and monitor the performance of their aircraft accordingly.
Who may benefit
- All pilots, including instructors and examiners, may benefit from the findings and lessons in this report.
Factual information Pārongo pono
Narrative
- At 1124 on Tuesday 15 December 2020, the owner and pilot (the pilot) of ZK-HEK, an EC120-B helicopter (the helicopter), took off from the pilot’s home base near Rangiora. On board were the pilot, the pilot’s partner, their two children and a friend of one of the children. The purpose of the flight was to take the family to a café at Kekerengu, 50 kilometres (km) northeast of Kaikoura for lunch. The pilot had earlier called the café to confirm the weather conditions were suitable for the flight.
- The pilot initially flew to Rangiora Aerodrome where they uploaded 200 litres of fuel. The helicopter left Rangiora at 1138, with the pilot flying north, inland of Cheviot, before reaching the coast about 10 km north of Kaikoura. Near the Clarence River mouth the pilot started a shallow descent from about 2000 feet (600 metres (m)) above mean sea level (amsl) towards Kekerengu.
- At 1237:45, the pilot started manoeuvring the helicopter seaward of the coast, to a position about 250 m offshore (400 m east of the café). The helicopter had a groundspeed of about 75 knots (135 kilometres per hour (km/hr)) as it crossed the coastline. The helicopter entered a left turn soon after passing abeam the café, remaining seaward of the coast. This put the café and landing area on the right side of the helicopter, the side the pilot was seated (see Figure 3. The tracking information was sourced from the onboard Garmin GPS and TracPlus™ tracking systems and Airways New Zealand’s tracking data. The EC120-B helicopter pictured in the diagram is not to scale but demonstrates the orientation of the helicopter relative to the wind direction as it conducted the second orbit).
- The helicopter initially remained level at about 300 feet (90 m) amsl in the early stages of the left turn. After passing abeam the café flying south the helicopter descended to about 200 feet (60 m) amsl. The helicopter continued in the left turn, with the turn tightening and the groundspeed of the helicopter reducing. As the helicopter turned left towards north for a second time, the groundspeed had reduced to about 25 knots (about 45 km/hr). The helicopter was now between 150 and 165 feet (45–50 m) amsl.
- Witnesses at the café and in the local area then saw the helicopter continue the left turn back towards the beach for a second time. As the helicopter approached the beach the witnesses described it starting to spin to the left. The rate of spin increased, and the helicopter then descended rapidly to crash on the beach at about the low tide mark.
- Witnesses immediately rushed to the helicopter to render assistance. The witnesses gained access to the helicopter through the doors and broken front window and removed the occupants. The witnesses, along with the help of several locals who had arrived shortly after, provided first aid until emergency services arrived. The three children were taken by air ambulance to hospital and treated for moderate-to-serious injuries. The pilot and pilot’s partner did not survive.

Personnel information
Pilot
- The pilot, aged 60 years, started flying training on helicopters in January 2019, nearly two years before the accident. All of the pilot’s early flying was on a Guimbal Cabri G2, a two-seat light helicopter. The pilot purchased a Cabri G2 soon after starting flying lessons. The pilot was issued a private pilot licence (helicopter) (the licence permitted the pilot to carry passengers, but not conduct commercial operations) on 5 March 2020, having accrued 84.5 hours of flight time by this stage (the pilot’s next check, a biennial flight review or BFR, was therefore not due until 5 March 2022). The pilot continued to gain experience and did additional training with an instructor after the issuing of the licence.
- In mid-2020, the pilot was seeking a larger helicopter and initially trialled and then purchased ZK-HEK, an EC120-B helicopter. The pilot obtained an EC120-B type rating on 31 July 2020, having flown 7.7 hours on the type, including transit time. After leasing out the Cabri, the pilot then flew only ZK-HEK. Shortly before the accident flight, the pilot had a second set of flight controls installed so they could undertake further training.
- At the time of the accident the pilot had accrued a total of 170 flying hours. The pilot’s logbook recorded 81 hours of dual instruction (flying with an instructor) and 89 hours as pilot-in-command. The pilot had flown 32 hours on ZK-HEK.
Pilot medical information
- The pilot held a class 2 medical certificate valid until 27 May 2022. The certificate required the pilot to wear spectacles. There were no known medical conditions identified that may have contributed to the accident. Commission investigators interviewed several witnesses who had interacted with the pilot during the morning of the accident. None of the witnesses reported any concerns about the pilot’s health or fitness to fly. Photographs taken shortly before departing on the flight, show the pilot wearing glasses and a baseball cap.
- The pilot’s autopsy results were negative for any performance-impairing substances and did not identify any health issues that may have contributed to the accident. The injuries sustained were consistent with the pilot operating the flight controls at the time of impact.
Other occupants
- The other occupants in the helicopter at the time of the accident included a 12-year old in the front left seat, the pilot’s partner in the rear left seat, an 11-year old in the rear centre seat and a five-year old in the right rear seat.
Aircraft information
- ZK-HEK was a Eurocopter (now Airbus Helicopters) EC120-B helicopter (the EC120-B was nicknamed the Colibri or Hummingbird), serial number 1023, constructed in December 1998. The helicopter was imported into New Zealand in February 2004 and had several owners before the pilot took possession on 9 October 2020.
- The EC120-B is a five-seat, high-performance, light-to-medium weight helicopter (Intermediate helicopters are considered to be between 3500 and 7000 pounds (1590 and 3175 kilograms)), powered by a single Turbomeca Arrius 2F turboshaft engine. The EC120-B is certificated for five seats, two in the front and three in the rear of the cabin. The pilot is typically seated in the front right seat, but with a second set of flight controls installed it could also be flown from the left seat.
- The EC120-B was fitted with a Fenestron type of tail rotor. See paragraphs 2.58 to 2.65 for further discussion on this tail rotor. Some 700 EC120-Bs were manufactured between 1995 and 2017 (Including the H120 variant).
- The helicopter was issued a certificate of airworthiness in the standard category after arrival in New Zealand. The certificate was non-terminating, provided the helicopter was maintained and operated in accordance with the prescribed documents. A review of the maintenance records for the helicopter recorded it was maintained as required.
- The last scheduled maintenance check on the helicopter before the accident was a 500-hour/12-month inspection carried out on 21 July 2020. At the same time, the then owner took the opportunity to replace the engine with another Turbomeca Arrius 2F engine, serial number 34021. A review of airworthiness was signed as having been completed on 22 July 2020.
- On 11 August 2020, a ‘pre-purchase inspection’ of the helicopter was undertaken at the direction of the pilot. This included an engine ground run to check engine parameters.
- The technical log for the helicopter was not recovered after the accident (a technical log provides a running written record of daily flying hours and serviceability state). The last entry in the aircraft maintenance logbook was on 9 November 2020. This was for a scheduled tail rotor re-torque check. It was calculated from this and the pilot’s logbook that the helicopter flew a further 4.3 hours until the accident, the helicopter having flown a total of 2626 hours at this time. The helicopter was therefore determined to have some 27 hours to run until the next scheduled maintenance check. At the time of the accident there were no outstanding airworthiness directives or service bulletins from the manufacturer. There were also no recorded or reported concerns about the performance of the helicopter.
- The helicopter had a recorded basic weight of 1070 kilograms (kg) and a maximum certificated weight of 1715 kg. Using the known weights of each of the occupants (obtained from medical and hospital records), and assuming a full fuel load at Rangiora, the helicopter was calculated to have weighed 1612 kg and was within the approved centre of gravity range as it started its flight north.
Meteorological information
- On 15 December 2020, a strong anti-cyclone was covering the country. A weak front was approaching the South Island, but this had yet to affect the weather north of Invercargill.
- The Meteorological Service forecasts for the coastal areas between Wellington and Christchurch over the duration of the flight predicted northeasterly surface winds of 5–10 knots, near unlimited visibility and no cloud.
- The automated weather report for Kaikoura Aerodrome issued at 1230 recorded the surface wind as 040° at 9 knots, varying between 320° and 070°. Visibility was 19 km, and the temperature 18°C with no cloud detected. The conditions remained similar for the next few hours. The weather reports for Wellington, Woodbourne (Blenheim) and Christchurch all recorded similar light northeasterly surface winds.
- Witness accounts, video recordings and several farm and vineyard weather stations all reported or recorded similar conditions. These included a light-to-moderate onshore breeze from the northeast with no cloud present. The wind was strong enough to generate ‘white-caps’ (about 10–15 knots, 20–30 km/hr).
Recorded data
- The helicopter was fitted with Garmin GPS and TracPlusTM navigation and tracking systems that recorded its flightpath. The flightpath of the helicopter was also recorded by Airways New Zealand’s tracking systems. However, Airways’ recording of the flight was intermittent at lower altitudes. The tracking systems, supported by witness observations, provided an accurate record of the helicopter’s flightpath for the duration of the flight.
Flight recorders
- The helicopter was not fitted with a flight data recorder or a cockpit voice recorder, nor was it required to be. However, the helicopter was fitted with a Vehicle and Engine Multifunction Display (VEMD), which is designed to record a range of engine-related parameters, including any exceedances.
- The VEMD from the helicopter was badly damaged in the accident. The VEMD was removed and sent to the Bureau d’Enquêtes et d’Analyses (BEA), the French Bureau of Enquiry and Analysis for Civil Aviation Safety, to determine if any information could be extracted (BEA is the representative for the state (France) in which the helicopter and engine were manufactured). The BEA was able to download the engine performance data for the last 30 flights. The data identified nothing unusual for the 30 flights, including the accident flight. There were no recorded engine exceedances or malfunctions.
Video recordings
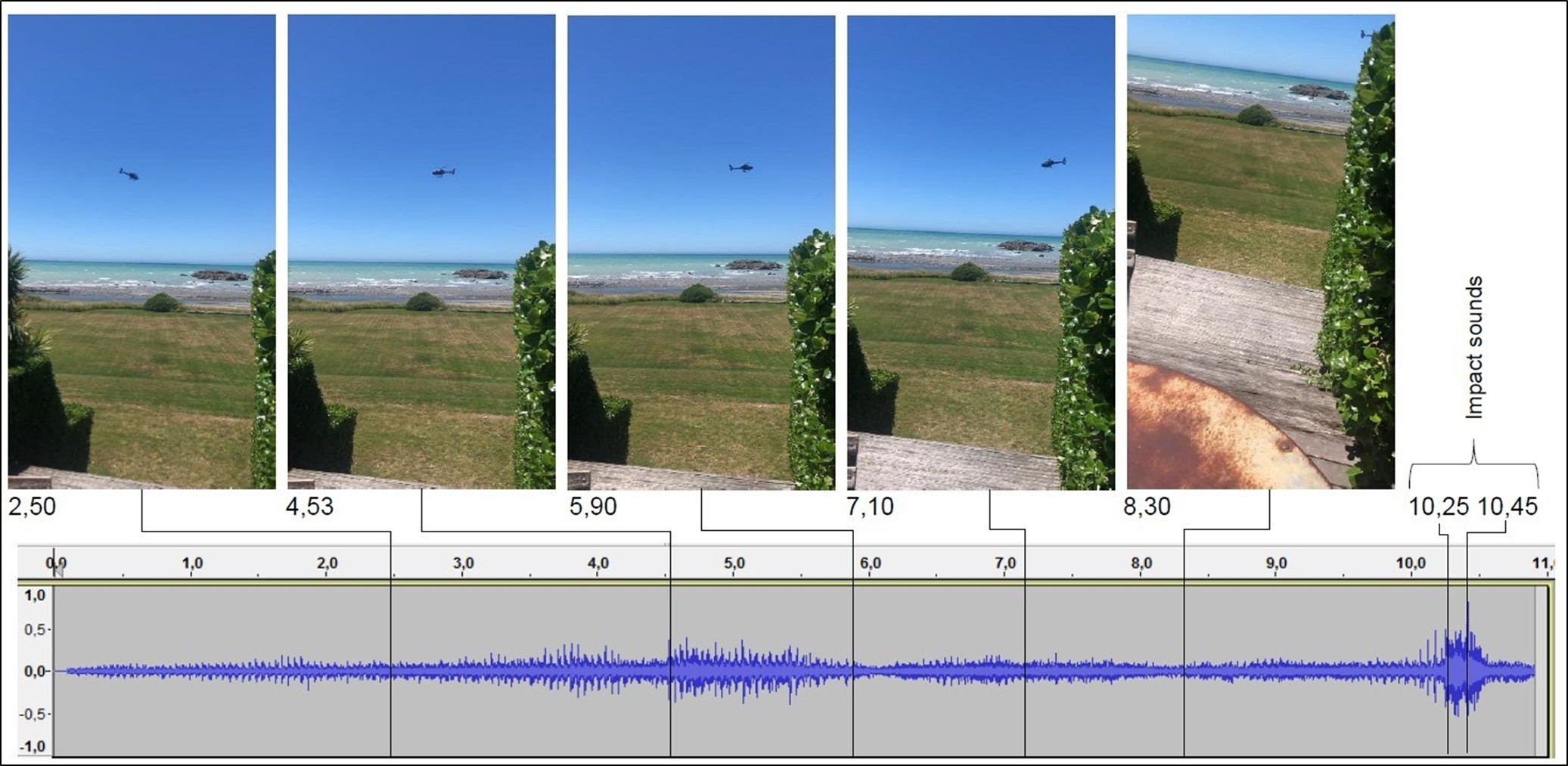
- Two witnesses to the accident collectively took three short video clips of the helicopter as it approached the beach, and as it started to spin and descend onto it. The two witnesses were on the eastern side of the café and had an unobstructed view of the helicopter until it disappeared behind some bushes.
- The three video recordings also included audio. The final video captured the sound of the helicopter as it descended behind the bushes and crashed on the beach. The audio clips were analysed to identify, among other things, the main rotor and tail rotor speeds (see figure 4).
Site and wreckage information
Site
- Helicopters regularly landed on the grass area adjacent to the café. The grass area was bounded by the café and trees to the west and south, and the beach and low bushes to the east and north. The grass area was large enough to land at least six helicopters, more with some coordination. There were no other helicopters on the landing area at the time of the accident and, according to witnesses, the grass area was clear of any café patrons or other people.
- The helicopter had crashed on the stony beach in front of the café, below the high-tide mark and just above the low-water mark. The helicopter, after hitting the beach, had come to rest on its right side. Witnesses who rendered assistance reported removing some of the panels or doors from the left side to gain access. They were also able to partly enter through the open front of the helicopter. The panels were later collected and secured.
- Because of the incoming tide, the helicopter was towed by witnesses and police some 40 metres across and up the beach. The wreckage was covered with tarpaulins and the site secured until the arrival of Commission investigators the next morning. The Commission was provided with images of the scene taken during the moving of the helicopter.
Wreckage
- Initial examination of the wreckage identified that the main area of damage was at the forward section of the helicopter. The front of the helicopter had broken away from the cabin above the front two seats. The floor of the helicopter remained attached but was deformed in several places. The instrument panel remained attached by its wiring only.
- One of the three main rotor blades had separated from the rotor head during impact. This was found washed up on the beach some 110 m to the north, the current moving in this direction. The outer portions of the two remaining blades were severely damaged, with blade fragments found washed up along the beach. Alerted by a witness, a main rotor blade tip weight was found below the guard rail of a road bridge some 230 m west of the accident site. The tip weight had penetrated the guard rail before falling onto the surface below. Otherwise, all major or critical components of the helicopter were accounted for at the site.
- While there was birdlife about the site, no evidence of a bird strike on the helicopter was found. A search of the general area located one dead seabird. The bird was intact and appeared to have been dead for several days. The video recordings showed no birds near the helicopter.
- The helicopter was lifted upright for safer access and eventual removal (see figure 5). The fuel tank was confirmed intact and still contained fuel. Nearly 300 litres were later drained from the tank. The fuel was determined to be of the correct type with no identifiable contamination. The fuel supplier for the installation at Rangiora Aerodrome confirmed that following the accident the installation was examined and that testing of the fuel found no anomalies.
- The emergency locator transmitter (ELT) had been removed and the helicopter battery disconnected. Helicopter emergency response personnel were reported to have performed these functions after their arrival on scene. See paragraphs 2.50 and 2.51 for further information.
- The wreckage was removed from the site and taken to the Commission’s technical facility for further detailed examination.

Examination
- Both landing gear skids were splayed outwards and had broken at their rear cross-tube attachments, which were bent backwards. Scrape marks along the right side of the fuselage were consistent with the helicopter being towed up the beach on its right side.
- The tail boom was still attached but displayed crumpling near the fuselage attachment area and sagged downwards. The tail rotor drive from the transmission was broken at the forward end of the tail boom. There was rotational scoring in this area, indicating the drive was turning at the time of separation.
- The empennage, containing an enclosed Fenestron tail rotor, was mostly undamaged. There were some score marks on the inside of the fairing surrounding the tail rotor blades where the tips of the blades had rubbed. There was also some damage on the fairing where a rope had been attached to tow the wreckage up the beach. There was no damage to the tail rotor blades.
- The main rotor head displayed rotational damage consistent with the main rotor turning at speed at the time of it striking the beach. The transmission mounts were intact but had bent from excessive movement of the main rotor and transmission.
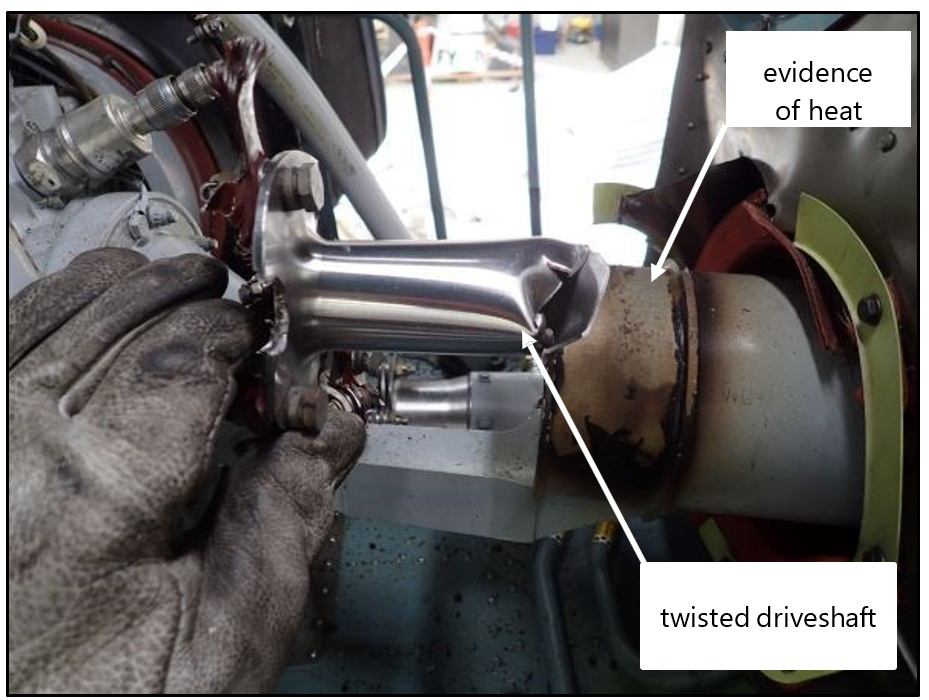
- The coupling between the engine and the transmission, termed the main gear box on the EC120-B, had broken. The direction of twisting of the coupling components was consistent with the engine continuing to try to drive the transmission (which in turn drives the main and tail rotor) until separation. There was evidence of heat damage at the engine end of the coupling as the now unrestrained engine oversped until it stopped. This was consistent with witness reports of hearing a high-pitched noise immediately after the accident and a light-coloured smoke coming from the engine bay area for a few minutes afterwards. There was no other evidence of fire (see figure 6).
- Commission investigators checked the magnetic chip plugs for the engine, transmission and tail rotor oils . The plugs are designed to collect any fine metal material carried in the oil that may indicate a failure of a component. An accumulation of material will result in an electrical circuit being made, activating a caution light to alert the pilot. The plugs were clear of any contaminants.
- Commission investigators confirmed the integrity of the cyclic and collective flight controls, despite the control rods being broken under the cabin floor where the floor had folded upwards. The operation of the tail rotor pedals corresponded to the correct movement of the tail rotor blades. The three hydraulic servocontrols for the flight controls were all intact with no evidence of deformation or leakage.
- The right set of tail rotor pedals were in their usual operating position, while the left set of pedals were in their fully extended position. This position would normally be used to help keep them clear of a passenger seated in the front of the helicopter, or for a very long-legged pilot.
- The collective lever was found in the partially up position and the engine throttle was found in the fully ON position. The flight and engine instruments provided no useful information.
Cabin and seating
- The cabin floor was severely distorted. There was an approximately 30° bend upwards forward of the bulkhead at the rear of the cabin. The three seats across the back of the cabin had also been bent upwards. Forward of this, in line with the rear of the front two seats, the floor was bent downwards by about 80° (this was when the helicopter was suspended by the rotor head). The two front seats remained attached to their floor mountings but had been forced over to the right by about 15–20°.
- The seat belts were all found intact but undone. According to witnesses, the belts had been released to help extract the occupants. The seats belts were checked and found to operate as designed.
Survival aspects
- The helicopter was fitted with an ELT designed to activate in a heavy impact. The ELT activated as intended with the Rescue Coordination Centre New Zealand receiving an alert signal at 1240. This, along with numerous 111 calls, resulted in activation of the emergency services that attended, including the Police, St John, Fire and Emergency New Zealand and helicopter rescue. The ELT and helicopter battery were disconnected soon after the arrival of the first rescue helicopter.
- At the request of the Commission, the three video clips, plus detailed measurements and images of the cabin and seating, were passed to Airbus Helicopters through the French BEA . Airbus undertook a review of the evidence to assess the damage sustained to determine the likely forces involved and the survivability of the accident. Airbus produced a report to this effect, which was reviewed by the BEA and provided to the Commission. Elements of that report have been incorporated into this report.
Helicopter control
- A helicopter generates lift using its main rotor blades, the blades acting much like the wing of an aeroplane. A pilot controls the direction of the lift or rotor thrust, and therefore the direction of flight, by the use of a cyclic control. To move forward or back the cyclic is moved forward or back. The more the cyclic is moved in a certain direction, the faster the helicopter will move in that direction.
- The amount of lift generated by the main rotor is determined by the pitch of the main rotor blades, which are in turn controlled by the pilot’s collective lever (the main rotor is designed to operate within a specific speed range. Engine power is used to help ensure that speed is maintained. For the EC120-B, the normal operating range was 390–415 rpm, with an optimum of 412 rpm for the cruise). As the main rotor is tilted in the direction the pilot intends to move, more lift or rotor thrust is required to prevent the helicopter from descending. The greater the rotor thrust required, the greater the amount of engine power needed to ensure the main rotor remains within its operating parameters.
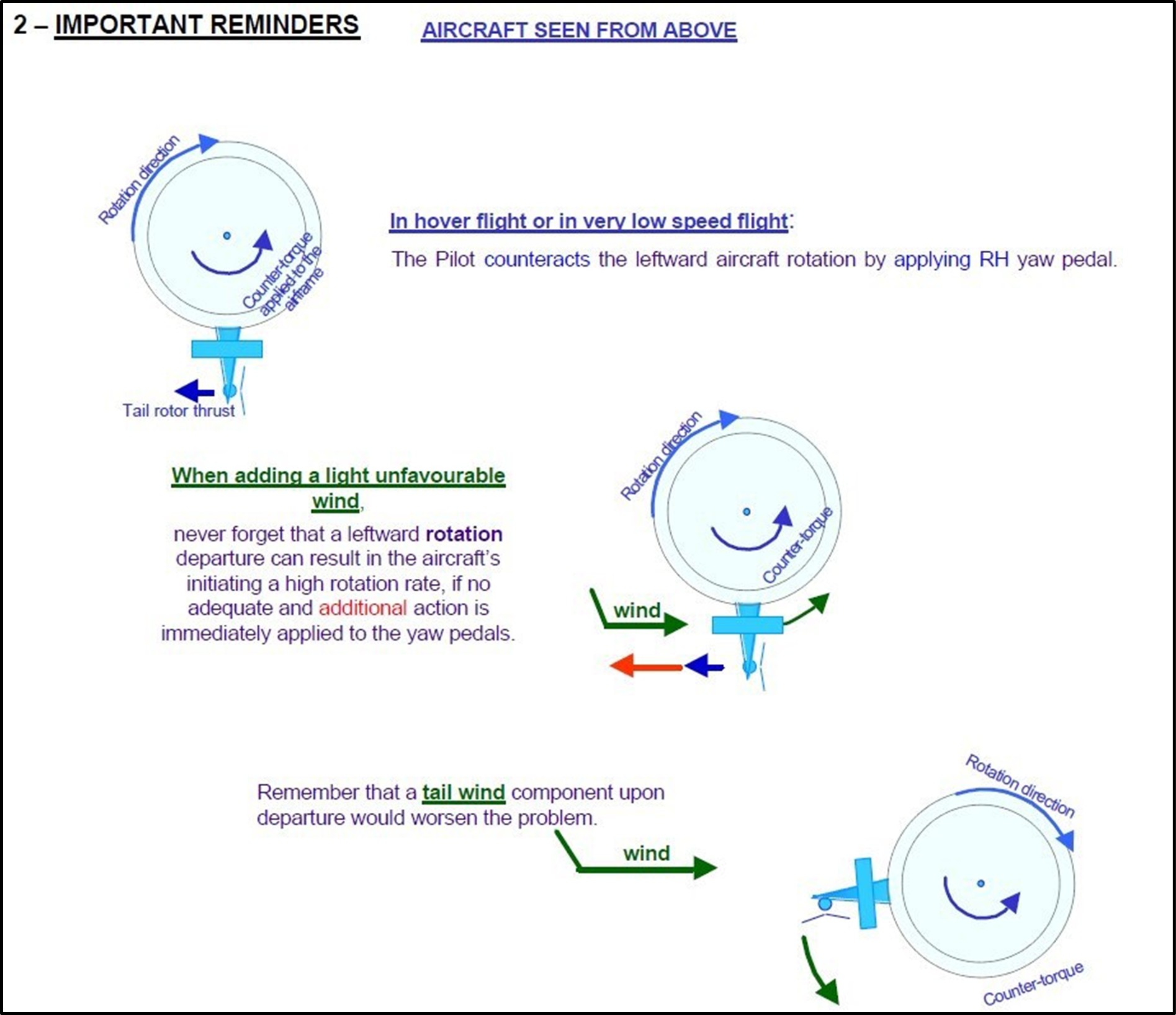
- The main rotor is driven from a single point that generates a torque reaction, which causes the fuselage to yaw or turn in the opposite direction to the main rotor. For the EC120-B, the main rotor rotates clockwise when viewed from above. The fuselage would therefore yaw left when power was applied (the main rotor blades of a large percentage of European helicopters, mainly French-manufactured helicopters, rotate clockwise, while the main rotors of all North-American-manufactured helicopters rotate anti-clockwise). The greater the power, the greater the torque effect. To manage this a pilot uses the tail rotor to generate a counter force. The tail rotor thrust is controlled through the tail rotor pedals, also called anti-torque pedals.
- For the EC120-B, to maintain the same heading as power is increased a pilot needs to increase right pedal input, most strongly in the hover or at low airspeed. At higher airspeeds the vertical fin at the rear of a helicopter provides a slipstream effect and mitigates the requirement for large pedal inputs.
- With experience the need for pedal input becomes more natural and intuitive: a pilot instinctively anticipates pedal changes as they increase or decrease power. With less experienced pilots pedal inputs can be mechanical and often after the helicopter has started to yaw. Greater pedal input is therefore required to return the helicopter to its original heading.
Unanticipated yaw
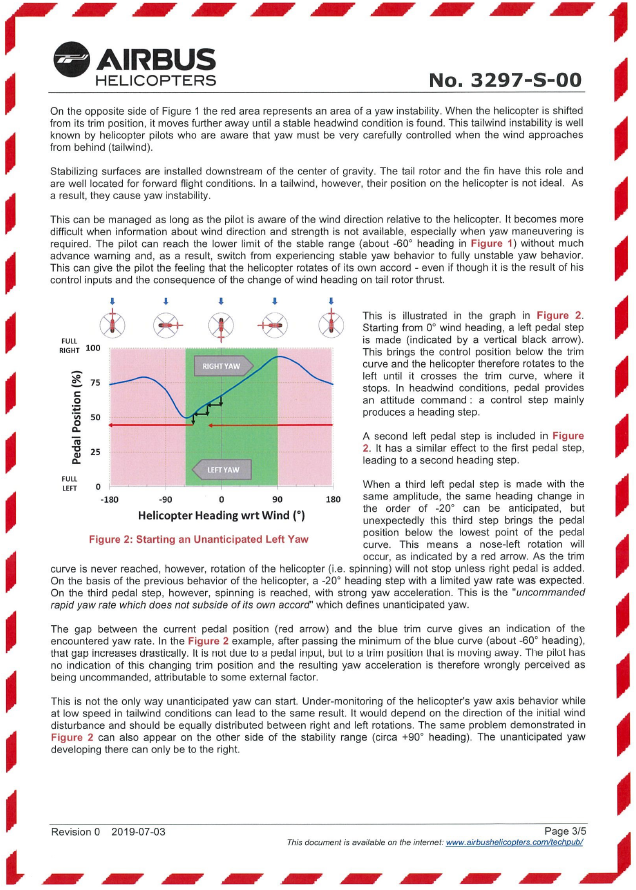
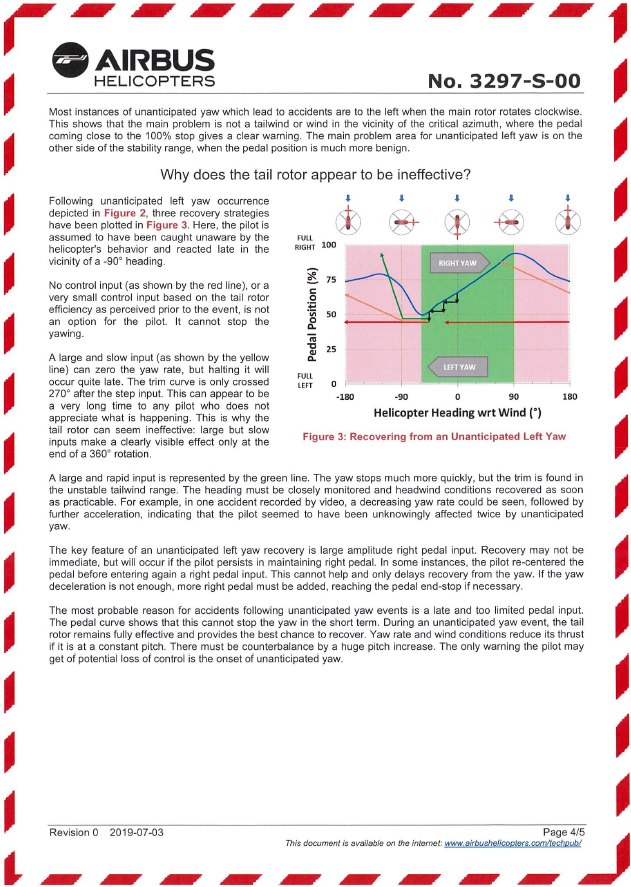
- Unanticipated yaw, sometimes referred to as uncommanded yaw or loss of tail rotor effectiveness (LTE) (the term LTE was first by the US Army), is the term used to describe the unexpected and sudden rotation of a helicopter about its vertical axis (the term ‘unanticipated yaw’ is preferred as the yaw is unexpected despite the tail rotor continuing to provide thrust). A single rotor helicopter, when compared to a twin rotor helicopter, is more susceptible to unanticipated yaw through a combination of high-power-generating, high-main-rotor torque, low airspeed and adverse relative wind. For a helicopter like the EC120-B, the unanticipated yaw would be to the left as viewed by a pilot.
Fenestron tail rotors
- The EC120-B helicopter, like the Cabri G2 the pilot was initially trained on, was fitted with a Fenestron tail rotor. The Fenestron is a shrouded type of tail rotor mainly found on French-manufactured helicopters. By comparison, a conventional tail rotor has exposed blades, typical of North American manufacturers. There are advantages and disadvantages to both types.
- To support pilot training on the Cabri G2, the manufacturer had produced a range of training materials on flying with Fenestron-equipped helicopters. The material noted that the Fenestron on the Cabri G2 was very powerful but behaved differently from a conventional tail rotor. Pilots were told to remember:
-
if rotor rpm is in the green, full right pedal will stop spinning to the left
-
excessive right pedal cannot cause any harm, NEVER hesitate to push FULL RIGHT PEDAL
-
be particularly careful when wind comes from the right side during the approach
-
anticipate the power increase and the loss of fin efficiency, NEVER let the nose go to the left (bold emphasis in the original).
An additional note advised that “25% of all accidents are due to insufficient right pedal input leading to loss of control in yaw.”
-
- The organisation that trained the pilot held copies of this material and advised that they had formed part of the pilot’s training.
Safety advice
Eurocopter/Airbus Helicopters
-
On 4 February 2005, Eurocopter issued Service Letter No.1673-67-04, about yaw control of helicopters with a main rotor rotating clockwise (service letters were typically emailed to registered recipients, which included the training provider. It was unknown whether the pilot was on the mailing list). A similar service letter was issued at the same time for helicopters with main rotor rotating anti-clockwise. Both letters referred to the Fenestron tail rotor, stating that:
With a Fenestron, when changing from cruise to hover flight (bold emphasis in the original), be prepared for a significant movement of the foot to the right (the second service letter referred to the left not right).
Insufficient application of pedal would result in a leftward rotation of the aircraft during the transition to hover
-
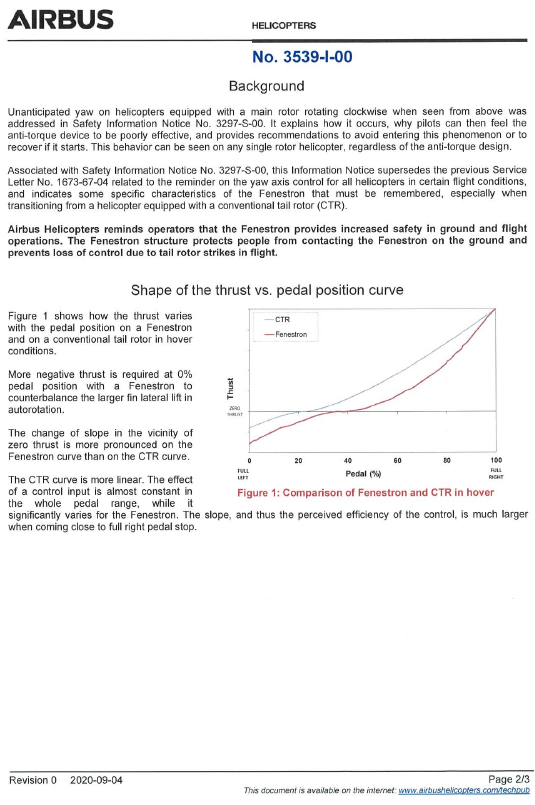
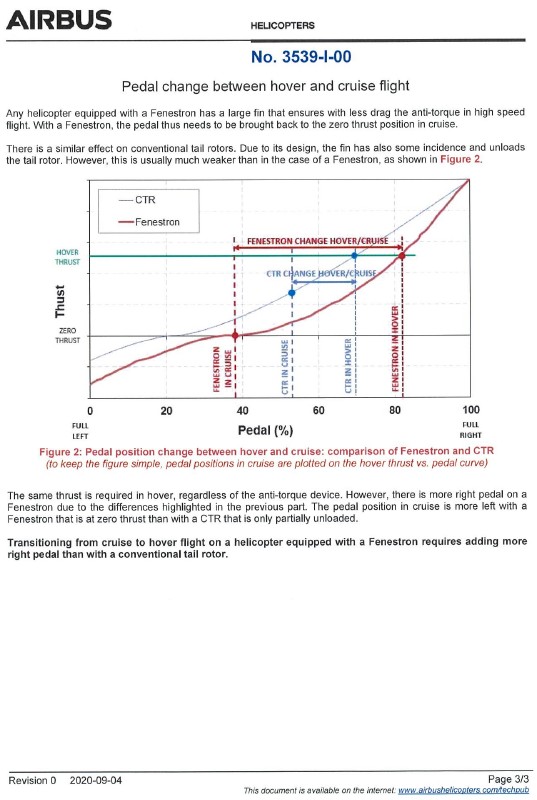
On 3 July 2019, Airbus Helicopters issued Safety Information Notice No.3297-S-00. On 4 September 2020, the service letter referred to in paragraph 2.61 was superseded by Airbus Helicopters Information Notice No.3539-I-00. The two notices informed pilots of the differences between a Fenestron tail rotor and a conventional tail rotor. See appendix 1 for the two notices (See the Airbus Helicopters web site for the current notices). The 2020 notice stated that:
Transitioning from cruise to hover flight on a helicopter equipped with a Fenestron requires adding more right pedal than with a conventional tail rotor (bold emphasis in the original).
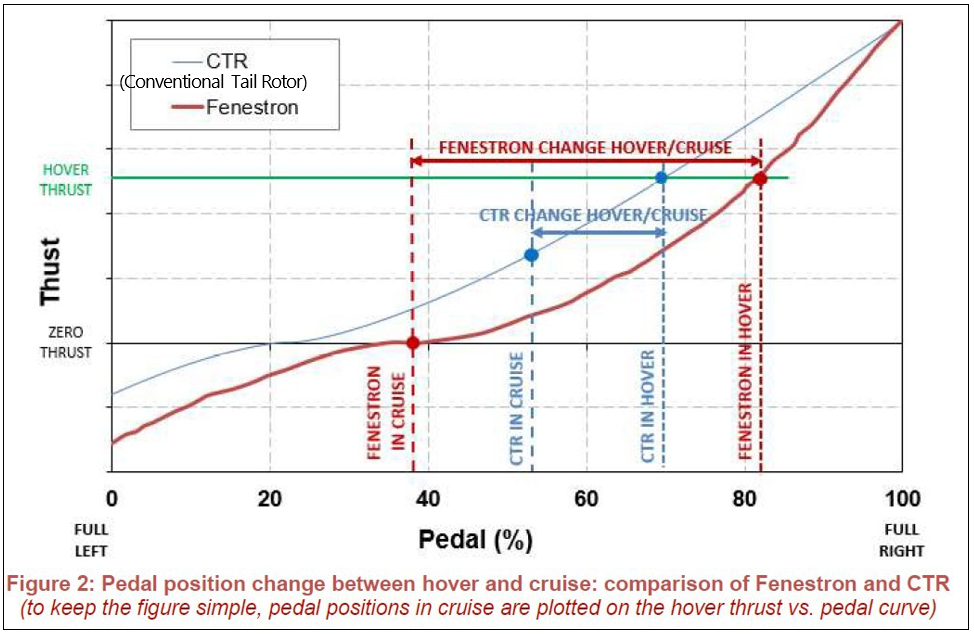
- The notice also included a diagram showing a comparison between a conventional tail rotor and a Fenestron when in hover and in cruise (see Figure 7).
- Similar material on unanticipated yaw was produced by other helicopter manufacturers, regulators and safety organisations. For example, on 7 February 1995 (updated on 8 August 2022), the United States Federal Aviation Administration issued Advisory Circular 90-95 Unanticipated Right Yaw in Helicopters. In March 2017, the United States National Transportation Safety Board (NTSB) issued Safety Alert SA-062 ‘Loss of Tail Rotor Effectiveness in Helicopters.
EC120-B operational evaluation
- On 16 May 2012, the European Union Aviation Safety Agency (EASA), the airworthiness authority that approved the type certificate for the EC120-B helicopter, issued an operational evaluation report on the Eurocopter EC120-B. The report updated recommended type rating requirements, including theoretical and flight training. The report recommended that for an initial type rating on the EC120-B a minimum of five hours of dual instruction be flown. The five hours was to include system, normal and emergency procedures. The requirement reduced to three hours if a pilot already held a ”single engine turbine pilot type rating”. For ZK-HEK, the pilot’s logbook records the pilot flying 12 hours under instruction before flying as pilot-in-command of the helicopter.
Previous unanticipated yaw occurrences
- The NTSB safety alert referred to in paragraph 2.63 stated that during the 10-year period from 2004 to 2014 it had investigated 55 accidents involving LTE (unanticipated yaw). It went on to describe three examples of accidents where the pilot was unable to recover from an unanticipated yaw situation. Detailed in appendix 2 are a selection of examples from New Zealand and overseas, the latter group all involving the EC120-B helicopter.
Analysis Tātaritanga
Introduction
- To be a safe pilot, a person needs to possess both ability and skill.25 There are a range of traits that underpin this, including:
- attention to detail – small mistakes can make a big impact, be it a checklist item or knowing what the wind is doing
- self-confidence – the willingness and ability to take control of a situation and not let it get further out of control, but not be over-confident, allied with the ability to remain calm under pressure
- situational awareness – an accurate understanding of what is going on and projecting forward
- humility – knowing one’s limitations, admitting mistakes and that there’s always room for improvement
- good communication skills – the ability to accurately and clearly transmit and receive information
- knowledge and the desire to learn – knowledge of the aircraft being flown, the operating rules and the willingness to continue improving personal knowledge and skills.
- Many of these characteristics relate to personal attitudes and abilities that may be challenging to change. However, through training and experience a pilot should gain knowledge and become increasingly skilful and safe.
- This accident occurred on what would be described as a good day for flying. It also involved a newly qualified private pilot in the early stages of their flying experience. Pilot experience has often been equated to the number of flying hours a pilot has flown. This ignores the quality aspect of the flight time. Pilot qualifications are therefore both competency- and experience-based. A pilot must not only accrue a minimum number of hours for a particular licence or rating, but also demonstrate to a flight examiner that they have the competency to safely fly an aircraft in accordance with the rules and limitations, both aircraft and personal.
- The following analyses the circumstances surrounding the event, including pilot experience, to identify those factors that increased the likelihood of the event occurring or increased the severity of its outcome. It also examines any safety issues that have the potential to adversely affect future operations.
What happened
- The purpose of the flight was for the pilot to fly their family and a friend from near Rangiora to Kekerengu for lunch and return. The weather was suitable for the flight, with essentially clear skies and a light-to-moderate northeasterly onshore wind. The flight north proceeded without incident until approaching Kekerengu.
- Approaching Kekerengu, the pilot positioned the helicopter out to sea before turning left to place the intended landing area on the right side of the helicopter. This would have enabled the pilot to have an unrestricted view of the landing area, to check it was suitable and clear.
- As the pilot continued the turn back towards the shore a second time, the helicopter slowed and started to yaw to the left. The rate of yaw increased and the helicopter descended rapidly, crashing into the beach in a steep nose-down attitude. The three children on board suffered moderate-to-serious injuries, but the pilot and the second adult in the rear seat did not survive.
Mechanical and medical factors
- Witnesses described the helicopter suddenly and rapidly yawing to the left as it approached the beach. This was not normal and indicates that there was a loss of control, possibly because of either a mechanical problem or pilot incapacitation.
Mechanical
- The damage to the airframe was consistent with the helicopter crashing onto the beach nose first, stopping the rotation of the main rotor and transmission and severely distorting the cabin. The damage to the main rotor blades, rotor head and the tip weight of one of the blades puncturing a hole in the bridge guardrail some 230 m away all confirm that the main rotor was operating at high speed when it struck the beach.
- The above evidence is supported by the analysis of the video recordings, which captured both main rotor and tail rotor speeds. These confirm that both were operating at their designed speeds as the helicopter descended and crashed onto the beach.
- Immediately after the main rotor blades struck the beach, the engine continued to try to drive the transmission, resulting in the coupling between the two breaking. The unrestrained engine then oversped. This resulted in the high-pitched noise, the transmission coupling displaying evidence of overheating and the light-coloured smoke observed by the witnesses immediately after impact.
- The absence of damage to the rear of the helicopter, in particular the tail rotor blades, does not indicate there was a problem with the tail rotor. The sudden stoppage of the main rotor combined with the mass of the still turning tail rotor caused the tail rotor drive shaft from the transmission to break. The score marks inside the tail boom show that the tail rotor and the section of connected drive shaft continued to rotate for several revolutions after the initial impact of the main rotor. The direction of the break and score marks support this sequence of events.
- There was no evidence of a pre-existing fault that may have contributed to the loss of control. The flight controls, including the tail rotor controls, functioned as designed.
- The position of the left front seat (nearly fully aft) and tail rotor pedals (fully forward) meant that it was exceptionally unlikely that the occupant of this seat could have interfered with the controls.
Medical
- There was no evidence of any form of pilot incapacitation. Wreckage evidence, autopsy results, toxicology and witness accounts, including from survivors, indicate it was very likely that the pilot was operating the flight controls at the time of impact. However, some form of partial incapacitation in the final seconds could not be fully excluded.
- The possibility of a bird strike affecting the pilot or helicopter was considered exceptionally unlikely. There was no evidence found of a bird strike and no witnesses or survivors reporting seeing birds close to the helicopter. The slow speed of the helicopter as it approached the beach the second time was considered too slow for a bird strike that could cause any damage or injury.
- Pilot age is discussed further in paragraph 3.56.
Helicopter design
- The unique advantage of a helicopter is its ability to operate in remote and confined landing sites. However, helicopter design and performance vary significantly between different types, resulting in a wide range of handling or operating characteristics.
- The EC120-B, like the Cabri the pilot initially trained on, was fitted with a Fenestron tail rotor. The Fenestron is a multi-bladed ducted fan placed in the tail of a helicopter. The Fenestron offers some advantages over a conventional tail rotor, including:
- increased safety – the tail rotor blades are surrounded by ducting or a fairing that provides increased protection and safety on or near the ground
- increased efficiency – the fairing reduces tip vortices on the ends of the blades and increases the slipstream effect of the tail during cruise
- reduced noise levels – the larger number of blades (ZK-HEK was fitted with eight tail rotor blades) at different spacings spread and reduce noise levels.
- The Fenestron also has some disadvantages, including:
- increased weight and drag – the ducted fan is heavier and larger than a conventional two- or four-bladed tail rotor
- increased cost – a Fenestron is more expensive to construct
- more power required at low speeds – this is particularly so in the hover.
- Regardless of which design pilots fly, tail rotor input is still required for changes in airspeed and power to counter the main rotor torque effect.
- From a pilot’s perspective, the designed differences between a Fenestron tail rotor and a conventional tail rotor are most noticeable in the tail rotor pedal inputs required as a helicopter is accelerated from a hover to cruise flight and back to a hover. For a conventional tail rotor, the relationship between tail rotor pedal input and tail rotor thrust is near linear. By comparison, when a Fenestron equipped helicopter is slowed to the hover, a pilot needs to apply a larger amount of tail rotor pedal for the same amount of tail rotor thrust (see figure 7).
- The helicopter starting to yaw left as it flew towards the beach a second time was symptomatic of insufficient tail rotor thrust, and not enough right pedal being applied to counter the torque effect of the main rotor as the helicopter slowed.
Accidents related to Fenestron tail rotors
- The accidents described in appendix 2 are examples of unanticipated yaw that occurred as the helicopters were moving very slowly, often when approaching land. In addition to the accidents described, there have been numerous other accidents involving Fenestron equipped helicopters.
- The investigation reports for the unanticipated yaw accidents involving Fenestron tail rotors identified a range of causes. These included pilots who had previously flown helicopters with a main rotor that turned in the opposition direction and as a result had subconsciously applied the incorrect pedal as the helicopter was slowed. There were accidents where pilots had not anticipated the requirement for more right pedal input as they slowed down. As a result, the helicopters started yawing left and the pilots possibly became disorientated and/or did not apply a full right pedal to counter the yaw.
-
In the investigation of an unanticipated yaw accident in 2015 involving an EC130 helicopter (similar to the EC120-B, but larger), the BEA conducted a simulation to determine the effectiveness of the tail rotor in recovering from the situation. The report stated:
A flight on a helicopter of the same type under similar conditions but at an altitude of 500 ft was used to evaluate the effect of the Fenestron tail rotor on the yaw rate. At an angular rate to the left of 100 degrees per second (when the pilot begins to decrease the collective pitch to land the aircraft), pushing the right rudder pedal to 70% of its travel stops the yaw rotation of the aircraft in three seconds (BEA Investigation Report 0647: Accident involving Airbus Helicopter EC130 B4 registered F-GOLH on 24 October 2015 at Megève (74).
- The video recording of ZK-HEK shows that the rate of yaw increased from when it first started to turn and continued until it descended from view behind bushes. The yaw rate for the first full turn was determined to average about 90° per second, increasing to over 120° per second for the second full turn. The yaw rate was approaching 180° per second for the last half turn before the helicopter went from view.
Downwind approaches
- It is preferable to land any aircraft into wind, as this assists in the control of the aircraft. Many of the accidents described the helicopters approaching the landing areas either downwind or crosswind. This had the potential to affect the helicopters in several ways. For a downwind approach, a helicopter’s airspeed would be less than its groundspeed. This would result in more power required earlier in the approach. An increase in power causing an increase in main rotor torque would result in the helicopter yawing. If pilots were not prepared for this, perhaps by not using the available visual cues, it could catch them unawares.
- A second effect of not approaching a landing site directly into wind is directional control. As a helicopter slows and airspeed reduces, the slipstream design of a helicopter will result in it trying to turn into the prevailing wind if no pilot action is taken.
- For an out-of-wind approach, the requirement for increased power and directional stability can occur simultaneously. This can result in a helicopter suddenly yawing, startling a pilot. This startle effect was cited in several investigations where there appeared to be no recovery action taken after the initial yaw. In this accident, there was no obvious recovery action initiated and the rate of yaw continued to increase as the helicopter descended. It therefore indicates that the pilot was very likely startled by the initial sudden left yaw (for further information on the startle effect see skybrary.aero).
- Out-of-wind approaches, however, can offer some advantages. For a helicopter with a main rotor that turns clockwise, like ZK-HEK, approaching a landing area with the wind on the right side of a helicopter can reduce the power required for an approach. As the helicopter is slowed, it will attempt to yaw right into the prevailing wind. This results in a pilot needing to use left pedal to continue to align the helicopter with the approach path. Left pedal reduces the power demand on the engine. It also ensures there is sufficient right pedal available when power is increased approaching the hover (see figure 8).
- However, pilots need to be careful when performing this manoeuvre. If directional control is not maintained, a helicopter could yaw left sufficiently to then place the wind on its left side. This would cause the yaw rate to suddenly increase further.
Response of manufacturers
- Emergency training is an integral part of gaining a pilot licence qualification and aircraft type training. For helicopters, this includes various tail rotor emergences that might occur, such as jammed pedals or loss of tail rotor thrust. The incidence of unanticipated yaw accidents, including those involving Fenestron tail rotors, resulted in manufacturers, regulators and safety organisations providing safety notices and educational and training material, to help better prepare pilots for this eventuality should it occur. The manufacturers of the Cabri and EC120-B types of helicopters were no different. See paragraphs 2.58 to 2.65.
- The investigation into this accident determined it was very likely the pilot of ZK-HEK was informed and trained in various tail rotor emergencies, including unanticipated yaw scenarios. The training included the pilot needing to anticipate the requirement of right pedal as power was increased when a helicopter took off or approached landing. Also, should an unanticipated yaw event occur, the pilot should apply full right pedal and, if possible, reduce power and/or fly away.
- However, to be able to safely escape an unanticipated yaw event, a pilot also needed to be able to recognise it and react immediately and appropriately. Early in a pilot’s flying, the response was likely to be very mechanical, which meant that they would first need to recognise the yaw before determining what action was required and then applying right pedal. With training and experience, this would become more intuitive, with a pilot anticipating the need for pedal input. For further information on the Fenestron tail rotor, see the Citations section.
Pilot training
Qualifications
- The pilot of ZK-HEK held a private pilot licence and at the time of the accident had flown a total of 169.5 hours, including 32 hours on the EC120-B. The pilot was therefore deemed legally able to fly the helicopter but was still in the early stages of gaining experience. However, as discussed in paragraph 3.3, flying hours alone do not tell the full story.
- To obtain the private pilot licence (helicopter), the pilot was required to have flown a total of at least 50 hours. This included 20 hours of dual instruction, 15 hours solo and five hours of mountain flying.32 The pilot then needed to complete a flight test with an appropriately qualified instructor or flight examiner. The pilot met these requirements with a total of 84.5 hours. The next flight after the flight test, nearly two weeks later, was with an instructor and included training on several more advanced manoeuvres.
- The pilot, after obtaining their licence, flew a further 85 hours before the accident. This included some 42 hours after completing the type rating on the EC120-B. The 42 hours were spread over about 24 flights and included cross-country flights with passengers, often to off-aerodrome landing sites, and additional advanced training with instructors. The pilot had recently had the second set of flight controls installed in anticipation of further training.
- To obtain the type rating on the EC120-B type helicopter, the pilot was required to pass a ‘basic turbine knowledge examination’, show satisfactory technical knowledge of the aircraft, fly one hour of instruction and demonstrate appropriate pilot skills (CAA Advisory Circular AC61-10 Pilot Licences and Ratings – Type ratings). The pilot obtained their type rating after having flown 7.7 hours with an instructor. The pilot then flew a further 4.3 hours with the instructor before completing their first flight as pilot-in-command. The pilot’s logbook records that the 4.3 hours included heavy-weight, high-altitude landings and mountain flying.
- The number of hours the pilot flew before obtaining their licence and type rating exceeded the minimum requirement. However, this was not considered to be a consequence of the pilot’s ability or skill. Rather, it reflected the pilot’s availability to undertake training and, according to those who were involved in the training, their wish to be competent and safe.
Training
- The pilot’s instructor and flight examiner both described the pilot as a good or average private pilot. They considered the pilot to be conscientious, had listened to advice and was keen to learn. Evidence was provided that soon after obtaining their licence, the pilot was considering purchasing an AS350 Squirrel helicopter. The training provider dissuaded the pilot from this, recommending that it would be “very beneficial to get experience before going to a bigger machine.” The pilot subsequently trialled the smaller EC120-B a month later.
- The pilot’s training records and logbook recorded that they received instruction on, among other topics, crosswind operations, wind awareness, confined areas, mountain operations, cross-country, hazards and emergencies. The logbook recorded that the pilot had not landed at Kekerengu before, but had flown past it on at least four occasions. The most recent time was two months before the accident flight. The training provider advised that the pilot was competent in cross-country flying and operating into remote, but easily accessible, landing sites.
Remote operations
- During helicopter training for remote, confined-area or off-aerodrome operations, pilots are instructed to conduct reconnaissance or recce passes to determine that the site is suitable to approach and land. Pilots will typically use the acronym of the ‘7 Ss’ to help in the assessment (CASA Australia and CAA New Zealand Helicopter Flight Instructor Manual, Issue 3, March 2012). These are:
- Size – is it big enough (subject to experience)?
- Shape – does the shape favour an approach from a particular direction (wind)?
- Slope – is the ground level enough for landing?
- Surface – what is the surface of the area? are there any hidden hazards or could the surface be a hazard, such as dust or snow?
- Surrounds – is the area around the landing site free of hazards, including approach and departure paths (wires)?
- Sun – might the sun restrict visibility on final approach or hide hazards lurking in the shadows?
- Select – choose the touchdown spot (for aeroplanes an eighth ‘S’ could apply – Stock (cattle or sheep grazing on a grass airstrip)).
- Early in a helicopter pilot’s training, the assessment of the intended landing site would be performed over several passes, typically referred to as an initial or high recce and a low recce. With experience and competence, the number of passes may be reduced.
Wind
- Fundamental to the assessment is knowing the wind direction. There was ample opportunity for the pilot of ZK-HEZ to be able to assess the wind conditions during the flight north (such indicators might include the Christchurch terminal weather report broadcast over the radio, windsocks at Rangiora and possibly smoke or dust along the route). The approach and departure paths the pilot flew at their home base and Rangiora were all flown into the same northeasterly wind.
- The northerly onshore wind was constant along the coast. The pilot would likely have had good indications of this, either visually or by comparing indicated airspeed readings with the various navigation groundspeed displays available as the flight progressed north.
- Approaching Kekerengu, the wind was strong enough to generate white-caps, and very likely other indications on the water or bushes. There was also a dark-coloured flag on a pole above the café building. The presence of white-caps indicates a wind velocity of between 10 and 15 knots was present. These potential indicators should have left the pilot in no doubt about the wind direction at the landing site.
- The optimal approach to the landing area in the conditions would have been directly from the south. This would have kept the flightpath clear of the road and buildings. It would also have placed the wind to the front right of the helicopter, possibly slightly to the right, thereby ensuring that there was ample power and pedal control available.
Pilot intentions
- In preparation for the flight the pilot had contacted staff at the café to confirm the weather conditions were suitable for it, which they were. The pilot had flown past Kekerengu before, but never landed there. So, after reaching the area the pilot positioned out to sea, turned left and completed one pass of the intended landing area. The helicopter was being turned back towards the beach a second time when it suddenly commenced yawing left. The video recordings show the helicopter was nose low as it started to yaw. A nose-down attitude is an indicator of a helicopter being accelerated into forward flight (see figure 9).
- It was therefore considered very likely that the pilot was undertaking a second low-level reconnaissance of the landing site when the helicopter started to yaw. The pilot likely intended to fly to the south for a short distance before reversing the turn and approaching the landing area into the prevailing wind.

- The left turn towards the beach resulted in the helicopter flying downwind. The result of the helicopter’s airspeed combined with the tailwind component should have generated an increase in the groundspeed compared with flying into wind. However, if a pilot is not alert to this, there can be an unintentional influence to maintain the same visual movement over the ground and so allow the airspeed to reduce. This is especially important when flying at low levels as the safety margins are reduced.
- In this case, the tracking data shows the helicopter slowing as it turned downwind. This was indicative of the pilot not monitoring the airspeed–groundspeed relationship by looking at the airspeed indicator on the instrument panel. It was therefore considered very likely that as the helicopter was turned towards the beach the pilot was focused on looking outside at the intended landing area to confirm it was still suitable and was not aware of the reducing airspeed. The reducing airspeed required more power to remain level.
- The pilot lowered the nose and increased power to accelerate away. This increase in power (and therefore torque), combined with the low airspeed and already high power setting, was sufficient to start the helicopter yawing. The helicopter only had to yaw left through about 20° before the wind started to come from the rear left side of the helicopter. Once the wind was on the left side, the rate of yaw would speed up further. This yaw, along with the nose of the helicopter rising up and then down as it yawed suddenly and rapidly about the rotor, would have been sufficient to startle and disorientate the pilot. As discussed in paragraph 3.30, this was considered to be very likely.
- There was very likely insufficient height available for the pilot to reorientate themselves and recover by:
- levelling the attitude of the helicopter and applying full right pedal
- lowering the collective lever to reduce the power and therefore the rotation
- cyclicing away and increasing the forward speed of the helicopter and slipstream effect
- a combination of the above.
- The pilot, instead of flying the left-hand pattern out to sea, could have flown a right-hand pattern around the café. This would have placed the intended landing area on the pilot’s right, the side they were seated, while flying into wind. The lower groundspeed would have given the pilot more time to assess the conditions. However, the pilot may not have considered this practical in the situation because of the steep terrain just west of the landing area and it would have resulted in the helicopter flying close to houses and people.
Pilot age
- The pilot was aged 60 and started flying 18 months earlier. While cognitive function may decline with age, likely owing to a decrease in working memory, there are many other human factors that can also affect pilot performance, with pilot attitude being a significant factor. There was no evidence that the pilot’s age was a contributing factor to this accident (the Commission investigated the role of pilot age in Inquiry 11-007: Descent below instrument approach minima, Christchurch International Airport, 29 October 2011). The pilot was considered by their instructor and training organisation to be a diligent and keen student. This was demonstrated by the pilot undertaking additional training before and after obtaining their licence, listening to the advice not to purchase a larger AS350 helicopter and planning further training.
Survivability
- All five occupants were retained in their seats following the helicopter crashing on the beach. Three children survived the accident. The pilot seated in the front right and the adult seated in the rear left did not.
- The force and angle of impact resulted in the cabin being severely deformed. This reduced the survivable space available, especially for the two adults. Also, the higher mass of the pilot, when compared to the other occupants, resulted in greater distortion of their seat. It also meant that the deceleration was not able to be absorbed by the seat to the same degree.
- The smaller physical size of the children meant that the disruption to the cabin was also not as critical. There was still survivable space available. Also, the smaller mass of the three children meant that their seats were able to better absorb the impact forces. Nevertheless, they still sustained a range of moderate-to-serious injuries. The prompt action of the witnesses and emergency services assisted in managing their injuries.
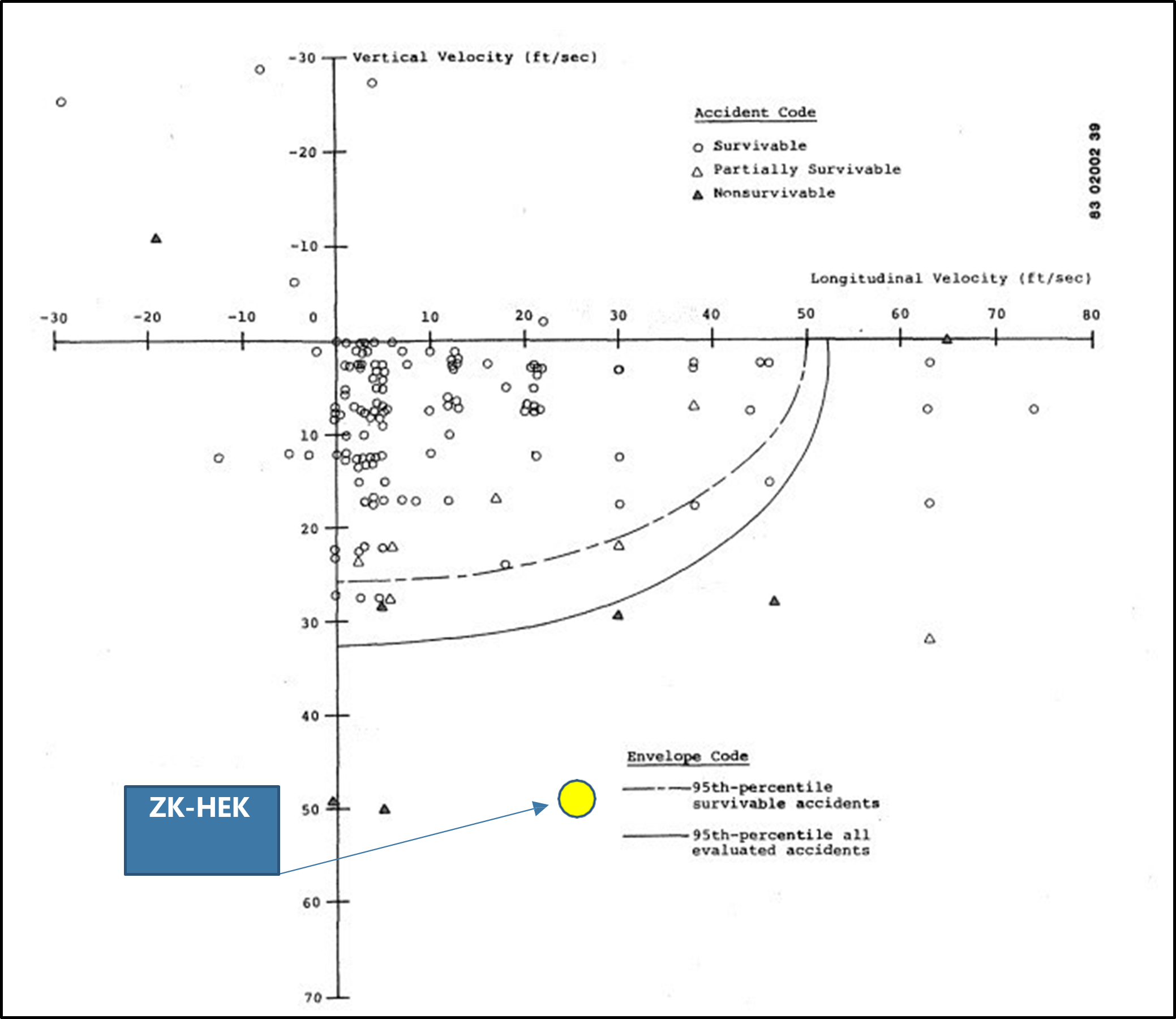
- Airbus Helicopters’ analysis of the damage determined that the impact forces were well beyond the level of crash protection for aircraft, including for helicopters, recommended by the United States Federal Aviation Administration (see figure 10).
Appendix 1. Airbus Information notices