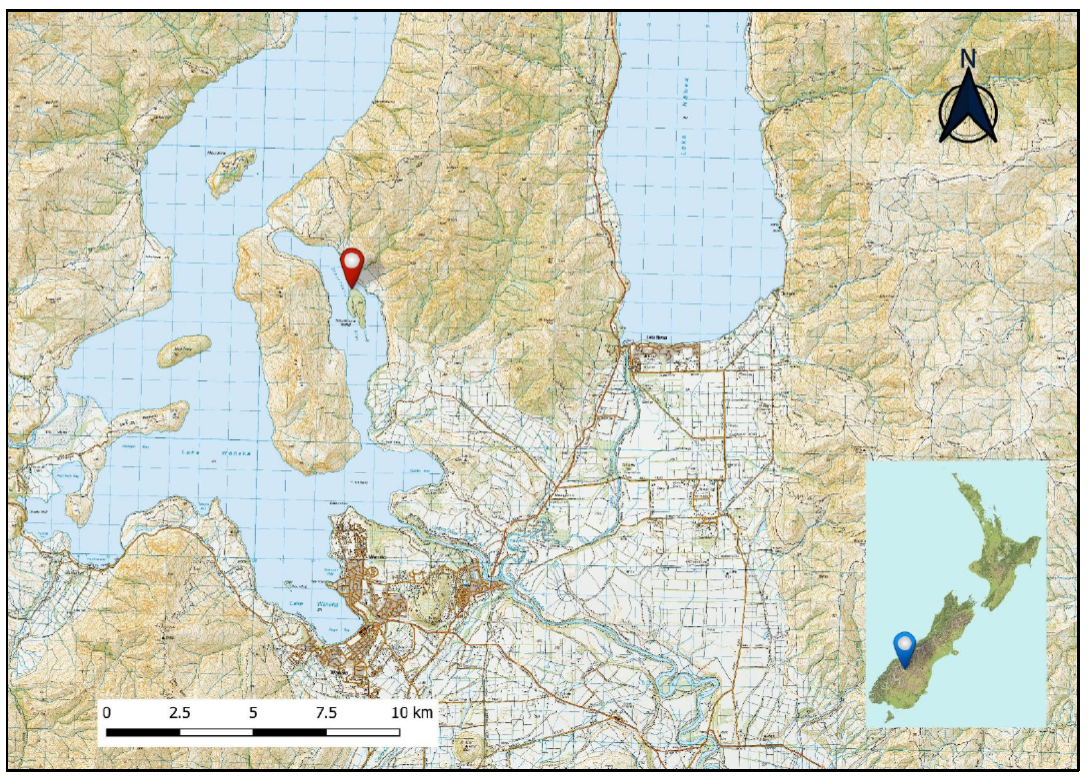
A Robinson R44 helicopter disappeared while on a short flight over Lake Wanaka. Searchers found an oil slick on the lake surface and some debris on land nearby.
Executive summary Tuhinga whakarāpopoto

What happened
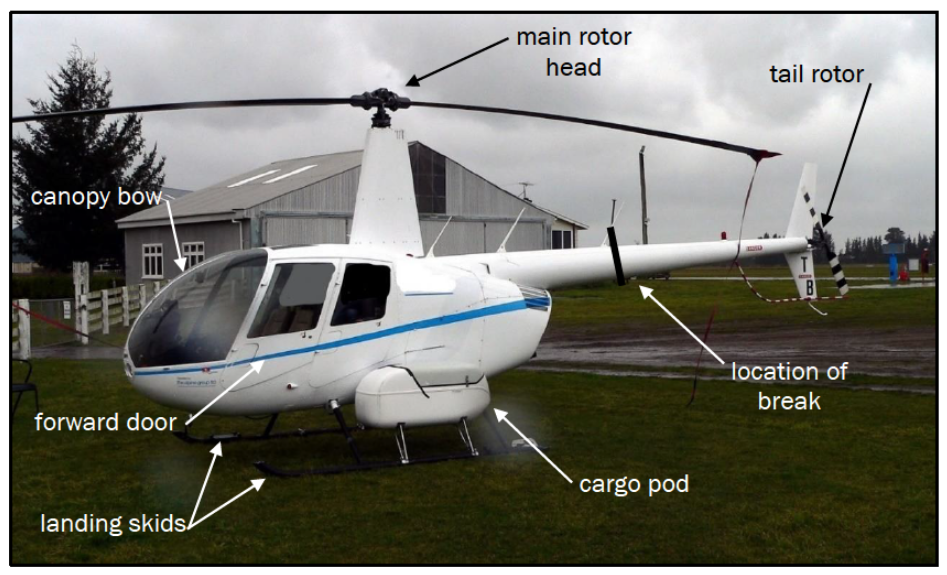
- On 21 July 2018, a Robinson Helicopter Company R44 helicopter, registered ZK-HTB, was en route from Wanaka to Upper Estuary Burn Valley when it suddenly departed controlled fight and crashed into Lake Wanaka, killing the pilot who was the sole occupant.
Why it happened
- The Transport Accident Investigation Commission (Commission) found that the helicopter was likely to have encountered unexpected turbulence of a magnitude sufficient to result ultimately in the in-flight break-up of the helicopter.
- The Commission also found that the helicopter’s speed at the last position report likely increased the risk of an adverse outcome in the mountainous operating environment.
- The Commission further found that investigations into loss-of-control or mast bumping accidents involving Robinson Helicopter Company helicopters continue to be hampered by a lack of data. Allied with this is a lack of understanding of how the main rotor performs in adverse conditions. This lack of factual information has limited the effectiveness of safety investigations.
What we can learn
- The R44 Pilot Operating Handbook used the non-standard term ‘significant’ to describe turbulence. The Commission found that the R44 Pilot Operating Handbook did not explain the meaning of this term. In June 2020, Robinson Helicopter Company amended Safety Notice 32: High Winds or Turbulence, contained within the R44 Pilot Operating Handbook, to define the term ‘significant’. The added definition aligned with commentary in a Robinson Helicopter Company safety video regarding Safety Notice 32.
- The key lesson from this inquiry is that pilots need to exercise caution when planning and conducting flights into areas of potential turbulence. Pilots should seek to avoid these situations. Should turbulence of any strength be encountered, pilots need to take immediate action to minimise its effects. Also, pilots of Robinson Helicopter Company helicopters need to be familiar with Safety Notice 32 and the associated video and avoid flying in high winds and turbulent conditions.
Who may benefit
- Pilots, operators and all potential users of Robinson Helicopter Company helicopter types may benefit from the findings and lessons learned.
Factual information Pārongo pono
Narrative
- On the afternoon of 21 July 2018, a Robinson Helicopter Company (RHC) R44 helicopter, registered ZK-HTB (the helicopter), was made available by its owner for a private flight. The pilot was to fly from Wanaka Aerodrome to a lodge in the Upper Estuary Burn Valley on the northern shore of Lake Wanaka, a flight of 15-20 minutes. The pilot was to meet two friends, who were to arrive at the lodge on another helicopter from Queenstown a short time later.
- Earlier that day a second pilot had flown the helicopter, taking three passengers and their gear to the lodge. Two cargo pods, one on each side of the helicopter, had been fitted for the morning flight. The pod on the right side was removed after the helicopter was returned to its hangar at Wanaka.
- At 1230 closed-circuit television (CCTV) cameras recorded the pilot beginning the pre-flight inspection before loading the helicopter in the hangar and taking it outside for refuelling. At 1245 the pilot started the helicopter, and while it was warming up loaded further items on board. Some of the items were seen on the CCTV footage to be placed in the back of the cabin, while others were placed in the cargo pod mounted on the left side of the helicopter.
- The pilot boarded the helicopter and at 1257:13 made a radio call on the local area frequency advising that the helicopter was lifting from the owner’s base. At 1257:38 the pilot radioed “taking off for Dublin Bay”, a prominent feature and reporting point about 10 kilometres (km) north-west of Wanaka Aerodrome.
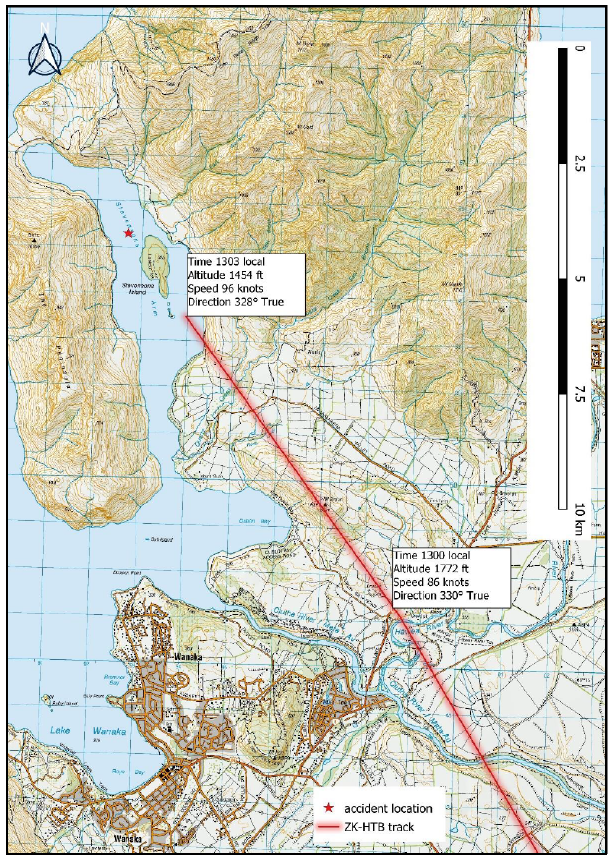
- The flight tracking system fitted to the helicopter made position reports every three minutes. The system transmitted its first in-flight report from the helicopter at 1300:25. It recorded the helicopter passing to the east of Albert Town, about halfway to Dublin Bay (see Figure 3). The helicopter was flying at an altitude (above mean sea level) of 1,772 feet (540 metres (m)), approximately 600 feet (180 m) above the ground, and at a groundspeed of 86 knots (160 km per hour (km/h)) (this is the groundspeed at the time of the report, not an average of the last two reports. A knot is a speed of one nautical mile per hour, equivalent to 1.85 kilometres per hour).
- The next and last report, made at 1303:25, recorded the helicopter 500 m south of Stevensons Island. The helicopter was flying at an altitude of 1,454 feet (443 m) or about 500 feet (152 m) above the lake, and at a groundspeed of 96 knots (178 km/h).
- At about 1308, a person responsible for maintaining ‘flight following’ for the aircraft noted that nearly five minutes had elapsed since the last position report from the helicopter. The duty person refreshed the display and, with no update seen, initiated the ‘aircraft overdue’ actions. The duty person tried calling the pilot several times but received no response. It was soon confirmed that the helicopter had not arrived at the lodge and it was then declared to be missing.
- Another helicopter tasked with flying the pilot's two friends from Queenstown to the lodge was approaching Lake Wanaka at this time. The two pilots on board, including the second pilot who had flown the helicopter that morning, heard the duty person's radio calls and diverted the helicopter to fly up Stevensons Arm, at about 1325. They saw nothing relevant. At 1336 another helicopter arrived on the scene and started to search the area around Stevensons Island. An oil slick was observed at a location about 500 m north-west of the island. A weighted buoy was later dropped at this location.
- Additional helicopters soon arrived in the area and a search of the lake arm and Stevensons Island was undertaken. The only things of relevance found were some items washed ashore on Stevensons Island. These included pieces of the helicopter and cargo.
- Over the next two days searches using New Zealand Police sonar and a Royal New Zealand Navy (RNZN) remotely operated underwater vehicle confirmed the location of the helicopter. The deceased pilot and helicopter wreckage were recovered on the night of 23-24 July.
Aircraft information
- ZK-HTB was an RHC R44 Raven II helicopter, manufactured in May 2006 and imported into New Zealand later that year. The helicopter had been purchased by the owner in March 2012 and re-registered as ZK-HTB.
- The R44 is a four-seat light helicopter, powered by a normally aspirated piston engine (non-supercharged or turbocharged). Hydraulically boosted main flight controls assist in reducing control forces and eliminate feedback from the controls to the pilot. The R44 is normally flown from the front-right seat, but control extensions can be fitted for the front-left seat to permit dual instruction.
- ZK-HTB had a certificate of airworthiness in the standard category. This was non-terminating provided the helicopter was maintained and operated in accordance with the prescribed documents. The helicopter’s maintenance documents recorded that it had been maintained in accordance with the RHC maintenance schedule.
- In February 2018 a pilot had reported a main rotor blade, or blades, “going out of track intermittently”. The maintainer had undertaken maintenance actions, which included removing the main rotor blades and examining rotor head components. These were determined to be serviceable; however, some play or looseness was found in the pitch links. Both pitch link upper and lower rod ends were replaced, and the swashplate drive link was re-shimmed. A post-maintenance check flight was flown and the main rotor tracking and vibrations were determined to be within limits. No further main rotor tracking problems were reported. Several pilots who had flown the helicopter commented that the helicopter had not been as smooth to fly as the owner’s second R44. One pilot used the term “rougher”.
- The last maintenance check on the helicopter before the accident was a scheduled 100-hour check of both the airframe and the engine; this was completed on 23 June 2018. The helicopter had flown a further 21 hours, accruing a total of 2,860 hours at the time of the accident. There had been no recorded or reported maintenance issues relevant to the accident flight.
- A second pilot had flown the helicopter on the morning of the accident. That pilot reported that the helicopter had been performing well, and while it had been “a little bit rough” (the term “rough” was used to describe how the helicopter flew – that is, not as smooth as the owner’s second R44) there were no safety concerns (the second pilot had flown R44 helicopters since about 2003 and was a qualified helicopter instructor).
Weight and balance
- The weight and balance of the helicopter at the time of the accident was calculated using an assumed fuel load of about 70% or 125 litres when departing Wanaka. This was based on the reported fuel load on completion of the morning flight and the known upload immediately before the accident flight. The cargo and its locations were determined from CCTV footage. The weight of the pilot, who was seated in the front-right seat, was obtained from medical records.
- The weight of the helicopter was estimated to be about 960 kilograms, 174 kilograms less than the maximum allowable weight of 1,134 kilograms. The longitudinal centre of gravity was estimated to be 2.55 m from the datum (the reference point about which centre of gravity calculations are performed. For the R44 helicopter, the datum is 100 inches (2.5 m) forward of the main rotor shaft centreline), which was within the range of 2.337-2.6 m allowed for the estimated weight.
Site and wreckage information
- The wreckage was located on the lake floor approximately 500 m north-north-west of Stevensons Island at a depth of 47 m. Approximately 95% by weight of the helicopter was initially recovered and available for examination. The main items missing included the Perspex® windows, a section of the front-left door frame, sections of both landing skids, and the cargo pod (see Figure 4). Some of the cargo was also not recovered.
- The objects found on the island included items loaded into the cargo pod and rear of the helicopter at Wanaka, and two sections of main rotor blade. Several small pieces of cardboard were also found in thick bush 5-10 m in from the shore. These were identified as part of the cargo that was on board the helicopter. The found objects were distributed along about 95 m of the shoreline.
- As the helicopter was lifted to the surface, the tail section comprising the rear portion of the tail boom and the empennage (the tail assembly, comprising horizontal and vertical stabilisers and the tail rotor) was observed to be attached to the main wreckage by electrical cabling only. This section was secured and recovered separately. Fuel was drained from the helicopter after it was lifted onto a barge and in preparation for transportation. The quantity of fuel was estimated to be about half the capacity of the main tank, and matched the estimated fuel load with which the helicopter had departed Wanaka.
- Small pieces of Perspex® were also found in shallow water 50-100 m from Stevensons Island. A sonar search of the area around the main wreckage site, and between there and the island, identified several larger items near the main wreckage. These items were identified using underwater video as being part of the left door frame, the left cargo pod and the rear half of the right skid. The cargo pod and skid section were recovered for examination.
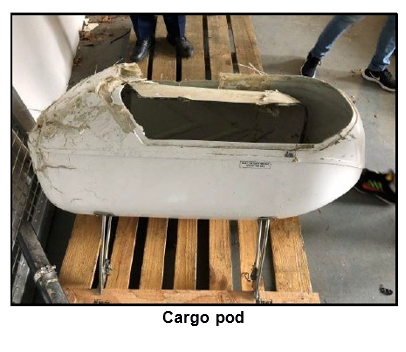
- The helicopter fuselage was severely damaged, with hydrodynamic deformation (crushing) evident on the front-left side. The line of deformation corresponded with the line of force applied to the front of the fairing (a structure whose primary function is to produce a smooth outline and reduce drag) covering the main rotor mast. The cargo pod also displayed deformation on the front, with the lid being torn off at its hinges. However, the lid remained connected by a spring used to assist in the closing of the lid. The three attachment points for the cargo pod showed the pod had been forced upwards and backwards. See Appendix 1 for a summary of the damage, including photographs.
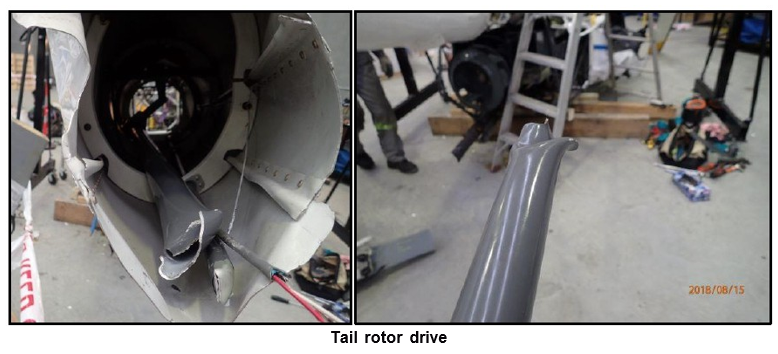
- The tail section, aft of where it had separated, displayed no obvious damage. The tail rotor rotated freely when examined. The direction in which the tail boom separated was to the left looking from the rear. The tail rotor drive tube displayed torsion or twisting-induced buckling. There was, however, no evidence of the tube contacting the inside of the tail boom after separating
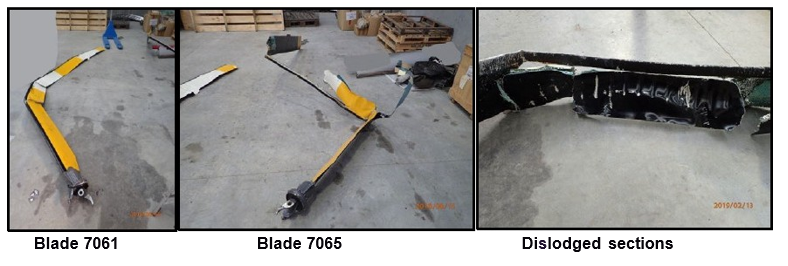
- Both main rotor blades remained attached to the hub but had rotated through about 180°. Scrape marks on both sides of the hub were consistent with the blades rotating to the upside-down position. One of the blades had bends of approximately 90° at about one-third and two-thirds along its length. A section of the aerofoil of the blade was also missing. The missing section started about 2.1m out from the hub and was nearly 1m in length. The two pieces of main rotor blade found washed ashore on Stevensons Island corresponded with the missing section.
- The two pieces of dislodged blade had evenly spaced score marks on their undersides. The score marks ran across their surfaces in a rearwards direction from behind the leading-edge spar. The spacing of the score marks matched the spacing of the screw heads on the canopy centre bow. Some secondary score marks also matched the spacing of screw heads on the window framing above the front-left passenger's seat. The paint coating on some of the screw heads on the window frame and canopy bow was scuffed. The compass, normally mounted on the canopy bow, had been forcibly detached.
- The second main rotor blade was complete and displayed no scrape marks. However, there was significant rearward bending of the blade at three locations along its length.
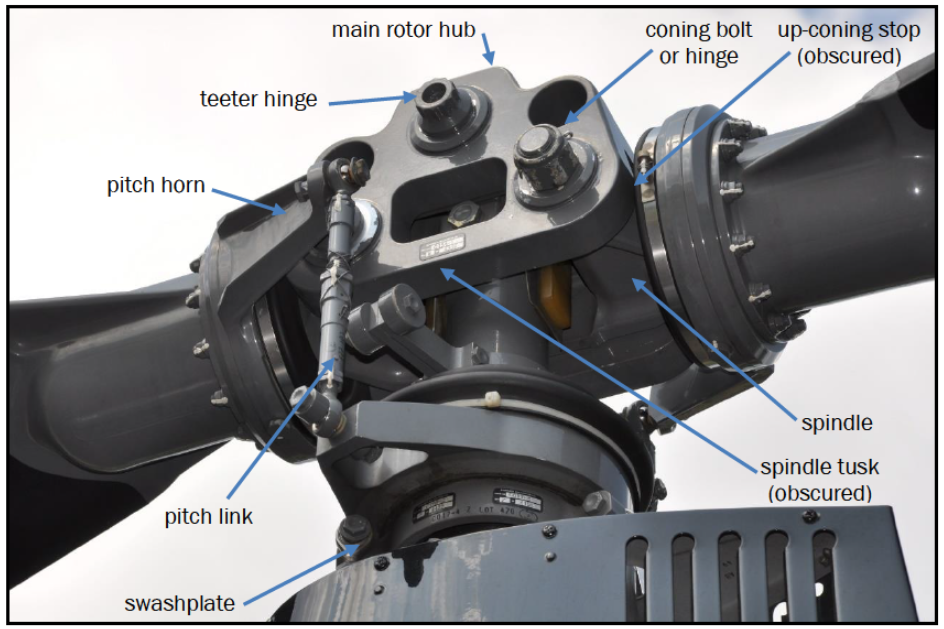
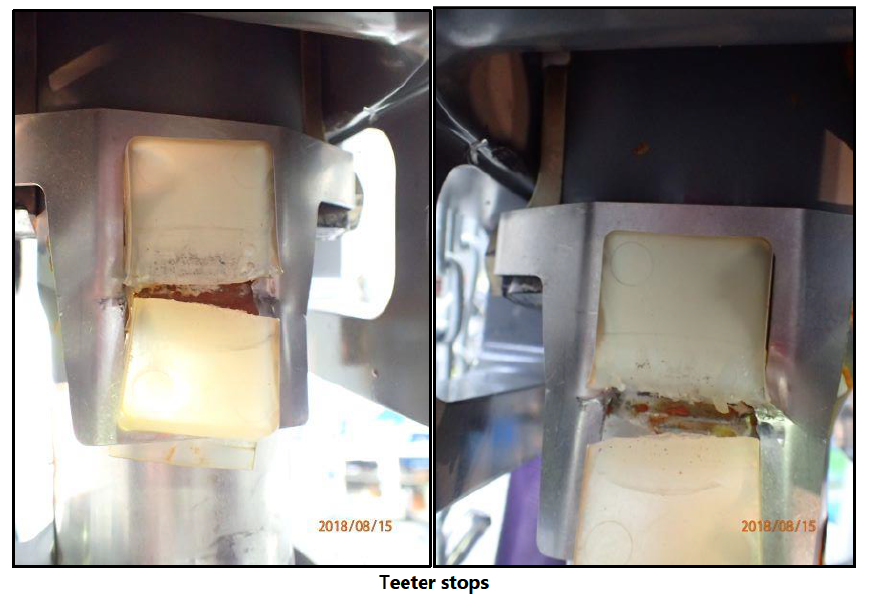
- The pitch links, which connected the main rotor pitch horns to the swashplate, and the flight control push rods had failed (see Figure 5). The teeter stops for both main rotor blades were crushed. The crushing had been of sufficient force to split the teeter stops in two. Both of the spindle tusks, one for each blade, were bent downwards by about 10°. Indentations corresponding to the profile of the spindle were visible on the adjacent surface of the up-coning stop, on the underside of the main rotor hub.
- The engine and associated accessories were closely examined. The engine crankshaft rotated without restriction. Each of the six cylinders had a satisfactory level of compression and suction as the engine was cycled.
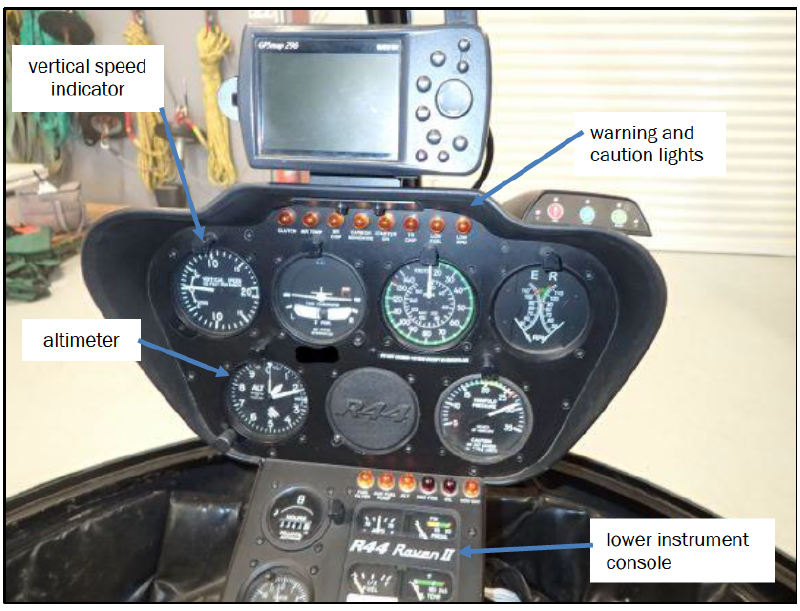
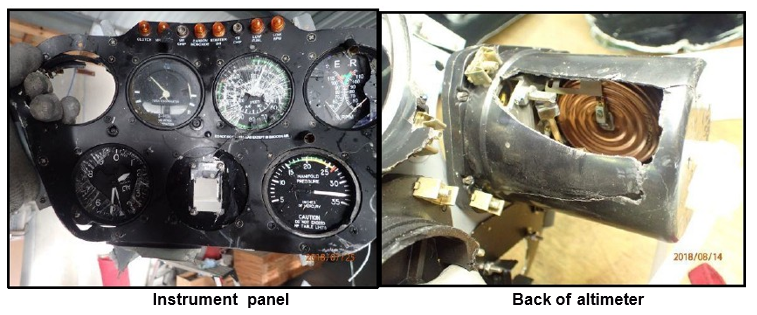
Instrument console
- The R44 upper instrument console contained the flight instruments and an array of warning and caution lights (see Figure 6). It was dislodged but remained attached by electrical wiring. The vertical speed indicator, located at the top left of the instruments, was missing.
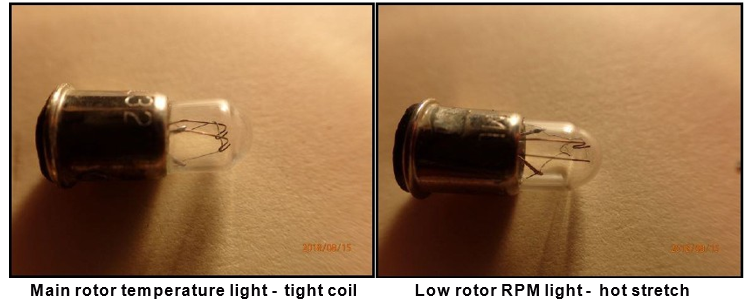
Warning and caution lights
- Both the 'Clutch' and the 'Low Rotor RPM' (low rotor revolutions per minute) warning and caution lights at the top of the panel displayed evidence of hot stretch. The remaining warning and caution lights either showed no evidence of hot stretch or were too damaged to provide any information.
Altimeter
- The glass face of the altimeter was broken and a section of its rear casing was missing. The missing section was on the upper side of the casing, exposing the internal mechanism. The initial examination found that much of the internal gearing, linkages and shafts either were damaged or had seized. The 10,000-foot (3,000 m) needle or indicator was free to rotate. However, the 100-foot (30 m) and 1,000-foot (300 m) needles had seized at a reading of 1,510 feet (460 m).
-
The altimeter was returned to the manufacturer in the United States to determine the validity of the reading. The manufacturer, under the supervision of two local Federal Aviation Administration (FAA) safety inspectors (acting on behalf of a National Transportation Safety Board (United States) accredited representative), examined the altimeter and concluded in its report that:
With a drastic impact to the top side of the altimeter, the linkage between the pressure sensing element and the top plate assembly (gear reduction mechanism) became disconnected. Based on the altimeter examination and discussion above, the altimeter was at 1,500 altitude when it received a momentary severe impact to the unit.
Telecommunications information
- The helicopter was fitted with a cellphone mount and connection that allowed a pilot to talk through their headset ‘hands free’. The microphone automatically activated when the pilot spoke into it. There was no requirement to operate a switch. Any radio transmissions took priority and muted the cellphone. The mount was located to the right of the upper instrument console in front of the pilot’s seat.
- Cellphone records showed that on the accident flight the pilot initiated an international cellphone call at 1258:49. This was approximately one minute after departing Wanaka Aerodrome. The connection ended at 1304:16. The recipient of the call was unaware that the pilot was flying at the time, nor did the content of the call, or the unannounced termination of the call, raise any concerns with them.
- The telecommunications provider advised that the manner in which the call disconnected showed that neither the pilot nor the recipient deliberately terminated the connection by either pressing ‘END’ or hanging up a receiver. Rather, the signal between the pilot’s phone and the cell tower, through which it was connecting, was suddenly lost.
- Transport Accident Investigation Commission (Commission) investigators confirmed that cellphone coverage in the area of the accident site was good. However, although voice calls were still possible, signal strength did reduce when descending to lake level.
Personnel information
- The pilot had begun pilot training in March 1999, initially flying aeroplanes and obtaining a private pilot licence (aeroplane) in January 2000. The pilot’s most recent biennial aeroplane flight review had been on 22 January 2017. The pilot had accrued a total of 880 hours on aeroplanes at the time of the accident.
- The pilot had started formal helicopter training in September 2012, obtaining a private pilot licence (helicopter) on 12 November 2012. The pilot’s log book recorded a total of 390 hours on helicopters leading up to the accident flight, including 375 hours on the R44 type of helicopter. The pilot’s last two-yearly RHC Safety Awareness Training refresher, which included classroom and flight training, had been conducted in conjunction with the biennial helicopter flight review on 5 October 2016. The person conducting the training reported that the training had included a review of RHC safety notices, and would have made reference to the associated safety videos. The training had identified no concerns.
- The pilot held a current ‘class 2’ medical certificate valid until 8 July 2019. The certificate contained no restrictions. The pilot’s latest aviation medical examination report and general practitioner files contained nothing of relevance. People who knew and saw the pilot on the day of the accident commented that they had had no concerns about the pilot’s health.
- The pilot’s helicopter log book recorded that the pilot had flown an R44 helicopter between Wanaka Aerodrome and the Upper Estuary Burn Valley area on nearly 370 occasions. The pilot had also flown the same route numerous times in aeroplanes.
- The pilot’s autopsy results found that the pilot sustained high-energy impact injuries. Toxicology results were negative for any performance-impairing substances.
Meteorological information
- A front was passing over the region at about the time of the accident. The MetService forecast for the Alpine Region, including Wanaka, was for west-north-west winds of 20-25 knots (37-46 km/h), with the winds backing (turning in an anti-clockwise direction) to become more westerly at higher altitudes. Moderate turbulence was predicted over most of the South Island with the passage of the front.
- The forecast for Wanaka Aerodrome, issued at 1116, predicted that between midday and midnight on 21 July the surface wind would be 310° true (a bearing of 310° from true north) at 15 knots, gusting to 25 knots (30-45 km/h), visibility of 20 km, with rain and scattered cloud (cloud is measured in eighths or oktas, with scattered being 3-4 oktas and broken 5-7 oktas) at 3,000 feet (914 m) above the aerodrome. Between 1200 and 1400, the wind was predicted to change to 330° true at 25 knots, gusting to 35 knots (45-65 km/h) before easing back.
- An automated meteorological station at Wanaka Aerodrome recorded the local weather conditions every 30 minutes. The report issued at 1300 recorded the following information:
- surface wind – 300° true at 8 knots (15 km/h), varying between 260° and 330° true
- visibility – 20 km with rain present
- cloud scattered at 3,300 feet (1,005 m), broken at 4,100 feet (1,249 m) and broken at 5,000 feet (1,524 m)
- temperature – 9° Celsius, dew point 5° Celsius
-
pressure – 997 hectopascals.
The recorded conditions at 1230 were similar to the above. After 1330 the wind backed slightly to become more westerly, while the other conditions remained about the same.
- CCTV footage taken from cameras located in the Wanaka township and at the aerodrome recorded showers passing through the area (see Figure 7). The wind was generally from the north-west, sufficient to cause swells and occasionally produce significant whitecaps.

- Further weather information was obtained from multiple private weather-recording sites located about the Wanaka basin. The local topography resulted in significant variations in the recorded wind strength and direction between sites. However, the information showed that a generally light to moderate north-west wind prevailed over the lake and basin, the area in which the helicopter was flying, at about the time of the accident.
- A witness who resided on the northern outskirts of Wanaka saw the helicopter flying north past Albert Town towards Stevensons Arm. The witness described the conditions into which the helicopter was flying as windy and raining. The wind was reported to be possibly strong enough to cause whitecaps on the lake.
- The two pilots who were the first on the scene about 20 minutes after the accident occurred (see paragraph 2.8) reported encountering some turbulence while en route to Queenstown, described as “bumpy” but not severe. However, by the time they approached Lake Wanaka the conditions had eased. At Stevensons Island the wind was assessed as being from the north-west at about 15 knots (30 km/h) on the lake surface, sufficient to produce the occasional whitecap. By the time the second helicopter arrived on the scene 10 minutes later, the conditions were such that the pilot of that helicopter easily saw the oil slick.
Analysis Tātaritanga
Introduction
- The pilot was on a flight between the helicopter owner’s base at Wanaka Aerodrome and a lodge in the Upper Estuary Burn Valley. When passing Stevensons Island the pilot encountered an unexpected and catastrophic event. The helicopter as a consequence fell uncontrollably into the lake, north of the island.
- The pilot was familiar with the route, having flown it regularly and often, including in weather conditions similar to those on the day of the accident.
- There were no witnesses to the accident and no in-flight recording of aircraft data or images. The Commission has discussed the safety issue of a lack of in-flight recording in previous investigations and made a recommendation to the Secretary of Transport on the matter (TAIC 2015) (Transport Accident Investigation Commission Final Report AO-2015-002: Mast bump and in-flight break-up, Robinson R44, ZK-IPY, Lochy River, near Queenstown, 19 February 2015).
- The following section analyses the circumstances surrounding the occurrence to identify those factors, which increased the severity of its outcome. It also examines any safety issues, which have the potential to adversely affect future operations.
Accident sequence
- The distribution of Perspex® and other small items where the helicopter was found and on the island, along the shoreline and several metres inland showed that the helicopter very likely broke up in flight. The spread of Perspex® in particular was indicative of the canopy being damaged in flight. The damage identified on the teeter stops also showed that the main rotor blade had teetered or swung beyond its limits and struck the teeter stops fixed to the main rotor shaft. The damage to one of the main rotor blades was consistent with it striking the canopy at this time. In addition, damage to the instrument panel and altimeter, and the missing vertical speed indicator, were consistent with the blade entering the cabin. The striking of the main rotor with the canopy was likely to have been the result of the main rotor blade flapping down at the front of the helicopter.
- The damage to the main rotor showed that it was likely to have stopped rotating just after this strike. This sudden stoppage of the main rotor and transmission almost certainly caused the torsional overload and subsequent failure of the tail rotor drive shaft. The evidence of low rotor RPM light illumination was also consistent with this sudden reduction in main rotor speed.
- Prior to the in-flight break-up, the satellite tracking data showed that the helicopter was in a steady cruise. The possible initiation events that resulted in this accident sequence are discussed below.
Initiation event
- The investigation considered several events that could have initiated the accident sequence. They were grouped into three categories:
- mechanical failures – cargo pod, flight controls, engine, rotor system, fuel exhaustion
- operational events – flight control interference, pilot medical event, bird strike, distraction
- mast bumping events – low rotor RPM, abrupt control movements, low-G (low gravity), turbulence.
- All of these categories were considered in relation to the circumstances of the accident, and are discussed in the following sections.
Mechanical or structural failure
- It was exceptionally unlikely that the cargo pod, located on the left side of the helicopter, came loose in flight and caused a loss of control. The pod was found on the lakebed within a few metres of the main wreckage. This, combined with damage to the front of the pod and its attachment fittings, confirms that the pod very likely separated as the helicopter struck the water nose-first.
- There was no evidence of a mechanical issue that might have contributed to the helicopter descending uncontrollably. The flight control systems were inspected and determined to have been intact before the helicopter departed controlled flight. There was sufficient fuel on board and the engine had been inspected and considered to be serviceable. Furthermore, the cellphone call by the pilot did not raise any concerns with the call recipient leading up to the helicopter departing controlled flight.
- A failure of a pitch link was unlikely to have initiated the accident sequence. Both pitch links were found to have failed; however, the failures were consistent with excessive blade flapping and striking either the cabin or water.
- The impact marks on the blade that struck the cabin started behind the leading-edge spar. This indicated the blade was still likely connected to the pitch link at the time of impact and flapped down excessively in a flat motion. The cabin may have also pitched nose-up coincident with the blade flapping down.
Operational event
- It was considered unlikely that any of the items loaded on board the helicopter would have interfered with the flight controls. Most of the items were secured either in the cargo pod or in the back of the cabin. The second set of flight controls was not fitted and there was no indication from the cellphone call of the pilot having any concerns about items moving about in the cabin.
- There was no evidence of any pilot health issue that might have contributed to the accident. The pilot was reportedly in good health, both generally and on the morning of the accident. There was also nothing found of relevance in the autopsy or toxicology tests.
- There was no evidence to suggest that a bird strike occurred.
Mast bumping event
- The term ‘mast bumping’ is associated with helicopters fitted with a ‘semi-rigid’ rotor head design, and describes the inboard end of a main rotor blade striking the main rotor shaft. This is caused by the main rotor hub swinging or teetering excessively about the teeter hinge (see Figure 5).
- The observed damage to the teeter stops in this accident indicated that mast bumping had occurred. The teeter stops were crushed through and both spindle tusks were bent downwards, which showed that the mast bumping was severe. However, evidence of mast bumping does not necessarily mean it was an initiator of an accident sequence. Mast bumping can, for example, occur as a result of a main rotor striking an object while still rotating.
- The difference between the angle of the main rotor disc, when it was perpendicular to the mast, and the angle required to strike the cabin was calculated to be about 55° (depending on the pitch angle of the blade at the time it struck the canopy. Data provided by RHC) In forward flight, the main rotor disc is tilted forward to propel the helicopter forward. A maximum allowable 10° downward movement of the blade about the coning and teeter hinges accounted for this tilting. The blades also coned or bent upward as a result of generating lift. Therefore, for the blade to strike the cabin, there needed to be significant additional tilting of the main rotor through a possible combination of the:
- deflection of the main rotor gearbox mounts
- distortion of the pitch link
- crushing-through of the teeter stop
- bending of the tusk
- flexing down of the main rotor blade.
- There are four known factors that, singularly or in combination, can contribute to mast bumping and result in excessively large downward deflection of the blade. They are:
- low main rotor speed
- large, abrupt control movements by the pilot
- low-G
-
turbulence.
Each of these factors has been considered with respect to the circumstances of this accident and are discussed in the following sections.
Low main rotor speed
- Low main rotor speed occurs when the power demanded exceeds the power available. This can occur while flying tight manoeuvres or lifting heavy loads. It can also occur when there is a power loss and a pilot does not lower the collective lever quickly enough to enter autorotation and maintain rotor speed.
- With reduced rotor speed, the blades deflect upwards. Unless immediately corrected, the rotor speed continues to decay and the blades continue to deflect up. If this situation continues, the blades stall and lift suddenly reduces.
- The upward deflection causes creases along the surfaces of the blades. The crease marks run chordwise from the leading edge of a blade to the trailing edge.
- In this accident there were no crease marks along the blades, so there was very likely no excessive deflection upwards of the blades. Similarly, there were no problems identified with the engine that would have prevented it operating. It was therefore exceptionally unlikely that the rotor speed reduced below the safe limit.
Large, abrupt control movements by the pilot
- Any large and/or abrupt movement of the cyclic will cause the rotor disc to teeter. This has the effect of reducing the separation between the hub and the mast. A United States National Transportation Safety Board (NTSB) study of RHC R22 accidents involving a loss of main rotor control found that “large, abrupt control inputs can lead directly to mast bumping” (NTSB 1996). The R44 shares the same design features as the R22 and is therefore similarly susceptible to pilot-induced mast bumping.
- The flight-tracking report showed the pilot was maintaining a steady cruise as the helicopter approached Stevensons Island. The trapped altimeter reading closely matched the altitude recorded in the final position report. There was nothing reported by the recipient of the cellphone call to indicate the pilot was overly concerned or in trouble. The pilot was also current with the RHC Safety Awareness Training and would have likely been cognisant of the need to avoid any sudden and excessive control input. It was therefore considered unlikely that the pilot made a control movement that was not in response to an external event that would have resulted in the mast bump.
Low-G
- Low-G is a situation when the occupants of an aircraft feel a sensation of reduced weight. Low-G can be induced by a pilot rapidly moving the cyclic forward. In a helicopter with a teetering rotor head, and because of the position of the helicopter’s centre of gravity and the tail rotor thrust line, a roll to the right can be induced if the pitch forward is strong enough and the tail rotor thrust line moves high enough (for a main rotor, like that of the Robinson types, which turn anti-clockwise when viewed from above). When unloaded, the rotor disc remains in the same plane of rotation, or slowly lags behind the right roll of the fuselage. In effect, the pilot experiences the helicopter starting to roll right, but the rotor disc may stay about level. If the pilot moves the cyclic left to counter the apparent roll, the angle between the rotor disc and the mast on the left side is reduced even further – possibly to the point where mast bumping occurs.
- A higher power setting will result in more rotor torque being generated, requiring more tail rotor thrust to counter the torque effect. In addition, the faster the helicopter’s airspeed, the higher the tail rotor thrust line is in relation to the helicopter’s centre of gravity. The combination of high power and a high thrust line results in a faster roll in a low-G encounter.
- As discussed in the previous section, it was unlikely that the pilot initiated the accident sequence by applying a large, abrupt forward movement of the cyclic during the cruise phase of flight. However, the helicopter may have entered an area of severe turbulence that generated a low-G situation. This is discussed further in the following section.
Turbulence
- Turbulence is an agitation of the air, resulting in changes in wind velocity (horizontal and vertical) that suddenly alter the flightpath of an aircraft. According to the International Civil Aviation Organization, turbulence is rated as light, moderate, severe or extreme, according to the effects on the aircraft and its occupants (see the glossary for a description of each category).
- Turbulence is a known contributor to mast bumping. Large, sudden upward or downward gusts can upset a helicopter and cause the blades to flap up or down excessively, or cause a low-G situation. Inappropriate or inadvertent pilot inputs or over-controlling by the pilot can further exacerbate the effects of the turbulence.
- On the day of the accident, the meteorological forecast for the area that covered the accident location predicted moderate turbulence. Witness accounts, weather station records and CCTV recordings also confirmed that at about the time of the accident there was a north-westerly wind present in the area of the flight, which varied in strength from light to moderate and possibly stronger in places.
- Although a meteorological forecast provides a pilot with a forecast of the weather for a region, reports from other pilots who have been flying in the region also provide useful information for localised conditions.
- A second pilot had flown the same helicopter along the same route earlier that morning. This pilot described the weather conditions in the morning as a typical north-westerly day. The wind at Wanaka Aerodrome was 10-15 knots (20-30 km/h) with the occasional passing shower. The wind at the windiest portion of the flight reportedly increased to 30-35 knots (55-65 km/h). While the second pilot observed whitecaps in Stevensons Arm, they did not recall any disturbances to the surface of the lake, which would normally indicate areas of strong downdraughts or turbulence (termed by local pilots as ‘williwaws’, to describe a strong wind gust striking the water and blowing up spray).
- The second pilot further commented that the weather changed significantly between the morning flight and the flight up Stevensons Arm about 20 minutes after the accident. The conditions changed from a strong north-westerly with little rain to a light wind with heavy rain. Pilots involved in the search reported that the weather continued to improve rapidly during the afternoon. These observations were consistent with the front passing through the region around the time of the accident.
- In addition, Stevensons Arm was known by local pilots as an area where strong, localised turbulence could be generated due to the surrounding terrain. They commented that this was especially so in north-westerly conditions, when the wind funnelled through the saddle at the top of the arm and swirled around in the lee of the hills. The turbulence would generally increase with an approaching westerly front, and dissipate rapidly as the front passed.
- In the absence of any other initiating factors, the Commission considered that the helicopter was likely to have encountered severe or extreme turbulence during the accident flight. The Commission was unable to determine if a single turbulence event resulted in the immediate loss of control, or if the pilot’s response to the turbulence contributed to the loss of control.
Flight planning
- The investigation examined several aspects of the planning of the flight. Good flight planning and decision-making involves examining all aspects of the planned flight, including the weather conditions and the limitations of the pilot and the aircraft, to determine whether the risks are acceptable.
Meteorology
- A key aspect of good flight planning and decision-making involves obtaining weather information from various sources. This ensures that the pilot has a good mental picture of the weather throughout the flight.
-
In the case of the accident flight, the forecast conditions and the observed conditions reported to the pilot showed a cold front was passing through the area. According to Meteorology for PPL Pilots Edition 2 2019 (Superseded by the 2022 edition) (https://static1.squarespace.com/static/67ca338c4955f86c9f7df437/t/68f584a91e3bde3f222e18e9/1760920745488/PPL-2023-digital-edition.pdf):
Cold fronts are most likely to produce thunderstorms and/or heavy showers because of their unstable nature. The poor weather associated with cold fronts generally lasts no more than 2 – 3 hours (although there are exceptions).
-
In regards to turbulence, the Civil Aviation Authority of New Zealand’s (CAA’s) booklet, Good Aviation Practice: VFR Met, stated the following:
Turbulence
Review wind conditions for departure aerodrome, the cruise, and destination. You will also need a mental picture of vertical wind profiles, so you can select the best altitude(s) for cruise flight, the best flight path to mitigate turbulence, and to determine whether wind shear is present.
Consider the wind direction and the effect terrain will have on the wind’s behaviour. A small angular change in the direction the wind is striking terrain can make a significant difference to turbulence, making it greater or lesser. Are the winds at departure and destination likely to be affected by a sea or land breeze?
Also take into account surface heating leading to convective turbulence. This will be particularly noticeable on warmer days.
-
The World Meteorological Organization’s Guide to Instruments and Methods of Observation (World Meteorological Organization Guide to Instruments and Methods of Observation, Part II, see https://library.wmo.int/doc num.php?explnum id=4147 Chapter 3. Aircraft-based Observations, 2018) stated that:
Turbulence, especially clear-air turbulence (turbulence in the absence of clouds), is an important and potentially dangerous phenomenon in aviation. Although for routine commercial operations flight paths are designed to avoid turbulence inevitably, aircraft will experience unexpected bumpiness and the departure from normal level flight can be measured by the aircraft instrumentation.
-
The guide went on to state that:
“… the severity of turbulence affecting an aircraft depends principally on airspeed, the mass of the aircraft, the altitude and the nature of the turbulence itself.”
-
Although the pilot had access to local-area forecast information, the mountainous environment in which the helicopter was being flown, local terrain and weather conditions meant the pilot’s knowledge of the flight route, local observations and reports from the other pilot would have provided more up-to-date and accurate sources of weather information. This is further reinforced in the CAA’s booklet, Good Aviation Practice, Mountain Flying, which states:
All mountainous terrain can be subject to severe and rapidly changing weather conditions… because conditions can alter with subtle changes of wind strength and direction, it should be obvious that a watchful eye must be kept on the weather conditions, both at the flight planning stage and throughout the flight.
- The pilot was reportedly familiar with the weather conditions present in the Wanaka basin on the day. The pilot also had access to local observations. The second pilot, who had flown the helicopter in the morning, had also talked to the pilot before the flight. During that conversation neither pilot had raised any concerns about the helicopter, the flight or the weather conditions. This local information identified that the weather was above the minimum requirements for a visual flight rules flight (flight in visual meteorological conditions (conditions in which flight solely by visual reference is possible).
Pilot
- The pilot had flown aeroplanes between 1999 and 2012 before beginning formal helicopter training. The pilot had accumulated more aeroplane flight hours than helicopter flight hours at the time of the accident. RHC had identified in the helicopter’s Pilot Operating Handbook that “airplane (aeroplane) pilots have a high risk when flying helicopters” (RHC Safety Notice SN-29, issued March 1993 and revised June 1994). This was due to the ingrained reactions of flying an aeroplane, which if applied in a helicopter could result in its destruction. This was especially so in the use of the cyclic. However, the pilot’s most recent RHC Safety Awareness Training, which had been conducted in conjunction with the biennial helicopter flight review, had identified no concerns. In addition, an instructor who knew the pilot well reported that they believed the flight to be within the pilot’s capabilities.
Helicopter
- The capabilities and limitations of an aircraft in the likely weather conditions should be considered when planning and conducting any flight.
- The RHC R44 helicopter had a teetering rotor design. In addition to the teetering design, the ‘tri-hinge’ rotor was unique to RHC helicopters. These design choices in RHC helicopters meant they were more susceptible to mast bumping conditions and less capable of operating in turbulence when compared to those with other rotor head designs. This required pilots of RHC helicopters to consider and monitor the likelihood of turbulent weather conditions much more closely than would be required when operating other helicopter types.
- This susceptibility to the effects of turbulence was also reflected in RHC documentation. The Pilot Operating Handbook for all RHC helicopters recommended that pilots reduce speed and use caution when flying solo or lightly loaded. It also recommended avoiding flying in high winds or turbulence. It was not clear whether this referred to all turbulence severities or severity above a specified level. (See paragraphs 3.61 and 3.72 for further discussion on this.)
Decision to fly
- Pilots are responsible for decisions to conduct private flights, and must consider all the available information when making those decisions. As they are individual decisions, when presented with the same information one pilot may elect to fly where another may not. This can be a result of the pilot’s experience, their awareness of their own limitations or their risk tolerance. When making decisions to fly, pilots should always err on the side of caution.
- In this accident the pilot had collected the necessary information to make an informed decision on the conditions of the day. The weather conditions were above the minimum requirements to conduct the flight, but the passing cold front, wind, forecast turbulence and reduced visibility meant they were not ‘good’ flying conditions. This meant that the decision on whether to fly was ambiguous and required the pilot to exercise judgement based on the available weather information, their own knowledge and weather limits, and the capability of the helicopter.
- The pilot also had alternative means available to reach the destination had the flying conditions been deemed unsuitable. These arrangements had been used in the past and indicated that there was unlikely to have been a self-perceived pressure to conduct the flight.
- Although in hindsight the decision to fly appeared to have been incorrect, the Commission determined that it was about as likely as not that the decision to fly was appropriate based on the information available at the time the decision was made.
In-flight decision-making
- Operating an aircraft requires the pilot to constantly anticipate and monitor the state of the aircraft and the environment in which it is operating. This ensures that appropriate and safe decisions are made to minimise the risk of adverse outcomes. This is especially so when the weather conditions are less than ‘good’. The investigation examined several aspects regarding the conduct of the flight.
Distraction
- Any additional task has the potential to distract a pilot and draw their attention away from the primary responsibility of operating the aircraft safely. This is more likely during a period of high workload, for example when landing or during an emergency.
- Cellphones, especially those connected to a pilot’s headset or helmet, are a common feature in aircraft flown by single pilots. They also have the potential to divert attention from activities necessary for safe operations (NTSB Safety Alert 025 – May 2013, Rev. December 2015).
- During the accident flight the pilot made a call, but only after take-off and when clear of the Wanaka Aerodrome circuit area, which were critical phases of the flight. However, the timing of the cellphone disconnection indicated that the pilot was very likely still on the phone when the helicopter departed controlled flight. Although nothing in the cellphone conversation indicated the pilot was under stress or in any trouble, the call had the potential to be a distraction for the pilot.
- The Commission was unable to determine whether the distraction associated with using a cellphone contributed to the accident. However, pilots should ensure that communication and electronic devices are not used for purposes other than those intended to support their flights.
Aircraft speed
Safety issue: The use of ‘significant’ in describing turbulence in the R44 Pilot Operating Handbook was non-standard and not defined. This had the potential to create further ambiguity in assessing the severity of turbulence.
- The flight tracking data showed that the flight was proceeding as expected when approaching Stevensons Island. Taking into account the prevailing north-westerly wind conditions and the geography of Stevensons Arm, the recorded groundspeed of 96 knots (178 km/h) at the second position report equated to an airspeed of 105-110 knots (195-200 km/h).
- The manufacturer of the cargo pods produced a pilot operating handbook supplement that stated that, with a cargo pod fitted, the maximum permitted airspeed was 115 knots (210 km/h) (the maximum permitted speed without a cargo pod fitted was 130 knots (240 km/h)). A placard beside the airspeed indicator in the helicopter read: DO NOT EXCEED 110 KIAS (KIAS – knots indicated airspeed) EXCEPT IN SMOOTH AIR. Therefore the 105-110 knot speed estimation is what would be expected in good conditions.
- The Pilot Operating Handbook recommended that pilots reduce airspeed to 60-70 knots (110-130 km/h) in significant turbulence. The term ‘significant’ was not defined in the handbook. An RHC educational video, produced in February 2017 in support of Safety Notice 32: High Winds or Turbulence (see 3.73), advised that the term ‘significant’ was used as this allowed a pilot to determine what was significant to them based on their experience and comfort level. In June 2020, RHC amended the R44 Pilot Operating Handbook to explain the term ‘significant’, which aligned with the commentary in the educational video.
- While the pilot would have likely had an indication of the weather conditions as the helicopter flew up Stevensons Arm, there were various pieces of information available indicating that flying close to the maximum permitted speed would have likely increased the risk of an adverse outcome.
- The helicopter was relatively light, which made it more susceptible to mast bumping in turbulence. The weather conditions were less than ideal and the helicopter was flying in a mountainous area that was known for localised turbulence. These factors should have been indicators that flying at close to the maximum permitted speed increased the risk of an adverse outcome. A high power setting would also have increased the risk.
- The cellphone call disconnected at 1304:16. This was 51 seconds after the last position report and when the helicopter was recorded as having a groundspeed of 96 knots (178 km/h or 49 metres per second). At this speed the helicopter should have travelled 2.5 km from the last position report. However, the main wreckage was located 336 m short of this position.
- This disparity suggested that either the helicopter slowed after the last position report and the cellphone disconnected during the initial strike, or the cellphone remained connected until about the time the helicopter struck the surface of the lake. Both scenarios were considered plausible.
- To have travelled from the last reported position to the crash site, the pilot would have had to slow the helicopter from 96 knots (178 km/h) to as slow as an average of 82 knots (152 km/h) (other variables include when in the sequence the cellphone disconnected and the distance the helicopter was thrown forward after the main blade strike). This reduction in average groundspeed could have been due to:
- an increase in headwind as the helicopter faced more into the prevailing wind;
- the helicopter slowing as a result of a levelling-off after descending about 300 feet (91 m) from the earlier position report; or
- the pilot slowing the helicopter to the recommended speed after the last position report in response to observed conditions.
Mast bumping accidents
Safety issue: The lack of reliable evidence on the initiating cause or causes of mast bumping occurrences continues to limit the effectiveness of safety investigations.
- In the 10 years preceding this accident, the Commission investigated five RHC helicopter accidents in the mountains involving mast bumping leading to in-flight break-ups (TAIC 2008, TAIC 2011, TAIC 2013, TAIC 2014, TAIC 2015). The CAA investigated one other (CAA 2012). Turbulence was cited as a possible factor in five of the six accidents. In the sixth accident the weather conditions were reported as calm, with the potential for isolated turbulence being considered ‘about as likely as not’.
- All six accidents occurred while the helicopters were transiting between locations. The helicopters all weighed less than the maximum allowable weight at the time of the in-flight break-ups, and in most cases they were significantly below the maximum weight limit.
- RHC has previously advised the Commission that pilot actions were most likely the primary reason for mast bumping accidents in New Zealand, by the pilots flying too fast for the conditions and/or reacting incorrectly to any helicopter upset (TAIC 2015). However, with no survivors or witnesses, it has been impossible to confirm or counter this assertion definitively.
- The Commission has previously identified the lack of evidence following an accident involving an RHC helicopter as a safety concern and made a recommendation on this matter (Transport Accident Investigation Commission, Final Report AO-2015-002: Mast bump and in-flight break-up, Robinson R44, ZK-IPY, Lochy River, near Queenstown, 19 February 2015, recommendations 014/16 and 015/16). Several parties, including RHC, are currently developing suitable recorders for installation on the various types of RHC helicopter.
- The Commission has also previously identified a lack of knowledge about the dynamic behaviour of two-bladed, teetering, underslung rotor systems and made a recommendation to the Federal Aviation Administration on the matter (Transport Accident Investigation Commission Final Report AO-2013-003: Robinson R66, ZK-IHU, Mast bump and in-flight break-up, Kaweka Ranges, 9 March 2013, recommendation 005/16). RHC has advised the Commission that it is currently providing additional information to the University of Maryland as part of a study of the performance of the main rotor system.
Training for RHC pilots in New Zealand flying conditions
- About 60% of New Zealand’s terrain and about 85% of the South Island’s terrain are designated as mountainous (Aeronautical Information Publication (AIP New Zealand), GEN3.3-17 and 3.3-18, effective 12 May 2005), the rest being mostly undulating. Mechanical turbulence or turbulence generated by the movement of air over terrain is therefore a common feature of flying around the country at low levels. However, turbulence and its severity can be difficult to predict. Turbulence can modulate in strength rapidly and can be localised. Predictions of turbulence therefore need to be general and cautious. In addition to meteorological forecasts, pilots need to be aware of the potential for turbulence by looking for the cues that indicate turbulence might be present and adjusting their flightpaths to suit, or be prepared to land if necessary.
- The RHC Pilot Operating Handbook for the R44 contained a safety notice regarding flying in high winds and turbulence:
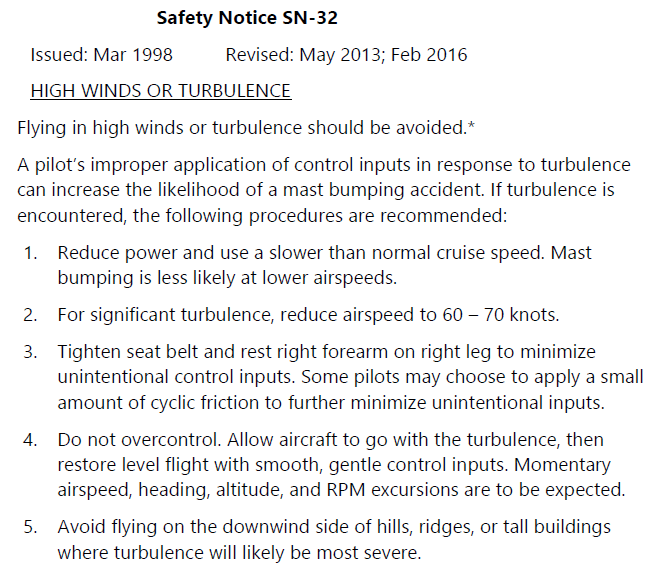
The helicopter is more susceptible to turbulence at light weight. Reduce speed and use caution when flying solo or lightly loaded.
* This sentence was added in February 2016.
-
Pilots who fly the R44 (and the R22) helicopter are also required to complete biennial Robinson Safety Awareness Training courses (CAA Notice of Requirement NTC 61.365, Revision 1 dated 30 October 2017). The training syllabus has ground and in-flight components that include such topics as mast bumping, low-G hazards, flight into turbulence and a review of RHC safety notices. On 10 June 2020, the CAA provided the Commission with further detail regarding this training:
The CAA is currently active in providing Robinson Safety Awareness Training (RSAT) to Robinson helicopter pilots. Included in the package is a safety video aligned to Safety Notice 32 which defines significant turbulence. The video is a resource that both instructors and pilots watch and the Robinson Helicopter Company have made it a discussion item rather than a formal definition in order to provide a student important information on the issues that can arise when encountering turbulence.
- The ‘package’ referred to CAA Notice of Requirement NTC 61.365 dated 30 October 2017. The notice covered Robinson Safety Awareness Training and a syllabus of training. The syllabus included a “review of RHC safety notices” but made no reference to any videos. The CAA later clarified that, while the training syllabus made no reference to the safety videos, “pilots would be made aware of exposure to high winds/turbulence, including a safety video” when undergoing Robinson Safety Awareness Training. Discussions with five of the larger training providers confirmed this assertion.
- The pilots involved in the accidents identified in paragraph 3.67 had completed the safety courses and met the currency requirements at the time of the accidents. In three of the accidents the pilots had extensive RHC helicopter experience, and in two of these the pilots were also instructors. These circumstances suggest that this training on its own is not sufficient to avoid these types of mast bumping accident. The manufacturer should continue its efforts to understand how these accidents occur to assist in implementing effective measures to prevent their occurrence.
-
The recommendations referred to in paragraphs 3.69 and 3.70 continue to be valid. Pilots also need to continue to be cautious in their decision-making when planning and conducting flights. For these reasons, mast bumping involving RHC helicopters remains on the Commission’s Watchlist, which states:
Operators must select a type of aircraft suited to the risk profile of the intended use. Similarly, all pilots must understand the helicopter’s operating limitations, avoid circumstances which could see these inadvertently exceeded, and receive proper training in the causes, dangers, and prevention of mast bumping, including in low-G conditions. It is particularly important for Robinson pilots to be aware of the risks of flying a lightly loaded helicopter at high speed in turbulence. Prohibitions against in-flight low-G demonstrations must be observed, and low-G recovery training must be conducted only on the ground.
Appendix 1. Wreckage examination
General
The fuselage of the helicopter was severely disrupted, with evidence of more extensive crushing to the front-left corner of the cabin. In comparison, the tail section, comprising the rear section of the tail boom and empennage, was virtually undamaged other than where it had separated at the tail boom.

Flight controls
With the exception of the centre section of the tail rotor push-pull tube, all flight control components were accounted for. Control continuity was confirmed with no evidence of any pre-impact wear or failure. The breaks and bending of the flight control systems were consistent with the distortion of the fuselage and were considered to have occurred on impact with the water.
Power train
There was little visible damage to the engine. Water was found in the cylinders. The engine could be turned, with suction and compression noted on all cylinders. Scuffing on the upper sheave was, according to RHC, "an indication of rotation of the engine at impact, regardless of rotation of the main rotor/tail rotor drive train and transmission". The drive belts were intact. The sprag clutch would initially not rotate. Water was drained and the clutch would then rotate, but it was still stiff and ratchety.
Instruments
The flight instrument panel had become dislodged, but remained attached by cabling. The warning lights were examined for indications of hot stretch. The filaments for both the 'Low Rotor RPM' and the 'Clutch' showed evidence of hot stretch. The indication lights for 'Low Fuel', 'Alternator', 'Oil Pressure - Engine' and 'Carbon Monoxide' displayed tight coils. The remaining lights were too damaged to determine their state.
The altimeter retained a trapped reading of 1,510 feet (460 m). The rear casing of the instrument was broken and internal connections were damaged.
Main rotor
Both main rotor blades remained attached to the hub. The pitch links that connected the main rotor blade pitch horn to the swashplate were both broken. Both blades had rotated about 180° to an upside-down position. The teeter stops for both blades were crushed through. The spindle tusks for both blades were bent downwards by about 10°.
One main rotor blade (serial number 7061) was relatively flat in plane with three rearward bends. There were no chordwise (leading edge to training edge) crease marks to indicate the blade had bent excessively upwards or downwards.
The other main rotor blade (serial number 7065) had two nearly 90° bends along its length. The first, approximately 1.4 m from the hub, was upwards. The second, approximately 3 m from the hub, was downwards. There were no chordwise crease marks to indicate excessive or sustained flexing of the blade. An approximately 0.9 m section of blade skin and honeycomb from behind the leading-edge spar and in-board of the second 90° bend was missing. The two pieces of blade found washed ashore on Stevensons Island matched the missing section. The two pieces displayed evenly spaced chordwise dents on the lower surfaces. The dents started behind the leading-edge spar. The spacing of the dents matched the spacing of the screws on the windshield centre bow.
Tail boom and rotor
The direction of break was to the left. There was no internal damage to indicate that the tail rotor drive had continued to turn as the tail boom separated. The direction of twist of the tail rotor drive indicated that the drive from the transmission had stopped and the tail rotor had continued trying to rotate.