Aerial firefighting operators need to respond to the latest advice about monsoon bucket structure and sling line length. Firefighting helicopter significantly damaged in heavy forced landing when tail rotor was disabled by lifting line of underslung collapsible monsoon bucket. Bucket aerodynamics changed when a steel ring holding top mouth open came loose. Hook-and-loop fasteners had come undone.
Executive summary Tuhinga whakarāpopoto


What happened
- On 17 February 2019, an Airbus Helicopters AS350 helicopter, registered ZK-HEX was one of several helicopters assisting with the suppression of forest fires. The fires had been burning throughout the Nelson region over the preceding two weeks.
- The pilot was the sole occupant while the helicopter was operating with an externally suspended monsoon bucket. After dropping a load of water on the target area, the helicopter was returning to a nearby pond to refill the monsoon bucket. The lifting line suspending the monsoon bucket made contact with and disabled the helicopter’s tail rotor, resulting in a loss of directional control. The pilot initiated a descent for a forced landing. The helicopter descended into a forested area and landed heavily, resulting in significant damage. The pilot received minor injuries.
Why it happened
- A tubular, segmented, stainless-steel ring was held in place at the top of the bucket with hook-and-loop fastener tabs. This ring was intended to maintain the circular shape of the top section of the bucket when it was being filled.
- It was likely that during the accident flight, one or more of the hook-and-loop fastener tabs came undone, allowing the ring to become insecure and the bucket to lose rigidity. This likely resulted in a sudden change to the aerodynamic stability of the bucket in the airflow, leading to the bucket trailing behind the helicopter and the lifting line contacting the tail rotor. The reason for the hook-and-loop fastener tabs coming undone could not be determined.
- The bucket manufacturer had developed design improvements to reduce the likelihood of the hook-and-loop fastener tabs coming undone, but the modification was not mandatory. Therefore, the Transport Accident Investigation Commission (Commission) has made a recommendation that the Cloudburst monsoon bucket manufacturer ensure that all Cloudburst monsoon buckets with this hook-and-loop fastener system are modified with the design improvements.
- The monsoon bucket lifting line was of a length that likely increased the risk of the external load coming into contact with the tail rotor. The Commission found that at the time of the accident, there was insufficient guidance available to pilots on the appropriate line length for monsoon bucket operations. The aircraft manufacturer has since published a Safety Information Notice on this issue and the operator has incorporated this guidance into its operating procedures.
What we can learn
- The bucket manufacturer had developed operational information on and limitations for the use of its monsoon buckets, but did not proactively promulgate this information to operators. This omission had the potential for operators to develop policies in isolation, possibly resulting in less-than-optimal safe working practices. As such, the Commission has made a recommendation that the bucket manufacturer review and enhance the Operation Manuals for all Cloudburst buckets to include any recommended operational and maintenance procedures, guidelines and limitations, and promulgate this information to all users of this equipment.
- All occurrences that have safety implications should be reported through the operators’ internal safety management system. The Civil Aviation Authority should also be notified of all occurrences that meet the Civil Aviation Rules Part 12 – Accidents, Incidents, and Statistics criteria. Not reporting a safety-related occurrence is a missed opportunity to prevent a similar occurrence.
Factual information Pārongo pono
Narrative
- On 17 February 2019, the pilot of an Airbus Helicopters AS350 helicopter, registered ZK-HEX (the helicopter), was using a monsoon bucket (the bucket) to drop water on a forest fire in the Wakefield area, near Nelson. The helicopter departed from a staging area at about 1408 (times are in New Zealand daylight time (co-ordinated universal time + 13 hours) and expressed in the 24-hour format) to commence the firefighting task. The pilot was the sole person on board.
- The pilot flew the helicopter in a pattern that involved dipping the bucket, which was suspended from the cargo hook on a lifting line, into a dipping pond then flying with the full bucket to drop the water where required. The helicopter then returned to the dipping pond to repeat the process. Each cycle of dipping, dropping and filling took about three to four minutes.
- At about 1449, the pilot dropped a load of water onto the target area approximately 1.7 nautical miles (one nautical mile equals 1.852 kilometres) from the dipping pond. The pilot then turned the helicopter back toward the dipping pond, while climbing and accelerating.
- The pilot reported that after reaching cruise airspeed, the helicopter unexpectedly yawed violently one way and then the other. The pilot then heard a loud bang and the helicopter commenced an un-commanded turn to the left.
- The pilot initiated a descent for a forced landing, jettisoned the bucket and transmitted a Mayday radio call. The pilot descended towards an area of light bush close to a forest access road, but the helicopter started to spin near the ground. The pilot recalled following the recommended procedure for a loss of tail rotor control by closing the throttle, shutting the engine down to stop the helicopter spinning, and conducting an autorotative landing.
- A number of fire service personnel were working on the ground in the nearby area. They arrived at the accident site within a few minutes and were able to assist the pilot out of the wreckage. The pilot received a minor ankle injury. The helicopter was substantially damaged.
Damage to aircraft
- The helicopter struck the ground heavily with minimal sideways movement. The impact resulted in the separation of the front section of both the left and right landing gear skid tubes, and the deformation of the front section of the cabin structure (Figure 3).
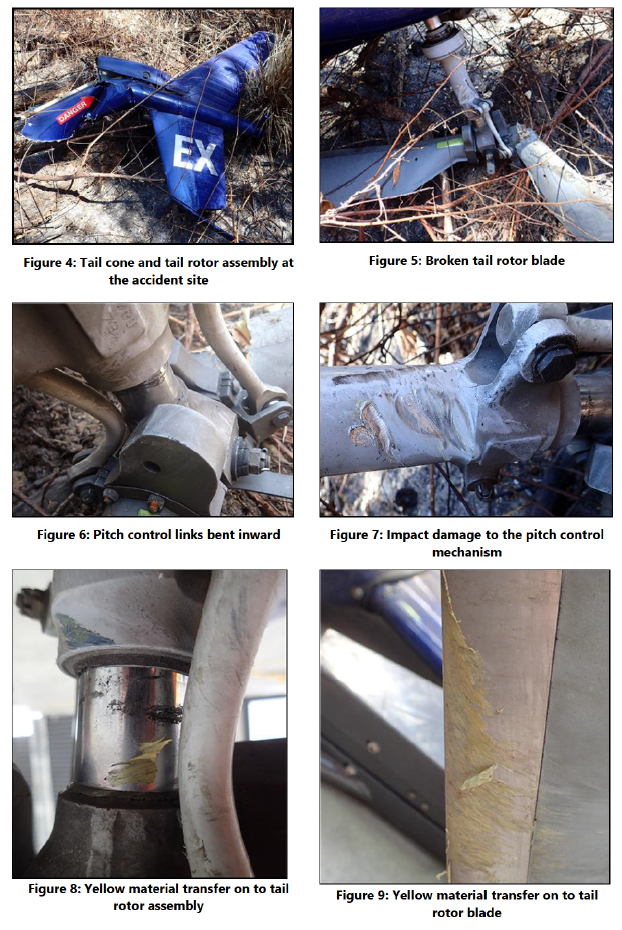
- The main rotor blades were substantially damaged and appeared to have struck the tail boom and surrounding foliage. The rear section of the tail boom and the tail rotor assembly had separated from the main airframe (Figure 4) and landed a few metres to the right of the fuselage.
- One tail rotor blade was broken at its root end but remained attached by its internal structure. The opposing tail rotor blade exhibited no external damage (see Figure 5).
- The two pitch control links on the tail rotor assembly were found deformed (Figure 6) and the tail rotor pitch-control slider had numerous indentations (Figure 7).
- Yellow synthetic material was found on the tail rotor assembly at various locations (Figure 8). The same yellow material was also found on the leading edge of the broken tail rotor blade (Figure 9).
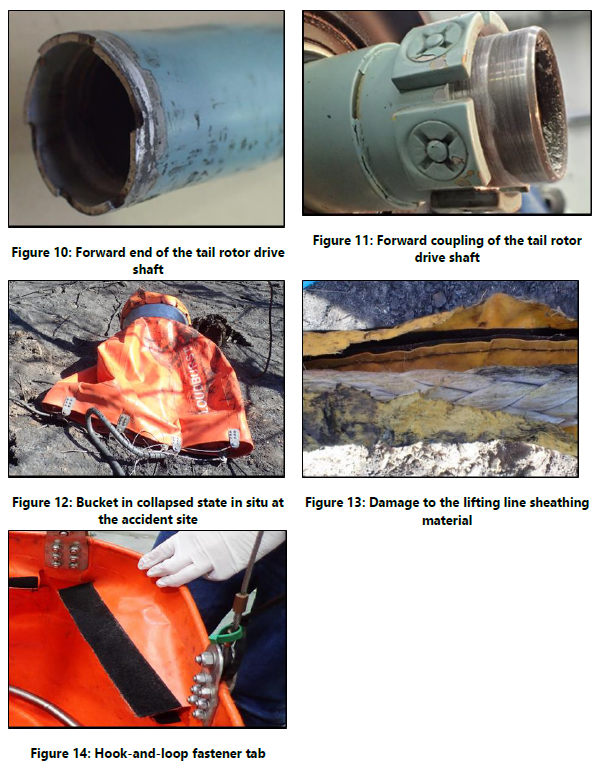
- The tail rotor drive shaft had failed at its forward coupling (Figures 10 and 11).
- The jettisoned bucket was found in a collapsed state in a forested area approximately 100 metres (m) to the south of the helicopter wreckage (Figure 12). A yellow synthetic sheathing was used to enclose the synthetic lifting line, electrical cable and pneumatic line (2.24); all of these exhibited damage at about the same point along the length of line (Figure 13).
- The bucket was inspected in situ. A tubular, segmented, stainless-steel ring normally held in place by hook-and-loop fastener tabs (commonly referred to by the brand name of Velcro®) at the top of the bucket (Figure 14) had come apart and was displaced.

Aircraft information
- The helicopter was constructed in 1982 as a ‘BA’ variant of the AS350 helicopter type. It was later converted to an ‘FX2’ variant. This conversion included, among other things, the replacement of the engine with a Honeywell LTS101 700 D-2, and an increase in the allowable maximum all-up weight limit with an external load, from 2,250 kilograms (kg) to 2,500 kg.
- The helicopter had recorded a total flight time of 5,816.43 hours at the time of the accident. The helicopter had been maintained in accordance with the operator’s approved maintenance programme. The maintenance logbooks showed that all scheduled maintenance had been carried out as required, and the helicopter had no recorded defects at the time of the accident.
- The helicopter was configured to operate with the monsoon bucket suspended from the cargo hook. The right-side pilot’s door had been removed, with the right sliding door locked back in the open position. The left-side sliding door and front doors were both in their closed positions. This configuration was permitted within the helicopter’s flight manual but it reduced the maximum allowable airspeed to 110 knots (the global positioning system and satellite tracking recorded ground speeds of no more than about 80 knots. A knot is a measurement of speed in nautical miles per hour, equivalent to 1.852 kilometres per hour).
Weight and balance
- The helicopter had been fuelled to about 55% of capacity (297 litres) at the start of the fuel cycle. Since then, the helicopter had been flying for about 40 minutes. The pilot estimated that the helicopter had about 40% (216 litres) of fuel remaining at the time of the accident. This equated to about 173 kg.
- The cargo hook beneath the helicopter was equipped with a load cell. This displayed the weight on the hook to the pilot in the cockpit. The pilot stated that the load cell weight was used to determine how much water was in the monsoon bucket during filling and that it was usually filled to about 800 kg.
-
The helicopter’s empty weight was 1,309.95 kg. The maximum allowable all-up weight of the helicopter with an external load was 2,500 kg. The all-up weight of the helicopter was estimated to have remained below this limit throughout the duration of the flight.
- The cargo hook was positioned directly below the main rotor mast. The helicopter’s centre-of-gravity position was within the allowable limits stated in the flight manual with the monsoon bucket both full and empty.
Monsoon bucket and associated lifting line
- The monsoon bucket was an earlier version of the Cloudburst CB1000MF, manufactured in New Zealand by IMS New Zealand Limited (IMS). It had a maximum capacity of 1,000 litres. The bucket was constructed using a flexible urethane fabric.
- The bucket assembly was purchased new by the operator in January 2013 and had been used for 300 hours. It had been maintained in accordance with the operator’s Civil Aviation Authority (CAA) approved internal maintenance programme.
- The synthetic lifting line was 8.5 m in length and attached to the helicopter cargo hook at its upper end and to the bucket control head at its lower end. The synthetic lifting line and associated electrical and pneumatic control lines were wrapped in a yellow, abrasion-resistant synthetic sheathing with a hook-and-loop closure.
- The bucket was suspended below the bucket control head by eight, 3 m-long steel cables (Figure 15). The symmetrical profile of the bucket was maintained by the pressure of the water acting on the inside surface of the bucket (Figure 16) when carrying water and by the tubular, segmented, stainless-steel ring in the upper section of the bucket when empty.
- To fill the bucket with water, the pilot lowered it into a dipping pond. To help the effective filling of the bucket, lead weights were installed on one side, speeding up the submersion and filling process.
- When assembling the bucket for deployment, the eight hook-and-loop fastener tabs (Figure 14) could be opened to accept the tubular, segmented, stainless-steel ring in the upper section of the bucket, then closed to secure it. This allowed disassembly for transport and storage (Figures 18 and 19). The ring had the effect of keeping the top section of the bucket rigid when empty. The operator had kept the bucket in a fully assembled state while in storage to enable rapid deployment.
- A small bladder was attached to the inside wall of the bucket. This bladder could be filled with an additive. Access to fill this bladder was easier with the top ring installed than without. Throughout the operation on the day of the accident, the bladder was filled during every helicopter refuelling cycle. The operator’s ground crew member who had carried out this task stated in the operator’s internal report that the bucket was in good condition during the last refuelling.


Monsoon bucket certification
- No requirement exists within the Civil Aviation Rules for manufacturers of this type of role equipment (equipment that is fitted to an aircraft to enable it to fulfil a particular mission or task) to be certificated or to produce operational information to assist with the safe operation of their products.
- The onus was on operators to identify risks associated with the use of any role equipment and mitigate those risks appropriately. The CAA’s involvement with such equipment was limited to assessing, and if satisfied approving, an operator’s exposition (documentation approved by the CAA that defined the organisation, identified the senior persons, and detailed the means of compliance with the applicable Civil Aviation Rules), in which maintenance and operating procedures for the use of such role equipment were defined.
Personnel information
- The pilot held a commercial helicopter pilot licence. All required medical and competency assessments were complete and current in accordance with Civil Aviation Rules and the operator’s exposition.
- The pilot had been flying helicopters with monsoon buckets in fire-fighting operations since the mid-1970s. The pilot had received recurrent training for the set-up and use of the monsoon bucket on 15 January 2019. At the completion of that training, the pilot had been authorised by the operations manager to conduct operational roles using the monsoon bucket.
- Drug and alcohol tests were conducted at the hospital after the accident. The results for these tests were negative (clear) for both.
Organisational information
- The operator held an operator’s certificate issued by the CAA under Civil Aviation Rules Part 135 – Air Operations Helicopters and Small Aeroplanes. The operating certificate permitted the operator to conduct commercial external load operations in accordance with its exposition.
Meteorological information
- Weather stations located at Nelson Airport and Richmond, both within eight nautical miles (15 kilometres) to the north-east of the accident site recorded a wind from the north of about 15 knots (30 kilometres per hour), with no significant cloud coverage and at least 19 kilometres of visibility about the time of the accident.
- The accident pilot, as well as another helicopter pilot working in the immediate area, estimated that the conditions at the accident site were similar to those recorded by the weather stations.
Survival aspects
- The helicopter structure was not specifically designed to be energy absorbing in the event of an accident, nor was it equipped with energy attenuating seats. However, most of the impact forces were absorbed by the forward landing gear and cabin support structure, when they deformed, as the helicopter struck the ground vertically.
- The pilot’s seat was equipped with a four-point harness. The pilot advised that the lap belt component of the harness had been secured and the shoulder strap had been positioned beneath the arms to enable sufficient movement to view the external load.
- The pilot was wearing fireproof overalls and a flight helmet as required by the operator’s internal checklist for conducting firefighting operations.
- The helicopter was equipped with an emergency locator transmitter. Impact forces during the accident automatically activated this transmitter. The MEOSAR satellite constellation15 detected and forwarded the transmission to the Rescue Coordination Centre New Zealand. The pilot turned the transmitter off after ground personnel had arrived at the accident site.
Tests and research
- The helicopter was equipped with a global positioning system (GPS) that recorded its flight path, as well as a satellite-tracking device that was configured to transmit flight data every two minutes. The data obtained from both these devices was analysed to determine the helicopter flight profile leading up to and during the accident.
-
An expert metallurgical and chemical analysis of the damage and material transfer observed on the tail rotor assembly was carried out. The report from this analysis concluded:
The samples of the yellow deposit taken from the leading edge of the fractured blade and the yellow sleeve were analysed using Fourier transform infrared (FTIR) spectroscopy. This analysis showed that the FTIR spectra of both samples was very similar, indicating that both samples were the same polyvinyl chloride (PVC) type material.
The evidence shows that the monsoon rope assembly had been caught in the tail rotor assembly when the tail rotor was rotating, and rotation of the rotor/driveshaft stopped abruptly as a result. Debris found on the tail rotor was analysed and found to be the same material as the yellow rope sleeve material. The rope would have very rapidly been tightly wound around the shaft until it bound, when the drive shaft failed. This process resulted in a hard object of some form impacting or embedding into the tail rotor shaft, bending the tail rotor blade control arms and breaking one of the tail-rotor blades.
Additional information
Fire-control activity standards in New Zealand
- In 2015, the National Rural Fire Authority issued the Standard for Use of Aircraft at Wildfires (the original standard). As the National Rural Fire Authority procured the services of aircraft operators for fire-control activities, the original standard was issued with the purpose of facilitating the effective, efficient and safe use of aircraft engaged in these operations. The requirements of the original standard were imposed by the National Rural Fire Authority (as the customer) in addition to Civil Aviation Rules.
- In 2017, New Zealand’s urban and rural fire services combined into a single, integrated fire and emergency service organisation known as Fire and Emergency New Zealand (FENZ). FENZ provided the overarching management of the firefighting resources, which were utilised on this fire, and procured the operator’s helicopter services.
- On 30 August 2017, FENZ updated and issued a new standard, which was active at the time of the accident (Fire and Emergency New Zealand, 2017).
- Since then FENZ has adopted an ‘all-of-government’ approach, which has allowed other New Zealand government agencies to utilise its new standard.
- On 1 May 2020, FENZ further updated the new standard to serve as an interagency standard for the procurement of aircraft to fight wildfires (FENZ has advised that its standard will be publicly available on its website from 1 August 2020: https://fireandemergency.nz).
- The Operational Supplement to the Inter-Agency Standard for Use of Aircraft at Wildfires includes, under Section 23.1 Pilots Using Underslung Loads, the following requirements:
- Operate the helicopter within the flight manual limitations, including limitations relating to configuration and role equipment.
- Only use buckets and related equipment in accordance with the technical requirements, operating instructions and limitations set by the equipment manufacturer and have regard to the effect of the bucket on aircraft performance.
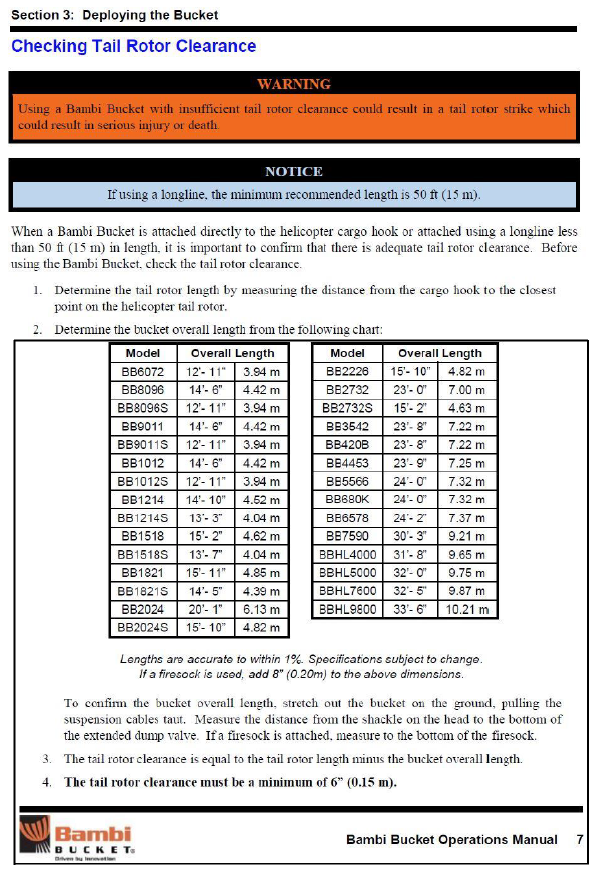
- Ensure the strop length (from the helicopter hook to the bucket attachment cables) is not less than 50ft (15.2 m) for all pilots and all helicopter types.
Operator accreditation
- FENZ stated that to obtain or maintain accreditation, an operator must meet the requirements of the current standard through a verification process and ongoing audit processes. Operators that are unable to conform are subject to a recheck procedure.
- The National Rural Fire Authority had conducted an audit of the operator on 4 May 2017 using the original standard. The operator was subsequently issued with a compliance certificate permitting it to provide helicopter support for fire-suppression operations with the National Rural Fire Authority.
Appendix 1. Bambi Bucket tail rotor clearance
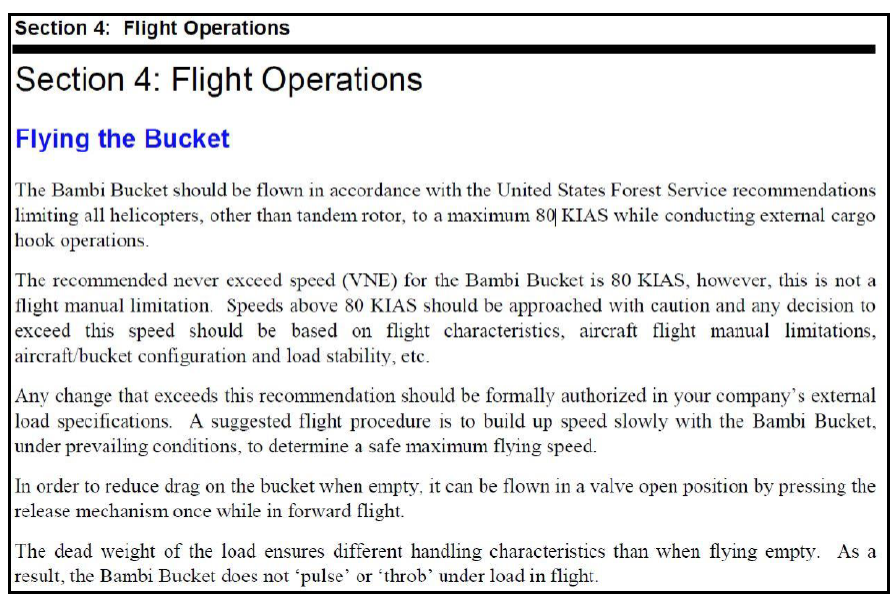
Appendix 2. Bambi Bucket flight operations
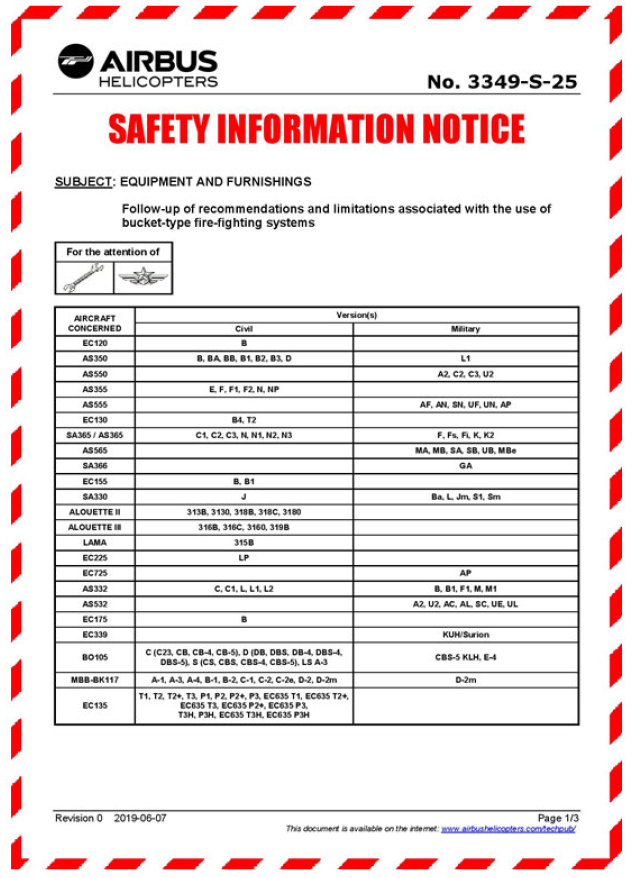
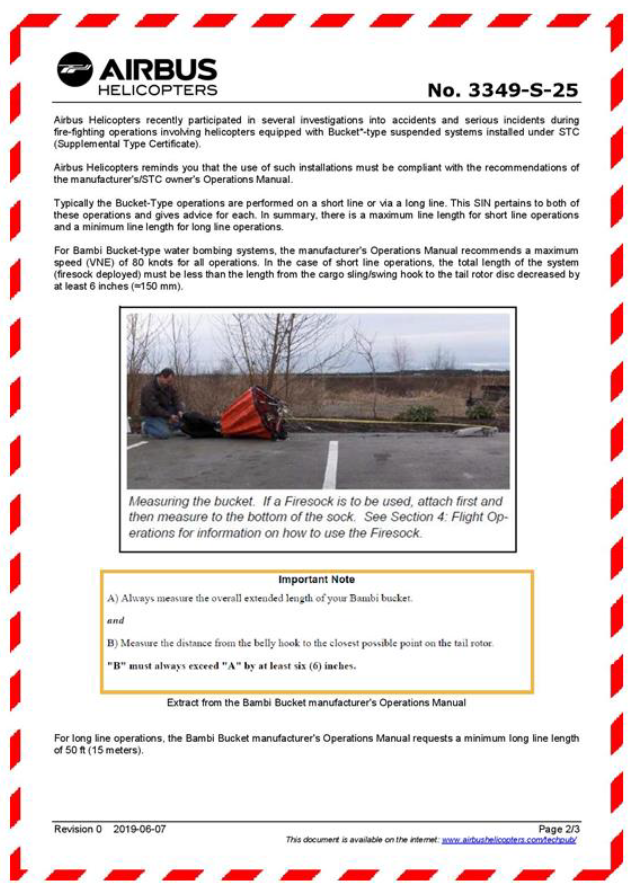
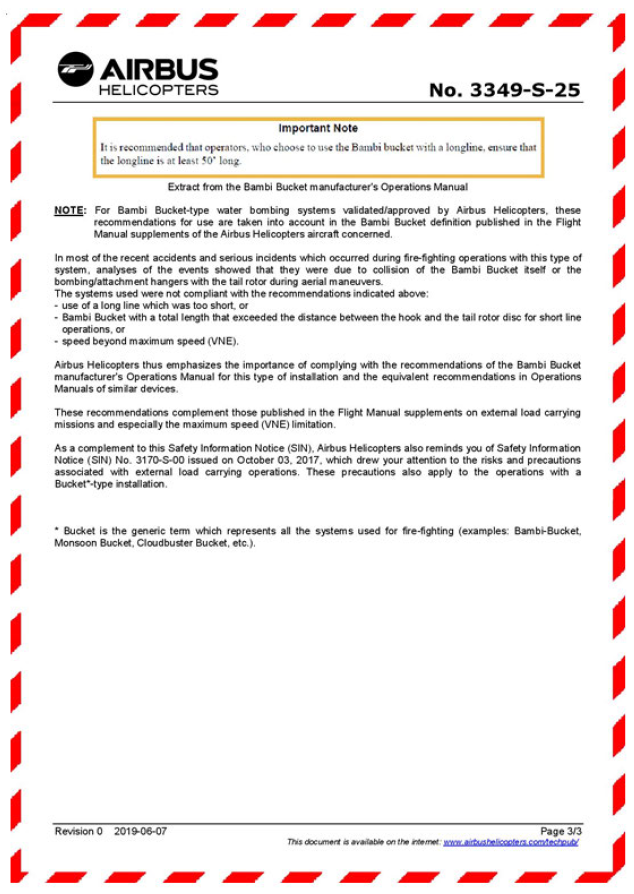
Appendix 3. Airbus Helicopters Safety Information Notice
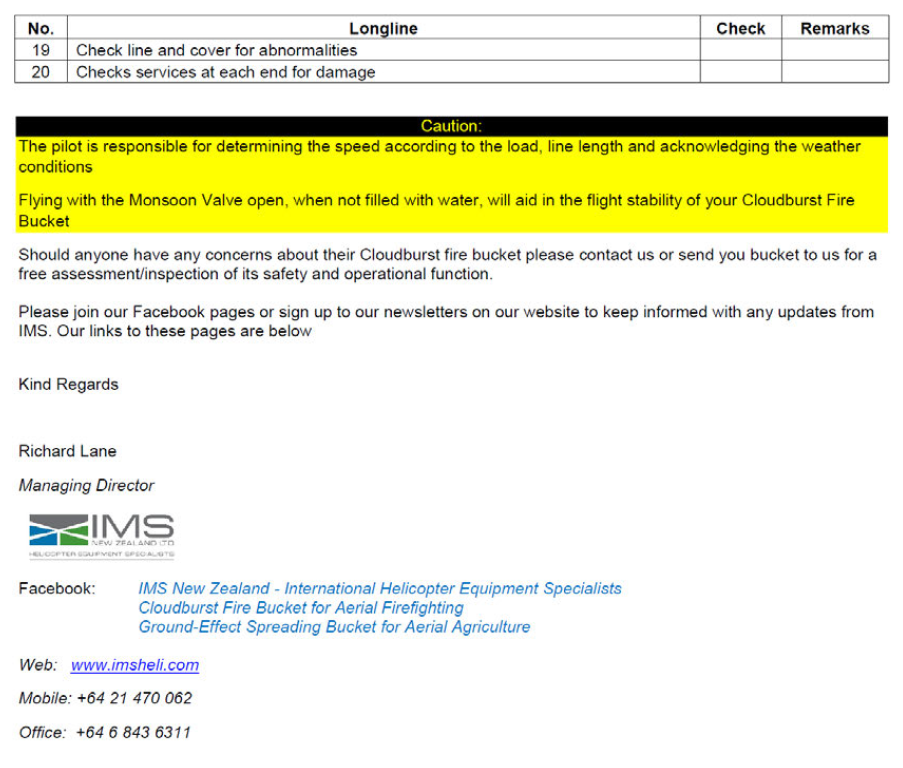
Appendix 4. IMS New Zealand Limited Safety Information Letter 6 April 2020
Appendix 5. IMS New Zealand Limited Safety Information Notice 3 July 2020