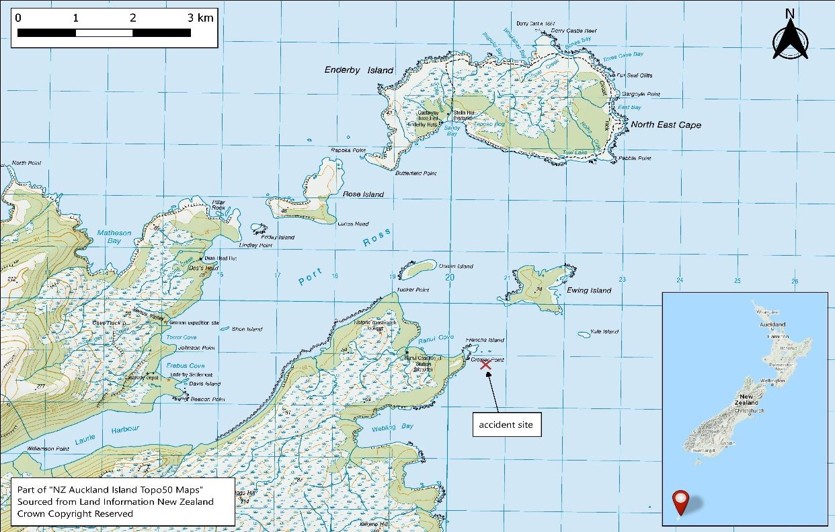
On 22 April 2019, a BK117-C1 helicopter (ZK-IMX) on a medical evacuation positioning flight to the Auckland Islands arrived after dark and continued under visual flight rules using night vision goggles. While attempting to descend below cloud near Enderby Island, the helicopter impacted the sea. The three crew escaped, swam to shore, and were rescued the next day with minor injuries. The helicopter was recovered three weeks later.
Executive summary Tuhinga whakarāpopoto

What happened
- On 22 April 2019, the operator was conducting a medical evacuation flight under visual flight rules (VFR) with a BK117-C1 helicopter, registration ZK-IMX. On board was the pilot, a paramedic in the front left-hand seat, and a winch operator in the rear cabin. The helicopter was to position south of New Zealand at Auckland Islands that day (the positioning flight). After camping overnight on Enderby Island, the helicopter crew would rendezvous with a fishing ship next day to heli winch and evacuate a sick crew member back to New Zealand.
- The positioning flight was intended to arrive during daylight, but unexpected delays to the departure time resulted in them arriving after dark. The crew carried night vision goggles (NVGs) and donned them during the positioning flight to continue under VFR using NVGs.
- The hills and coastline around Port Ross and part of Enderby Island were visible through NVGs, but the pilot believed that the landing area was covered in cloud. The pilot planned an alternative approach to descend in the clear area to below the cloud and then follow the coastline back to the landing area.
- The pilot descended and was turning back towards the landing area when the crew member (paramedic in front left-hand seat) alerted them to cliffs rising immediately ahead. The pilot reacted, but the helicopter impacted the sea.
- The crew were able to escape while the helicopter was partly submerged, but it sank soon after. They were all wearing immersion suits that kept them afloat and enabled them to make their way to shore. After sheltering under cover overnight, they were spotted the next day by one of the rescue helicopters and brought back to Invercargill to be checked in the hospital.
- The winch operator in the rear cabin was knocked unconscious during the impact, but was able to be evacuated by another crew member. They regained consciousness during the swim to shore. Otherwise, the crew only suffered minor injuries.
- The helicopter was recovered about three weeks later.
Why it happened
- The helicopter was operating normally at the time of the accident.
- The Commission found that the pilot had misinterpreted the image seen through the NVGs as cloud covering the landing area when it was very likely to have been fog near the sea surface and downwind of the shore. The planned descent and approach in the clear area was made using visual reference outside and to the global positioning system (GPS) map display. However, the helicopter’s descent rate became high as the pilot, relying primarily on visual depth perception, believed the helicopter was further from the surface of the sea than it was. When the crew did see an image through the NVGs it was the 20-metre high cliffs several hundred metres ahead and above them. During the manoeuvre to avoid the cliffs, the helicopter impacted the sea.
- The Commission found that the operator’s exposition2 for single pilot VFR operations into the Southern Ocean was inadequate at the time to manage the risks associated with such operations. The operator has since made significant improvements, including engaging an external auditor and introducing a new standard operating procedure for Sub Antarctic Island flights. Therefore, the Commission considered that no safety recommendations to the operator were necessary.
- The Commission also identified regulatory gaps in the New Zealand Civil Aviation Rules (CARs) regarding minimum safety requirements for helicopters operating under Part 119 and Part 135 air operator certificates (AOCs). The gaps related to:
- Helicopter air ambulance (HAA) operations.
- Night vision imaging systems (NVIS) and operations.
- Crew resource management (CRM) for operations conducted with multi-pilot or a single pilot with a non-pilot crew.
- Pilot logging of NVG flight time.
- The Commission made two safety recommendations to the Civil Aviation Authority (CAA) in section 6 to address these safety issues.
What we can learn
- The key lessons from this investigation are listed in section 7. In summary they are that:
- The minimum requirement for NVG currency does not equate to proficiency.
- Helicopter underwater escape training (HUET) and immersion suits can increase survivability.
- If the operation needs crew to wear immersion suits, they should also carry essential emergency items on their person.
- All crew with flight-related duties need to be aware of the importance of radio altimeters when conducting NVIS operations and how to interpret the instrument and its alerts.
- Pilots should ensure their NVG flight time is separately logged.
- Overloading helicopters is a safety hazard.
- To be effective, emergency equipment such as a life-raft must also be accessible in an emergency and deployable for the crew to use.
Who may benefit
- Pilots and operators involved with HAA operations, those using NVIS, and the regulator may benefit from the findings and recommendations in this report.
Factual information Pārongo pono
Narrative
The task plan
- On 22 April 2019, a Kawasaki Heavy Industries (KHI) BK117-C1 helicopter, registered ZK-IMX (the helicopter), was tasked by Southern Lakes Helicopters (the operator) for a medical evacuation (medivac) in the Southern Ocean off Auckland Islands. A crew member on board a fishing vessel required urgent hospital treatment and the first aid stocks on the vessel needed replenishment.
- The helicopter was based in Te Anau. The vessel was 210 nautical miles (nm) south of Auckland Islands, but intended to make way towards this destination where it would anchor in a sheltered area for the medivac transfer. The vessel was expected to arrive at the rendezvous point at about 0750 on 23 April 2019.
- The flight was to be conducted under VFR. Due to a frontal weather system approaching New Zealand from south of Auckland Islands, the operator planned to position the helicopter at this destination prior to the front arriving there. They would stay overnight and then complete the medivac and return to Invercargill the next day.
- The helicopter crew would stay at a hut on Enderby Island where the operator had a fuel store. The plan was to take minimal equipment out to the rendezvous point and initially bring the patient back to the hut. The patient would be transferred to a more comfortable stretcher and stabilised, and the helicopter refuelled and then prepared for the return flight to Invercargill. The vessel needed to replenish the medical supplies used to treat the patient and these would be delivered during the patient transfer.
- The task was approved by the operator to proceed, and the crew of one pilot, a paramedic and a winch operator was selected. The paramedic and winch operator were both trained and current ‘NVIS crew members’ (this is a term for crew trained to assist a pilot with NVIS. See Glossary and paragraph 2.70 for explanation of NVIS). They decided that the paramedic would sit in the front with the pilot and perform the role of NVIS crew member on the flight down. The return flight would be in daylight.
- The winch operator was some distance away from base at the time, but was in transit by road back to Te Anau. They would be picked up by the helicopter on its way to Invercargill.
- The pilot and paramedic prepared the helicopter and loaded the equipment, but the release of the required medical supplies and delivery to the helicopter delayed the departure time. The original plan had been to arrive at Enderby Island in daylight, but the crew were now committed to a night-time arrival.
The flight
- The flight left Te Anau at 1543 for Invercargill with the pilot and paramedic on board, and they picked the winch operator up on the way at Athol. They refuelled at Invercargill and the crew put on their immersion suits and life-jackets. They rechecked that their NVGs were working and the pilot fitted theirs to their helmet. The pilot was in the front right seat and the paramedic in the front left and they both had green phosphorus NVGs. The winch operator was sitting in the back next to the left-hand side door.
- The flight departed Invercargill at 1703 and the pilot filed a verbal flight plan with the local air traffic controller. The Invercargill air traffic control zone extended south to near Stewart Island and the service would go off watch before this flight terminated. The flight duration to Enderby Island was expected to be about three hours from Invercargill. The pilot updated the local air traffic controller when the flight departed the control zone with an estimated time of arrival (ETA) at Enderby Island of 1944. They initially set off at about 6000-7000 feet, but dropped down to cruise under 3000 feet most of the way because the wind was more favourable at that altitude.
- The operator provided their own flight following and communications service for all its operations, and was monitoring this flight with a satellite tracking system (TracPlus) fitted to the helicopter. The flight following service was provided from its base office at Te Anau during working hours and by the chief pilot from their home after hours. They also had very high frequency (VHF) radio contact for part of the route through the operator’s repeater at Stewart Island and by satellite phone beyond that. The pilot regularly called back to base during the flight with position and operational reports.
- At about 90 nm from Enderby Island, at approximately 1850, the pilot contacted the chief pilot to discuss the flight's progress and decide if it was suitable to continue. They were still in daylight at their altitude and could see the cloud with the approaching frontal system on the horizon. After a discussion with the chief pilot, they decided to continue.
- Civil twilight had ended in their location at 1831, and the pilot and paramedic confirmed in a situation report to base logged at 1858 that they were on NVGs. They could see the hills of Auckland Islands on the horizon about 60 nm ahead. The winch operator in the back was not using NVGs, and recalled it being pitch black.
- The pilot discussed their view of the approach to the landing point with the paramedic. They both recalled that a large bank of cloud covered the landing point and extended to the south, but that there was a clear area over Port Ross extending out toward the northwest. If they could not follow the coastline, they had alternative landing points on the islands programmed into the GPS that they could land at and camp out for the night. The pilot pointed out the area clear of cloud and advised the paramedic that they would continue to head south past Ewing Island, descend in the clear area, and fly back along the beach to the planned landing point on Enderby Island. They turned south at 1934, passing 1.5 nm to the east of the landing point.
- The pilot said they set the radio altimeter reference to 1000 feet and started a descent. After reaching the set height, the pilot reset the reference to 500 feet and continued to descend. The pilot then reset the radio altimeter to 250 feet and slowed to 75 knots, but continued to descend on a westerly heading about 0.25 nm south of Ewing Island. The paramedic alerted the pilot to some cliffs that appeared directly ahead in their flight path. The pilot flared to slow the helicopter and started to turn north to avoid the cliffs. The helicopter stopped suddenly when it hit the water at 1937.
Post-impact
- The helicopter had impacted the water at speed and flipped upside down, but initially remained partially submerged at the surface. It was dark, but there was enough light for the crew to see each other and make out their surroundings. The two front seat crew escaped underwater and gathered on the northern side of the helicopter. The winch operator had been knocked unconscious in the accident and was dragged out of the helicopter by the paramedic. The NVGs the front seat crew were wearing had been lost in the accident. The crew recalled that the sea state was dead calm. Some floating items were collected, and after extracting the winch operator the paramedic re-entered the rear of the cabin with the intention of retrieving the life-raft. However, in the darkness it was difficult to identify the various items and a gear-bag was mistakenly taken instead. The helicopter sank shortly after along with the emergency bag.
- None of the crew had an emergency beacon or survival equipment on their person or in their immersion suit pockets. They had packed all their personal locator beacons (PLBs) and other survival gear into an emergency grab-bag that was stowed in the rear cabin and this was lost with the helicopter when it sank.
- The crew could see the outline of the cliffs about 100 metres away and were supported in their immersion suits without needing to inflate their life-jackets. They paddled as a group to the cliffs and climbed through a kelp bed onto the rocks. The winch operator had regained consciousness, but needed assistance from the other two. They made their way along the coastline to the north and found shelter in the bush for the night.
- The crew heard an Orion aircraft fly overhead at times during the night, but were not able to make a signal to attract attention. They also saw vessels out off the coast at times, but again could not attract attention.
The rescue
- The chief pilot was monitoring the flight and immediately noticed the flight following signals had stopped updating. After attempting to contact the helicopter crew on the satellite phone, and confirming with the TracPlus call centre that it was not a system fault, the chief pilot notified the Rescue Coordination Centre New Zealand (RCCNZ) at 2008.
- RCCNZ tasked a Royal New Zealand Air Force (RNZAF) P3 Orion aircraft to conduct a visual search near the last known point. The P3 Orion left from RNZAF Base Whenuapai at 2251 and arrived on scene early next morning at 0120. Cloud cover prevented a close search at low level so an infrared scan was conducted searching for life forms. Flares were dropped along the east coast of Auckland Islands. The P3 Orion continued to patrol the search area during the night and then departed the scene at 0815 for RNZAF Base Ohakea to refuel and change crew.
- RCCNZ also tasked five fishing vessels operating nearby to assist with a sea search. The first fishing vessel arrived in the area on 22 April at 2323. The Antarctic Discovery6 also headed to the area, but then diverted to Bluff with their patient. The five fishing vessels remained on scene and conducted a coordinated search in the designated search area. This extended south of Ewing Island towards and beyond Yule Island. At 0803, one of the fishing vessels found the left-hand sliding cargo door from the helicopter floating within the search area.
- Three rescue helicopters departed New Zealand at about 1015 on 23 April 2019. The first arrived on scene at 1142 and saw the three crew members in their brightly coloured immersion suits walking on a beach near Crozier Point at 1145. The other two rescue helicopters dispatched from Dunedin arrived a few minutes later. After providing first aid to the three crew and refuelling, the rescue helicopters flew the crew to Invercargill hospital.
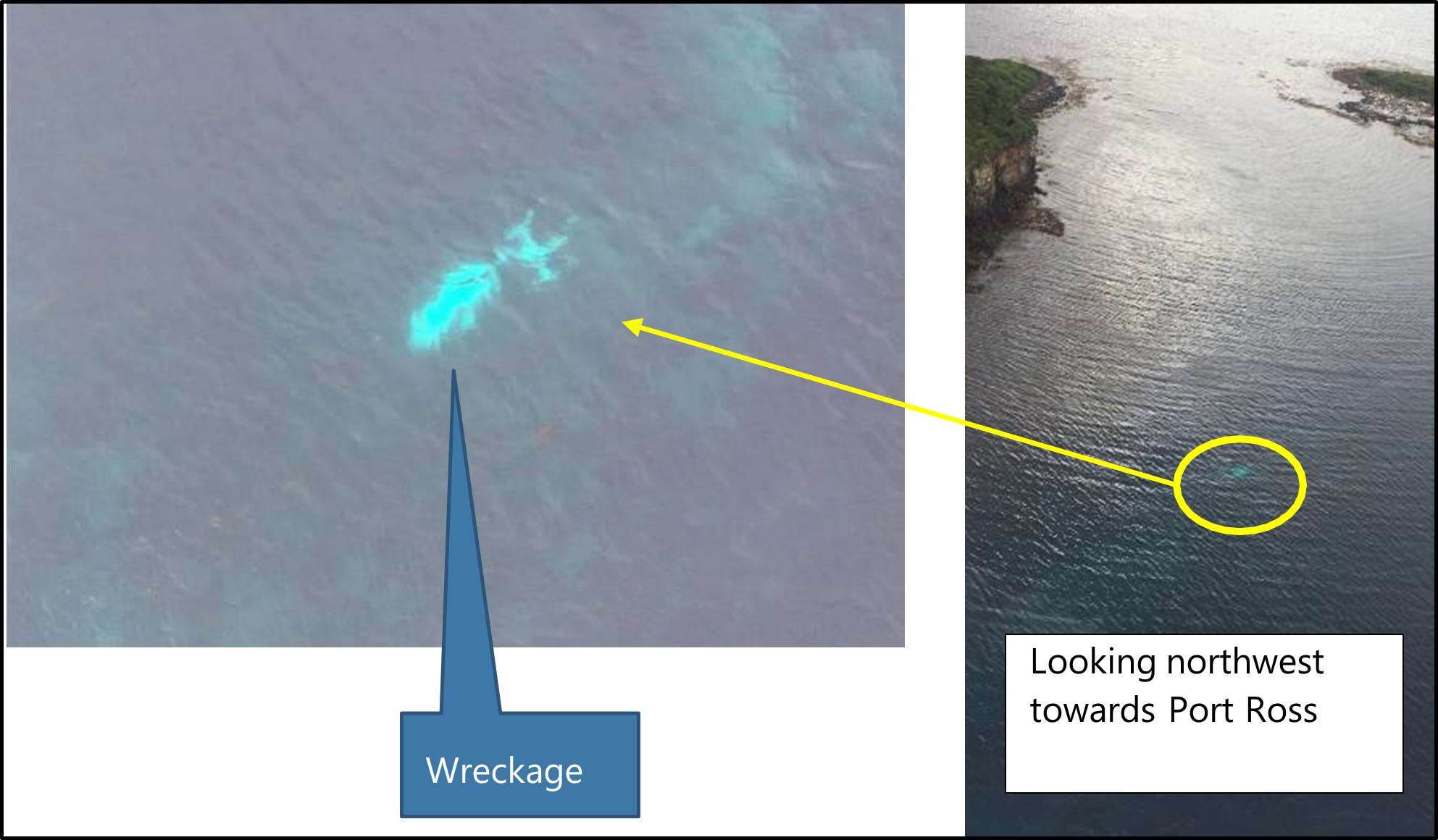
- The wreck was observed in the water just off the northeast coast of Auckland Islands near Ewing Island. It was upside down in water about 15 metres deep.
- Most of the wreckage was retrieved 18 days later by a private operation and taken to Bluff for inspection by Commission investigators. The tail boom and main rotors were not retrieved. The wreckage was later transported to the Commission’s technical facility in Wellington.
Personnel information
Pilot
- The pilot held a commercial pilot licence for helicopters CPL(H) from 2006 with approximately 6673 hours logged before the accident flight and was rated for VFR only. Recent flights included 43 hours on the BK117 type of helicopter during the last 90 days and 135 hours on all types in the same period. The pilot held a Class 1 medical certificate valid to 26 August 2019 and was required to have spectacles readily available with a spare set.
- All required competency assessments were complete and current in accordance with CARs and the operator’s exposition. The pilot’s flight crew check and training for NVG (AC91-13), sling load (Part 133) and air operations (Part 135) were revalidated in December 2018 and current until 27 December 2020.
- The operator arranged other training specific for their operations. The pilot had completed HUET training in July 2013. In 2014, the pilot completed a specialist helicopter CRM training course for low-level helicopter operations. This was run in New Zealand by an organisation from the United States of America (USA), Utilities Aviation Specialists. In 2018, the pilot attended a two-hour human factors course based on the Federal Aviation Administration (FAA) Handbook AMT-8083-30, Chapter 14 (FAA, 2018).
- The pilot received initial NVG ground training in 2013 and then completed a pilot-specific NVG training course later that year. At the time of the accident flight, the pilot had about 73 hours of total flight time at night. The pilot did not distinguish between night VFR or night VFR flight on NVGs in their logbook, but said all recent night flight time with the operator was on NVGs.
- The pilot had logged 0.5 hours on NVGs in the last seven days before the accident and another 0.4 in the last 90 days. Both night flights started as a daytime flight, but returned at night. The pilot advised that they ensured each recent night flight included three take-offs and landings on NVGs to maintain their currency (see 2.89 for NVG currency requirements). The pilot did not hold an instrument flight rules (IFR) rating, nor was this required for NVIS operations. The pilot’s total instrument time recorded in their logbook was 10.2 hours.
Paramedic
- The paramedic was employed by another company and flew as crew with the operator when required for medical services. The operator trained the paramedic to be an NVIS crew member and ensured they remained current for that role (see NVIScrew members).
- The paramedic had undergone annual NVG crew training and records were sighted back to 2015. They were current in accordance with the operator’s exposition, with the last revalidation check 14 days before the accident flight. The paramedic had a total logged time on NVGs at the time of accident of 198 hours.
- The paramedic had completed their last HUET training on 18 May 2018 with over a year to their next refresher course after this accident. The paramedic had received ‘emergency training’ in accordance with the Operator’s exposition for flight over water that included life-raft operation, the ditching procedure and aircraft evacuation.
- The paramedic had also attended the helicopter CRM training course run by Utilities Aviation Specialists for the low-level environment in August 2014.
Winch operator
- The winch operator was a casual employee to operate the winch when needed. The operator had also trained the winch operator as an NVIS crew member and ensured they remained current for both roles. Their last revalidation check for operating the winch fitted to the helicopter was completed in June 2017.
- Their total time on NVGs was 120 hours and they had completed an NVIS crew member revalidation check in November 2018
- The winch operator last completed a HUET refresher course in September 2013, which included ‘emergency training’ in accordance with the Operator’s exposition for flight over water. That training included life-raft operation, the ditching procedure and aircraft evacuation. They had also completed the low-level environment CRM training course held in 2014.
Aircraft information
- The BK117-C1 helicopter was constructed in 1996 by KHI in Japan. It was imported to New Zealand with the certificate of airworthiness completed on 5 May 2016 at 5387 hours. It was purchased by the operator on 6 July 2017.
- The helicopter’s last recorded total flight time was 6558.95 hours at 23 March 2019, 30 days before the accident. The helicopter’s Technical Log, where more recent flights were recorded, was lost at sea. The helicopter had been maintained in accordance with the operator’s approved maintenance programme for KHI BK117-C1. The maintenance logbooks showed that all scheduled maintenance had been carried out as required, and the helicopter had no recorded defects at the time of the accident.
- The BK117 has a four-bladed rigid rotor system that rotates anti-clockwise (when viewed from above). The pilot sits on the right-hand side. The helicopter had two Turbomeca Arriel 1E2 engines rated at 692 shaft horsepower each.
- The helicopter had NVIS compatible instrument lighting installed in April 2017, which was certified in simulated blackout conditions by the CAA in December 2017. The helicopter was listed on the operator’s AOC as being NVIS compatible and that NVIS certification was current at the time of the accident.
- The helicopter was fitted with a radio altimeter that had a single display in the pilot’s console. It had a manually adjusted height alert setting (the height setting bug) with a visual indication light that illuminated when the helicopter was at, or below, the selected height. It did not have an aural alert signal. The radio altimeter display was visible from the left-hand seat, but any person seated there would need to lean towards the pilot to read heights without parallax error. The helicopter also had an autopilot system.
Weight and balance
- The helicopter’s empty weight recorded in the logbook on 21 February 2019 was 2101 kilograms. The helicopter’s type certificate stated that the maximum certified take-off weight was 3350 kilograms.
- The operator had a set of standard helicopter loading guides to enable pilots to quickly check the loading was correct. In this case the appropriate guide was called ’Weight Loading Guide – BK117-C1 Medivac Configuration’ (see Appendix 1).
- The exposition (exposition, weight and balance, item 3 (Version V17.21)) required pilots to use a weight and balance application on their phone, or a company iPad called iBal Rotary, and to email the loading file to the office for flight following. Alternatively, they could use the guides. In this case the pilot used the iBal Rotary application on their phone, but did not email a copy to the office. The helicopter loading was checked for this investigation by using the standard weight loading guide.
- The operator’s standard loading guide for a medivac operation in this helicopter allowed for a typical medivac configuration, from which the pilot could then select the appropriate fuel loading. In this case, the aircraft was configured with full fuel, plus two full external range extender fuel pods for a flight duration of 3.4 hours plus internal cargo and three crew. The return flight would have an additional medivac passenger.
- According to the guide, 166 kilograms was available for cargo, including a 100-kilogram pilot and the standard medivac equipment of seating, oxygen, stretchers, life-raft and life-jackets. Items recovered post-accident were taken to the Commission’s technical facility and weighed. The weights of missing items that were known to be on board were estimated. In this case, the excess cargo included: a winch, the associated winch stretcher and gear, a long-distance internal stretcher, additional medical equipment, a fuel transfer pump, the crew’s survival kit, three NVGs and their containers, camping gear, food for three people overnight, and the two crew members with their immersion suits and helmets (see Appendix 2 for calculated weight).
- The exposition at the time stated that the final loading check was for the pilot to conduct a dynamic power and control check in the hover position before continuing (exposition, operations, weight and balance, item 7 (Version V17.21)).
Meteorological information
- The flight was conducted as a Commercial Transport Operation (CTO) under VFR. This meant that the pilot was required to manoeuvre the helicopter so that other traffic and any obstructions could be observed in time to avoid a collision. The night approach into Enderby Island required meteorological conditions of not less than a 2000 foot AGL cloud ceiling and a flight visibility of not less than 5 kilometres (CAR Part 135.155).
-
The MetService provided the Commission with a description of the weather situation for the 48-hour period covering the accident (the accident occurred at 1937 on 22 April) from 0000 NZST (NZST means New Zealand Standard Time at Universal Time Coordinated plus 12 hours) 22 April 2019 to 0000 NZST 24 April 2019:
At the start of the period a narrow ridge lay over the southern South Island, and a weak warm front over the Auckland Islands. The observations from Enderby Island suggest that there was low stratus and drizzle over the Auckland Islands at this time. The weak warm front moved away to east and weakened further around mid-morning on 22 April 2019.
The Enderby Island observations show that the drizzle ceased at this time, however the relatively humidity remained high and the air temperature was close to the sea surface temperature. This would suggest that sea fog or low stratus persisted about the Auckland Islands from mid-morning on 22 April 2019 until the early morning of the 23 April 2019.
A cold front then arrived from the west crossing the Auckland Islands around 0800 NZST 23 April and continued northeast, passing through Invercargill around 1800 NZST 23 April 2019. The Enderby Island observations showed a period of rain from 0300 to 0930 NZST 23 April 2019 associated with this cold front. Following the cold front, it was initially fine over the Auckland Islands, but cloud periods gradually increased and it is possible that there were a few light showers.
Sea: 1m occasional 1.5m, but eased for a time around dawn on 22 April 2019, and rose to 1.5m occasional 2.2m from the afternoon of 23 April.
Swell: Westerly between 2.5 to 3m through the period, sheltered east of the Islands.
- The situation at the time of the accident is shown on the synoptic chart in Appendix 3. This covered the period from midday when the flight planning started to after their departure.
- The operator had found from experience that standard aviation weather forecast information was not reliable for the Southern Ocean. They obtained their own weather information from several different but well-known sources, including the automatic weather station (AWS) on Enderby Island, then made their own assessment. In this case, they were aware of the cold front approaching Auckland Islands and had planned to arrive before it and weather out the night on the ground. The medivac would take place the next morning on 23 April and the return flight north back to Invercargill would be in the clearer air behind the cold front.
- The sun set at Auckland Islands at 1757 that day and civil twilight ended at 1831. The moon phase was in its third day after full moon with 94 per cent illumination (in relation to full moon at 100 per cent). The moon was still below the horizon at the time of the accident and rose at 1949 (Timeanddate.com, 2022). The predicted night illumination levels at Auckland Island for the time of arrival was not available to the pilot. Subsequent research found that the illumination level was at its minimum at the time of arrival (see Tests and research).
- The record from the MetService AWS at Enderby Island showed that for at least 20 hours prior to the accident the temperature and dew point were less than 1°C apart at about 11°C. This had resulted in a steady relative humidity of between 97 per cent and 99 percent. The wind at the time of the accident was trending from 290 degrees through to 310 degrees True and was steady near 11 knots with maximum gusts to 18 knots. The pressure was steady at 1022 hectopascals and it was not raining. This AWS does not measure cloud base or record video.
Communications and aids to navigation
- The helicopter had VHF communications through the operator’s repeater network and the Airways aviation infrastructure. The coverage did not extend for the full flight distance. The helicopter was also fitted with a satellite phone for communications outside normal radio coverage.
- The pilot used a Garmin 296 GPS with map display to navigate.
Recorded data
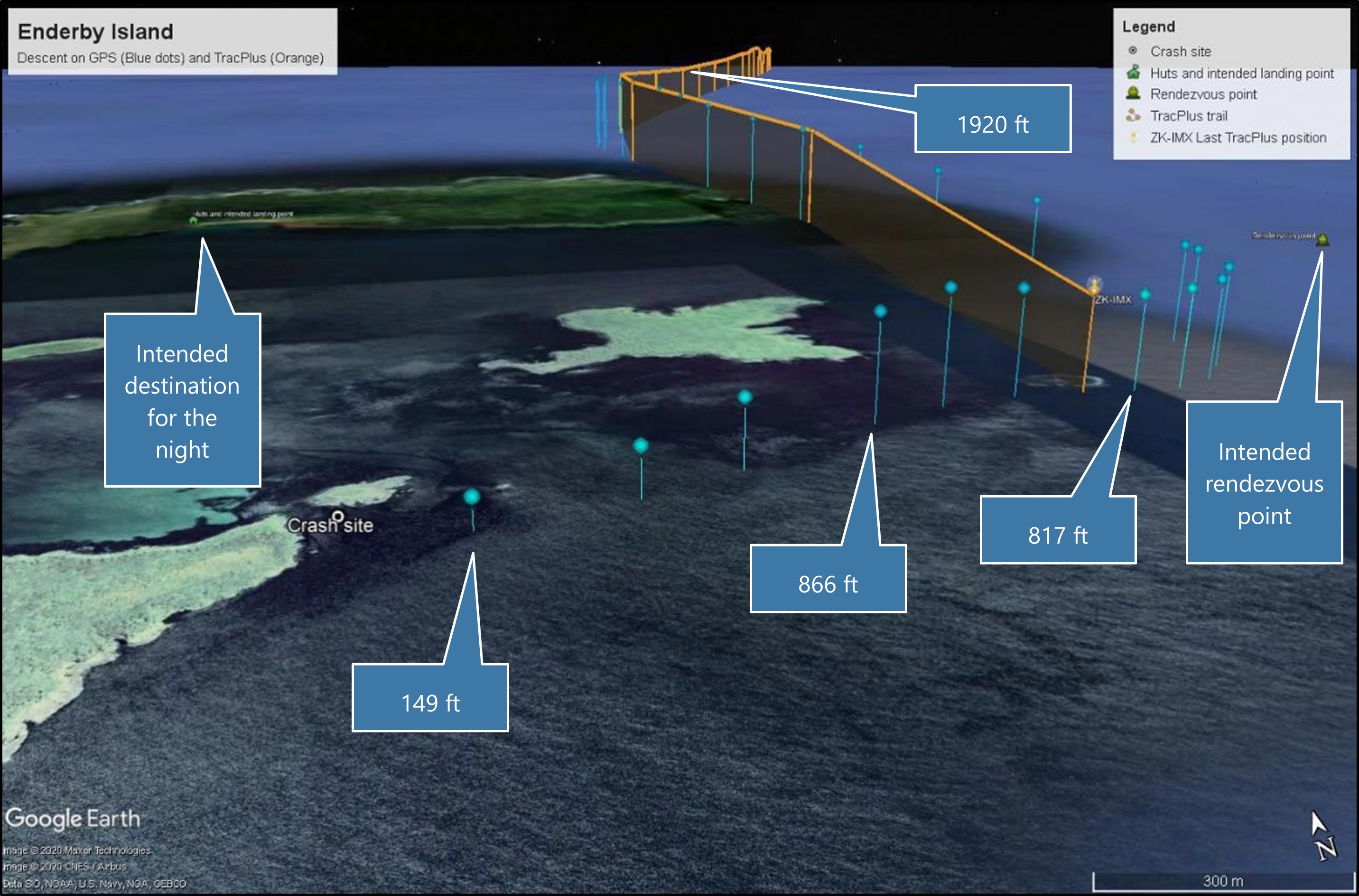
- The helicopter was fitted with a TracPlus, satellite-based, flight following system. This system reported the helicopter’s GPS position and height every minute to a computer server via the Iridium satellite network. The operator connected to the server to monitor the helicopter’s progress. The last reported position was less than a minute before the accident and was made available for the search and rescue efforts. The Commission obtained recent records of the helicopter’s flight tracks for this investigation.
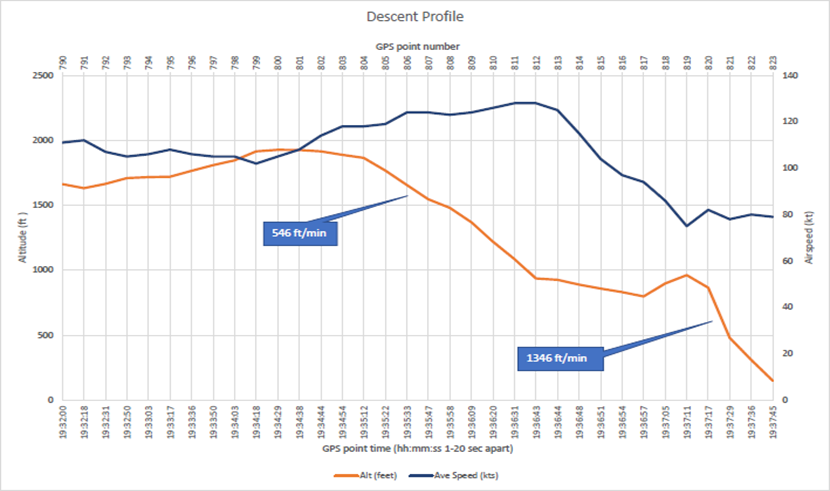
- The helicopter was also fitted with a Garmin 296 GPS with moving map display. This unit was recovered with the helicopter and transported to the Commission’s laboratory in Wellington. The unit was dried and cleaned, and the memory chip removed and connected to a chip reader. The GPS flight track (flight track included: Time, position, GPS derived altitude and heading. Ground speed is calculated from the data) was recovered from the memory chip. The data records covered the entire flight at a sample rate of between one and 20 seconds, including six points after the last known position from the TracPlus (see Figure 4).
Site and wreckage information
Flight path
- The helicopter’s flight path data from the GPS and the flight tracking system is presented in Figure 4. The orange points are from the TracPlus logged at 1 minute intervals and the blue points from the GPS logged at less than 10 second intervals (varies depending on GPS operating firmware). The GPS derived altitude at several points is marked in Figure 4. The last reported position on TracPlus was at just over 800 feet near Ewing Island, about one minute before the accident.
Wreckage
- The wreckage had been lying on the sea floor for 18 days and sustained additional damage during that time. The sea floor was rocky with rough gravel and coarse sand and covered with a light kelp forest.
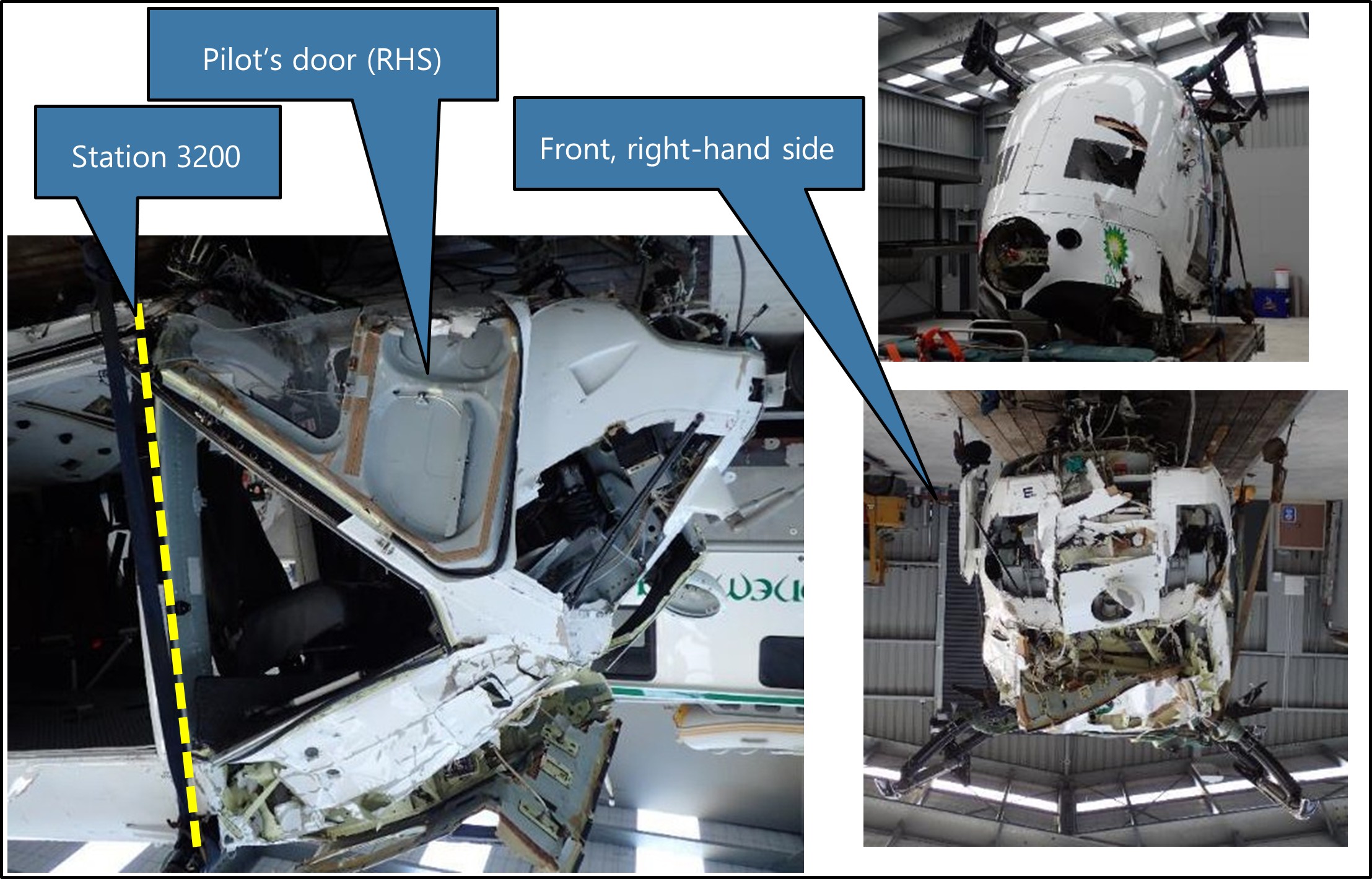
- The helicopter had been upside down, firmly resting on the sea floor, but able to sway with the water currents. The tail boom and tail rotor assembly had separated from the main body of the helicopter and drifted away. They were not recovered, but were still attached immediately after the accident (as seen in Figure 3). The left-hand sliding cargo door detached during the accident. It was found floating on the surface by a search vessel several nautical miles south, retrieved, and then returned when the vessel next berthed in New Zealand. The emergency exit window was still in place and had not been opened.
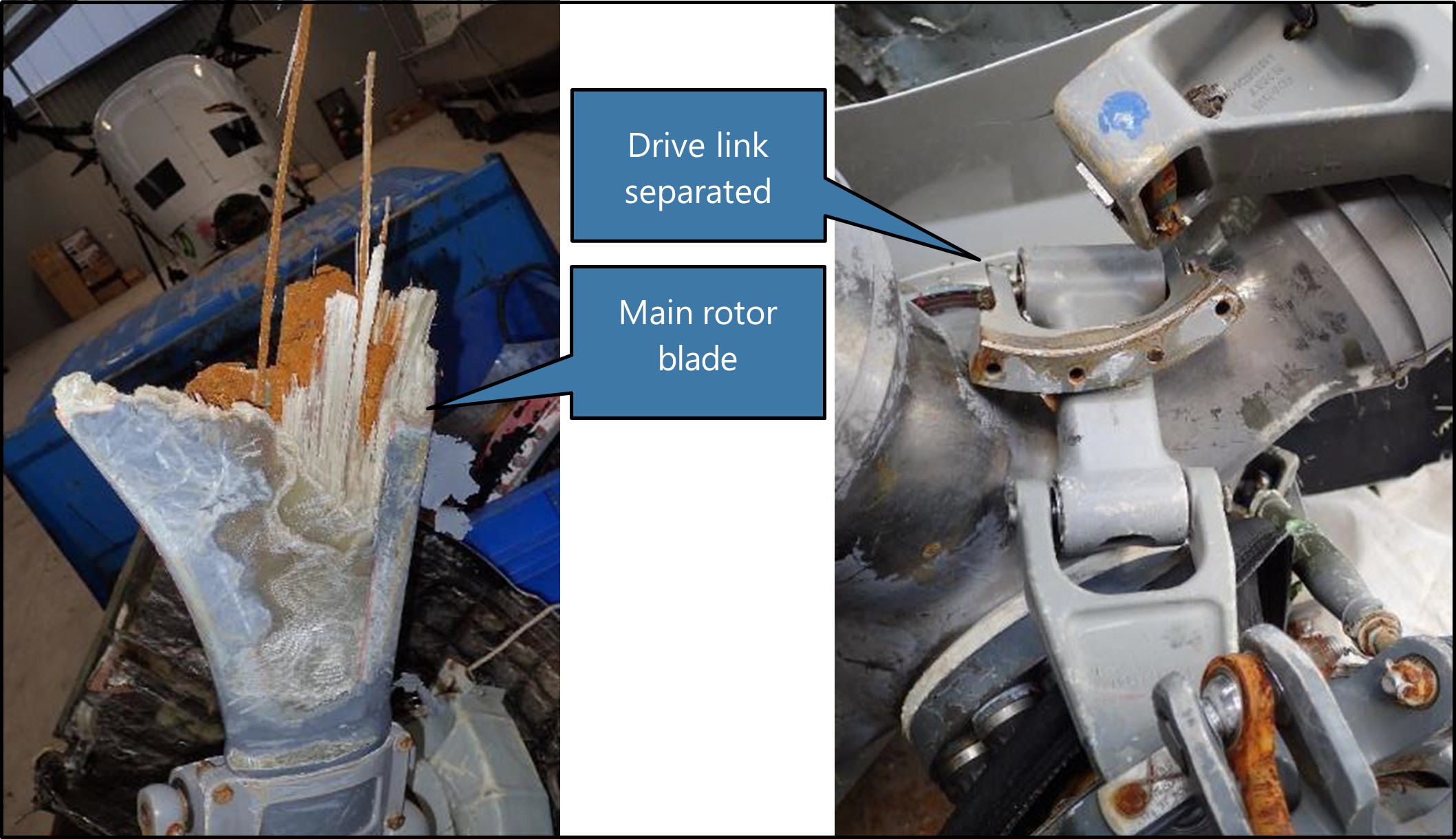
- The transmission and rotor head assembly and the remains of the main rotor blades attached to the rotor head had separated on impact. The transmission and rotor head assembly dropped about 20-30 metres away from the main wreckage. Three of the main rotor blade stubs had been ground down by abrasive movement with the sea floor. The splintered stub of the other one remained (see Figure 6). The main rotor blades were not retrieved. The pitch links had snapped at one end. The drive link attachment bolts to the rotor head had sheared and the drive link was distorted.
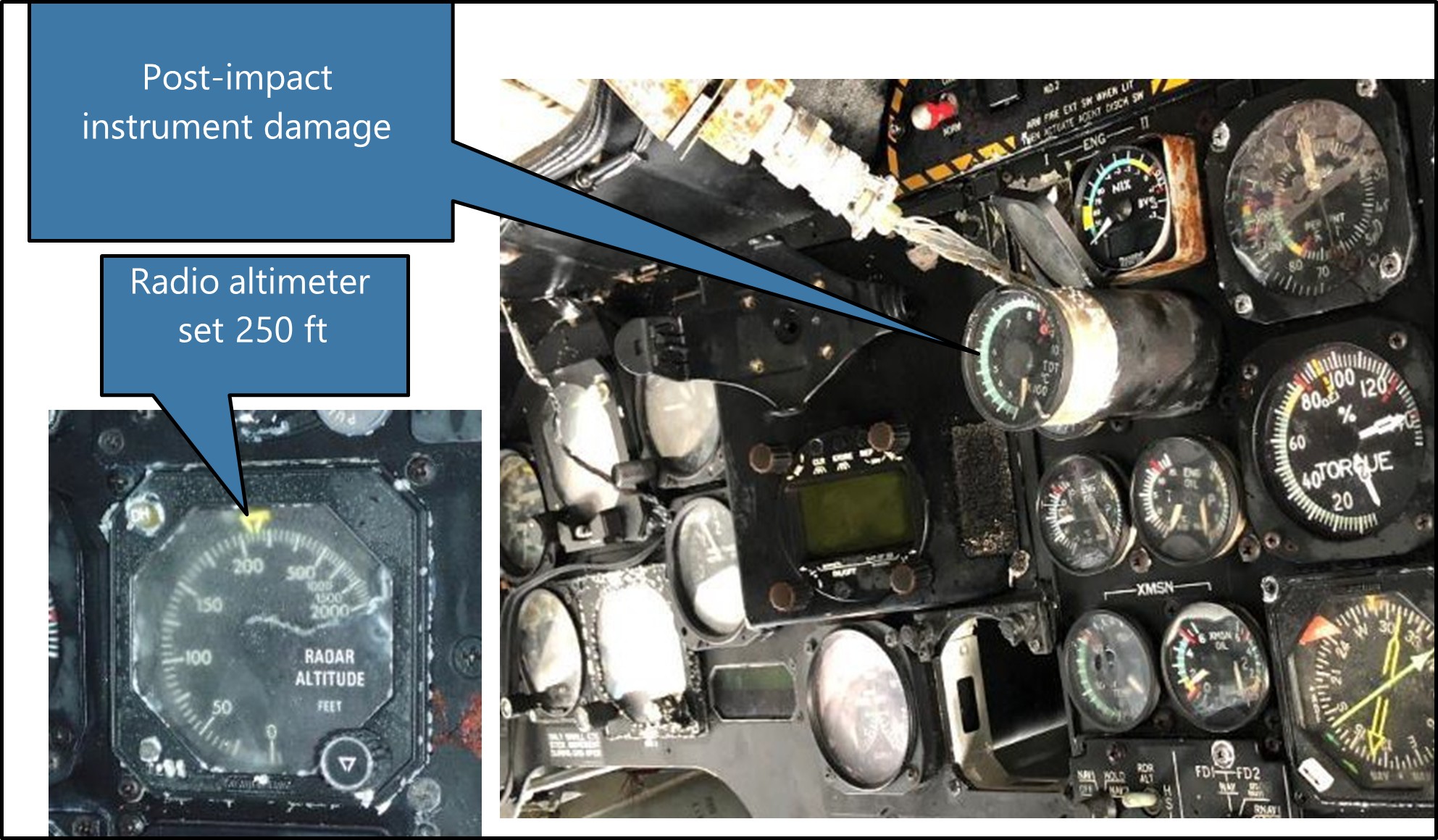
- The panels around the nose, front windows and instrument mountings were damaged by water impact. The cockpit floor had been forced upwards slightly and pivoted around a point in the floor where the front cross-brace for the skid penetrates, back towards the rear of the front door frame at station 320015 (see Figure 5). Some instruments had slid aft in their panel mounting very likely due to the impact-induced water pressure in the nose area behind them (see Figure 7).
- Damage to the wreckage was consistent with the helicopter impacting the water at speed, with the power on, and in a shallow angle of descent with a slight right-hand bank. The helicopter would have tipped forward until the main rotor blades contacted the water. This action would have rotated the helicopter fuselage up and around and then hard down onto the left-hand side. The transmission and rotor head and the two left-hand doors would likely have departed during this stage of the impact.
Survival aspects
- The crew were wearing immersion suits and helmets. The suits kept them warm in the cold water (about 10°C) and provided sufficient flotation for them not to activate their inflatable life-jackets.
- The helicopter flipped end-for-end and lay partially submerged for a short period of time. The cockpit was underwater, but the rear cabin was only partially under. The front crew were restrained to some extent by their harnesses. Both made their way out of the helicopter from underwater. All crew were trained and experienced in the techniques of escaping from a helicopter while underwater (known as HUET).
- The winch operator was sitting in the cabin sideways to the direction of impact with their back to the left side and seated just aft of the sliding door opening. Their seat was a standard KHI high-density, three-person seat running along the side wall of the cabin. The seats were designed to withstand forces of 4 G (front, back, left and right),
- The winch operator was flung forward and knocked unconscious. The sliding door detached in the accident sequence. The paramedic evacuated from the front left seat, and found the winch operator floating on their back in the cargo cabin and dragged them out of the helicopter. 1.5 G (upward) and 8 G (downward) with up to three persons weighing 80 kilograms. Each seat had a four-point harness with central quick release (the seat belt harnesses were replaced in accordance with Supplemental Type Certificate 5/21E/29 issued to National Aircraft Interiors Ltd, Nelson). The load capacity of the seat belts was 6.865 kN and the snap-on bracket was 15 kN. The winch operator’s left-hand seat belt snap-on steel bracket broke in overload where it attached to the seat base (see Figure 8).
- A four-person life-raft was in the helicopter, but proved difficult to identify in the darkness and was not retrieved before it sank. The approved life-raft was an EAM-T4 type (EAM is the manufacturer Eastern Aero Marine) manufactured in accordance with FAA TSO-C70a, Type II (this is the FAA Technical Standard Order that specifies the minimum performance standards for this type of life-raft). It was lying in amongst other cargo in a standard EAM container coloured ‘International Yellow’.
- The crew had emergency PLBs and other emergency gear in a grab-bag in the back cabin of the helicopter. It was not found before the helicopter sank. They did not have any emergency items on their person, except one crew member had a pocketknife and torch.

Night vision imaging systems (NVIS)
- An NVIS collectively refers to each of the elements that are required to safely operate an aircraft using NVGs. In addition to the NVG unit itself, NVIS elements include the following:
- Components on board the aircraft to support the use of NVGs, such as compatible lighting systems, external illumination lighting, and radio altimeters to indicate clearance height from the surface.
- Operational procedures, including flight planning and risk management to ensure NVG flights are conducted when environmental conditions are suitable (eg, not less than VFR meteorological minima and illumination criteria).
- Training, competency and currency requirements for personnel using NVGs.
- Airworthiness (maintenance) requirements for both the aircraft components and NVG equipment, including pre-flight procedures to ensure functionality.
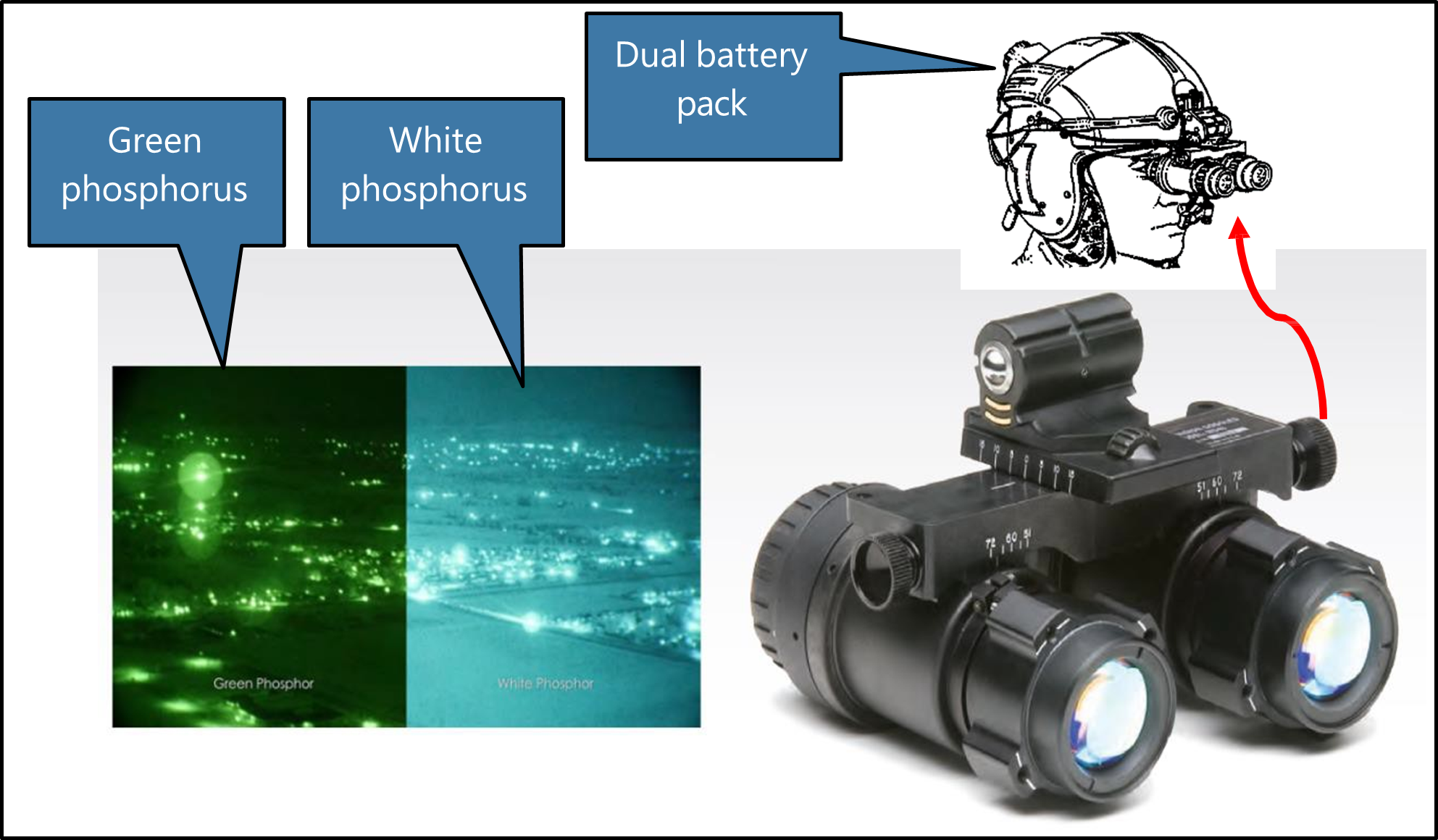
- NVG use enhances a pilot’s ability to operate in dark and low-light conditions by receiving and intensifying ambient light, resulting in an amplified light image that is presented to the eye (Parush, 2011). The intensifier tube section of NVGs has a maximum response within the infrared light range that is not visible to the human eye. The amplified electron stream generated within the intensifier tube is then focused onto a phosphor screen, which reproduces the image in shades of green light that is visible to the eye. (The recent option of white phosphor offers some improvement in clarity).
- The device is head-mounted and self-contained by way of a battery pack that is positioned at the rear of the head to counter the weight of the goggles sitting over the operator’s eyes (see Figure 9). Additional weights can be added inside the battery pack to balance for individuals. Used correctly, in most conditions NVGs provide a pilot with a significantly enhanced means of distinguishing the horizon, objects, terrain and weather when compared to unaided night vision.
- Advancements in NVG technology have improved both physical comfort and image quality compared to earlier generation models. There are, however, inherent limitations associated with NVGs. These include:
- Visual acuity: This is related to the luminance of the NVG screen, which varies as a function of the ambient light (eg, full moon versus overcast starlight). NVG-assisted acuity declines with decreasing celestial illumination. Acuity is also related to target contrast and deteriorates more rapidly for low-contrast items when illuminance levels decline.
- Monochromatic image: Colour differences between components in a scene aids recognition of objects and discriminating between them, as well as assists with depth perception and distance estimation. The lack of colour variation in the NVG image (shades of white or green) degrades these capabilities to varying degrees.
- Limited field of view (FOV): In normal vision, an unaided FOV covers an elliptical area of approximately 120 degrees laterally and 80 degrees vertically. This is reduced to around a 40-degree circular area when wearing NVGs, significantly reducing peripheral vision in particular.20
- Physiological implications: While NVG units and helmets are adjustable to an individual, muscle fatigue, neck strain and headaches can occur, particularly with prolonged use. They can also conflict with other apparel such as flying jackets, immersion suits and life-jackets.
- NVG image quality is variable, depending on the operating environment, atmospheric conditions and the degree of illumination. All NVGs require some illumination of the subject and reflectance of that illuminance back to the NVG lens to produce an image. For example, light rain or mist is generally not as easily perceived when compared to dense clouds and large rain droplets, but will affect contrast, distance estimation and depth perception. Featureless terrain (such as large bodies of water) have a distinct lack of contrast, particularly when there are no distinguishable white caps or enough surface disturbance to reflect light back to the NVG observer (CASA, 2022).
- Illumination can be either artificially or naturally acquired. The moon provides the greatest source of illumination, and both the phase and elevation will determine how much moonlight will be available. Lunar illumination is expressed in percentages (100 per cent illumination being a full moon). Information about illumination levels can be obtained from the moon data in the ‘Time and Date’ website (Timeanddate.com, 2022) or through a dedicated software package such as Met Office Night Illumination Model (MONIM) from the UK Met Office. Sky glow also contributes to natural lighting levels and is dependent on latitude and the time of year. Cultural lighting, or the artificial lighting sources common with human habitation, also contributes to night illumination.
- Due to the many possible combinations of the variables that will affect image quality, NVG users require techniques to help interpret images in different circumstances. Such techniques include an understanding of how to use terrain features (this includes cues such as object size, shape, contrast and shadows), to aid visual recognition and the ability to determine distance information, depth perception and closure rates. Given that NVIS operations take place at night (albeit with better visual acuity than unaided night operations), the limitations associated with NVG use means that pilots and crew are still susceptible to the visual illusions typical of night VFR that can affect loss of a reference horizon.
Night vision goggle (NVG) helicopter operations
Aviation rules
- There are currently no CARs regulating the equipment or conditions of use of NVGs during flight within New Zealand. Instead, information about the standards, practices and procedures for the safe use of NVGs is provided by way of an Advisory Circular (AC), AC91-13 Night Vision Imaging Systems – Helicopter (The AC was developed as a means of facilitating the introduction of NVIS into the New Zealand civil aviation environment and draws extensively on documentation from the RTCA and the FAA). The CAA formalise NVIS operations through their approval process for issuing an operator’s AOC.
- The AC states that it relates to helicopter operations conducted under CAR Parts 91, 119 and 135. All references to rules are from within the AC (eg, the content of an AOC, equipment standards and maintenance requirements). The rules do not make any cross-reference back to the AC or mention the terms NVIS or NVG. At the time of the accident, AC91-13 had undergone one revision and this was effective as of 20 June 2011 (CAA, 2011). The initial issue date was not published.
- The AC includes information on the acceptable technical standards for an NVIS and the associated aircraft installations. It also provides guidance for appropriate operator procedures, training programmes, pilot competency and currency requirements, and the maintenance requirements to safely utilise NVGs during night VFR flight in helicopters.
- Each operator who wishes to use NVIS is expected to define their own NVG operating procedures, which they may base on the AC or not. The AC lists three Radio Technical Commission for Aeronautics (RTCA) documents that formed the foundation of civil NVG operations in the USA and Europe and would be acceptable to CAA for use in New Zealand.
- This operator had integrated the requirements of AC91-13 into their exposition.
-
Similarly, there were no CARs covering Helicopter Air Ambulance (HAA) (this term is preferred to HEMS by the FAA and has been adopted for this report) operations within New Zealand. The CAA clarified this by stating that:
There are no specific Civil Aviation Rules (CARs) for Helicopter Emergency Medical Services (HEMS) operations. However, all operators that engage in HEMS operations operate in accordance with CAR Pt 119, CAR Pt 135, CAR Pt 91 and CAR Pt 133.
Equipment requirements
- The primary helicopter equipment required for NVIS is an internal and external lighting system, both of which must be specifically compatible for NVG use. Installation of an NVIS into a helicopter is deemed to be a ‘major modification’ and must include a Flight Manual Supplement. For the holder of an AOC, evidence of an NVIS compatibility inspection is recorded on the Operations Specification and it expires after two years.
- The helicopter was listed on the operator’s AOC and the NVIS inspection was current to 20 December 2020.
- The AC adopts the FAA standards referred to in FAA AC27-1B with differences for New Zealand. The AC also lists ancillary equipment for an NVIS equipped helicopter as being: a radio altimeter, skid/slip indicator, gyroscopic attitude indicator, gyroscopic direction indicator or equivalent, and vertical speed indicator. Given the reduced FOV a pilot has when ‘goggled up’, these instruments are required to be positioned in such a way so as to reduce the amount of head movement required to view them and therefore minimise the potential for spatial disorientation. Instruments and cockpit displays must be capable of being viewed with unaided vision (ie, for the crew to look at them underneath their NVGs).
- The radio altimeter fitted to the helicopter had a maximum range of 2500 feet and single display in the pilot’s instrument console. The pilot could select the height setting bug to any height under the maximum range and a visual alert would illuminate while the helicopter was less than that height from the surface. It did not have an audio alert function (see Glossary for altimetry).
NVIS pilots
-
The recommended requirements for pilots wishing to become certified for NVG use are described in AC 91-13 under NVIS Pilot Prerequisites. The minimum licence requirement is a private pilot licence (PPL), but the flight experience and performance parameters are broadly based on those that are required for the issue of a CPL with a night endorsement. This includes the ability to demonstrate instrument flight proficiency, and the AC notes the following:
…the emphasis is for a pilot flying night VFR utilising NVIS to obtain, and maintain, proficiency in instrument flying skills. It is recommended, but not essential for the pilot to hold an instrument rating. The holder of an instrument rating will be better placed to cope with the night VFR/NVIS environment.
- Pilots must complete an approved NVIS ground training course with a minimum syllabus outlined in the AC. Generic topics include aeromedical, NVG theory, interpretation of NVG imaging, environmental factors and NVIS flight planning. Operator-specific training is also covered, as is aircraft ground training for familiarisation of NVIS equipment on the helicopter. There are no recommended teaching times specified for any of the subject matter.
- A minimum of five hours of approved NVIS flight training is required. Once a pilot has passed their initial flight check, their logbook will be certified with a night flight endorsement to use NVIS.
- NVIS currency requirements include recency of NVIS experience and an annual proficiency check with an NVIS certified flight instructor or examiner. The AC refers to CAR 61.37 Recent Flight Experience, which defines that to remain current a pilot must complete at least three take-offs and landings at night within the last 90 days.
- Recurrent training consisting of the initial flight check syllabus and selected elements of the initial ground theory course is required to be conducted on an annual basis. The proficiency check must represent a typical NVG flight operation and include demonstration of the ability to cope with both a NVG malfunction and recovery from inadvertent IMC penetration.
- CAR 61.29 describes the requirements for pilots to record their flight time in their logbook. There is no requirement to differentiate between VFR night flight and NVIS night flight using NVGs.
NVIS crew members
- In addition to the minimum requirement of having at least one NVIS trained pilot when operating with NVGs, the AC allows an operator to utilise a second trained NVIS crew member when considered necessary for safe operations.
- The AC defines an NVIS flight crew member as being a trained crew member who is required to perform essential inflight duties to ensure safe operation of the aircraft during NVG flight operations.
- A crew member may be a second NVIS trained pilot, but this is not a requirement. According to NVIS Crew Member Training Prerequisites in the AC, the minimum qualification and experience for a person wishing to become an NVIS crew member are only those specified by the operator and documented within their exposition.
- To become a certified NVIS crew member, individuals must complete the same NVG ground theory syllabus as pilots. Once completed, a crew member must undertake a minimum of two hours of NVIS flight training and checking with an approved organisation (a Part 141 certified training organisation or an air operator certified in accordance with Part 119 provided the certification authorises NVIS training and checking). The flight training syllabus covers selected elements of the more extensive syllabus for pilots, specifically preparation, emergency procedures, CRM and post-flight procedures. Any special procedures specific to the type of operation (eg, winch training) must also be covered.
- Once a helicopter crew member has been endorsed as a qualified NVIS crew member, this is acknowledged by way of a certificate (as NVIS crew members are not required to be pilots, a certificate takes the place of a logbook endorsement), which is to be retained in the operator’s files. Crew are not to act as an NVIS crew member unless they have either completed three NVG flights in the preceding 120 days or have completed their initial or recurrent training within that time. Recurrent training consisting of the initial flight check syllabus and selected elements of the initial ground theory course is required to be conducted annually.
- Each operator must ensure that crew members are trained and competent to perform their assigned duties (in accordance with Subpart I (Training) CAR Part 135)). Section 3.2.1 NVIS Crew Member of the AC states the following about the duties a crew member is expected to perform as part of an NVIS operation:
An NVIS crew member needs to – Participate in crew briefings prior to each shift to:
- become familiar with the general weather conditions
- confirm that the NVIS equipment has been pre-flight checked
- know any restrictions to NVIS flight operations; and
-
participate in crew briefings prior to a NVG flight operation to:
- obtain a general knowledge of the weather conditions along the route of the flight
- obtain a general knowledge about obstacles and significant terrain along the route of flight; and
-
during a NVG flight operation:
- use crew resource management principles to maintain crew situational awareness; and
- maintain appropriate cockpit and other aircraft lighting discipline.
Risk management for NVIS operations
- As part of NVIS operations, the AC recommends an operational risk assessment be performed before any NVG flight (AC91-13 3.3 Operational Risk Management Procedures), with at least the following points being considered:
- Illumination level of the flight environment.
- Forecast and reported weather conditions along the intended route and at the intended destination.
- Recency of experience for pilot and crew.
- Crew composition.
- Operator/crew experience with NVG flight operations.
- PIC field of regard.
- PIC/crew rest condition and health.
- Aircraft serviceability (MEL & Tech Log)
- Windshield/window condition.
- NVG tube performance/battery condition.
- Types of operation allowed and applicable standard operating procedures.
- External lighting environment.
- The operational risk assessment is covered as part of the Preparation component of the flight training syllabus for pilots. It is also taught during the NVIS Flight Planning component of the ground theory syllabus and is a selected element required to be repeated during ground theory recurrency.
Tests and research
- The illumination level at Auckland Islands at the time of arrival could be predicted. One method was to use a software product available from the United Kingdom (UK) Met Office, but there is also information published on public websites.
- The UK Met Office was contacted by the Commission to obtain an illumination prediction for Auckland Islands around the time of the planned medivac flight arrival. They used their product MONIM, which supersedes their previous versions called ‘Night Illumination’ as used by the RNZAF. The UK Met Office provided a graph of the predicted night illumination at Auckland Islands, which showed that the natural illumination was least at about 1930 (see Appendix 4). At that time, it was predicted to be about 0.3 millilux. It would rise to over 10 millilux after 2200, but actual illumination was still dependent on cloud cover, so could be less.
- Illumination of one lux (1000 millilux) is that of a candle projected onto a flat surface 1 metre square at 1 metre distance from the candle. A typical level of illumination on the ground at night from a full moon is about 300 millilux, which drops to about 1 millilux when the moon is below the horizon.
Previous occurrences
- Some previous occurrences with relevant conditions are described below.
- New Zealand, 17 December 2020, CAA incident 20/6775, BK117 B-2, Gowanbridge. During a patient transfer at night using NVGs in a single-pilot VFR operation the pilot lost spatial orientation. The NVIS crew member, who had by chance decided to sit in the front left seat, assisted the pilot to recover and land. There were four people on board with no injuries. The CAA’s investigation concluded that the contributing factors were the pilot’s unfamiliarity with that helicopter, a distracting source of light, very low natural illuminance, and a higher-than-usual mental workload maintaining visual reference with traffic on a road.
- USA, 10 December 2015, NTSB WPR16FA037, Bell 407, McFarland, California. An HAA flight was on a patient transfer VFR operation at night using NVGs. The helicopter began to descend and then entered a left descending turn. The ground speeds were fluctuating, and the descent rate was about 2210 ft/min until impact. There were four fatalities. Conditions at the time were likely to include fog and rain. The pilot had an instrument rating, but with only 2.3 hours on NVGs in the last seven months before the accident and 11 hours on the helicopter. The National Transportation Safety Board (NTSB) investigation concluded that the probable cause was that the pilot lost control while attempting a course reversal after inadvertently entering an area of reduced visibility. The pilot’s lack of recent NVG experience was considered to have contributed.
- Baltic Sea, 28 February 2014, BFU 3x006-14, BK117 C-1, 3 nm north of Prerow. During VFR night-hoist training with two pilots (both Airline Transport Pilot Licence (ATLP) holders) the helicopter collided with the sea with three fatalities and one survivor. The pilots were not using NVGs. The German Federal Bureau of Aircraft Accident Investigation (Bundesstelle für Flugunfalluntersuchung) BFU investigation concluded that the contributing factors included: lack of experience with this type of operation, airspeed and rate of descent were not stabilised, insufficient monitoring of instruments, loss of situational awareness in combination with loss of control, and non-reaction to visual and audio altitude warnings on the radio altimeter.
- USA, 5 February 2010, NTSB CEN10FA113, AS350, El Paso, Texas. Pilot and two paramedics on a simulated night pick-up in the desert. The helicopter banked about 45 degrees then entered a steep nose-down attitude and impacted the ground. Three fatalities. Pilot was using NVGs and a non-NVG spotlight to illuminate the ground. It was a 0 per cent moonlit night with very little cultural lighting and low contrast. The pilot had recently completed training with NVGs, but it had been on nights with more moonlight. The NTSB investigation concluded that the probable cause was the pilot’s loss of situational awareness due to unfamiliarity with the hazards of low-contrast area while using NVGs.
Organisational information
- The operator’s exposition defined their authorised operations as Part 135 air transport and CTOs in New Zealand and Antarctica that included VFR day and night and NVG flight operations. The operator had also been approved to conduct CTOs beyond the New Zealand flight information region (NZFIR) over the previous 20 years.
- Helicopters operated by the company included eight on the company register and six leased. The types operated included BK117, AS 350, R44 and EC120.
Emergency locator transmitter
- The helicopter was fitted with an emergency locator transmitter (ELT) model Artex C406-1HM. The ELT is designed to activate automatically on detection of impact G-forces more than 2.3 G in the forward direction of crash impact and 12.5 G in the other five perpendicular axes (rear, left, right, up and down). Units made after 2019 have a sensor with a lower threshold of 6 G to 8 G. It would then start transmitting an emergency signal within the next 60 seconds. The unit is mounted at the base of the tail boom and the antenna on the cabin roof. It will transmit a low-power amplitude modulated signal on 121.5 and 243 MHz and a digital signal burst on 406.025 MHz.
- No alert signal was received from the ELT by the RCCNZ.
- Weak signals were occasionally detected by the searching RNZAF Orion aircraft on 406.125 Mhz and suspected to be from the ELT, but a location fix could not be obtained. This was approximately 12 hours after the accident. The helicopter had sunk and was lying upside down on the sea floor at the time at a depth of about 15 metres.
- The manufacturer believed it unlikely that the ELT would have radiated a signal from the antenna while underwater.
- The crew had PLBs on board in a grab-bag, but they were lost when the helicopter sank.
Analysis Tātaritanga
Introduction
- The operator regularly flew helicopter operations in the Southern Ocean down to Auckland Islands and Campbell Islands so had established a procedure with remote accommodation and fuel replenishment facilities. This flight was similar in that it was a long-distance positioning flight over water to a remote base where they would conduct shorter local flights. At the completion of the local flights, they would prepare and conduct the long return flight. The helicopter’s GPS navigation system already had the waypoints and local landmarks stored in its database for these Southern Ocean flights.
- The pilot had appropriate flight experience with the operator, including meeting the minimum recency with NVGs and the required company authorisations to conduct this flight. They had also flown the route once before in daylight.
- The pilot and crew members were trained and proficient in underwater escape techniques from a submerged helicopter and they were wearing full immersion suits. These safety considerations kept the crew alive and buoyant in the cold water.
- The following section describes what happened and then analyses the circumstances surrounding the event to identify those factors that increased the likelihood of the event occurring or increased the severity of its outcome. It also examines any safety issues that have the potential to adversely affect future operations. Safety issues that influenced this accident were identified as:
- Single-pilot VFR operations into the Southern Ocean.
- Regulatory void for NVIS and air ambulance operations.
- CRM training in helicopters.
- Lastly, two safety issues regarding helicopter loading and survival equipment are explained. These safety issues were identified during the investigation as safety factors that increased risk, but were not considered to have had a causal effect on the accident. However, they are regarded as safety issues because of their systemic nature and risk to other helicopter operations.
What happened
- The impact forces and damage to the nose area showed that the helicopter had impacted the sea at a shallow angle, but at a speed that was consistent with the crew's accounts. Post-accident inspection of the helicopter, supported by interviews of the crew, showed that the helicopter was operating normally with the main rotors being driven by the engines when they were suddenly stopped by impact with the water. It was also determined that the helicopter had sufficient fuel remaining to safely land.
- The helicopter arrived at Auckland Islands after dark at about 1930 and the pilot was using NVGs, as was the paramedic who was acting as NVIS crew member for the flight. The islands are uninhabited so had no artificial lighting to assist the NVG illumination. The only illumination was from the celestial night sky, but that was consistent with the crew's accounts. Post-accident inspection of the helicopter, supported by interviews of the crew, showed that the helicopter was operating normally with the main rotors being driven by the engines when they were suddenly stopped by impact with the water. It was also determined that the helicopter had sufficient fuel remaining to safely land.
- The helicopter arrived at Auckland Islands after dark at about 1930 and the pilot was using NVGs, as was the paramedic who was acting as NVIS crew member for the flight. The islands are uninhabited so had no artificial lighting to assist the NVG illumination. The only illumination was from the celestial night sky, but that was limited by local cloud and atmospheric conditions. The moon had not risen by this time and the predicted night-time illumination was at its lowest level for the night.
- Both the pilot and NVIS crew member said they saw the hills as they approached Auckland Islands and a cloud layer over the landing area with an opening wedge from the northwest. The pilot recalled seeing the outline of Port Ross and part of Enderby Island. They also both recalled seeing the cliffs a few seconds before the accident. The winch operator in the rear cabin did not have NVGs on and recalled that it was too dark to see outside. This shows that the NVGs were functioning and complementing the front seat crew’s night vision at the time of the accident. They also recalled that after the accident, while swimming around the helicopter and recovering items from the wreckage, there was sufficient ambient light for them to see the cliffs 100 metres away with unaided vision.
- The pilot saw cloud that covered the landing point and a very dark area adjacent that they interpreted to have been clear of cloud. The pilot expressed this opinion to the NVIS crew member who accepted that explanation. The cloud was below their current altitude of between 1500 and 2000 feet and was very likely to have been sea fog. The dark area would very likely have been an absence of reflected light from the calm sea surface to the crew.
- The pilot described their intention to the NVIS crew member to descend in the area clear of cloud and then follow the coastline back towards the landing point. If that was not possible, they would head to a higher landing point and camp out the night. The GPS had several suitable landing points saved in memory from previous trips. The pilot said that the coastline is usually more clearly defined through NVGs due to the greater light scatter from the rough surface.
- The pilot set the radio altimeter reference to 1000 feet and started a descent. According to the GPS log, this descent rate from 2000 feet to 1000 feet was slightly over 500 ft/min and at approximately 125 knots (see Appendix 5). The NVIS crew member started to read out the altimeter heights. The pilot did not expect the crew member to do this, ask for it, question the source of the information, or stop it. The NVIS crew member was reading from the left-hand barometric altimeter, which was still set at the reference pressure for their departure at Invercargill. While the local QNH33 for Auckland Islands was available to the operator, this was not provided to the pilot. Based on the pressure difference, the barometric altimeter would have been displaying about 50 feet higher than the helicopter actually was above the sea surface.
- The pilot set the radio altimeter reference to 1000 feet and started a descent. According to the GPS log, this descent rate from 2000 feet to 1000 feet was slightly over 500 ft/min and at approximately 125 knots (see Appendix 5). The NVIS crew member started to read out the altimeter heights. The pilot did not expect the crew member to do this, ask for it, question the source of the information, or stop it. The NVIS crew member was reading from the left-hand barometric altimeter, which was still set at the reference pressure for their departure at Invercargill. While the local QNH for Auckland Islands was available to the operator, this was not provided to the pilot. Based on the pressure difference, the barometric altimeter would have been displaying about 50 feet higher than the helicopter actually was above the sea surface.
- After reaching 1000 feet, the pilot had slowed to about 80 knots and maintained about 900 feet for about three minutes (see GPS flight record in Appendix 5). The helicopter was making a gentle turn from south through west towards a final track to the north. The pilot reset the radio altimeter to 500 feet and continued to descend. According to the GPS, the descent rate was above 1200 ft/min, which is consistent with the pilot’s account of descending into the clear area. The NVIS crew member was concerned about the descent rate and called out to the pilot to check their “speed”. The NVIS crew member was not a pilot, or trained to have any flying capability such as the reading and interpretation of instruments, or trained in the use of correct aviation terminology. The pilot was confused by the call (see paragraph 3.30), but happy with the airspeed so carried on.
- After reaching 500 feet, the pilot reset the radio altimeter to 250 feet and continued to descend. This height above sea level would have been clear of the local terrain. The pilot recalled seeing the radio altimeter alert light illuminate, but said that they did not continue to monitor the height.
- The NVIS crew member was reading out the barometric altitude as they descended, and it became steady at 200 feet for several calls. The NVIS crew member was also looking out and noticed a cliff face directly ahead that they were closing in on very fast. These were the cliffs to the south of Crozier Point. The cliffs were 20 metres high above the beach (66 feet) and then the land is almost flat from there across the peninsular to Port Ross. The NVIS crew member immediately alerted the pilot who also saw the cliffs and started to flare and bank right to avoid hitting them. Without any further warning, the helicopter impacted the sea.
Why did the helicopter impact the sea surface?
- The Commission found that several factors contributed to this accident. Each of those factors is described below under separate headings.
Flight planning
- This flight was initially planned to have been completed in daylight.
- The operator’s exposition included helicopter flights deep into the Southern Ocean from New Zealand to Auckland Islands and Campbell Islands. They also operated local flights in the Antarctic. They had established procedures, remote bases and the infrastructure to support these types of operations.
- The pilot was experienced in the company’s operations in New Zealand, the Antarctic, and had flown once before to Auckland Islands. The pilot had about 73 hours of experience flying at night and met the operator’s minimum NVG currency of three take-offs and landings within the last 90 days. They were also current with their knowledge of the company’s operational procedures, NVIS competency and the Part 135 operations flight crew competency check.
- The NVIS crew member was trained and current in NVG operations, HUET and CRM. They had flown two previous medivac flights to Auckland Islands with another pilot. They had also flown one local NVG medivac with this pilot from a Southland site a few days before. The NVIS crew member had just under 200 hours of experience in that role on NVGs.
- The risk profile changed as the day progressed, but the plan remained the same. The first step change to the risk profile was due to the delay in departure while waiting for the medical supplies to arrive. This delay meant that the landing at Enderby Island would be at night and it required the illumination level at the destination to be considered,34 along with a night descent procedure over water on NVGs.
- One of the known risks while using NVGs is the potential loss of contrast that a flat calm sea creates. It makes height judgement more difficult and the sea surface may not be visible through NVGs. These types of situations are described in AC91-13 (CAA AC91-13, section 3.2.3 Overwater operations) and in the operator’s exposition (SLH Exposition V17.21, Overwater Night HNVGO operations) (see Appendix 6 for the extracted text from the Exposition). It is possible to gain a significant improvement in safety by the NVIS crew member contributing to the pilot’s situational awareness in a more effective way. This is explained later in the section on CRM.
Pilot had minimal NVG recency
- The flight was progressing normally as they flew south in daylight. The situation changed after night fell and the crew were wearing NVGs. The second step change in risk profile occurred when the crew realised that the landing point was covered in cloud.
- It was getting near to the maximum duty time for the pilot. The exposition allowed for up to 8.5 hours flying in any 11-hour period, but had no weighting for NVG time. AC119-3 (AC119-3 Air operation certification – Part 135 operations) provides examples for flight and duty time and suggests a weighting multiplier of 2.3 for every hour flown on NVGs. The pilot had completed a short flight in the morning before this operation. It had been about four hours of flying since they left Te Anau with about three hours of planning and waiting for medical supplies before that. As there was not enough fuel to return to the mainland, the crew were committed to landing somewhere on Auckland Islands.
- Although the pilot met the minimum requirement to remain current with NVGs, the actual logged flight time on NVGs over the last 90 days was less than one hour. The required three take-offs and landings had been part of two separate flights that had extended into night, and the take-offs and landings were not needed for the operations, but were made after dark to remain current with night VFR. The pilot’s last flight crew competency check on NVGs was conducted four months before the accident flight. Low-level flight over water was not checked in that flight check.
- CAR 61.29 defines what information pilots must log in their logbooks. It does not differentiate between VFR or IFR night flight and night flight using NVGs. It just requires a record of flight at night for both VFR and IFR. The pilot did not record their NVG flight time separately and some of that total night-time included an initial night VFR rating. The two separate VFR night flight records could be merged for any pilot and a pilot’s logged night flight is therefore ineffective to determine recent flight experience in either night VFR or NVG at night.
- With more currency on NVGs, the pilot may have questioned their impression of a dark area beyond the cloud. With a different expectation from the CRM, the NVIS crew member may have been more effective in challenging the pilot’s perception. They had experienced a low layer of fog about an hour earlier in the flight during daylight. At that time the sea surface state and the wind direction would have been visible and may have helped to anticipate conditions at their destination.
Unstable descent near the surface
- The next step change in the risk profile occurred when the pilot made a steep descent near the surface on NVGs and continued below their selected reference height.
- The exposition (SLH Exposition V17.21, Overwater Night HNVGO operations) stated that the maximum descent rate on NVGs was 300 ft/min and for pilots to use the radio altimeter both on descent and while in the area, setting the decision height alarm accordingly. The GPS record showed that the pilot descended initially at about 500 ft/min down to 1000 feet above the surface, then at over 1300 ft/min until just before impact.
- The last radio altimeter setting was found to have been 250 feet. A controlled descent and level off at this height would have allowed the pilot to search for visible ground references through the NVGs or use the pilot-controlled spotlight to assist. The pilot said they set the decision height on the radio altimeter, but then did not control the helicopter to remain above that set height. The pilot recalled that they were primarily looking outside while noting the NVIS crew member’s calls and judging the helicopter’s height using depth perception. When the pilot saw the cliffs, they recalled being surprised that the helicopter was lower than expected, indicating a disparity between their situational awareness and the actual position of the helicopter.
- The NVIS crew member became concerned about the descent rate and attempted to challenge the pilot. However, the terminology used did not convey that message to the pilot. The word “speed” directs a pilot to verify the aircraft’s airspeed (forward speed through the air) and they would do this by looking at the airspeed indicator. To draw a pilot’s attention to the aircraft’s rate of descent, the correct terminology would be “descent rate”, which is shown on the vertical speed indicator. The NVIS crew member’s training was limited to observing for obstacles during take-off and landing and providing directional clearance information to the pilot. With more appropriate CRM training (see later at CRM training for helicopter operations), the NVIS crew member’s assistance could have been more effective as a risk control.
- The pilot did not have an instrument rating. Not having an IFR rating meant they were likely more reliant on external visual references for flight attitude than referring to instruments. A descent at night on NVGs with minimal celestial lighting required more reliance on the radio altimeter and GPS and familiarity with their use. With the reduced FOV through NVGs, it is also likely that the pilot was fixated on looking outside for ground reference to the detriment of an instrument scan inside. It is possible that the descent would have been better controlled if the pilot also had an instrument rating and was proficient at switching between visual and instrument reference systems.
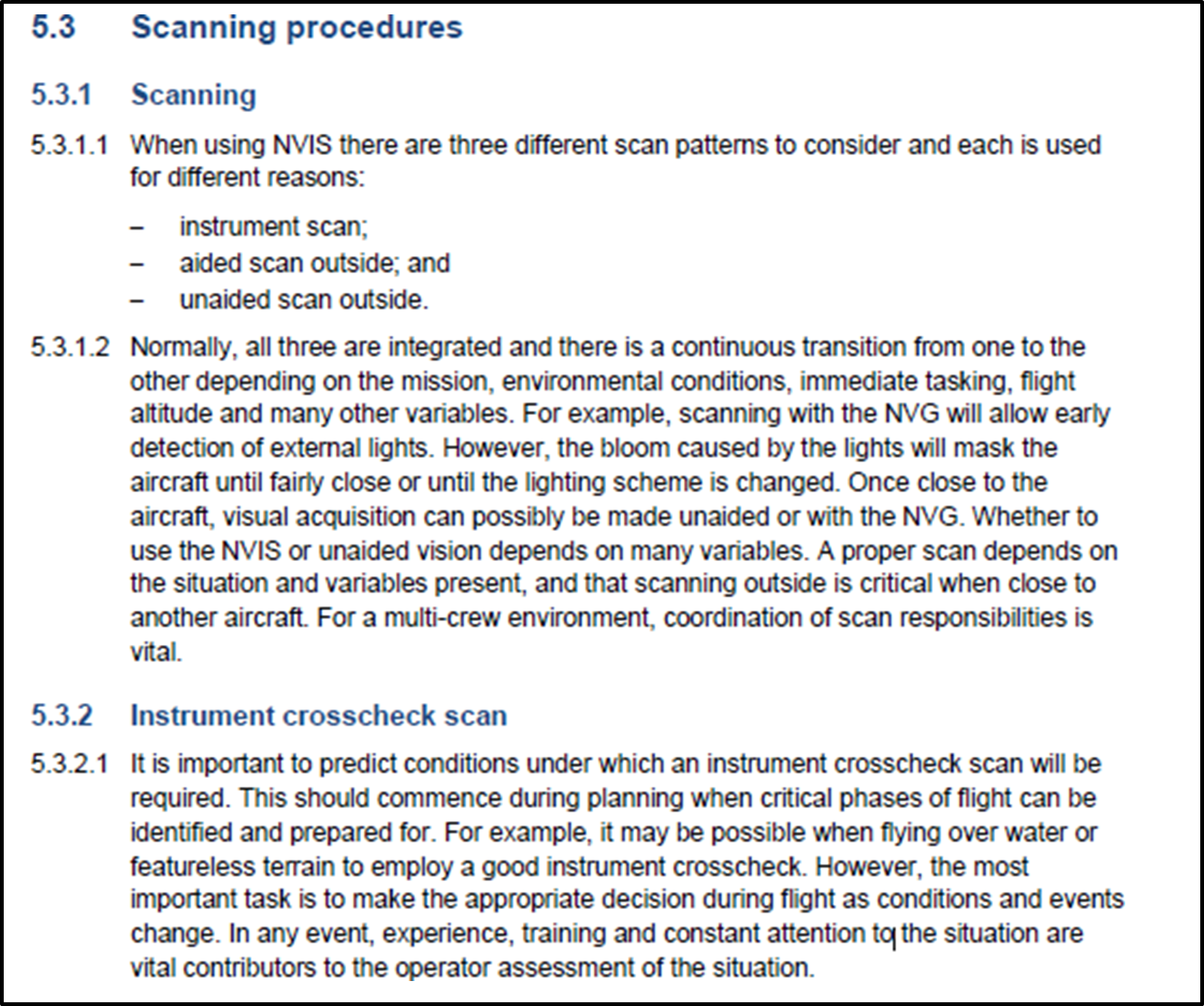
- An extract below from the Australian CASA Advisory Circular, Multipart AC 91-13 (CASA, 2022) describes scanning procedures while flying with NVGs. Under high workloads, CRM is an effective safety measure with scanning. The AC states that for a multi-crew environment, coordination of scan responsibilities is vital.
Other factors
- Two other factors also contributed to this accident – single-pilot VFR operations into the Southern Ocean and CRM. They are covered later in more detail.
Single-pilot VFR operations into the Southern Ocean
Safety issue: The operator’s procedures for single-pilot VFR operations into the Southern Ocean were not complete or adequate at the time of this accident to safely manage the flight.
- This type of operation carried a significant amount of risk over more common medivac operations within the NZFIR. The helicopter had a normal duration on internal tanks of two hours, but the flight south was beyond that range. Extra fuel had to be carried in external pods and the helicopter needed to be refuelled just before leaving the NZFIR. Cargo weight was critical with extra gear needed for the helicopter winch extraction, patient care, passage over the sea, overnight stay and remote refueling. The weight of the cargo was limited by the extra fuel carried and would be further constrained with the patient weight on return (see Helicopter loading).
- The crew were aware that they would be landing after dark and would be using NVGs for the approach and landing to an unlit and uninhabited remote island. They needed additional skills and equipment to conduct this flight and to be current in its use. They also needed to assess the weather at the landing point and if they had time to reach it while the visibility conditions and illumination levels were still suitable for night VFR.
- At some point along the way they would reach a decision point from where they could still return and land safely. A little later they would reach a point where they could not return from (the point of no return or PNR) and they would be committed to continuing and landing at Auckland Islands. They could see Auckland Islands before the decision point and were able to visually assess if the weather was suitable to proceed. They also had access through their base support to weather information from MetService’s AWS located on Enderby Island.
- The operator had conducted flights into the Southern Ocean before and the situation was included in the exposition under ’Offshore air operations for flights beyond the NZFIR’. That procedure listed minimum conditions for such flights before they could proceed including: aircraft type, minimum height, fuel endurance, weather minima, emergency equipment, crew briefing, flight following and HUET training.
- Another procedure in the exposition under ’Flights over water’ described the requirements for long-range offshore flights. The procedure permitted VFR flights if they were less than 100 nm from the shore, but beyond that distance they had to be IFR. By using Stewart Island, Snares Island and Auckland Islands, the flight could remain within the 100 nm distance limit all the way to Campbell Islands.
- The chief pilot and the pilot had discussed the proposed flight before the task was approved. The pilot was already authorised by the operator for long-range offshore operations. They had decided that the crew composition, pilot currency, and the risks of landing at night at Enderby Island using NVGs were adequately managed and that the task should proceed.
- Pre-flight planning was led by the pilot using the operator’s standard flight planning mnemonic (GSMEACQ) and based on the general content from the exposition. This planning procedure was inadequate for an NVG operation and for this long-distance flight over water for several reasons.
- The illumination level at the time of expected arrival was not considered and the operator did not have a means of obtaining that information. The operator’s exposition describes the extra planning and risk assessment procedures required for an NVG operation under ’Overwater Night HNVGO (HNVGO means helicopter night vision goggle operations) Operations’ where it stated, “illumination levels to be considered”. The requirement is also in AC91-13 as described in section 2 of this report under the heading Risk management for NVIS operations.
- The NVGs were reportedly checked and then packed away until they were donned prior to departure from Invercargill. The check did not discover the missing battery pack weights. On the flight down, the pilot’s NVG battery pack was too light and being pushed up by the rolled hood in their immersion suit collar. The NVIS crew member swapped their heavy battery pack with the pilot’s light pack to fix that problem. The balance weight in the pilot’s battery pack had been used by another pilot and not replaced.
- The immersion suits were reportedly checked at Te Anau before departure. According to the exposition (SLH Exposition V 17.21, Offshore air operations for flights beyond the NZFIR), the pilot should have had flares a PLB and a cut-away knife in their immersion suit, but had none of these. Another crew member had a pocketknife and torch in their immersion suit, but none of the crew had a PLB.
- The helicopter was loaded above the maximum weight limit and a flight plan load sheet was not submitted to the operator’s base.
- The flight would leave the NZFIR within 30 minutes after leaving Invercargill. The operator had their own flight monitoring system in place to arrange flight following, weather information, advice, and to initiate search and rescue if that was required.
- The CAA had placed a restriction on the operator’s AOC that did not permit CTOs outside the NZFIR at the time of this flight. The operator was unaware of this limitation and had not been consulted. The CAA had approved the operator for the last 20 years to operate beyond the NZFIR. It was later discovered to have been an administrative error by the CAA when the limitation was introduced in an updated AOC dated 28 September 2018. The CAA corrected the error on 25 February 2020 with a revised AOC. Consequently, no action was taken against the operator for conducting this flight beyond the NZFIR and outside their current AOC.
- While the operator had substantial procedure manuals for major operations, such as flying in the Antarctic or when working with the local search and rescue organisation, the guidance procedures for this high-risk type of operation was spread across several sections of the exposition. Much of the operator’s experience had yet to be documented.
- The operator had started a document called the ’Southern Ocean Safety Plan’ to describe all aspects of planning and conducting VFR flights into the Southern Ocean. It would eventually provide a comprehensive guide and set the standard required for pilots to conduct such flights, but it was in draft form at the time of this accident and had not been made available to all pilots. The operator later provided a copy of their Southern Ocean Safety Plan dated 1 December 2019.
Definition of crew member
- The definition of a crew member in the CARs is not without ambiguity (the Commission had considered the crew status in investigation AO-2018-005 (MD600N forced landing at Ngamatea Station)). The CAA issued a Legal Information Bulletin No.4 (LIB 4) to clarify to operators the CAA’s interpretation of the term ‘crew member’ for Part 135 operations. However, LIB 4 means that although an operator may consider and assign a person to be a ‘crew member’, including training them appropriately for the role, the CAA might classify them differently as a passenger, or a ‘passenger performing a task’. This scenario can arise with paramedics and winch operators.
- Furthermore, the term ‘NVIS crew member’ is defined in the AC91-13, but not the CARs, creating ambiguity as to whether such a person is a crew member or passenger. Questions can also arise as to whether an NVIS crew member's role could change from being a crew member to a passenger based on their actions during flight. For example, during the flight to Auckland Islands, whether the paramedic was a passenger until they donned the NVGs.
- The Commission considers that the differences in status of persons on board aircraft continues to be a source of confusion for pilots and operators.
Present regulatory void for NVIS and air ambulance operations
Safety issue: There are no formal risk controls in New Zealand for helicopter NVIS or air ambulance operations unlike other jurisdictions that have set minimum standards in response to the high accident rate in this sector.
- As described earlier (See ‘Aviation rules’), there is no formal regulation or performance standard for NVIS or for HAA operations in New Zealand. Presently, the CAA can impress a discretionary level of control through the CAA’s approval process for an operator when they apply to add these types of operations to their AOC. This operator had voluntarily adopted much of the content from the AC91-13 into their operating procedures.
- The most recent issue of the AC was in 2011. Activity in the HAA and NVIS aviation sectors in New Zealand has increased significantly since that time as it has overseas. Trends with overseas regulators have been to increase the requirements for crew training, CRM, operational recency, aircraft equipment, and to require pilots to be instrument rated.
- In New Zealand, the lack of formal regulation or performance standards for HAA operations remains, but has been somewhat compensated for by the activities of consumer and interested sector bodies. Ambulance New Zealand and the NZ Helicopter Association (a division of Aviation New Zealand) developed a joint standard called the ‘New Zealand Aeromedical and Air Rescue Standard’ (NZAARS) (see the full citation to access a copy of this standard (Ambulance New Zealand, 2018)). This came into use during the early 2000s with its first three-year review being completed in December 2012. All contracted helicopter operators providing helicopter services to Health New Zealand must comply with this standard and be independently audited against it (as this flight was a privately-funded medical evacuation, the NZAARS did not apply).
- The goal of the NZAARS is to ensure the quality of service provided by aeromedical services and air rescue services in New Zealand and that it promotes safety, consistency and is patient- or recipient-focused. From an aviation perspective, the standard defines the minimum crew experience for each group (helicopter aircraft groups defined in the standard are: Group 1 – IFR multi-engine turbine for aeromedical and SAR; Group 2 – VFR multi-engine turbine for same as operations as Group 1; Group 3 – VFR single engine turbine for SAR; Group 4 – VFR single engine for SAR) of aircraft operation, the aircraft type suitable for those operations, minimum equipment and crew training requirements. It also sets out criteria for human factors and CRM that must be part of the operator’s wider safety management system (SMS).
- For the NVIS requirements, the NZAARS defers to the CAA AC91-13, but also adds criteria aimed at recency and refresher training that is greater than required in the AC. Radar (radio) altimeters are required for some group operations as minimum equipment, but there are no other expectations. This standard is, in effect, like the Basic Aviation Risk Standards (BARS) requirements described later under Flight Safety Foundation and fits within the category of a mandated change driven by customers in the ‘HEMS Industry Risk Profile’ (See the full citation to access a copy of this risk profile (Flight Safety Foundation, 2009)).
United States of America
- In 2006, the NTSB published a special investigation report on emergency medical services operations (NTSB, 2006). This was after investigating 55 accidents in the HAA sector. NVIS was new to civil aviation at the time, but the report concluded that proper use of NVGs could help pilots avoid hazards at night.
- New Zealand’s CARs are structured like those of the FAA, with FAA Part 135 (USA Title 14 of the Code of Federal Regulations (14CFR), Part 135) used for CTOs. The FAA uses OpsSpecs for specific activities in CTOs so an operator may have Part 135 certification then add other activities to their operating certificate. HAA operations were covered under OpsSpec A021 and NVIS under OPsSpec A050. In 2014, the FAA revised several rules and the HAA requirements were shifted to Part 135, Subpart L. The FAA said about the new rules release that it addressed many of the concerns the NTSB had with HAA operations.
- Two aviation phrases were formalised with the new rules and in FAA documentation. The changes were to:
- Replace helicopter emergency medical service (HEMS) with the term HAA.
- Discourage the use of the term “mission” because of its implication of acceptable losses in military aviation.
- In 2017, the FAA instructed that all HAA Pilots-in-Command (PICs) must have a current instrument rating.
- In 2022, the FAA updated OpsSpec A050 for NVIS operations. One of the changes was a significant increase in the NVG recency requirement for pilots before they could fulfill the role of PIC. The requirement for three take-offs and landings in the last 90 days was increased and the period reduced. The take-offs and landings were extended to a full departure, cruise and approach to land. Area departure and arrivals were included and transitions to and from aided flight (using NVGs). They also needed to have completed six NVG operations in the period to remain current.
Australia
- The Civil Aviation Safety Authority (CASA) had issued a similar advisory document in 2007 as the New Zealand CAA AC91-13 with the CASA Civil Aviation Advisory Publication CAAP 174-01. However, in Australia it was enforced with Civil Aviation Order CAO 82.6. The process for operators was to use the CAAP 174-01 as a guide to make the necessary changes to their operation procedures to meet the requirements of the CAO and then to apply to CASA for approval to use NVGs.
- In 2021, the rules in Australia were changed and now all the requirements for the use of NVGs are included within the new rules structure CASA Parts 61, 133 and 138. A new multi-part manual of standards is out for consultation and the multi-part Advisory Circular AC91-13, AC133-09, AC138-06 was issued in 2022 (CASA, 2022). The CAO 82.6 and CAAP 174-01 were repealed.
- Pilots are required to have a night VFR rating and then may gain an NVIS rating for their licence in accordance with Part 61, Subpart P. To maintain that rating a pilot must complete an annual proficiency check.
European Union and United Kingdom
- The European Union (EU) Commission Regulation 216/2008 was issued in 2008 to provide the common rules for air operations in each member country. This was revised in 2012 with Regulation 965/2012 (European Union, 2012) that contained Specific Approvals (SPA). The SPAs related to additions to a basic AOC.
- Subpart J of the 2012 regulation was the SPA for helicopter emergency medical services called SPA.HEMS.100. Subpart H was the SPA for helicopter NVIS operations called SPA.NVIS.100.
- A helicopter intended for use at night with NVGs must have a specific airworthiness approval for NVIS in accordance with Regulation 1702/2003.
- In 2014, the UK CAA issued a Safety Directive (UK CAA, 2014) that added specific requirements to both the EU Commission Regulations for emergency medical services and NVIS operations conducted within UK. This Safety Directive increased the minimum requirements for pilots, to only allow single-pilot HEMS to proceed if the pilot held a valid instrument rating.
Flight Safety Foundation
- The Flight Safety Foundation publishes a set of BARS that they provide for guidance to aviation sector operators. In a standard intended for organisations that contract aviation services from air operators is a set of minimum standards for NVIS operations called ‘Contracted Aircraft Operations’.
- Appendix 5 of that BARS covers NVG operations. It describes the known risks in a Bowtie risk model format, with each of the threats and appropriate controls given. The listed threats are: NVG failure, Flight considerations (pre-planning), Helicopter compatibility, Flight crew experience, Flight crew recency and General NVG considerations.
- The BARS has a higher requirement than New Zealand AC91-13 for: the radio altimeter, the minimum crew experience and CRM, and the flight crew recency of experience.
- In 2009, the Flight Safety Foundation published an industry risk profile for helicopter emergency medical services (Flight Safety Foundation, 2009). The profile focuses on the voluntary change that the industry sector can control to manage risk, but recognises that input from other participants in the system may also be required to minimise that risk. Those other participants are government legislators, regulatory bodies and customers. The profile lists 26 high-level risks that have been determined from HAA industry data and analysis and outlines the appropriate risk treatment strategies to reduce the risk level.
Radio altimeter requirements
-
The New Zealand requirement for radio altimeters is in AC91-13. The AC requires that a radio altimeter is fitted, but the specifications are very general and say that:
It is recommended that the radar altimeter be equipped with an audio and/or visual warning device that can be triggered at a pilot selectable height.
-
The BARS ’Implementation Guidelines’ have a section on helicopter offshore operation. It relates mostly to oil rig support helicopter operations with two-pilot crew who are both instrument rated, but it does indicate the ideal situation about preventing controlled flight into terrain (or water) (CFIT) through the appropriate use of radio altimeters. The standard states at section 21.6:
The aircraft operator must document in the Operations Manual or MEL a requirement for at least one radio altimeter with dual displays, both of which must be serviceable at the time of dispatch for any offshore flight at night or flight conducted under IFR. Aircraft operator procedures should address the requirement for setting any aural alerting systems on the radar altimeter and the procedures to be followed in the event of an unexpected alert (Flight Safety Foundation, 2014).
- A later BARS document in 2021 for offshore helicopter operations safety performance requirements describes one of the accident prevention goals for preventing CFIT accidents as a radio altimeter with dual displays. The difference from their 2014 standard is that each display should provide an analogue indication with a visual alert and automated voice alerting device capability. It emphasises that the operator must have procedures for any user adjustable voice alert features and for actions to be taken by the flight crew in the event of an alert (Flight Safety Foundation, 2021).
- By having a radio altimeter fitted with a visual alert capability, the helicopter complied with the recommendation contained within AC91-13. However, the fact that the AC only required either an aural alert or a visual alert makes it differ from some overseas jurisdictions which require both forms of alert, including that the visual indication (light) is displayed at both crew stations, not just for the PIC (EASA AMC1 SPA.NVIS.110(b) Equipment requirements for NVIS operations, CASA Manual of Standards Part 133 11.64 Minimum equipment for NVIS flight). Some also require separate altitude displays at those crew stations.
- From an information-processing perspective, visual cues rely on the visual processing channel, and to work they must, in the first instance, be seen. Because FOV is significantly restricted when using NVGs, cues that may be readily seen with normal peripheral vision require the pilot to be looking at, or very near to, a particular instrument to receive that information. The auditory processing channel, however, does not have this limitation since sound is omnidirectional and therefore the auditory sense can receive input from any direction.
- Despite physiological and ergonomic limitations, the pilot’s FOR will, at any time, be dependent on their scan technique. This in turn, will be determined by the phase of flight and associated workload of the pilot at the time. During busy periods, where attention is required to be distributed across multiple (and potentially complex) tasks, pilot scan rates can slow or even become fixated on a particular instrument to the detriment of other flight parameters.
- The increased demands NVGs place on a pilot's visual system can be assisted by the utilisation of other sensory modes (Wickens, 2022) (Redundantly coding a target across modalities (such as coupling an aural alert with a visual warning) improves the accuracy of information processing. Auditory stimuli are particularly effective in alerting attention as they not only target the auditory processing channel, but they also cue an individual’s visual attention. Further, the short-term auditory store (echoic memory) is longer than that for vision meaning individuals can not only register the alert, but return to examine/process it after approximately three to six seconds). In the final stages of the approach toward Enderby Island, the pilot was mostly focused on the outside environment to navigate visually around the cloud cover and maintain their bearing regarding a suitable landing spot. During the post-accident interview, the pilot mentioned that it had been helpful having the crew member call out the altitude readings (at the time, the pilot did not know whether the readings were from the barometric altimeter or the radio altimeter), as their attention was primarily outside of the cockpit at that time.
- Whether this accident would have been prevented had the radio altimeter been fitted with an aural alert is unknown. It is possible that the pilot may have been more conscious of the helicopter’s position above the sea surface as the aural alert generally encourages more active engagement with the instrument itself as opposed to passive monitoring (the aural alert can be cancelled while the light would remain on until being reset for a different height). Potentially, it could also have made the fact that the NVIS crew member was calling incorrect altitudes more readily apparent as there would have been a discrepancy between their call-outs and the aural alert sounding.
- While it cannot be determined to what degree the lack of an aural alerting function contributed to this accident, not requiring what is a well-recognised safety measure for NVIS operations puts the CAA’s risk controls out of step with other overseas regulators and NVG operational best practice.
Summary
- The introduction of NVIS operations for the commercial helicopter sector within New Zealand was intended to improve safety. The lack of a robust regulatory framework to support this activity, however, meant that some of the risks associated with NVG use were not sufficiently managed. Technical standards and practices used in New Zealand for NVIS operations are still based on those common in the early 2000s when NVGs were first used in civil aviation. Externally from the regulator, the HAA sector has introduced a higher standard for NVIS operators through contracted HAA services with the NZAARS standard, but it only applies to selected operators.
- While the major regulators in the international community have recognised the benefit of NVIS helicopter operations for rescue and air ambulance operations, they have also addressed the significant risks by providing appropriate guidance and performance expectations. The CAA is still reliant on a non-transparent (two separate operators could have very different conditions they must meet for CAA through their respective AOC approval processes) and possibly unique individual arrangement they have with each operator through their air operator certification process. The international community has advanced considerably and the CAA’s guidance on NVIS helicopter operations is no longer fit for purpose.
CRM training for helicopter operations
Safety issue: The lack of comprehensive CRM training qualifications for non-pilots acting as crew members, combined with a lack of guidelines on crew members assisting a pilot during NVIS operations, creates an ongoing risk that helicopter NVIS crews will not have effective CRM.
CAA rules requirements for CRM
- CRM is typically defined as the effective use of all the resources available to crew members, including each other, to achieve a safe and efficient flight. While CRM falls within the broader field of human factors, it is considered a specialised subject regarding training and assessing competency standards as acknowledged in AC121-4 The Training and Assessment of Human Factors and Crew Resource Management (part 121 is applicable to Air Operations Large Aeroplanes (seating configuration of more than 30 seats or payload capacity of more than 3410 kilograms)) (CAA, 2013).
- Given most two-pilot operations occur within an airline environment, CRM training is graduated across the different licensing levels. Within the Private Pilot Licence (PPL) Human Factors theory syllabus, a student is simply required to explain how outside resources can contribute to the management of a flight. The CPL Human Factors theory syllabus builds on this, covering 25 items under the headings of Social Psychology and Flight Deck Management. The theory for ATPL Human Factors is broadly similar to that for the CPL licensing requirements.
- Within New Zealand, air operators conducting operations under CAR Part 121 Air Operations – Large Aeroplanes (CAA-1, 2020) and CAR Part 125 Air Operations – Medium Aeroplanes (CAA-2, 2020) are required to have programmes in place for CRM training and a means by which to assess CRM competency on an ongoing basis as part of recurrency/proficiency checks (Competency assessment for ‘soft’ or non-technical skills such as CRM is significantly complex. Best practice, such as that encouraged by AC121-4, requires assessment of individual behavioural markers by qualified examiners trained in specific, well-developed methodologies, including inter-rater reliability). There are no such requirements for operations under CAR Part 135 Air Operations – Helicopters and Small Aeroplanes (CAA, 2019).
The benefit from CRM in small size aircraft
- The reason NVIS helicopter operations allow for the utilisation of a non-pilot crew member is to provide additional safety. For this to be achieved, however, both pilot and crew member must be highly proficient in all aspects of CRM. The NVIS crew member on the accident flight used an incorrect term for “rate of descent” by calling “speed”. A central tenet of CRM is the ability to draw the pilot’s attention to flight path deviations. If a crew member uses the incorrect terminology, the pilot might focus their attention on the incorrect parameter, potentially to the detriment of a more critical one – in this case the vertical speed of the helicopter.
- Effective CRM results in all crew members sharing a common mental model of their situation, which is essential for the pilot to be able to make the best decision(s) with the information provided. To assist in forming a shared mental model of the environment, it is imperative all crew members understand from which source flight data is being provided. When the NVIS crew member was calling out altitudes during the final stages of descent, the pilot assumed that it was from the radio altimeter. The NVIS crew member would need to have leaned over to read the radio altimeter accurately. If the information provided was incongruent with the pilot’s own mental model, it would be potentially more dangerous than receiving no information at all from that crew member.
- The ability for flight crew to communicate effectively is critical to flight safety. Numerous accidents due to poor communication and misunderstandings on the flight deck is the fundamental reason the concept of CRM was developed within the airline industry. While CRM programmes – and the associated check-and-training components associated with them – are considerably advanced, the requirements to implement these within New Zealand are dependent on the particular Part 119 certificate an operator holds. In the case of a helicopter CTO, there was no CAA rule requiring comprehensive CRM training as required by other multi-crew operations under Parts 121 and 125.
What is the role of a non-pilot crew member during NVIS operations?
- When interviewed about their duties following the accident, the NVIS crew member stated that in addition to their obstacle clearance responsibilities, they liked to call out altitude information to pilots, but if a particular pilot didn’t necessarily want that information, then they did not have to listen. The chief pilot said they were not clear on exactly what CRM training a non-pilot crew member would have received, but that those who were more familiar with cockpit instrumentation could prove quite helpful to the pilot during flight.
- According to AC91-13, the purpose of an NVIS crew member is to perform “essential inflight duties to ensure safe operation of the aircraft during NVG operations” and that they should “use CRM principles to maintain crew situational awareness”. The AC does not define what constitutes an essential inflight duty and therefore it is unclear which CRM principles might be applied on board. Potentially, this could include reading cockpit instrumentation and providing that information to the pilot for situational awareness purposes.
- While the AC is silent on this role definition, Appendix 1 of the AC points to an operator’s exposition to list the responsibilities and authorities of an NVIS crew member. In doing so, this allows individual operators to define how, and to what extent, a non-pilot can interact with the pilot and participate during safety critical phases of flight. In this case the operator’s exposition allowed a crew member to “offer timely suggestions and opinions”, “critique faulty decisions” and “advocate for a different position, if necessary, to ensure the safety of the flight”. Whether this could include interpretation of flight data from the instrument panel and verbalisation of those interpretations to the pilot appears ambiguous. However, evidence would suggest that there was certainly variation amongst different NVIS crew members and pilots within the organisation and that expectations were not clearly defined either in the exposition or during pre-flight briefings.
- Crew members were required to communicate “effectively’’ using “standard” or “generally accepted” aviation terminology, yet the exposition contained only examples of such terminology specific to defined manoeuvres. If this was intended to mean that non-pilot crew members were not to offer advice outside of this particular list, this was not clearly specified. Despite this, had the pilot felt that the crew member’s called heights were causing an unnecessary distraction or risk, the correct course of action would have been to request that the NVIS crew member to stop. That did not occur.
Who can teach and assess CRM for NVIS operations?
- The CAA provides no guidance on how to teach CRM principles for use with NVIS crew, or how practical competency ought to be assessed and graded. For licensing, an NVIS flight instructor is only required to hold a CPL, and as such may have covered only the rudimentary elements of CRM as part of their CPL human factors theory course. To then be in a position to not only teach, but also assess, CRM competency and standards in a multi-crew environment (including for personnel who are not pilots themselves) poses a significant risk to flight safety.
NVIS requirements for jurisdictions outside of New Zealand
- New Zealand Civil Aviation requirements to become an NVIS crew member are considerably less rigorous that those required by some other jurisdictions, such as the European Union Aviation Safety Agency (EASA) and CASA (see Table 1 below). AC91-13 permits any personnel who are a necessary part of a commercial helicopter operation (e.g. winch crew, paramedics) to qualify as an NVIS crew member if they are using NVGs to support a single-pilot operation. Aside from the NVIS endorsement itself, there are no additional requirements to be able to act in this capacity apart from what an operator may themselves choose to put in their exposition. Essentially, this means that a non-pilot is permitted to occupy a control seat of a helicopter and give flight guidance commands to the PIC without the additional training.
- Table 1 compares the regulatory pre-requisites for NVIS flight crew member training in three different jurisdictions.
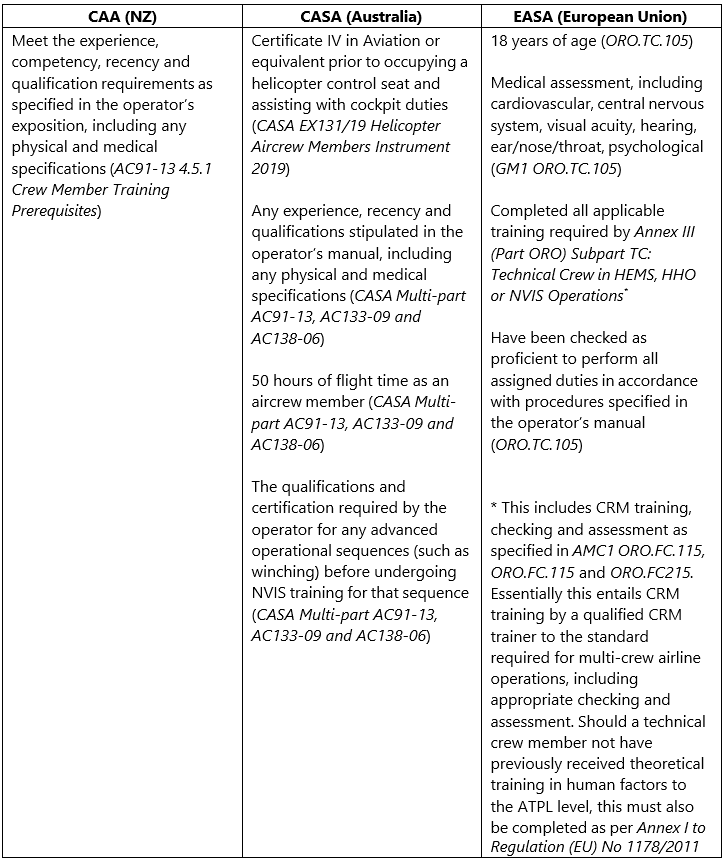
-
As well as requiring more extensive qualifications, the duties that non-pilot crew members can partake in during NVIS operations are well defined in CASA and EASA legislation. In addition to obstacle clearance duties, Australia, for example, allows an aircrew member to assist with navigation, radio communication, tuning navigational aids, helping with checklist use, and assisting the pilot monitor their systems and instrumentation. To do the latter, dedicated training is required to:
…adequately recognize, identify, announce, and provide verbal correction (the con) to the pilot for drift, rates of climb or descent, obstacle avoidance, and ground hazards for example dust and debris (CASA, 2022).
- EASA regulations (AMC1 SPA.HEMS.130(e) Crew requirements) also list the specific duties a HEMS technical crew member can fulfil. Like CASA, in addition to the primary task of collision and obstacle avoidance, EASA certified crew members can also partake in the following duties: navigation, radio communication and radio navigation aid selection, reading of checklists and monitoring of flight parameters. To assist the pilot with flight monitoring, EASA regulations (GM2 SPA.NVIS.130(f) Crew requirements) require a crew member to be trained in instrument flight techniques, specifically: instrument scanning, role of instrumentation in NVIS flight, and unusual attitude recovery procedures. In addition, one hour of blind cockpit drills must be performed.
Summary
- Having a non-pilot crew member wearing NVG and assisting the pilot was intended to be an additional safety feature that reduced the risk associated with single-pilot NVIS operations. For this to be effective, thorough training and a clear expectation around the extent of a non-pilot NVIS crew member's duties is required, but this guidance does not exist in New Zealand.
- At the time of this accident, there were no prerequisites to become an NVIS crew member, the definition of what that role entailed was ambiguous, and the rules did not require CRM training to any defined level of competence.
- In this case, the accident crew were generally able to work together using the broad principles of CRM. However, they did not have the depth of training, or share a common understanding and use of aviation phraseology, to support the CRM techniques required to manage high-risk situations more effectively.
Helicopter loading
Safety Issue: The helicopter was loaded above its maximum certified weight limit for the rescue flight and would have further exceeded it on the return flight.
- This accident is another example of where a helicopter was overloaded, but where that action was considered unlikely to have influenced the accident. The Commission has found in previous accident investigations (for example, two recent accidents reported in TAIC reports are: AO-2014-005, Collision with terrain, Mt Alta, and AO-2015-007, Collision with terrain, Fox Glacier, (TAIC, 2014) and (TAIC, 2015), respectively) that helicopters were loaded above the maximum certified weight limits for the accident flight. The Commission has also found that although an operator’s procedures may clearly describe what is required, and an operator has provided the tools to ensure that a helicopter’s maximum all up weight is not exceeded, pilots routinely violate their procedures.
- The operator had procedures and quick loading guides to reduce the workload for pilots. The guide in Appendix 1 was the applicable quick guide for this flight. It was arranged with the percentage of maximum fuel loads and the associated maximum cargo loads. The base weight included an allowance for the role equipment. Ultimately, the pilot held responsibility to ensure that the helicopter was not loaded above the maximum limits specified in the type certificate.
- Misuse of standard loading guides, or omissions of certain items or underestimated weights in a loading calculation, may result in an apparently acceptable load. It could mean the difference between a departure now or a delay to weigh items or leave some items behind. If the load is above limits slightly, fuel burn will eventually bring it back into normal loading limits. The final test for pilots is often made with a dynamic check. This is where the pilot slowly lifts off into a low hover, while checking that the load is not limiting control movement to hold the helicopter level and there is still a margin of power available.
- The type certificate limits are defined for many reasons and are not necessarily the same as the maximum load that can be lifted in the environmental conditions at the time. Exceeding the aircraft weight limitations introduces fatigue that may then shorten the operational life of some components. Some helicopter type certificates allow a higher loading if part of the load is external and can be jettisoned (not applicable to the BK117). Some helicopters also have sufficient power at sea level to lift more than the maximum rated internal load. Therefore, a dynamic check will establish that the helicopter can be flown, but not if it is overloaded.
- The pilot said that their iBal Rotary calculation of weight and balance for the accident flight was on their phone lost and at sea. They recreated one from memory. The recreated loading calculation showed that the helicopter was within weight and balance limits, but it did not match the actual weights. Table 2 below shows the main differences between the pilot’s recreated estimate and the calculated loading shown in Appendix 2.
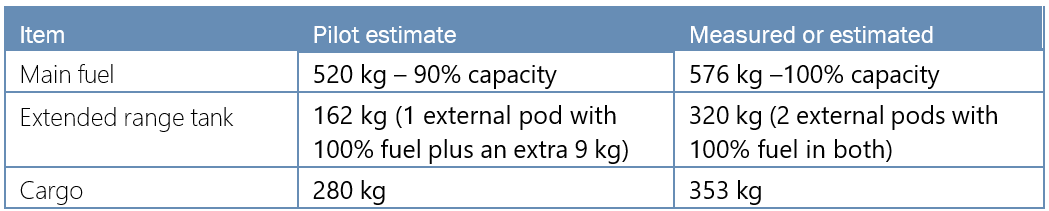
- The medivac configuration loading guide (Appendix 1) showed the maximum load that could be carried over the standard role equipment fitted for that configuration and remain within the helicopter’s loading limits. The guide included an allowance of 100 kilograms for the pilot. With 100 per cent fuel and two external long-range fuel pods, also with 100 per cent fuel, this additional discretionary load was 166 kilograms of cargo.
- The recovered items were weighed and the weight of other items not available were estimated from discussions with the operator. The calculated helicopter loading is given in Appendix 2 and shows that it was approximately 295 kilograms over the maximum allowable weight of 3350 kilograms when the helicopter departed Invercargill. It would take approximately one hour of flight time to burn that excess weight in fuel.
- The overload was slightly less at initial take-off from Te Anau because the winch operator was not on board. After the 27-minute flight to Athol, the fuel burn would have compensated for the winch operator boarding so the helicopter would again be similar to the take-off weight at Te Anau.
- Assuming that all fuel tanks would have been refilled to 100 per cent for the return flight from Auckland Islands, the weight of the medivac patient would have been additional to that calculated loading.
- The task was at the limits of the helicopter’s capability and endurance. With the amount of fuel required for the long-distance flight to Auckland Islands, and the crew and equipment carried on board, the flight was only possible by exceeding the maximum certified all-up weight.
- The airworthiness and life-cycle of an aircraft structure and its components are evaluated by aircraft manufacturers based on operations within the prescribed limitations found documented in the Aircraft Flight Manual. Exceeding aircraft weight limitations increases the risk of fatigue failures occurring at a lower life limit or inspection interval than that published by the manufacturer.
Life-raft and survival equipment
Safety issue: For a life-raft to be an effective device for increasing the chance of survival in the event of a ditching, it must also be easily extracted from the aircraft so it may be deployed when needed in an emergency.
- The life-raft was an aviation-style life-raft. Certification under FAA TSO-C70a meant that it had a survival kit inside with food and other emergency items. As a ‘Type II’ life-raft it was intended for CTOs, but not for transport category aircraft (passengers), and it was therefore correctly matched to this type of operation.
- The TSO-C70 includes requirements for the life-raft and container, its colour and marking. The operating instructions must be printed on the outside of the container and visible when stowed. The retaining line is usually attached to the aircraft to prevent the life-raft from floating away. The life-raft pack is then thrown away from the aircraft. A survivor must reach the floating life-raft pack, lift the cover flap to expose a red handle attached to a lanyard, and pull the red handle until the life-raft inflates.
- CAR rule 91.525 sets out the requirements for New Zealand air operations over water. It states that life preservers, life-rafts, signalling devices, ELT(S) and Emergency Position-Indicating Radio (EPIRB) must be installed in conspicuously identified locations and must be easily accessible in the event of an aircraft ditching. Life preservers, including constant wear anti-exposure overalls (immersion suits), must meet the requirements set out in Appendix A.14 of CAR Part 91.
- In this accident, impact with the water was at night, unexpected and sudden. The helicopter lay semi-submerged in an inverted attitude for a short period and then sank. The life-raft was loaded into the rear cargo area amongst the rest of the provisions for that rescue flight. After rescuing the winch operator, the paramedic tried to extract the life-raft from the cargo area, but could not find it before the helicopter sank. The crew were wearing full immersion suits and life-jackets.
- The crew had emergency location and communications devices in a grab-bag in the cargo area, but not on their person. This grab-bag was also lost with the helicopter.
- This raises several safety factors with over-water operations that operators need to address. They must ensure that emergency equipment is available for the crew to use in an emergency and that all survival equipment can be used effectively. The safety factors include:
- The type of life-raft that would be most suitable for an operation
- Where that life-raft (or rafts) will be stowed and how it will be attached to the aircraft
- If any additional visual aids are required to make a stowed life-raft visible in an emergency, such as a water-activated light or highly reflective tape, or an activated glowstick
- What training crew will require and what refresher interval is needed to ensure all crew are familiar with where to find a stowed life-raft and how to deploy it
- What personal survival equipment will be required and where it should be stowed.
Appendix 1. Standard medivac loading
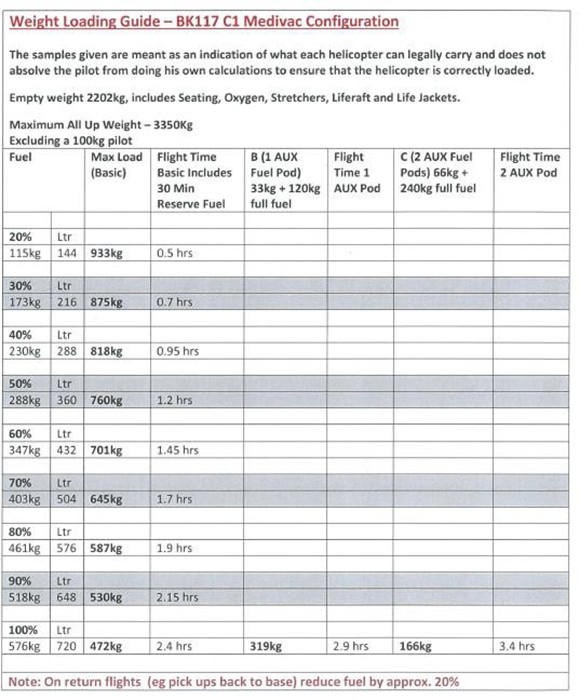
Appendix 2. Calculated loading
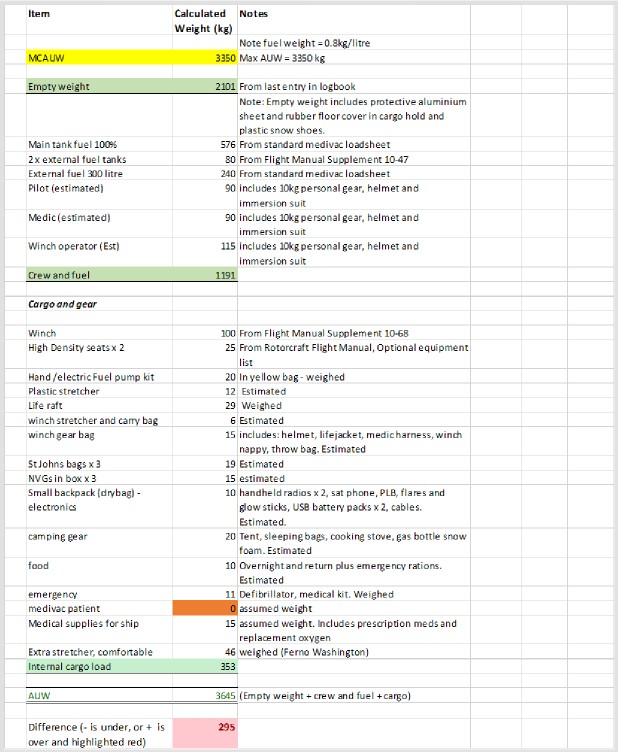
Appendix 3. Weather analysis from noon 22 April 2019 (NZST)
Appendix 4. Estimated Illumination (UK Met Office)
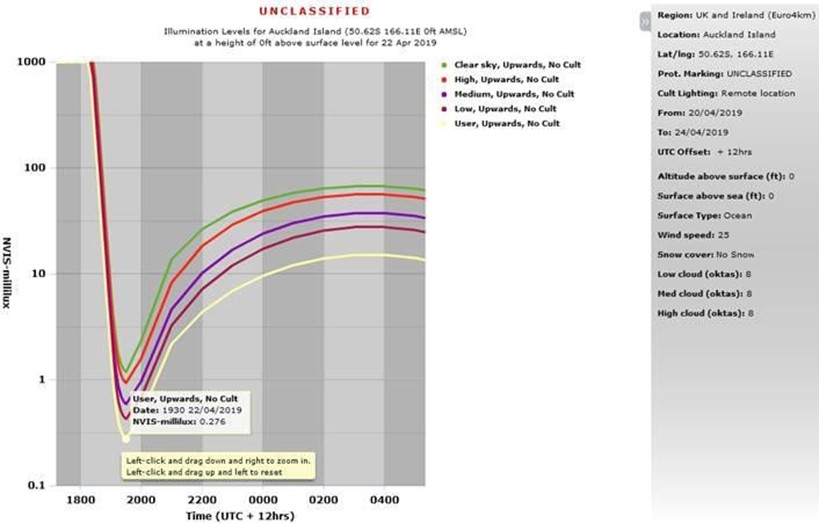
Appendix 5. Descent rate into Auckland Islands