A skydive tandem pair crash-landed into a lake following a double parachute malfunction. The tandem rider’s lifejacket did not properly inflate, and the rider was lost in the lake, presumed deceased. Parachutists everywhere need to practice water landings, which are even riskier than you might think. TAIC recommends changes to aviation rules and incident reporting.
Executive summary Tuhinga whakarāpopoto


What happened
- On 10 January 2018, NZONE Skydive was conducting commercial tandem skydiving operations from its Queenstown site near Lake Wakatipu, when a tandem pair experienced a double parachute malfunction.
- The tandem pair was the last of nine tandem pairs to exit the aeroplane at 14,000 feet (about 4,300 metres) above the site. The droguefall stage was uneventful and the tandem master deployed the main parachute slightly higher than usual in order to reach the parachute landing area with ease.
- The main parachute did not open symmetrically and the lines twisted. After unsuccessful attempts to correct the line twist, the tandem master cut away the main parachute and deployed the reserve parachute. By this time the tandem pair had drifted further out over the lake.
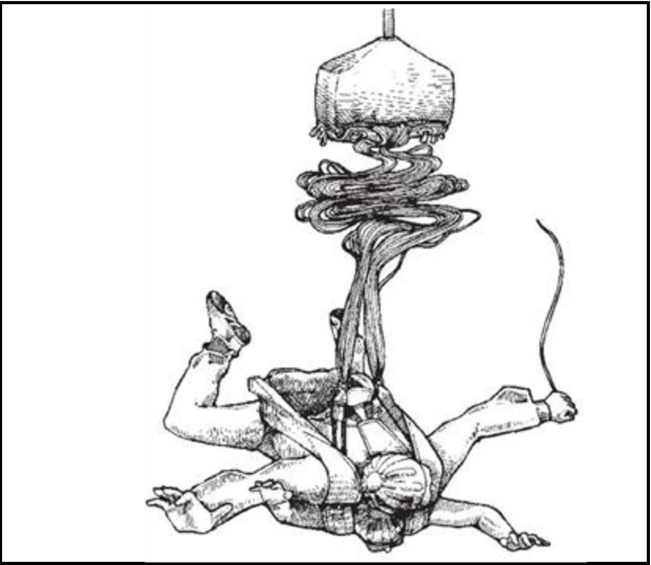
- The reserve parachute opened, but tension knots in the suspension lines prevented the canopy fully inflating, which distorted its shape. This caused the tandem pair to spin in a clockwise direction. The tandem master was unable to overcome the centrifugal forces generated by the fast spin rate, which prevented the tandem master making a safe recovery. The tandem rider donned their lifejacket for an impending water landing; however, the tandem master did not have a lifejacket. Just prior to impact, the tandem master took action to minimise the spin rate and the impact forces expected at the moment they struck the surface of the lake.
- After impact with the water, the tandem master was able to clear the lines entwined around both their legs and assist the tandem rider to partially inflate their lifejacket. Attempts to inflate the lifejacket further were unsuccessful. The tandem master was rescued after a short period of time, but the tandem rider was not found and remains lost in the lake.
Why it happened
- The Transport Accident Investigation Commission (Commission) found that the asymmetric opening of the main parachute canopy and subsequent line twist were likely due to the way the main parachute had been packed. The cause of the tension knot forming in the suspension lines of the reserve parachute could not be conclusively determined.
- The tandem rider’s lifejacket likely could not be inflated sufficiently to support their head above water. The reason for the lifejacket not inflating fully and its state of serviceability before it was used could not be conclusively determined. In addition, the tandem master was not equipped with a lifejacket, which decreased their ability to remain afloat.
- The Commission also found that the operator’s planned water emergency response did not have due regard to the minimum survival time for people immersed in cold water. This increased the likelihood of the water emergency response not providing timely assistance.
What we can learn
- The Commission considered several aspects of this accident to be safety issues that had the potential to affect other parachuting activities in New Zealand:
- maintenance programmes ensure that equipment is airworthy and able to perform its functions when required. The operator’s lack of a maintenance and inspection programme for lifejackets introduced a risk to the operation
- rules and operating procedures are put in place to ensure a basic level of operational safety is achieved. If this guidance is not well defined, organisations that are required to comply may not achieve consistent or desired outcomes. The Civil Aviation Rules did not clearly define the minimum safety requirements for tandem parachute descents being conducted near significant bodies of water. This resulted in inconsistencies between the parachuting entities guided by the Civil Aviation Rules such as parachute organisations and Part 115 parachute operations, and increased the risk to parachutists
- standards are in place for emergency equipment to ensure it meets a set of minimum requirements. The standards referenced in the Civil Aviation Rules for lifejackets did not consider the specific requirements for parachuting. There is a risk that products certified to these standards will not be suitable for parachuting conditions
- emergency response plans ensure that timely assistance can be provided in an emergency. These plans need to consider the likely environments in which emergencies will occur. In not adequately considering the minimum survival times for people immersed in cold water, there was a risk that any water emergency response by the operator would not be able to provide timely assistance
- effective safety management in the entire parachute sector relies on the assessment of occurrence data. Without key fields being recorded by the Civil Aviation Authority for parachute occurrences that include the equipment fitted to the parachutes, the effectiveness of this tool for safety management in the sector is reduced.
- Since this accident the operator has made several improvements to its policy and procedures regarding the safety issues identified. As such, no recommendations have been made to address those issues.
- The Commission made two recommendations to the Secretary for Transport and one to the Director of Civil Aviation:
- the Commission recommends that the Secretary for Transport review and revise Civil Aviation Rule Parts 105 (Parachuting Operating Rules), Part 115 (Adventure Aviation Certification and Operations) and Part 149 (Aviation Recreation Organisations Certification) for parachuting operations, in conjunction with the Part 149 organisations’ operating procedures and standards, to reduce the potentially adverse consequences of an unintended water landing
- the Commission recommends that the Secretary for Transport review and revise Civil Aviation Rule Parts 105, 115 and 149 for parachuting operations, in conjunction with the Part 149 organisations’ operating procedures and standards, to define flotation devices that are suitable for use by parachutists
- the Commission recommends that the Director of Civil Aviation review the parachute accident and incident reporting system under Civil Aviation Rules Part 12 (Accidents, Incidents, and Statistics) and Advisory Circular AC12-1 (Mandatory occurrence notification and information), in conjunction with the Part 115 parachute operations and Part 149 organisations’ requirements, to provide a more effective national resource to manage the sector’s safety.
- The key lesson identified from the inquiry was that if a parachute operation is based near a significant body of water, the operator needs to consider and mitigate the additional risks presented by a parachutist unintentionally landing in the water.
- All parachutists would benefit from gaining practical or simulated experiences of a water landing before being issued with their initial parachutists’ certificates.
- All parachute-sector participants may benefit from continued engagement with each other to improve industry guidance and the safety of parachuting in New Zealand
Who may benefit
- Parachutists, tandem riders, operators, parachute organisations and the New Zealand adventure tourism industry will benefit from this report.
Factual information Pārongo pono
Narrative
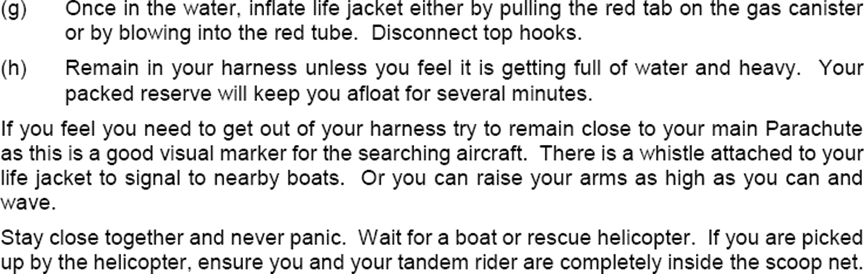
- On 10 January 2018, NZONE Skydive (the operator) was conducting commercial tandem skydiving operations from its Queenstown site at Jardines aerodrome (the aerodrome). The aerodrome is located about seven kilometres south of Queenstown Airport near Lake Wakatipu (the lake).
- The parachute-drop aeroplane, registered ZK-KPH (the aeroplane), departed at 1316 (times are in New Zealand daylight time (co-ordinated universal time + 13 hours) and expressed in the 24-hour format). On board was one pilot (the pilot) and 18 passengers consisting of nine tandem pairs. Each tandem pair consisted of a tandem master and a tandem passenger (rider).
- The pilot climbed the aeroplane to 15,000 feet (4,600 metres [m]) altitude above mean sea level (note that all vertical distances in this report are referenced to sea level unless marked otherwise. Jardines aerodrome is approximately 1,000 feet (305 m) altitude above mean sea level. Parachutists work in heights above the ground level at the landing point, so the drop heights are referenced above ground level) to commence the jump run in a southerly direction above the parachute landing area (PLA) at the aerodrome. The accident pair was the last tandem pair to exit the aeroplane, at 1332.
- The tandem pair’s initial droguefall (the portion of a tandem descent when a drogue has been deployed. It occurs between the initial freefall and the main parachute deployment. A drogue is a trailing ‘parachute-looking’ device used to create drag and regulate the fall rate of a tandem pair) descent was uneventful. At about 5,400 feet (1,600 m) above ground level (AGL), the tandem master deployed the main parachute, which opened fully but was facing approximately 120 degrees to the left of the tandem pair’s heading. This resulted in their spiralling, then their spinning anticlockwise below the canopy and the parachute lines twisting. The tandem master was unable to clear the line twist. At approximately 4,800 feet (1,500 m) AGL, the tandem master performed a ‘cutaway’ of the main parachute then deployed the reserve parachute at 1334.
- The right-hand side of the reserve parachute did not open properly, which caused the tandem pair to enter a clockwise spin (see Figure 3). The tandem master was unable to correct the problem, but was able to reduce the spin rate intermittently by pulling down on the left brake line to well beyond the normal control movement.

- Recognising that they were going to land in the lake, the tandem master instructed the rider to don their lifejacket (the term 'lifejacket' is used throughout this report. It is otherwise known as a personal flotation device or life preserver), which they did before contact with the water. The tandem master was not required by the operator to wear a lifejacket and did not carry one.
- The tandem pair was forced outwards by the centrifugal force of the spinning parachute, to lie right-side down at an angle of about 30 degrees to the lake surface. They struck the surface of the lake at 1336, approximately 800 m from the shoreline (see Figure 4) then sunk to a depth of about 1 m before resurfacing. The canopy and suspension lines collapsed above them.
- The tandem master unclipped the rider's harness, and instructed the rider to inflate their lifejacket by pulling the red handle. The lifejacket did not inflate so the tandem master attempted to inflate it manually with the mouthpiece, but was also unsuccessful.
- The tandem master was still attached to the reserve parachute, and the suspension lines were tangled around both the rider's and the tandem master's legs. The tandem master dived and used the hook knife from the tandem rider's harness to cut lines and free the rider's legs. The tandem master dived several more times to clear tangled lines and remove the parachute harness.
- After about four minutes the tandem master lost sight of the tandem rider. The crew of a small boat rescued the tandem master about 13 minutes after their impact with the water. The tandem master was in a semi-conscious state and the rider was not found. The rescuers transferred the tandem master to shore where emergency services applied first aid before a rescue helicopter flew the tandem master to hospital.
Search and rescue
- Ground safety observers at the PLA raised the alarm after observing the reserve parachute deploying. When they realised that the tandem master was unable to control the reserve parachute and that it was descending over the lake, the operator activated its water rescue plan.
- The first stage of that plan was to confirm that the tandem pair was going to land in the lake. The radio operator contacted the pilot of the skydive aeroplane to advise that a tandem pair had deployed their reserve parachute and were likely to land in the lake. The pilot diverted the aeroplane to search for the tandem pair. The pilot observed the reserve parachute and tandem pair in the water and transmitted a ‘PAN-PAN’ (the international-standard urgency signal that someone aboard a boat, ship, aircraft or other vehicle uses to declare they have an urgent situation) radio call to Queenstown air traffic control. The pilot requested that Queenstown air traffic control contact the harbourmaster for immediate assistance.
- The harbourmaster dispatched the Coastguard Queenstown boat and requested assistance from other boat operators.
- By chance, a helicopter pilot working nearby at Cecil Peak Station, across the lake from the operator’s base, heard the PAN-PAN call and offered to assist. The helicopter pilot transported the Cecil Peak Station manager to where a boat was moored, then flew to the parachute and hovered above to mark that location.
- The Cecil Peak Station manager launched the boat and reached the parachute at 1349. After retrieving the tandem master from the water, they continued to search for the rider. At 1405 the tandem master was transferred to another boat and taken ashore, then to hospital by rescue helicopter.
- The operator conducted an aerial search for the rider, then at about 1430 Coastguard Queenstown arrived and took control of the marine search. The search was called off at 1642. An underwater search by New Zealand Police a few days later was unable to find the tandem rider; they remain lost.
Injuries to persons
- The tandem master reported that the tandem rider survived the impact with water, remained conscious and was able to speak with the tandem master. The extent of the rider's injuries from the initial impact remains unknown.
- The tandem master received bruising from the initial impact. Prior to being rescued the tandem master ingested a significant amount of water and was semi-conscious and cold. After being recovered from the lake to the shore, the tandem master was observed to be in a foetal position and shivering uncontrollably. Ambulance officers applied first aid before the tandem master was taken to hospital by helicopter. The tandem master was discharged from hospital the following day.
Survival aspects
- The water temperature was approximately 10º Celsius and the surface was calm with a five-knot southerly wind. By 1500 the wind had increased to about 12 knots and the surface was choppy with white caps.
- During the descent under the spinning reserve parachute, the rider verbally confirmed to the tandem master that the rider could swim. The tandem master had significant swimming experience, including through parachuting into water and scuba diving, and as a lifeguard.
- The operator’s water rescue plan relied on a response from the harbourmaster and the coastguard in Queenstown. The Cecil Peak Station manager and crew arrived first on the scene in their boat, about 13 minutes after the tandem pair entered the water. The first of the planned responders arrived from Queenstown about 30 minutes after the tandem pair struck the water.
Equipment
Parachute assembly
- The parachute assembly was identified by the operator’s numbering system as rig C46 and by the Civil Aviation Authority of New Zealand (CAA) registration system as 31Z. The parachute assembly was a combination of components that broadly consisted of three main items (see Appendix 2 and the Sigma Tandem manual (UPT Vector, 2019) for more details of the components):
- the container – complete with harnesses, the main drogue chute, the reserve pilot chute, control handles and the automatic activation device (AAD)
- the reserve parachute – complete with lines
- the main parachute – complete with lines.
- The components had initially been packed into the parachute assembly on 6 October 2017. Since then the parachute assembly had been used for 341 jumps.
- The operator’s parachute technicians inspected each tandem parachute assembly and repacked the main parachutes on a monthly cycle. The parachutes were usually collected for these inspections while they were unpacked, immediately after use, then placed back into service after the inspections had been completed. The previous monthly inspections for the accident parachute assembly had been on 7 December 2017 and again on 8 January 2018.
Main parachute
- The main parachute was an Icarus Tandem, manufactured in New Zealand in 2017 by NZ Aerosports Limited. The canopy was a mildly elliptical, nine-cell, ram-air style made with a zero-porosity fabric with a surface area of 300 square feet (sqft) (28 square metres [m2]). It had HMA (High Modulus Aramid, also known as Technora; a very strong, small-diameter line) 1200, black suspension lines and a maximum rated load of 227 kilograms (kg).
- The main parachute had last been inspected and repacked as described above on 8 January 2018. On the day of the accident the parachute assembly had been used four times and the main parachute repacked three times.
Reserve parachute
- The reserve parachute was a model VTC-1, manufactured in the United States of America (USA) for Uninsured United Parachute Technologies, LLC (UPT). It had been manufactured under contract to UPT by Performance Designs, Inc in May 2017 in accordance with the Federal Aviation Administration (FAA) Technical Standard Order (TSO) C23b (FAA TSO C23b). The Performance Designs model was a Vector Tandem II.
- The canopy was a square-wing, nine-cell, ram-air design made with F111 ripstop woven fabric. It had three centre cells without crossports and open stabilisers connected to the outer line attachment points. It was fitted with Dacron15 continuous (non-cascaded)16 lines. The parachute size was 360 sqft (33 m2) and it had a maximum rated load of 227 kg.
- The reserve parachute was just over six months old. It had initially been assembled and packed into the parachute assembly on 6 October 2017 by the operator’s parachute technician. The next inspection and repack as required by the Civil Aviation Rules (Civil Aviation Rules Part 105.51) was not due until May 2018. The reserve parachute had never been deployed.
Container
- The container and harness system was a Micro Sigma, manufactured in the USA by UPT, also in accordance with FAA TSO C23b.
- The harness was attached to the tandem master, and the tandem rider wore a separate passenger harness (see details of the harness and container in Appendix 2). The tandem rider’s harness was attached to the tandem master’s harness at four attachment points. A hook knife to cut lines in an emergency was stowed in a pouch on the rear of the tandem rider’s harness for easy access by the tandem master.
Lifejacket
- The lifejacket used by the rider was a Switlik model AV-200 (see Figure 5) that had originally been designed for commercial aircraft passengers and manufactured to FAA TSO C13F. This lifejacket was modified by Air Safety Solutions Pty Ltd (Australia) specifically for use by parachutists in Australia under the authority of the Australian Civil Aviation Safety Authority Technical Standard Order ATSO-1C13, and in accordance with Australian Parachute Federation (APF) equipment standard APF071206-I.

- The modification removed a whistle and light and changed the container from a sealed plastic bag to a waist-mounted zipped bag. This enabled the lifejacket to be fitted on the front of the tandem rider with a belt.
- The lifejacket had a single inflatable cell that was inflated by pulling a red handle attached to a mini-inflator. The action of pulling on the handle normally pierced the membrane of a small, compressed-gas cylinder that was screwed to the mini-inflator. The compressed gas then vented into the lifejacket cell. A separate red mouthpiece was provided for additional manual inflation.
Equipment inspection
- A detailed inspection was carried out of the parachute assembly and the following were noted:
- the reserve static line remained attached to the right main harness. It could be disconnected by the tandem master to allow the main canopy to be cut away without deploying the reserve parachute. This is a required action for some malfunctions where there is a risk of a reserve parachute becoming entangled with a rejected main parachute
- the AAD had not activated. It would only have activated if the tandem pair’s descent rate and heights had met the trigger threshold set in the AAD (see 2.45)
- the loaded rib wall in the reserve canopy between Cell 9 and Cell 7 (the two outer left-hand cells) and the non-loaded rib wall in Cell 9 had ripped apart. These ribs each had two crossports to equalise the cell pressure and help inflate the canopy from the central cells towards the outer edges. The ribs had ripped through almost the full chord length of the rib at the weakest point, across the centre of the two crossports
- eleven reserve parachute suspension lines (see Appendix 2, Line Trim Chart) had been cut: Cell 1 left-hand side – B1; Cell 1 right-hand side – A1 and B1; Cell 2 – A2 and B2; Cell 3 – B2 and C2; Cell 4 – A3 and B3; Cell 6 – A4; and Cell 8 – A5
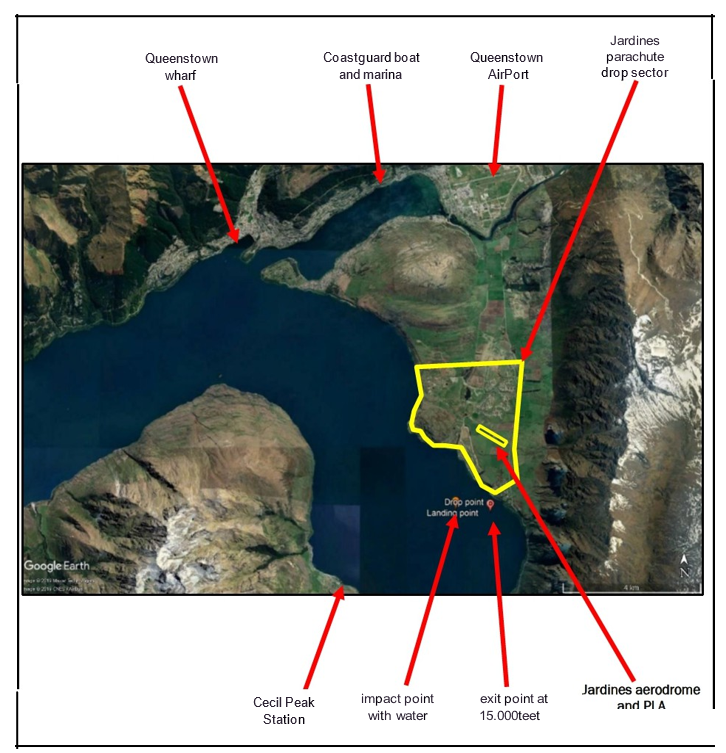
- two reserve parachute suspension lines to the two outer right-hand cells had permanent compression marks in three localised spots (line D4 to Cell 6 and line C5 to Cell 8, shown in Figure 6). The suspension lines were new and the fibre weave was loose from not having been under tension before, so the localised compression marks were visually different from the rest of the suspension lines. No other lines had similar marks. These compression marks were consistent with the pressure that could be exerted by a tension knot. These lines connected to the rear right-hand side of the canopy and passed through the same eyelet in the slider (see Figure 7)
- two areas of damage to the reserve canopy were consistent with post-accident damage when it was recovered onto a boat. The top surfaces of the left-hand outer cells (Cells 7 and 9) had two rips and the right-hand cells were stained with diesel fuel
- the main canopy showed signs of use but no damage.

Tandem parachute descent
- In an uneventful tandem parachute descent, after exiting an aeroplane the tandem master deploys the drogue chute to reduce the descent rate. Prior to 5,000 feet (1,500 m) AGL, the drogue chute is released using the drogue release knob. This opens the parachute container and withdraws the main parachute in its deployment bag to unpack the lines (see Figure 7 and Appendix 2). When the lines are extended, the deployment bag is withdrawn from around the packed canopy. The canopy inflates from the centre outwards. The slider controls the rate of inflation, and in doing so reduces the opening shock loads on the tandem pair. The slider slides down the lines as the canopy is inflated, to sit above the risers.
- When the main canopy opens, the tandem pair normally transitions from a horizontal to an upright position. Under normal conditions the parachute opens and the tandem pair continues to descend at a gentle rate. The forward airspeed and direction are controlled by the tandem master until landing.
Parachute opening problems and malfunctions
- Parachutes will often open correctly, but parachutists may experience opening problems. Parachutists are trained to check for problems when their parachutes open and take immediate action to resolve them. Two common types of opening problems are line twists and tension knots.
- A line twist occurs when suspension lines attaching a parachute harness to a canopy become twisted. Recovery techniques usually involve the parachutist kicking in the opposite direction, pulling the risers apart or using the forward air speed to assist with untwisting the lines, or a combination of the three.
- A tension knot occurs when one or more of the suspension lines form a loop that catches and develops into a knot as the line tension increases when the canopy inflates. The tension knot effectively shortens all lines caught up in it and can deform the canopy. Recovery techniques involve temporarily removing the tension from the line. One method of doing this involves pulling down on the knotted lines to shorten them and distort the canopy, then releasing them. As they relax, the tension grip in the knot is released and the canopy inflates fully.
- If an opening problem is unable to be corrected, it becomes a malfunction and the parachutist initiates the emergency procedure to open the reserve parachute. A tandem master can cut away the main parachute by pulling the cutaway handle on the right main riser. This releases both the right and the left main parachute risers and allows the tandem pair to fall away from the rejected main canopy.
- A reserve static line connected to the departing right main parachute riser then releases the reserve pilot chute, which deploys the reserve parachute. This reserve static line can be manually disabled at the right riser if the parachutist needs to separate from the main canopy and deploy the reserve parachute manually later.
- Two other devices are connected to the reserve static line. The first is a backup device called a ‘Collins Lanyard’. This device ensures that the left main parachute riser is also released with the right riser. The second device is a ‘Skyhook’. A lanyard is connected from the reserve static line to a Skyhook on the bridle of the reserve pilot chute. The Skyhook’s purpose is to use the rejected main canopy to withdraw the reserve parachute more quickly than the pilot chute would normally do. If the reserve pilot chute has already deployed, the Skyhook releases the connection with the discarded main canopy and allows the pilot chute to continue to deploy the reserve parachute.
- The reserve parachute is packed into the same container as the main parachute but is located in its own compartment. Because of its safety-critical function it is packed by a parachute technician and inspected, checked and repacked every seven months (as required by Civil Aviation Rules Part 105.51). Reserve parachutes are designed to deploy rapidly and open under harsher conditions than main parachutes do.
- The reserve parachute may also be deployed automatically by the AAD if the AAD detects that the tandem pair is below a pre-set safety height and descending faster than normal at that height. This may happen, for example, if the tandem master is incapacitated or unable to open the parachute normally.
Personnel information
- The tandem master had commenced parachute training in Canada. After qualifying, the tandem master had conducted commercial tandem parachute descents in Canada and Fiji before arriving in New Zealand in October 2017.
- The tandem master's overseas ratings were not initially accepted in New Zealand. After confirming that the tandem master met the required standard of proficiency, the New Zealand Parachute Industry Association (NZPIA) had issued the tandem master with a Commercial Parachutist Certificate on 14 October 2017.
- The tandem master held ratings for other parachute systems, and had undertaken a full conversion-training course for the Micro Sigma system with the operator in 2017.
- At the time of the accident the tandem master had conducted approximately 4,000 parachute descents, including 2,500 as a tandem master. Their New Zealand experience with the operator had included approximately 550 tandem jumps, with 206 of those being in the previous three weeks.
- The tandem master recalled experiencing roughly six main canopy cutaways and reserve parachute deployments during their career, but none with the Micro Sigma rig.
- The tandem master’s ratings, qualifications and medical certificate were current and appropriate for conducting tandem parachute operations.
- The tandem master had completed and passed pre-employment drug and alcohol testing. The operator did not conduct a post-incident test on this tandem master, although it was standard procedure. Post-incident testing would have been a urine or breath test, but as the tandem master was treated by paramedics at the edge of the lake then hospitalised, the operator did not conduct these tests. A urine test was conducted three days later with negative (clear) results.
Organisational and management information
- The operator had recently purchased the tandem skydiving operation, which had operations at Queenstown, Wanaka and Glenorchy. The operator was in the process of amalgamating the three operations into one organisation. A change to a standard jump aircraft and tandem parachute rig was part of that process. The parent company was an Australian skydive operator with several operations in Australia.\
- The operator was certificated under Civil Aviation Rules Part 115 (Adventure Aviation – Certification and Operations) as an Adventure Aviation Operation, and had nominated the NZPIA as its Part 149 parachute organisation (the term used in this report to describe organisations that have Aviation Recreation Organisations Certification issued in accordance with Civil Aviation Rules Part 149).
Meteorological information
- According to the weather condition report for Queenstown Airport at the time of the accident:
- the surface wind was 10 knots from the south
- the wind at 2,000 feet (610 m) was five knots and variable in direction
- there was a broken layer of cloud at 5,000 feet (1,500 m)
- the visibility was 40 kilometres
- the temperature was 18º Celsius
- the dew point was 12º Celsius.
- The wind at the drop height of 15,000 feet (4,600 m) was approximately 15 knots from the southwest, and at about the parachute opening height of 5,000 feet (1,500 m) AGL it was approximately five knots from the northwest.
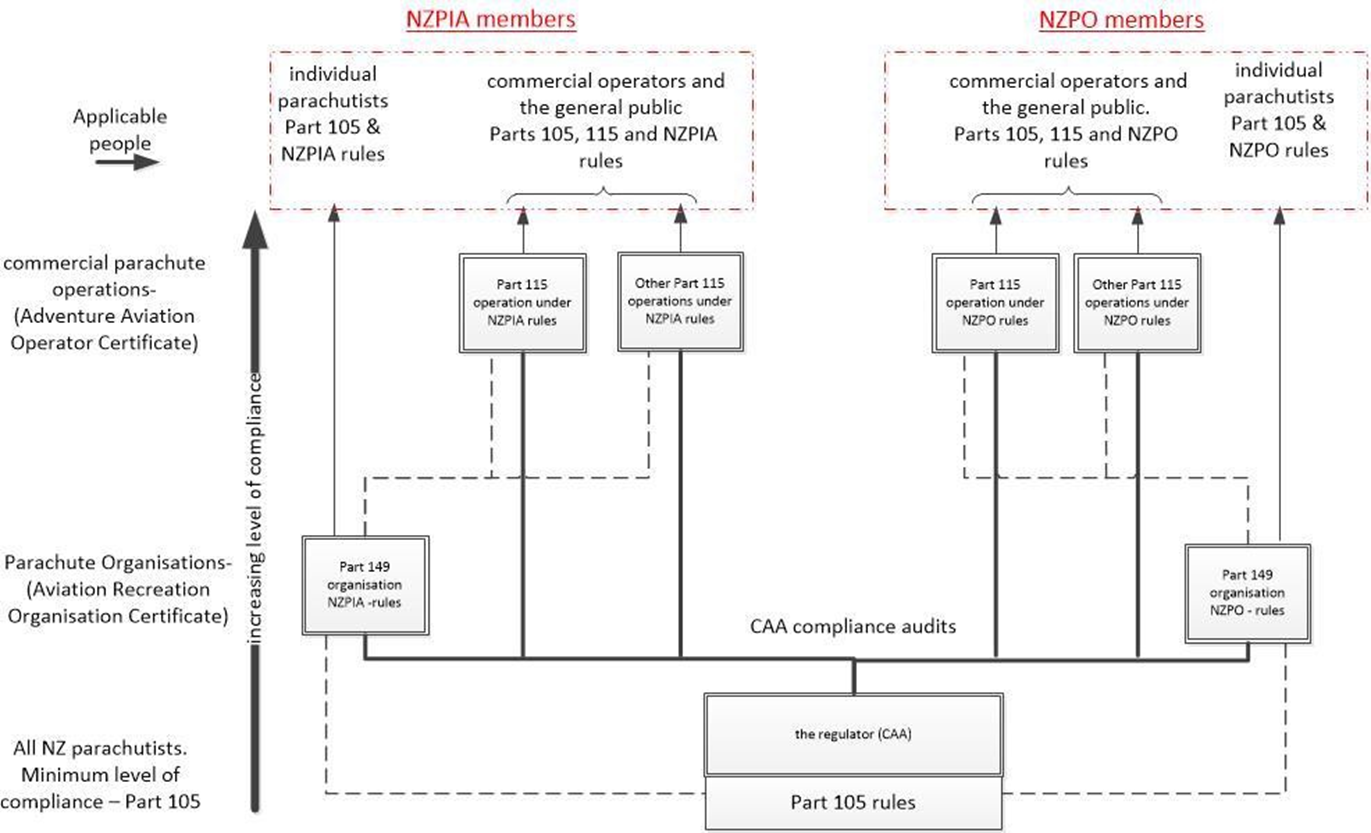
Regulatory structure
- The CAA set the organisation structure for the rules to conduct skydiving operations (see Appendix 1). There are several references to common Civil Aviation Rules parts, but only three principal parts govern these operations:
- Part 105 – Parachuting Operating Rules
- Part 149 – Aviation Recreation Organisations Certification
- Part 115 – Adventure Aviation – Certification and Operations.
Part 105 – Parachuting – Operating Rules
- An individual parachutist must meet the minimum requirements to participate in the activity as defined in Civil Aviation Rules Part 105, and must also belong to a ‘parachute organisation’ that has an ‘Aviation Recreation Organisation Certificate’ issued in accordance with Part 149.
Part 149 – Aviation Recreation Organisations – Certification
- A parachute organisation sets the minimum standards for equipment, operations and competency for all parachute activities that its members conduct.
- In accordance with Civil Aviation Rules Part 149, parachute organisations are delegated by the Director of Civil Aviation to assess or review the competency of individuals for the issue and renewal of certificates authorising those individuals to carry out specific functions within the sector, for example commercial parachutist certificate, tandem master and parachute technician. They can also have their own operating procedures and standards in addition to the minimum requirements of Civil Aviation Rule Part 105.
- Currently two parachute organisations exist in New Zealand, but the Civil Aviation Rules allow others to be approved. The two in operation at the time of the accident were the NZPIA and the New Zealand Parachute Organisation (NZPO).
Part 115 – Adventure Aviation – Certification and Operations
- A Civil Aviation Rule Part 115 parachute operation is set up specifically to conduct commercial tandem-parachute operations. The operator must become a certificated ‘Adventure Aviation Operation’ and obtain an operating certificate issued in accordance with Part 115. They must also have their own operating and maintenance procedures, which must embody the conditions in Civil Aviation Rule Part 105 and the rules of the Part 149 organisation to which they subscribe.
Recorded data
- The tandem master had a dual GoPro camera mounted on their left wrist, which was for commercial purposes. One camera was set to record video at 50 frames per second with audio and the other still photographs at one per second. The tandem master restarted both cameras while still in the skydive aeroplane and they recorded the complete parachute descent. Both cameras were recovered and the media files downloaded. Due to a missing memory card cover, the GoPro video camera stopped recording soon after impact with the water. The still camera remained watertight and kept operating until the rescuers turned it off.
- The tandem master wore a separate wrist-mounted electronic altimeter. This device recorded up to 10 minutes of the last jump data with timing, vertical speed and altitude. It also recorded an electronic log book of the past 200 jumps with data on the date and time, a jump number with exit height, freefall time, main canopy deployment height and under-canopy time. The device did not have a facility to download data to an external system, but a video record was made of the last jump replay, and the recent jump data was manually recorded.
- The tandem master had an audible altitude-alerting altimeter fitted in the lining of their helmet. This altimeter had alerts set at 6,500 feet, 5,500 feet and 4,500 feet (2,000, 1,700 and 1,400 m) AGL.
- The AAD continuously monitored the height above the ground and the descent rate. It was set to record when the descent speed exceeded 115 feet (35 m) per second and to stop 24 seconds after the descent speed dropped below that threshold. The saved record also included the seven seconds before the start point. Multiple records or an extended record could be created during a single parachute drop if the descent speed exceeded the AAD threshold again after the main canopy had been cut away.
- The AAD was sent to the New Zealand agent for data download. Three jump records were recovered from the accident flight (jump record numbers 343, 344 and 345). An analysis of these records showed that the first of the three jump records (number 343) accurately matched the descent to when the main parachute opened and continued for 24 seconds (see Appendix 3).
- The recorded data from the last two records indicated a parachute descent that would have been physically impossible. Record 344 showed the tandem pair climbing at more than 300 feet (91 m) per second and descending to 1,200 feet (366 m) below ground. The last record, number 345, showed the tandem pair climbing and descending between 1,000 and 2,000 feet (305 and 610 m) below ground at speeds of up to 200 feet (61 m) per second in both directions. The last two records were considered by the manufacturer to be erroneous data likely due to the crash impact and the AAD being submerged in the lake.
- The aeroplane was monitored by secondary radar and tracked in controlled airspace by a Queenstown air traffic controller. Electronic records of the aircraft track and radio and telephone communications with the tower controller were obtained from Airways New Zealand.
Tests and research
- All the recovered equipment was initially inspected in Queenstown by the Transport Accident Investigation Commission (Commission) investigators with the assistance of the NZPIA safety director. A further inspection was carried out by the CAA and the operator’s parachute technician, under the supervision of the Commission investigators.
- A detailed inspection of all the equipment was later conducted at the Commission’s technical facility.
- An experienced tandem master and parachute technician, independent of the operator, was engaged to assist the Commission in inspecting and analysing the evidence.
Analysis Tātaritanga
Introduction
- Parachuting is an adventure activity that is known to carry an inherent level of risk. During a tandem-parachuting operation in Queenstown, the tandem master experienced a double malfunction with the main and reserve parachutes that resulted in the tandem pair descending uncontrollably and striking the water. The tandem master was rescued but in a hypothermic state. The tandem rider was not found.
- Available data shows that this double malfunction was a rare event. The APF did not have a specific category to record double malfunctions because they were so rare. The APF’s Australian incident data for the five years from 2013 to 2017 showed that an average of 165,000 tandem jumps were performed per year. During that five-year period, the rate of malfunctions that required deployment of the reserve parachute averaged at one per 1,500 tandem jumps (APF, 2017).
- APF data provided to the Commission showed that in the 12 years up to and including 2017, 112 reserve parachute activations used the same reserve parachute as used in this accident. Nineteen of those reserve parachute activations had minor opening problems, but six of those opening problems could not be cleared and the incidents were subsequently classified as double malfunctions. No fatalities occurred in this data set.
- New Zealand data from the CAA did not record sufficient detail to determine if a reserve parachute was deployed during a malfunction, and it did not identify the type of reserve parachute. CAA data in the five-year period 2013-2017 showed an average of 78,000 tandem jumps per year with 41 malfunctions per year. That equates to about one malfunction per 1,900 tandem jumps.
- The CAA did not record if a parachute landing was into water. The operator stated that this was its first double malfunction and its first unintended water landing.
- The tandem master continued to support the rider in the water. The video and still image records show that the tandem master’s skill and training assisted the tandem pair’s chances of survival. The tandem master remained calm during this accident and kept talking to the tandem rider.
- This analysis describes what happened during the accident and identifies the factors that contributed to each of the malfunctions. It also discusses other safety factors that did not contribute directly to the outcome but increased risk.
What happened
Main parachute malfunction
- The recorded data showed that the tandem master opened the main parachute at about 5,400 feet (1,600 m) AGL. The tandem master’s video recording showed that they were in a stable attitude but the load came on to the right risers first. This was likely due to the canopy opening on the right side slightly before the left side, causing it to turn in a left-hand direction while it continued to inflate. A consequence of the canopy turning was that it created a right-hand line twist. The video recording then showed the parachute canopy had opened fully and was flying straight but to the south, away from the PLA.
- A further consequence of the canopy not opening in line with the tandem pair was that it caused them to spiral around to their left. The spiralling movement initially unravelled the right-hand line twist, but the tandem pair’s momentum continued the rotation. As the radius of the spiral decreased, the spin speed increased to one revolution per second, and this resulted in a severe left-hand line twist.
- After a few spins towards the left, the lines and risers twisted. The main parachute was fully inflated but un-steerable because the brake toggles were locked in the twisted risers and the parachute was flying further over the lake.
- The tandem master was able to reduce the number of twists by kicking in the opposite direction, but after 34 seconds under the main canopy the tandem master cut it away at about 4,800 feet (1,500 m). This would have likely been enough height for the tandem pair to reach the PLA on the reserve canopy.
- A line twist is regarded within the sector as a routine opening problem that can be corrected. After attempts to correct it have been exhausted, it becomes a malfunction, which then initiates the parachutist’s emergency procedures to open the reserve parachute.
Camera operation
- Typical parachuting industry procedures require tandem masters to assess any opening problems immediately and then decide if emergency actions are required. The operator’s standard operating procedures re-emphasised this process in its instructions to tandem masters for when they were using wrist-mounted cameras.
- The tandem master in this accident waited for about 15 seconds while observing the line twist and before taking action with both arms. The tandem master stated that, in this instance, it was preferable to wait until the line twisting slowed before taking action with both arms to avoid getting their arms trapped in the twisting risers. The tandem master stated that they were also shifting their weight in the harness (not captured in the video) to counteract the spin. The tandem master continued to hold their left arm out and record video on their wrist-mounted cameras during this period.
- In another of the operator’s video records from a previous cutaway in 2017, a tandem master continued to hold their arm out and record video using their wrist-mounted camera before taking action with both arms. That incident involved the same type of parachute rig but different people. These two similar videos raised the possibility of a systemic training issue with wrist-mounted cameras.
- After this accident, the operator took action on this concern of a potential training issue. It revised the tandem-master training relating to the use of wrist-mounted cameras. The desired result was to ensure that tandem masters focused on resolving any emergency over and above obtaining video records of tandem riders’ experiences.
Reserve parachute malfunction
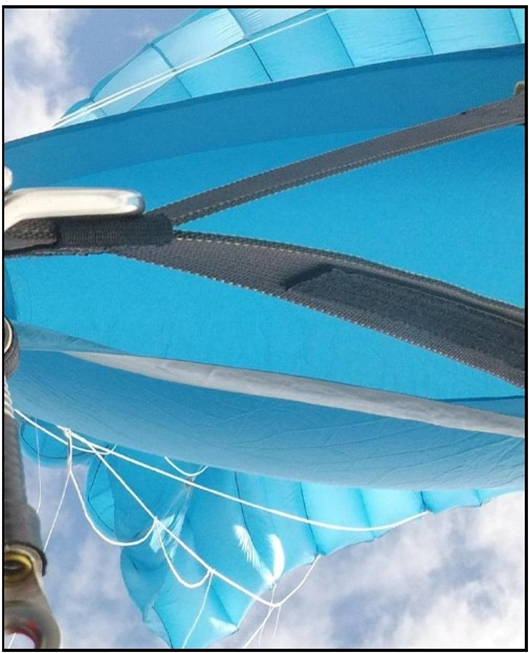
- The tandem master followed a standard emergency procedure that included pulling the main cutaway handle, immediately followed by pulling the reserve parachute ripcord handle. The reserve canopy opened within one second of activation, but it was deformed. Figure 8 shows the right side of the reserve canopy with the risers and slider in the foreground. The canopy leading edge (may also be referred to as the nose) is at the top and the tail at the bottom. A knot hidden from view behind the slider has prevented several suspension lines extending to their full length.
- The reserve parachute immediately entered into a steep spin to the right. The video recording showed that the right-hand-side brake lines near the canopy tail were loose and flapping in the airflow. The tandem master reported seeing two tension knots in the lines either side of the brake cascade knot.
- The video showed the reserve parachute was spinning at about one-third of a revolution per second for the 136-second duration of the descent under the reserve canopy. The tandem pair was subject to high centrifugal forces in the spin and the tandem master was concerned about losing consciousness. These forces prevented the tandem master climbing up a riser to attempt to clear the tension knot while supporting their and the tandem rider's weights.
- The tandem master decided to minimise the spin rate after being unable to clear the tension knot. After three or four spins, the tandem master would pull down the left brake line much further than normal to slow the spin rate and stall the left-hand side, then release it. This cycle continued with the last pull and release timed to reduce the speed of impact with the surface of the lake.
- The tandem master instructed the rider to open the lifejacket container and place the lifejacket over the rider’s head. This action was completed by approximately 2,000 feet (610 m) above the lake. The operator’s normal procedure before a water landing was for the tandem master to disconnect both lower passenger harness connections. This would prepare them for separation immediately after landing. The tandem master was only able to disconnect the lower-right passenger harness connection before impact because their left arm was operating the left brake line.
Unintended water landing
- The tandem pair struck the water while spinning in an almost horizontal, right-side-down attitude. A conservative estimate of the combined vertical and rotational velocity just before impact was in the range of 50 to 70 kilometres per hour. The tandem master reduced this slightly by judicious use of the left brake line. They were submerged during the initial impact and the canopy and suspension lines came to rest on top of them. The following description is based on the tandem master’s account and supported by video and still images recovered from the tandem master’s wrist-mounted camera system.
- The tandem master recalled releasing the rider’s harness and pushing the rider towards the surface. The reserve parachute lines had become entwined around both the tandem master’s and the rider’s legs.
- While treading water, with the harness and reserve parachute still attached, the tandem master dived to clear the parachute lines from around the rider’s legs. The tandem master retrieved the hook knife from the rider’s harness then started to cut the lines from around the rider’s feet. The tandem master also recalled trying to remove the main harness and reserve parachute.
- The tandem rider could not inflate the lifejacket by pulling the red handle, so the tandem master tried but was also unable to inflate it. The tandem master then used the manual inflation pipe but could only partially inflate the lifejacket.
- The tandem master recalled diving again to remove the main harness completely and cut the remaining tangled lines from around their own legs.
- The tandem master lost sight of the rider after about four minutes in the water, then was rescued by a small boat after a total of about 13 minutes of treading water.
Why it happened
Main canopy malfunction
- A main canopy malfunction can principally be the result of equipment failure, a parachutist’s actions leading to an unstable opening, or packing problems. In the absence of any equipment failure being identified, the investigation considered the remaining two possibilities.
Unstable opening
- The operator had recently changed parachuting equipment (from the ‘Strong’ Dual Hawk tandem container system with the Hop 330 main canopy to the UPT Micro Sigma container system with Icarus 300 and 330 mains). Two key differences between the old and new equipment were with the drogue behaviour on the deployment of the main parachute and the lack of a pre-set brake setting in the new main parachute. As a result of these differences, the new equipment required tandem masters to use a new opening technique. If the old technique were used with the new equipment, there was a risk of an unstable opening, which could lead to a main canopy malfunction. Since changing to the new equipment the operator had noticed an increase in the rate of main canopy malfunctions.
- With the previous container system, the drop speed remained the same as the drogue was released to deploy the main parachute. However, the new container system collapsed the drogue chute, which briefly accelerated the tandem pair’s descent rate when the drogue was released.
- The previous and new main canopies performed similarly when fully inflated, but the previous canopy would open to fly at a lower speed with half-brake set, while the new main canopy would open and fly at maximum speed without brake.
- The combined effect of these two differences could accentuate any instability or asymmetric forces applied to the tandem pair and canopy during the opening sequence and lead to opening problems. The operator was aware of these differences and had trained all tandem masters on the correct techniques for the new equipment before they were allowed to take commercial passengers.
- An analysis of the video recording with the independent industry advisor (tandem master and parachute technician experienced on the Micro Sigma system and the Icarus main canopies. (Further details in 9.7)). showed the tandem pair was in a stabilised attitude at opening and facing the PLA. Although the video did not show all the tandem pair’s body movements, the background view and the risers being drawn out cleanly without a twist were good indicators of their stability.
- The video also showed that the right riser loaded up first and the tandem pair was swung onto their backs and around to their left towards the direction in which the main canopy was flying. This showed that the tandem pair’s attitude was unlikely to have contributed to the main canopy turning as it inflated.
Main parachute packing problems
- There are three possible packing issues that could induce a line twist: an uneven deployment bag, a line dump and an uneven canopy inflation. Of these three possibilities, the advisor was unable to determine which may have been most likely in this accident.
- Packers were trained, checked and generally supervised while they repacked main parachutes. The workload was shared between the packers on duty for the day.
- The main canopies were repacked in an open area with several parachutes being packed simultaneously, and the packers were under time pressure to meet operational demands for the day. On the day of the accident six packers were on duty and they each repacked one or two main parachutes after each plane load. They had repacked at least 13 main parachutes each by 1300 that day, which is considered to be a high but not an excessive workload.
- The operator’s packing records and incident reports were checked for any standout repeat incidents. The packing history of the packer who packed the accident parachute was also checked. No evidence was found in the operator’s records that could have suggested any link between the packers working that day and the main parachute opening with a line twist.
- The packer should have been tested for drug and alcohol immediately after the incident, in accordance with the operator’s procedures, but was not. The operator reported this was because the operator’s staff were engaged in the search and rescue operation. The packer had passed a test four weeks earlier.
- After this accident the operator engaged an independent parachute technician to check the reserve parachutes and the operator’s general packing process (see 3.61 for further detail). That parachute technician identified several potential improvements for the main parachute repacking process that the operator has since implemented. One of these related to line twists.
- Given the above evidence and the process of elimination, the advisor believed that the packing likely contributed to the asymmetrical main canopy inflation, leading to a line twist.
Reserve canopy malfunction
Tension-knot formation
- The permanent compression marks found in the two suspension lines in the reserve parachute were likely caused by a tension knot. The accident flight was the first in which the reserve parachute had been deployed. The two compressed sections of suspension line D4 to Cell 6 shown in Figure 6 were about 1,300 millimetres apart, which coincided with the length of one ‘S’ fold in the free bag’s line pouch. The other line that showed a similar compression was line C5 connected to Cell 8. Both lines passed through the same grommet in the rear right of the slider and were therefore likely to have been involved in the same tension knot.
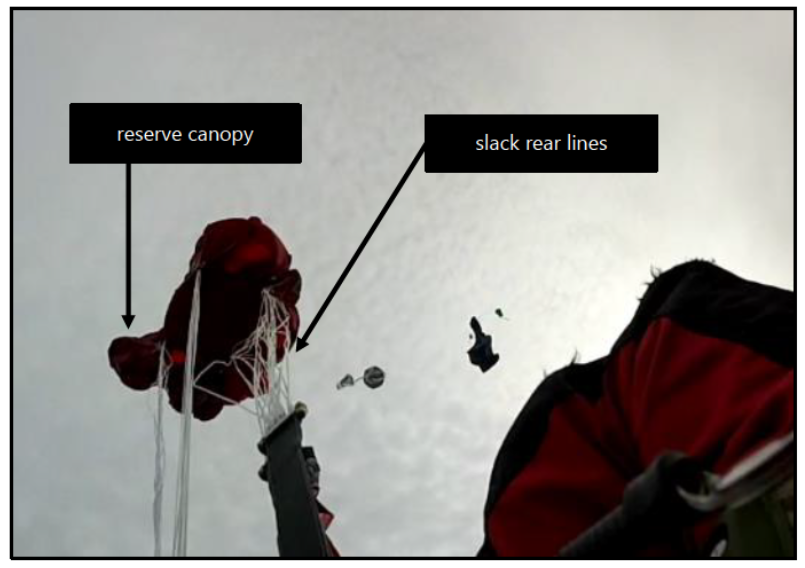
- A tension knot is unable to form without a slack loop of line. Therefore it is likely that a tension knot formed in the right-rear line group in lines D4 and CS as the lines unfurled from the free bag pouch, and that the knot passed through the slider grommet but remained knotted and caused the canopy distortion. The example in Figure 10 from another incident shows the reserve canopy starting to inflate with the shorter front line groups taut and the rear line groups still slack and affected by the disturbed airflow around the tandem pair.
- As with the main parachute malfunction, the Commission considered the contribution of equipment, the tandem pair's attitude at opening, and packing in the reserve parachute malfunction.
Parachute type
- The VTC-1 reserve parachute was designed to open safely in the worst situation for a tandem pair at terminal velocity and was manufactured in accordance with a historical standard (FAA TSO C23b) as an individual component of a parachute assembly. The standard came into effect in 1962 and was superseded in 1984, but equipment manufactured to that standard is still approved by the FAA for use today. The version (see page 2-4 of the Parachute Rigger Handbook (FAA, 2015) for the history of this TSO and the handbook's associated appendix for versions of the TSO) current in 2020 was TSO C23f, which called on a Parachute Industry Association technical standard PIA TS-135 for the performance standard. That performance standard covered the complete tandem reserve parachute assembly with components, rather than individual components as previously.
- The operator had preferred not to use the VTC-1 reserve parachutes in its new containers. The operator believed that the VTC-1 was a dated design and more susceptible to malfunctions than its proposed alternative reserve parachute. The operator’s concerns were based on three design aspects of the VTC-1 reserve parachute (see Figure 11):
- it used continuous lines, which increased the bulk of line material to be packed
- it used Dacron fibre for the lines. This resulted in a thicker line than other materials of the same loading, and the operator believed that Dacron lines tended to grip against other lines when packed together
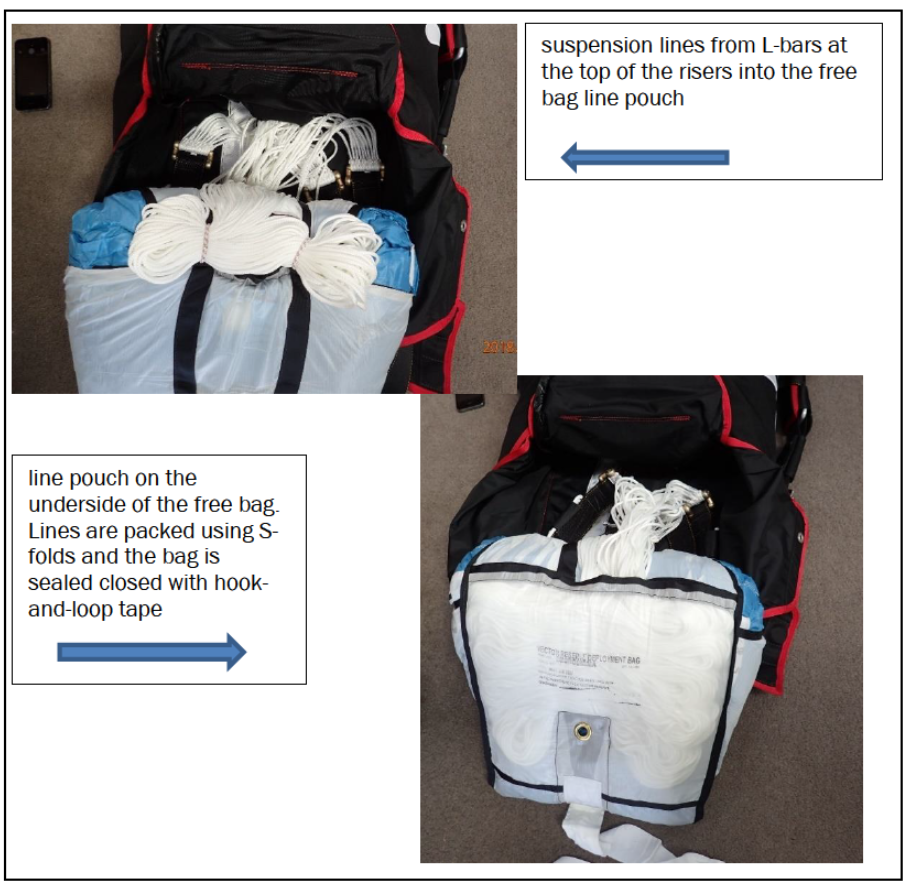
- the lines were packed into a free bag pouch that was then sealed closed with a hook-and-loop (often referred to by trade names such as ‘Velcro') sealing strip across the open end of the line pouch. The operator believed that when the lines were extracted during deployment, they were pulled through the line pouch’s sealing strip and could fray and catch other lines.
- The operator stated that it had experienced five malfunctions with the VTC-1 reserve parachute over several years at its Australian operations and that these had resulted in serious injuries. The Australian Civil Aviation Safety Authority had approved the operator’s request to use an alternative manufacturer’s reserve parachute in the Micro Sigma container for its operations in Australia. The operator stated that since the change, it had had 15 years of trouble-free use from its preferred alternative reserve parachute and wanted to use the same combination in New Zealand.
- In mid-2016 the operator asked the CAA flight operations inspector, who was in regular contact, about making a similar change to its New Zealand tandem parachute assemblies. Email exchanges and meetings on the subject continued between the CAA and the operator for a few months, but a pathway for that change was not clear to the operator. At the time of the accident these discussions had not progressed to a formal application by the operator to change the reserve parachute in its Micro Sigma tandem parachute assemblies or its Part 115 exposition.
- Civil Aviation Rule 105.51(b)(1) requires tandem reserve parachute assemblies to comply with the technical standards of a parachute organisation. In this case, NZPIA’s technical standard deferred such decisions on equipment compatibility between individually approved components (as is the case when approved to FAA TSO C23b) to a ‘parachute technician’ under NZPIA rule 19.2.2(4). Therefore, an operator could evaluate the compatibility of components in a parachute assembly using its own parachute technicians. Any change in components for the parachute assembly would then require formal approval from the CAA to revise the Part 115 operator’s exposition.
- The Commission sought accident data to provide a context for the operator’s claims of unreliability. Data was requested from the CAA to compare reserve parachute reliability levels in New Zealand. The CAA data records lacked the detail needed to extract performance information on this type of equipment.
- The Commission also sought the manufacturer’s opinion. UPT explained that the reserve parachute system had undergone substantial testing to achieve its TSO compliance status and that it had been designed to open safely carrying a tandem pair at maximum permissible weight falling at terminal velocity free-fall (no drogue chute). The primary reason for UPT selecting continuous Dacron lines was their performance under such extreme opening conditions and the distribution of shock loads across the canopy.
- UPT stated that the VTC-1 reserve parachute had been in service for more than 30 years with proven reliability. It compared the operator’s claim of five malfunctions with the VTC-1 reserve parachute with its own records and believed that five was considerably higher than anywhere else in the world. The Commission was not able to obtain data from USA or United Kingdom aviation regulators and parachuting organisations. The 'high number' of reserve parachute malfunctions in Australia could also have reflected the fact that Australia has a more extensive parachuting-occurrence database than other countries.
- UPT expressed concern with a generalised 'mix and match' approach to a parachute assembly. It stated that each major component of a parachute assembly, apart from the main canopy, was certified separately. UPT also stated that it had research and development test data for the VTC-1 reserve parachute and its compatibility and functionality within the entire Vector and Sigma tandem systems going back more than 30 years. UPT advised that where operators chose to mix parachute types in variance with the Micro Sigma system, operators would no longer have the benefit of that performance assurance unless they conducted their own testing.
- UPT also confirmed that in its opinion Dacron was the best line type for its reserve parachute. Based on its global experience in the parachute industry, it believed that the most common line type used on tandem main and sport main parachutes was Vectran, which it also believed was the line type most associated with tension knots.
- The Commission was unable to determine with any certainty if the VTC-1 reserve parachute was more susceptible to tension knots than any alternative tandem reserve parachute.
- UPT advised the Commission in January 2021 that it had been working on the design and testing of a new tandem reserve parachute since about 2012. It was released for sale in late 2020 as the Sigma-II Reserve 340. This new reserve parachute was designed to have less packed bulk and to fit into the smaller Micro Sigma container and free bag (the standard Sigma container is wider and deeper than the Micro Sigma container. The same VTC-1 reserve parachute is used in both containers, but it has to be packed slightly differently to fit into the smaller free bag in the Micro Sigma container). The lines are cascaded Vectran rather than Dacron and the reserve parachute meets the current TSO-C23f standard. UPT discontinued production of the VTC-1 (also known as the VR-360) from 8 December 2020.
Parachutists’ attitude at opening
- Reserve parachutes are designed to open reliably in unusual circumstances, but these circumstances were not unusual. The video record showed the tandem pair was suspended vertically and spinning when the tandem master cut away the main canopy. They were descending at sub-terminal speed and the extraction of the reserve canopy free bag from the parachute container was fast. It was assisted through the Skyhook connection to the rejected main canopy. The tandem master said that the reserve deployment was clean and symmetrical.
- The spinning attitude was more or less likely to have affected the lines as they unfurled, but there was no evidence to show that it led to the formation of a tension knot. The Commission was unable to determine with any certainty if the tandem pair’s attitude influenced the formation of the tension knots in the reserve parachute’s lines.
Packing technique for reserve parachutes
- The reserve parachute was one of a batch of 62 new parachute containers purchased by the operator. Two of its parachute technicians had assembled and packed all of them. These parachute technicians had trained in the USA as master riggers (equivalent to master parachute technician in New Zealand) but held different ratings in New Zealand and were both experienced with packing reserve parachutes, including the VTC-1 reserve.
- The Commission, the CAA and the operator randomly selected four, packed tandem parachute assemblies from the parachute racks to unpack and inspect. No packing errors or concerns with the packing techniques were found in this sample of parachute assemblies.
- The operator subsequently brought in another independent parachute technician from a competitor’s operation to review its packing operations and another sample of reserve parachutes. This technician noted that one reserve parachute was found with a 180-degree twist in the rear lines. That parachute technician considered that this twist was unlikely to cause a major problem but that it was not acceptable.
- As a result of this review, the operator made several improvements to its packing operations.
- The Commission contacted the manufacturer of the reserve parachute (UPT) to seek its opinion on the reserve malfunction. UPT could find no reason for the reserve parachute not opening fully. UPT agreed that the canopy distortion was in the right rear corner, but could not positively identify why this had occurred.
- UPT suggested that, although it believed that the reserve parachute had been packed correctly, small changes in packing technique could improve reliability. It stated, “Tension knots, like all parachute malfunctions, are not 100% preventable. A correctly built, correctly packed, correctly deployed parachute, main or reserve, can still malfunction. That is the nature of parachutes in general.” UPT offered several possible reasons for a packing technique to lead to a tension knot:
- an uneven or asymmetrical stowage of the reserve parachute lines within the free bag’s line pouch
- free bag line pouch hook-and-loop mating inconsistencies across the bag
- the placement of the reserve risers and the ‘fanning’ of the reserve risers in the reserve pack (a reserve parachute packed into its compartment in the parachute container) tray during the packing process
-
the placement of the ‘free’ reserve lines (outside the pouch) in the reserve pack tray from the reserve risers to the reserve free bag
-
the orientation of the reserve bag extraction based on tandem-pair body position during the reserve deployment. (The multi-axis separation forces between the free bag and the tandem pair will vary with the spin state of the main canopy being cut away.)
- After a reserve parachute has been deployed, it is not possible to ascertain how it was packed, apart from through its behaviour on opening. The Commission was unable to determine with any certainty if the way the reserve parachute was packed influenced the formation of the tension knots in the reserve parachute’s lines.
Lifejacket malfunction
Safety issue: The operator did not have a maintenance and inspection programme in place for its lifejackets to ensure they remained in a serviceable condition.
Safety issue: The operator expected the tandem master to have the reserve parachute pack for flotation and therefore did not require them to also wear a lifejacket.
- The operator had recognised that the Queenstown site posed a risk of unintentional parachute landings in the adjacent lake, and after taking ownership had taken steps to mitigate that risk. It had purchased modified lifejackets certified for use by parachutists in Australia and provided them to all tandem riders (see 2.32 to 2.33 for details on the modification). It had also conducted water survival training for tandem masters in late 2017 using the new Micro Sigma container. It also had a rescue plan in place for an unintended water landing.
- Although the modified lifejacket was a certified aviation product for parachutists in Australia, it was not certified in New Zealand. Additionally, the modification was not authorised by the original manufacturer and the lifejacket no longer conformed with the original manufacturer’s TSO for its intended use in passenger aircraft. The design compliance stamp stated that it still conformed with TSO C13f and remained on the front of the lifejacket. This was misleading, but otherwise the lifejacket was deemed fit by the APF for its new purpose in the parachuting sector.
- The APF equipment standard required that the lifejacket be uniquely identified and undergo a regular maintenance and inspection programme to ensure it remained serviceable. The New Zealand Civil Aviation Rules and NZPIA’s rules did not recognise or endorse the APF standard, nor did they have equivalent requirements for these lifejackets in New Zealand. Consequently, the CAA rules did not require the operator to have a maintenance and inspection programme for its lifejackets at the time of this accident.
- While the lifejackets were new, they were in unsealed, zippered pouches. The greater risk was for the end users. There was no external marking to indicate that the lifejackets were still in a serviceable state before being worn (much like the details a tandem master would check when conducting a parachute pre-flight check (see Civil Aviation Rules 105.109, which lists details for a pre-flight parachute check)). The operator has since implemented a maintenance and inspection programme to ensure that only serviceable lifejackets are made available for parachute descents.
- The tandem master had the option of wearing a lifejacket but neither the CAA rules nor the operator required them to do so. The operator had tested and proven that the reserve pack would assist a tandem master to remain afloat, while a tandem rider had their own lifejacket. If the tandem master chose to wear a lifejacket model used by tandem riders, in its packaged state it would fit between them. This situation could make it more difficult for a tandem master to extract and fit their lifejacket over their head before a water landing. In this accident, the tandem master deployed the reserve parachute and therefore the reserve pack was not able to provide flotation support.
- The reason for the lifejacket used on this parachute descent not fully inflating could not be conclusively determined and it has not been recovered. Possible reasons in sequential order of occurrence are: a manufacturing fault; an empty or loose gas bottle when either it was last packed and placed on a rack ready for use or, during the descent after being fitted on the tandem rider; damage upon impact with the water; and damage while in the water.

Minimum standards for operations near water
Safety issue: The CivilAviation Rules did not set minimum safety requirements for tandem parachuting operations to mitigate the risk of an unintended parachute landing in water.
Safety issue: The standards for lifejackets that the CAA referenced in Civil AviationRules were not directly applicable to or suitablefor skydive operations.
- The minimum safety equipment for parachute descents when there is a risk of an unintended water landing is prescribed in Civil Aviation Rules 105.57 (see Appendix 4). The rule lists only two specific situations where parachutists must wear 'flotation equipment'. These are when a jump into water is intentional and when the parachutist is a student and the jump is near water. The rule is silent on lifejackets for tandem masters, tandem riders and other qualified parachutists. (Note this report has standardised the term 'lifejacket'. In this section, other terms emphasised in single quotation marks are as used in the associated referenced documents.)
- Civil Aviation Rules Parts 105 and 149 do not set minimum levels of skill or training to ensure that qualified parachutists are prepared for unintended water landings. The two parachute organisations set additional requirements for parachutists to cover this aspect of risk, but the organisations' requirements differed.
- The NZPIA's procedures reflect the conditions of Civil Aviation Rules 105.57. Additionally, an NZPIA instructor must brief an NZPIA member on emergency water landings before that member can gain a parachute certificate. NZPIA instructors must complete simulated water-landing training. NZPO parachutists must also be briefed on water landings to gain A certificates, but there is no requirement for NZPO instructors to have experience in water landings. Neither parachute organisation requires its qualified parachutist members to have assessed skills in actual or simulated water landings. The NZPO requires tandem riders to wear lifejackets if exit or landing areas are near water, but the NZPIA just recommends that they wear lifejackets in these situations.
- Civil Aviation Rule Part 115 does not specifically require tandem parachute operators to consider the key safety factors in maximising parachutists’ chances of survival after unintended water landings, such as the likely survival times for parachutists in water and their rescue. However, Part 115 parachute operators do have a non-specific requirement under Civil Aviation Rules 115.209 and Part 100 (part 100 was in implementation phase and was not applicable to the operator at the time of this accident) to identify and manage associated risks to their operation. Part 100 would require operators to have safety management systems and to identify and manage all relevant hazards. This operator still had six months to submit its draft safety management system to the CAA for review. The CAA planned to apply the rule to the sector by February 2021.
- In comparison, the United States Parachute Association (USPA) requires all advanced parachutists (holders of USPA B licences) to complete water-landing training as a prerequisite to the issue of their licences. The USPA also considers the associated risks of unintended water landings and emphasises in its training that a parachutist’s survival after an unintended water landing depends on a means of flotation and effecting a successful rescue (Daniel, 2015).
- The Civil Aviation Rules reference several standards (Civil Aviation Rules Part 91, Appendix A14) for ‘life preservers’ that are approved for use in aircraft (the CAA Legal Information Bulletin No3 defines that a parachute is an aircraft). However, these standards correspond with ‘life preservers’ designed for use in aircraft and marine situations, and are not directly applicable for use in a parachuting situation where such devices could be hazardous to use.
- Lifejackets used in aircraft are usually stowed in the aircraft until required, but they are not suitable for attaching to parachute harnesses for use by parachutists. Such devices worn with parachute harnesses are also subject to harsher operating conditions than stowed devices. Similarly, not all ‘personal flotation devices’ made in compliance with New Zealand Standard 5823:2005 (specification for Buoyancy Aids and Marine Safety Harnesses and Lines) would be suitable for use in parachuting operations. For example, Maritime New Zealand Rules 91.4-Personal flotation devices require personal flotation devices to be worn for commercial marine operations. The associated Maritime New Zealand Advisory Circular AC91-2 lists multiple specialist personal flotation device types that substantially comply with the New Zealand Standard 5823 for specific water activities.
- Civil Aviation Rule Part 105 requires all parachutists to comply with the technical standards of a Part 149 parachute organisation. Part 105 specifically refers only to technical standards for parachute equipment and does not mention lifejackets. Consequently, neither of the New Zealand parachute organisations has technical standards for suitable lifejackets or associated requirements to ensure such lifejackets remain in a serviceable state.
- The NZPIA has since reissued its rules and operating procedures to provide more clarity on equipment maintenance and water landings.
Survivability
Safety issue: The operator’s planned water emergency response did not have due regard to the minimum survival time for people immersed in cold water.
- The operator had not experienced a water landing previously, but had an emergency response plan should this occur. It included raising the alarm through an air traffic controller and the Police emergency number. It relied on the harbourmaster and Queenstown Coastguard providing a waterborne rescue effort.
- The operator’s plan did not ensure parachutists were rescued in a time appropriate for survival in the conditions, nor did it have a vessel to implement such a recovery. However, the plan was an improvement on the previous operator’s plan for that location, and the operator has since provided its own rescue vessel at the aerodrome.
-
The water temperature was about 10° Celsius, which limited the likely survival time of the tandem pair. A research report prepared for Transport Canada in 2001 identified four stages after immersion in cold water where death can occur (Brooks, 2001). They are, in order of severity:
1 – cold shock
2 – swimming failure
3 – hypothermia
4 – post-rescue collapse.
- The research report stated that the anticipated survival times had usually been based on a person reaching the hypothermic stage, but it is now considered that stages 1 and 2 are more common causes of death. Drowning can occur from cold shock affecting the circulatory and respiratory systems within five minutes, followed by loss of dexterity within 30 minutes, leading to an inability to remain afloat. The operator’s water emergency response plan could not get rescuers to a parachutist within five minutes of their entering the water at Lake Wakatipu.
Accident and incident data
Safety issue: The CAA dataset for parachuting occurrences did not include key fields, which likely reduced its effectiveness as a tool for safety management in the sector.
-
The CAA policy on the collection of safety information defines its expectations as paraphrased below.
The CAA has a set of tools it can deploy to change the attitudes and behaviours of participants in the civil aviation system. To make these tools effective, the CAA collects safety data and information, assesses it and disseminates it… The CAA will make a reasonable attempt to verify the safety data and information supplied to it but expects those providing mandatory reports [under Civil Aviation Rules Part 12 – Accidents, Incidents, and Statistics] to ensure the data and information contained within the reports is accurate (CAA, 2009).
- For a safety management system to be effective, it needs to be based on a comprehensive record of occurrence data. Analyses of that data may identify trends and enable a safety manager to implement solutions before these trends result in accidents. Individual Part 115 parachute operators are required to manage their own occurrence databases and to report occurrences to the CAA. The data from these reports is then entered into the CAA occurrence database to provide a national resource.
- However, when the Commission examined the CAA occurrence data, it found it to be rudimentary and not thorough enough to identify some trends. For example, the CAA database did not record relevant details about a parachute assembly even if they were provided in the parachute operator’s Civil Aviation Rules Part 12 (Accidents, Incidents, and Statistics) report. Relevant examples for this accident were: the type of reserve parachute; if the reserve parachute was activated; how the reserve parachute was activated; and if the reserve parachute opened without problems.
- The CAA introduced a dedicated skydiving incident-reporting form after this accident, but it is not included in Civil Aviation Rules Part 12 and its use is not described in the associated Advisory Circular AC12-1. The new form also lacks any fields for the equipment details of a reserve parachute and AAD or if one had been activated. The CAA subsequently advised, on 16 October 2020, that AC12-1 was being updated to include adventure aviation reporting.
- This mismatch between submitted occurrence data from operators and a reduced subset of data recorded by the CAA was a lost opportunity for the CAA to gain national insights into the safety performance of the parachute sector.
Appendix 1. Civil Aviation Rules structure
Appendix 2. Parachute equipment
A typical ram-air parachute is shown below with component parts. Component names unique to reserve parachutes are enclosed in brackets.
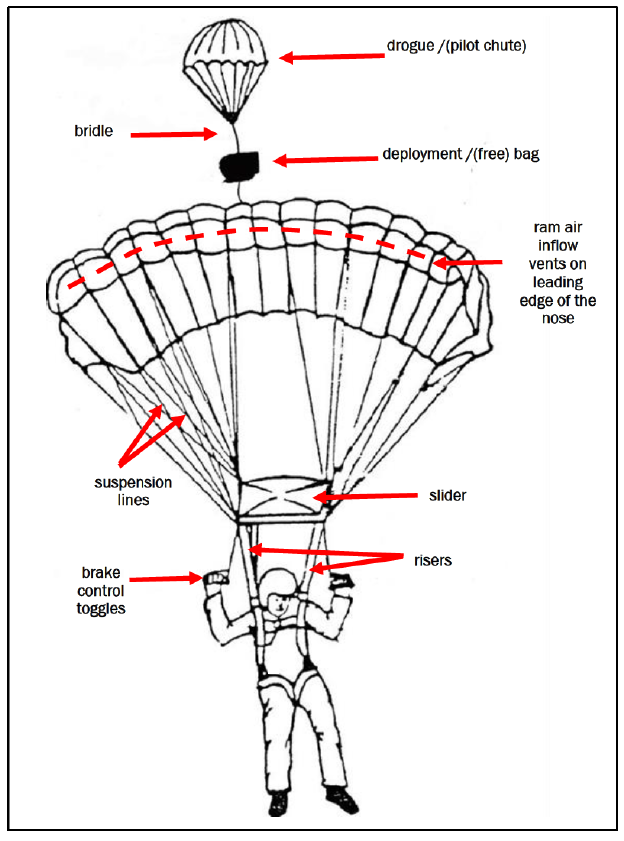
Both the main and the reserve parachutes were the ram-air design. Ram-air parachutes are made from two layers of fabric (top and bottom) connected by fabric ribs to form 'cells'. The cells are pressurised through the open air vents on the leading edge of a parachute to inflate into an aerofoil shape.
The main parachute is packed into a deployment bag. In the case of the reserve parachute, a free bag is used, which detaches from the canopy after deployment. The two parachutes in their deployment bags are packed into their own compartments in the backpack harness container system.
Suspension lines connect the parachute canopy to risers, which are lengths of webbing that connect the lines to the harness. They are arranged in rows from the nose to the tail and named A to D from front to back. The A lines are made shorter to hold the nose down when the canopy inflates. There were four risers, each one connected to its own line group.
Once correctly inflated, the parachute is controlled by brake lines attached to either side of the canopy along the trailing edge (canopy tail). The brake lines are routed down to hand toggles. Pulling down on one toggle will increase the drag on that respective side of the parachute, resulting in a turn in that direction. Pulling both toggles together will slow the entire parachute down; it acts like a brake during landing.
Ram-air parachutes may be rectangular or tapered. High-performance ram-air parachutes are the tapered style with an elliptical shape.
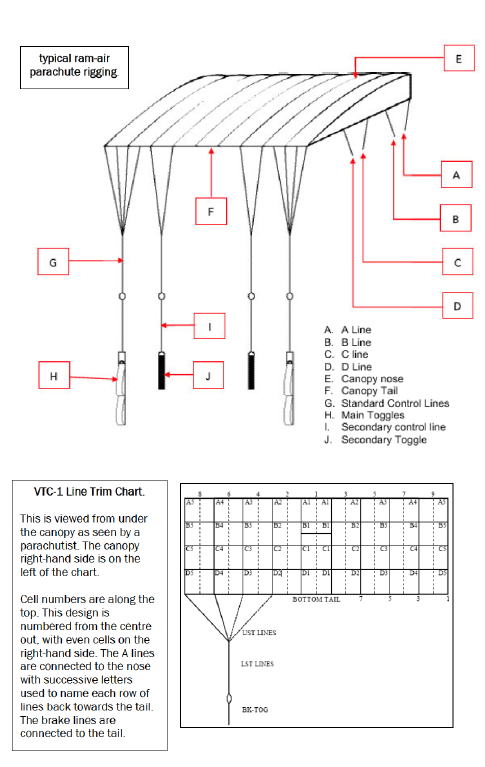
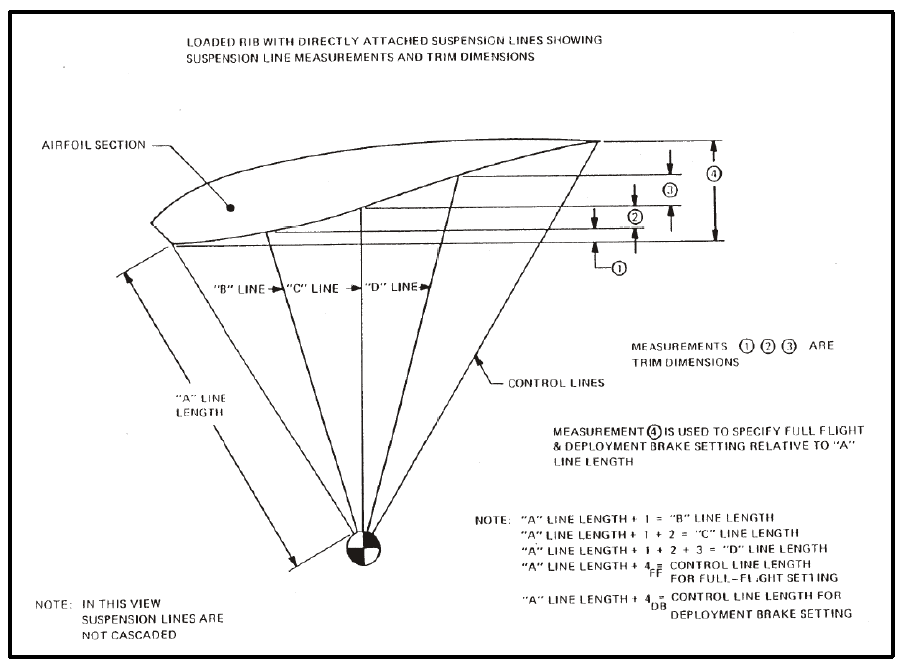
Typical parachute suspension line lengths (from an early version of the Parachute Industry Association Technical Standard 100, dated 23 January 1984).
UPT Micro Sigma tandem parachute assembly.
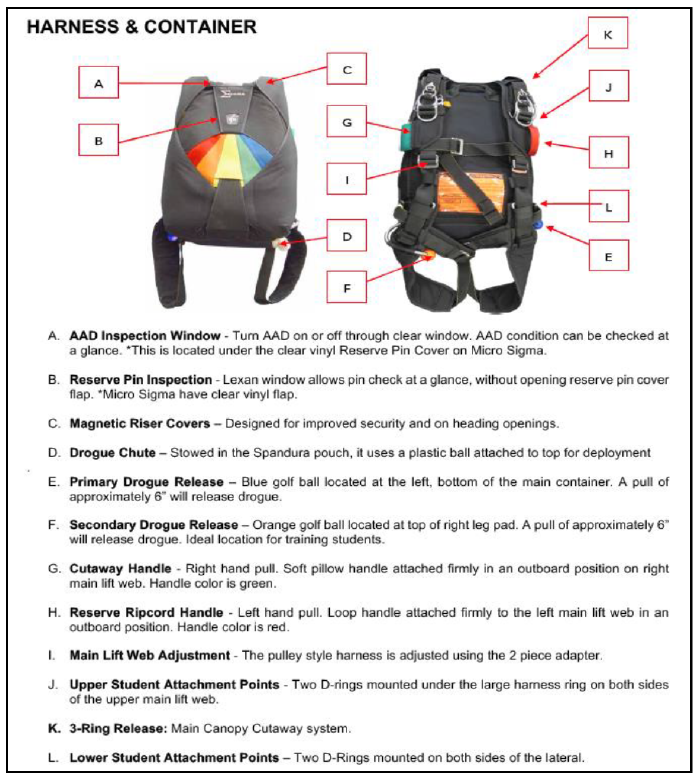
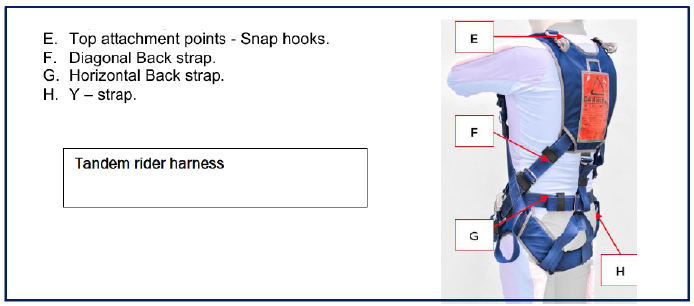
Appendix 3. AAD record
This is the AAD record of the droguefall stage of the accident parachute jump.
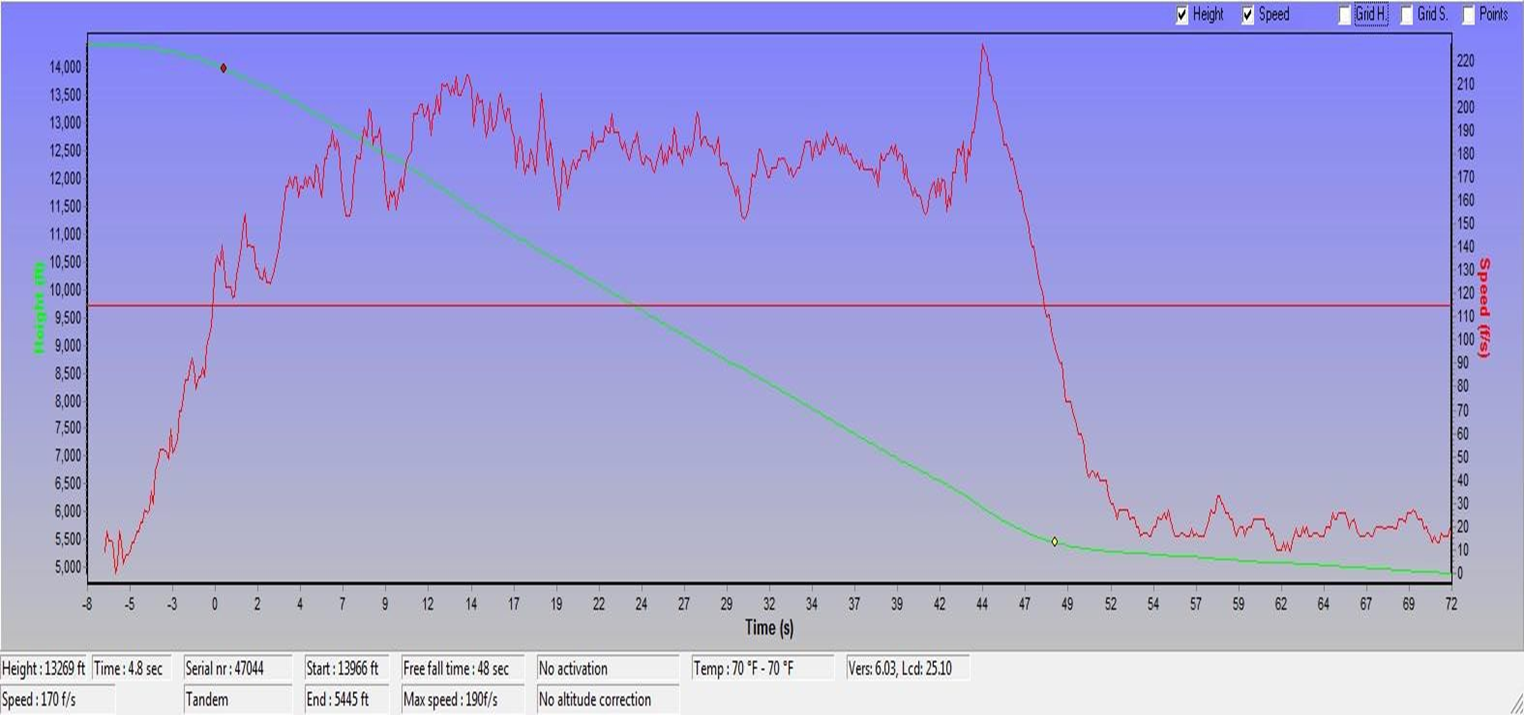
Appendix 4. Extract of Civil Aviation Rules for operations near water
Civil Aviation Rules
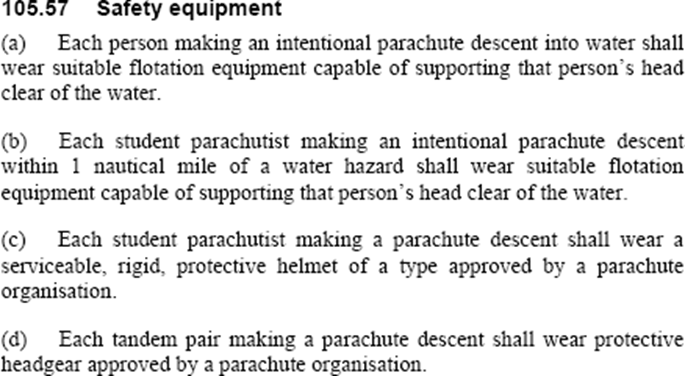
The NZPIA rule for this aspect is:
The operator’s exposition at the time stated: