A BK117 helicopter was transporting a power pole. Pilot at risk of distraction, didn’t recognise and respond promptly to unanticipated yaw (helicopter unexpectedly turning about its vertical axis). The pilot lost control and ditched in shallow water. Minor injuries for pilot, substantial damage to helicopter.
Executive summary Tuhinga whakarāpopoto


- On Tuesday 2 May 2017, a BK117 A-3 helicopter was being used to transport three 11-metre long hardwood power poles from a staging area on one side of the Pāuatahanui Arm of Porirua Harbour and place them in holes that had been prepared near the shoreline on the other side of the Arm.
- The first pole had been connected by a sling to the cargo hook beneath the helicopter. The helicopter lifted the pole from the staging area and was flying across the water when the pilot began to lose control of the helicopter. The pilot made an emergency ditching into shallow water.
- The pilot escaped from the partially submerged helicopter with minor injuries. The helicopter was substantially damaged.
- The Transport Accident Investigation Commission (Commission) found no mechanical issues with the helicopter that would have likely contributed to the accident.
- The Commission found that control of the helicopter was lost likely due to a phenomenon known as unanticipated right yaw. The Commission also found that operational pressure likely combined with other stressors to increase the risk of the pilot becoming distracted.
- The pilot did not undergo post-incident drug and alcohol testing as per the operator’s drug and alcohol policy, but the pilot did undergo a Police breath alcohol screening test immediately after the accident.
- There was no evidence to suggest that the pilot’s previously diagnosed medical condition or the medication prescribed was a factor in this accident. However, non-disclosure of the medical condition and prescribed medication to the Civil Aviation Authority was a serious concern for the Commission.
- The Commission found several significant anomalies in the maintenance records for the helicopter, which had been left unresolved at the time the Civil Aviation Authority issued it with a certificate of airworthiness.
- The helicopter had not undergone all the inspections and verification-of-maintenance tasks required before the Civil Aviation Authority issued the certificate of airworthiness.
- During the inquiry it was discovered that other aircraft owned and operated by the same company that imported the helicopter into New Zealand also had significant anomalies in their maintenance records.
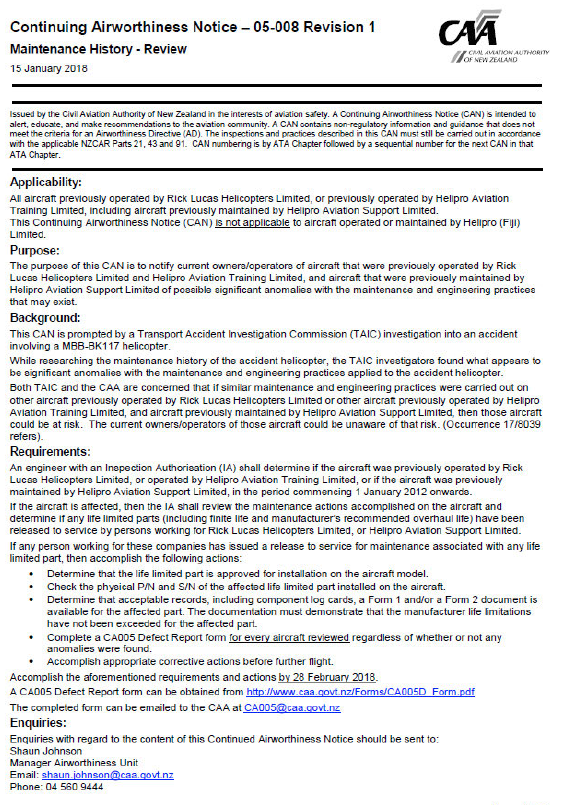
- In its interim report on the accident, the Commission raised with the Civil Aviation Authority that the number and nature of maintenance anomalies involving aircraft operated by Helipro were a safety issue. The concern was that there could be historical or latent maintenance issues with some of Helipro’s other aircraft that had been on-sold and were then being operated on the New Zealand register by various other companies.
- The Civil Aviation Authority immediately issued a Continuing Airworthiness Notice to address that safety issue. It was subsequently withdrawn after no reports were received.
- In this report the Commission has identified a further safety issue, whereby the Civil Aviation Authority’s process for entering second-hand imported aircraft into the New Zealand regulatory system was not clearly defined; was not clearly understood by some staff; and did not have the checks in place to ensure it was followed.
- The Civil Aviation Authority subsequently arranged an independent review of the process for issuing a certificate of airworthiness, including the conformity inspection process for second-hand aircraft. However, the Commission believes further action needs to be taken. As a result, the Commission has made one recommendation to the Civil Aviation Authority to address that issue.
- Key lessons arising from the inquiry include:
- pilots can experience distraction during all phases of flight. Pilots must remain vigilant to ensure that their performance is not degraded by distraction when attending to various tasks necessary to the safe operation of an aircraft
- unanticipated yaw is a flight characteristic to which all types of single-rotor helicopter can be susceptible. Pilots need to remain cognisant of the conditions in which the phenomenon is likely to occur and the actions required for recovery
- the disclosure of medical conditions and prescribed medication to the Civil Aviation Authority ensures that their aeromedical significance can be determined. It does not automatically preclude a pilot from carrying out their duties, but does ensure a pilot can operate an aircraft safely
- it is essential that all maintenance and inspection tasks are conducted and properly recorded in accordance with applicable rules.
Factual information Pārongo pono
Narrative
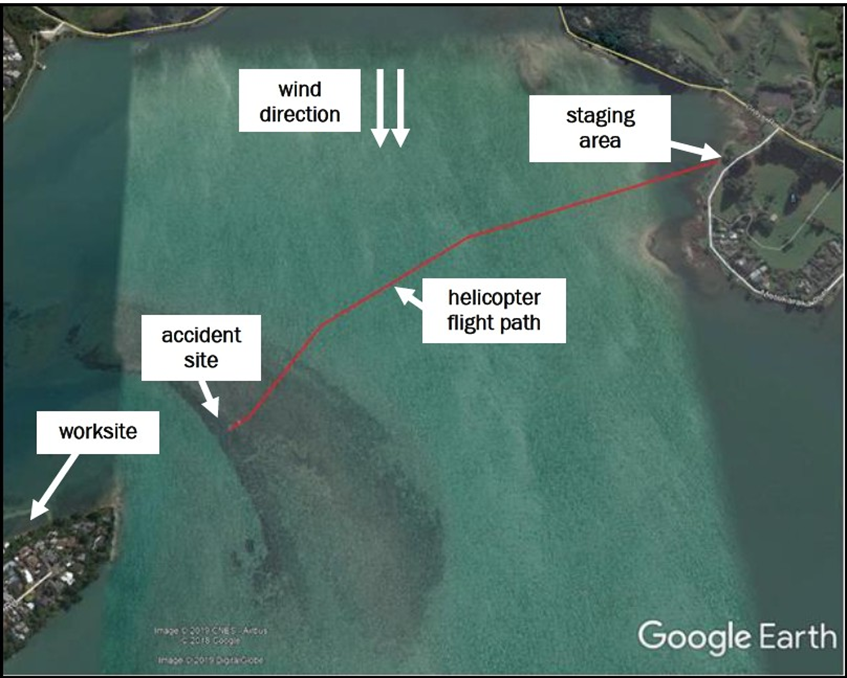
- On 2 May 2017, a Messerschmitt-Bölkow-Blohm GmbH BK117 A-3 helicopter (the helicopter), was being used to transport three 11-metre long hardwood power poles from an area of open land (the staging area) near the shore on one side of the Pāuatahanui Arm of Porirua Harbour and place them in holes that had been prepared near the shoreline on the other side of the Arm (refer to Figure 3).
- The weather in the Porirua area at the time of the accident was reported by MetService (New Zealand’s sole certificated aviation weather forecast provider: http://www.metservice.com/national/home) as partly cloudy, with a northerly wind of eight knots (15 kilometres per hour [km/h]), gusting to 20 knots (37 km/h), and good visibility. The temperature was 13.5° Celsius. Witnesses in the area described similar conditions.
- On the morning of the accident, the pilot arrived at the staging area by road and briefed staff from the electricity network on the lifting operation. The pilot had previously given a hand-held portable air-to-ground radio to the electricity network staff at the worksite across the harbour to communicate with the pilot while placing the poles in the holes. There was an additional hand-held radio for staff at the staging area to communicate with the helicopter during the operation.
-
The pilot prepared the first lift by joining two slings together to make a 20-metre lifting line, which was then attached to the first pole lying on the ground. The operator’s chief pilot was also at the staging area conducting an internal audit of the operation.
- Meanwhile another pilot (the staff pilot) was ferrying the helicopter from the operator’s Wellington base to the staging area.
- Following a brief handover of the helicopter from the staff pilot and the removal of the right-hand door, the pilot took control of the helicopter and lifted into a hover while a member of the ground crew attached the lifting line to the helicopter’s cargo hook. The helicopter then lifted the pole, and global positioning system (GPS) data showed that the helicopter climbed vertically to approximately 120 feet (37 metres). The helicopter repositioned, turned and transitioned forward to a speed of about 40 knots (74 km/h), climbing to 230 feet (71 metres) above the water. It flew in a southwesterly direction towards the worksite (see Figure 3).
- The operator’s chief pilot at the staging area overheard, on the portable radio, the pilot make a call to the staff at the worksite as the helicopter made the short trip across the water. The pilot did not get a response. The staff at the worksite stated that they did not receive the call.
- After the short transit across the water, the pilot began to slow the helicopter as it was nearing the worksite. The pilot later recalled changing radio channels to make contact with staff at the worksite, when what the pilot described as “a significant medium-frequency airframe vibration” occurred, which then “amplified with pronounced oscillation”, followed by a “sudden rotation of the helicopter to the right”.
- A witness at the staging area stated they could hear on the radio the pilot attempting to call staff at the worksite. The witness described seeing the helicopter's nose pitching up and the helicopter starting to rotate immediately after the pilot made the call.
- The pilot reported that they abruptly lowered the collective lever, which had the effect of slowing the rotation, but caused the helicopter to descend more quickly than the pilot expected. The pilot then raised the collective lever again, but the helicopter rolled to the right, pitched nose down and struck the water. The pilot did not recall jettisoning the load from the helicopter's hook, although one witness saw the pole fall after the helicopter started rotating.
- The helicopter struck the water right-side low and suffered substantial damage to the main rotor blades, engines and engine drive shafts. The fuselage remained relatively intact.
- The helicopter came to rest on its right side in shallow water. The pilot was seated on the right side, wearing a three-point seat harness, and had to perform an underwater evacuation for which they had previously received training. The pilot suffered minor injuries.
Personnel information
- The pilot held commercial pilot licences for helicopters and aeroplanes. The pilot’s total flying experience was approximately 8,300 hours, with approximately 7,000 of those hours on various helicopter types. The pilot held a Category B flight instructor rating and a multi-engine instructor rating, for which a renewal check was conducted on 13 December 2016.
- The operator’s chief pilot conducted the pilot’s last flight crew competency check on 1 November 2016.
- At the time of the accident, the pilot held a current class one medical certificate with an endorsement for spectacles to be available. On 5 May 2017 (three days after the accident), the Civil Aviation Authority (CAA) withdrew the certificate. The notice of withdrawal stated that ‘records at CAA indicate possible medical circumstances that may jeopardise flight safety’.
- The pilot had been prescribed medication to treat a medical condition. The medication and condition were of aeromedical significance, but neither was disclosed to the CAA, and according to the pilot, the prescription medication had not been taken. The pilot had seen a different general practitioner (GP) from their declared GP for this medical condition.
- There was nothing in the pilot’s medical records for the five months prior to the accident to indicate that the pilot had consulted their declared GP. Ministry of Health records for this period showed there had been no prescriptions dispensed to the pilot since December 2016.
- The operator of the helicopter had a drug and alcohol policy that required a pilot to be tested after an accident. The pilot underwent a Police alcohol screening test after the accident, which returned a negative result, but did not undergo a drug test as required by the company policy. A witness who had been located at the staging area, who knew the pilot, said that the pilot looked physically tired on the day of the accident.
Organisation information
- On 26 March 2014, the helicopter was first registered in New Zealand to another company trading as Helipro.
- Helipro Aviation Support Limited (Helipro Maintenance) was a part of the Helipro business. Helipro Maintenance was a maintenance provider certificated under Civil Aviation Rules (CAR) Part 145 (the holder of a CAR Part 145 certificate is authorised by the CAA to perform maintenance in accordance with the specifications in their exposition and the general maintenance rules in CAR Part 43. Without the certificate, maintenance could be performed only in accordance with CAR Part 43, which limited the scope of the maintenance that could be performed) until July 2014.
- Helipro Maintenance staff prepared the helicopter for the CAA airworthiness certificate inspection in August 2014. The helicopter was then maintained under CAR Part 43 General Maintenance Rules as it was not being used for air transport operations.
- The pilot was the chief pilot and a director of Helipro until November 2014. Helipro had been placed into receivership in October 2014.
- On 7 November 2014, Precision Helicopters Limited (Precision Helicopters) became the registered operator of the helicopter. It was being operated under that company’s air operator certificate at the time of the accident. The helicopter was leased to Heliforce under a business arrangement whereby Heliforce employed the pilots who flew the helicopter and arranged the work contracts with clients.
- The helicopter was added to the Precision Helicopters ‘operational specification’ (the conditions imposed by the Director of the CAA on the air operator certificate, including any authorisations, limitations and procedures that form part of the certificate). The helicopter was then operated from Wellington Airport, with Precision Helicopters controlling the maintenance, training and quality systems of the operation.
- Precision Helicopters was authorised under CAR Part 119 to perform air operations and associated activities in accordance with CAR Parts 135 and 133, as detailed in the operations specification and the organisation’s exposition.
- The lifting task on 2 May 2017 was a permitted operation for Precision Helicopters. The pilot was employed by Heliforce, and held a category A pilot status with the operator. This meant the pilot could have, and was given, sole charge of the lifting activities. However, as the operator, Precision Helicopters had responsibility for ensuring it was conducted in accordance with its policies and procedures.
Aircraft information
- The BK117 A-3 helicopter is powered by two turbo-shaft engines. Power from the engines is transmitted to the main rotor transmission through drive shafts with flexible couplings. Each engine drive shaft is connected to a freewheel clutch within the main rotor gearbox to enable single engine operation or to facilitate autorotation. The helicopter has four glass-fibre-reinforced main rotor blades connected to a titanium rigid rotor head. The BK117 has an anti-clockwise rotating main rotor when viewed from above.
- The tail rotor comprises two semi-rigid, glass-fibre-reinforced-plastic tail rotor blades with a central flapping hinge. The tail rotor gearbox is fitted to the top of the vertical fin, with an intermediate gearbox at the base of the fin. Attached to the horizontal stabiliser, either side of the vertical fin, are vertical stabilisers.
- The accident helicopter had a ‘yaw stability augmentation system’, which applied limited control inputs to the tail rotor through an electro-hydraulic servo. The control switch for this system is located in the cockpit. The system was normally switched on, as it was in this case.
- The maximum allowable all-up weight for the helicopter was 3,200 kilograms (kg). A flight manual supplement for the hook assembly specified that the underslung load limit on the hook assembly was 900 kg, although this was later determined to be erroneous at the time of the accident and the correct load limit was 1,200 kg.
- The helicopter was manufactured in Germany in 1985 by Messerschmitt-Bölkow-Blohm GmbH (later part of Airbus Helicopters). It was imported into New Zealand from the United States in January 2014, having accrued a total time in service of 11,123 hours.
- A second BK117 helicopter, with serial number 7124 (helicopter B), was imported from the United States at the same time. Parts from helicopter B were later installed on the accident helicopter.
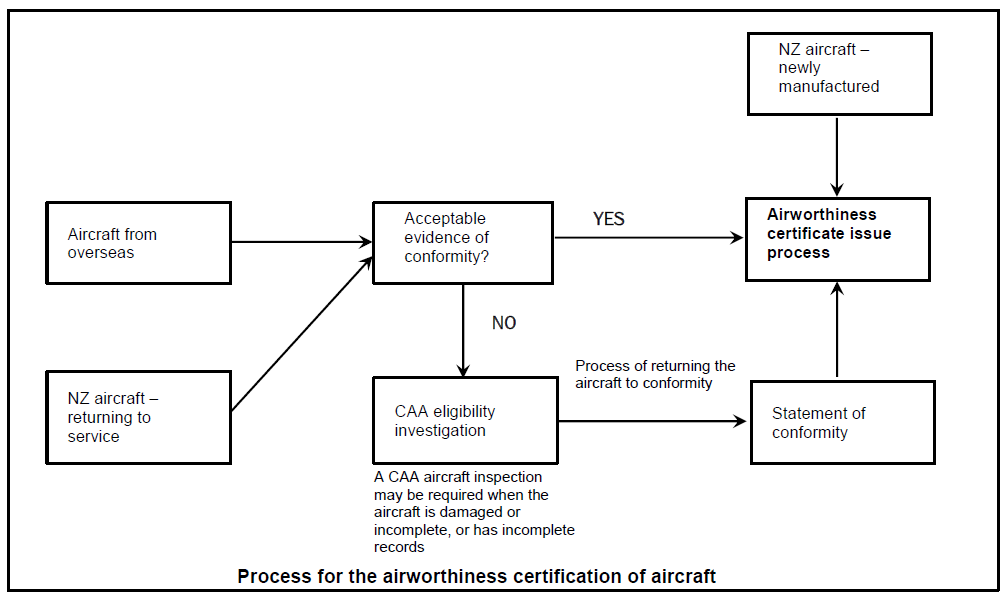
- For an aircraft to be eligible for an airworthiness certificate in New Zealand, it must have a statement of conformity. Neither helicopter came into New Zealand with a United States Federal Aviation Administration (FAA) export certificate of airworthiness. Therefore, in order for an airworthiness certificate to be issued, the CAA required an inspection of the helicopter and its associated documentation by its staff, as well as a review of airworthiness by an ‘authorised person’ (a person who is the holder of a ‘certificate of an inspection authorisation’ issued by the CAA) in order to be satisfied that the helicopter conformed to its type certificate (a document issued by the State of Design to define the design of a product and to certify that the manufacturer has demonstrated its compliance with regulatory requirements). More information on these aspects is included in section 4.6 below. On 21 August 2014, the CAA issued the helicopter with an airworthiness certificate (helicopter B was not issued with a New Zealand airworthiness certificate).
- The helicopter had flown a total of about 11,512 hours at the time of the accident. The last annual review of airworthiness had been completed on 24 October 2016. The last scheduled maintenance had been a 50-hour airframe inspection carried out on 18 November 2016.
Wreckage and impact information
- Moderate damage to the right-hand underside of the helicopter (see Figure 4) indicated that the helicopter had a right bank and level pitch attitude when it struck the water.

- There was a slight twist in the tail boom structure. All four main rotor blades had been destroyed from striking the water while under power.
- The forward left main rotor transmission mount had buckled under compression loading from the vertical component of the impact forces.
- The power output assemblies of both engines were damaged by overload forces applied during the sudden stoppage of the main rotor.
- The tail rotor blades and associated drive train appeared to be undamaged and remained connected to the main rotor transmission.
- The flight control system was undamaged, with no defects evident.
- The left side of the vertical fin had failed and separated and the right-hand side was buckled (see Figure 5).
- The vertical fin spar was found to have a diagonal crack extending through it (see Figure 6).


Tests and research
- A licensed aircraft maintenance engineer, rated on the BK117, and a technical adviser from Airbus helicopters found no defects in the tail rotor assembly or drive train that could have caused a loss of tail rotor control or that could have contributed to the failure of the vertical fin structure.
- Other known BK117 accidents were considered. In 1997 a BK-117-B2 struck terrain and was investigated by the National Transportation Safety Board of the United States (NTSB). The investigation found that the tail fin had failed due to fatigue. The use of blind rivets had increased the tail fin structure’s susceptibility to fatigue. In 2006 a fatigue crack was identified in the vertical fin of a BK-117. The manufacturer subsequently issued an Alert Service Bulletin to helicopter operators to address the issue.
- Solid rivets were fitted to the accident helicopter, not the hollow rivets that had contributed to the fatigue-related structural failure in 1997.
-
An expert metallurgist engaged by the Commission examined the vertical fin and determined that the crack in the spar was the result of structural overload during the forced landing. The Defence Technology Agency (DTA) (the main provider of research, science and technology support to the New Zealand Defence Force and the Ministry of Defence) also carried out testing. They visually inspected the vertical fin and then inspected six possible crack initiation sites using scanning electron microscopy (SEM) (the use of a scanning electron microscope, which is a type of electron microscope that produces images of a sample by scanning the surface with a focused beam of electrons). The results of the DTA inspection were consistent with the results of the previous expert metallurgist examination. The DTA concluded:
DTA inspection of the fracture faces of samples … are consistent with overload fracture upon impact. There was no evidence of fatigue cracking, brittle fracture or pre-existing defects.
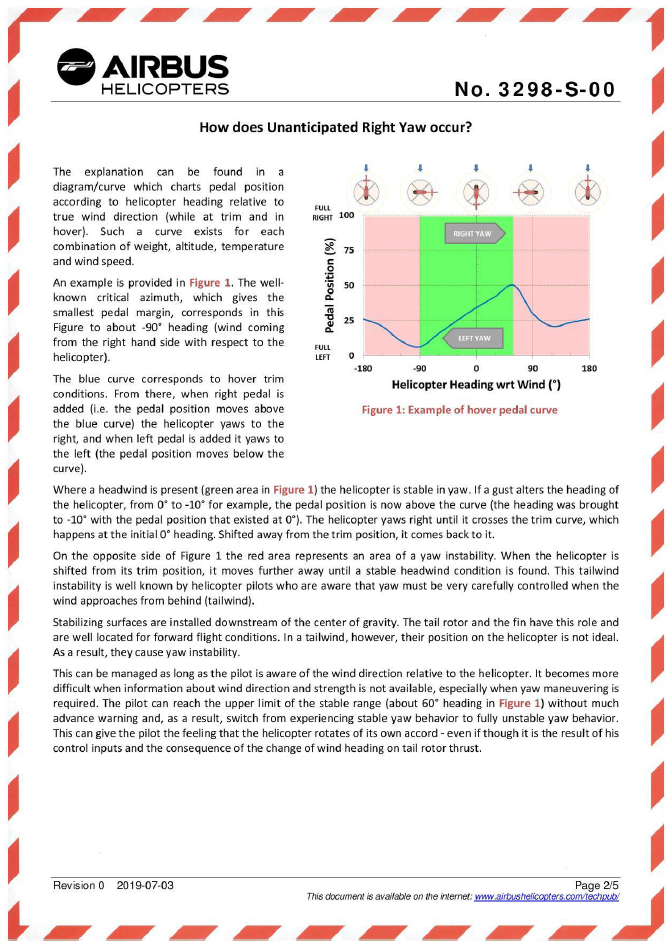
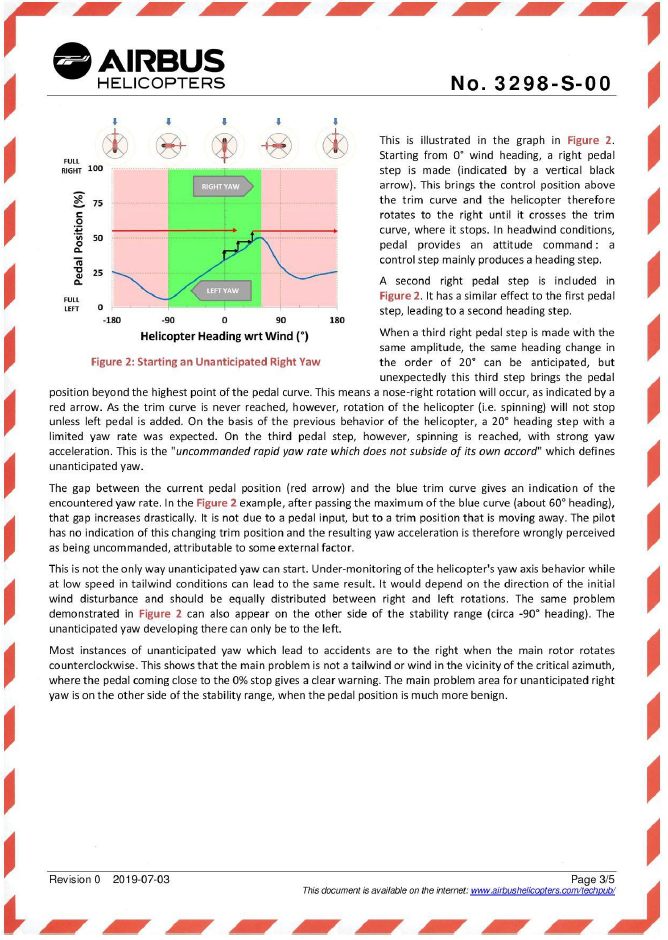
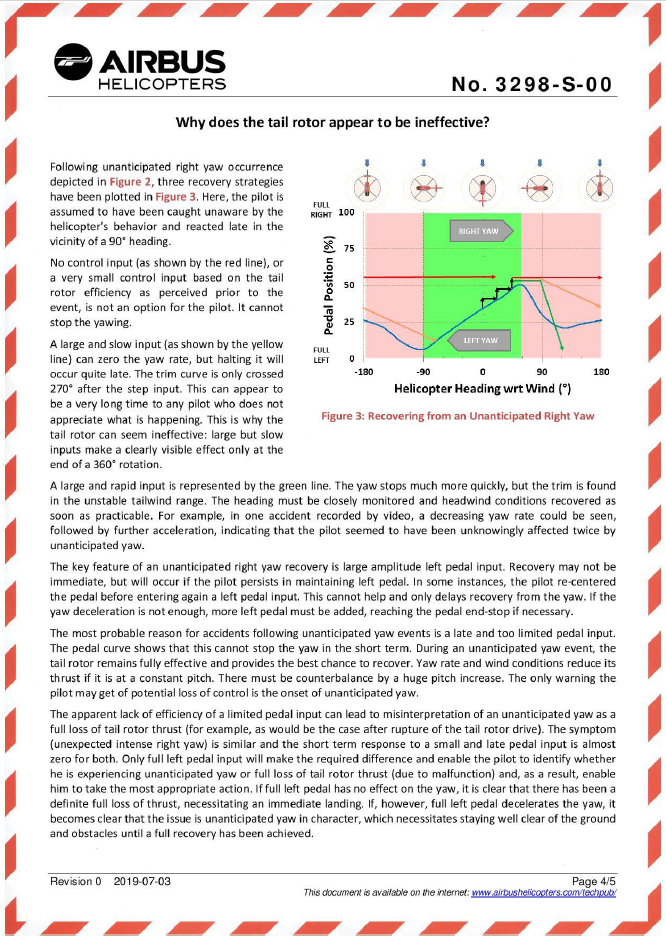
Appendix 2. Airbus Helicopters Safety Information Notice No. 3298-S-00
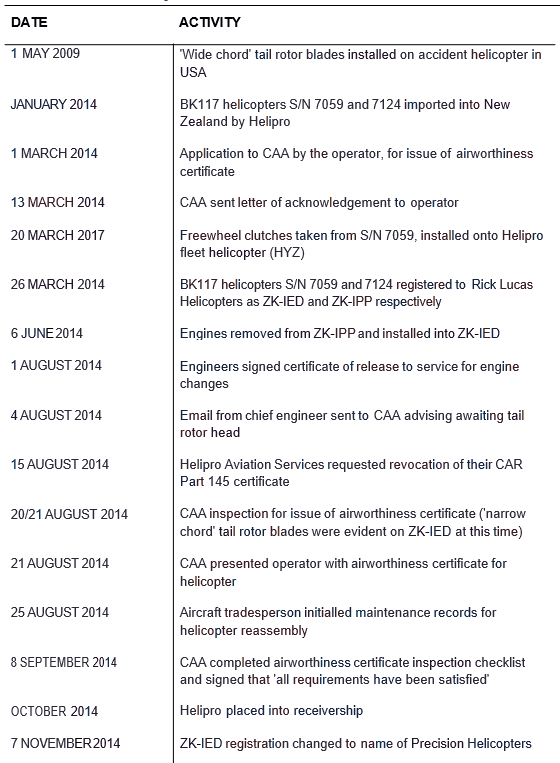
Appendix 3. Sequence of events related to the accident helicopter
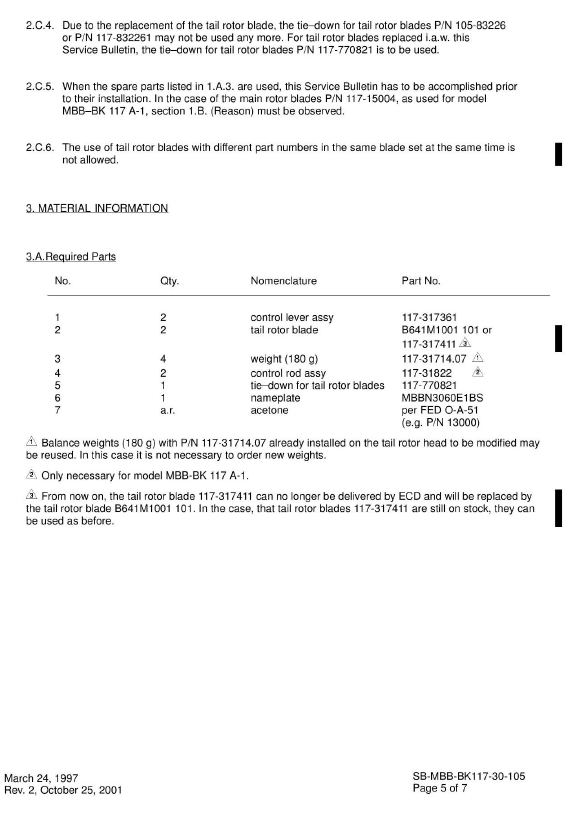
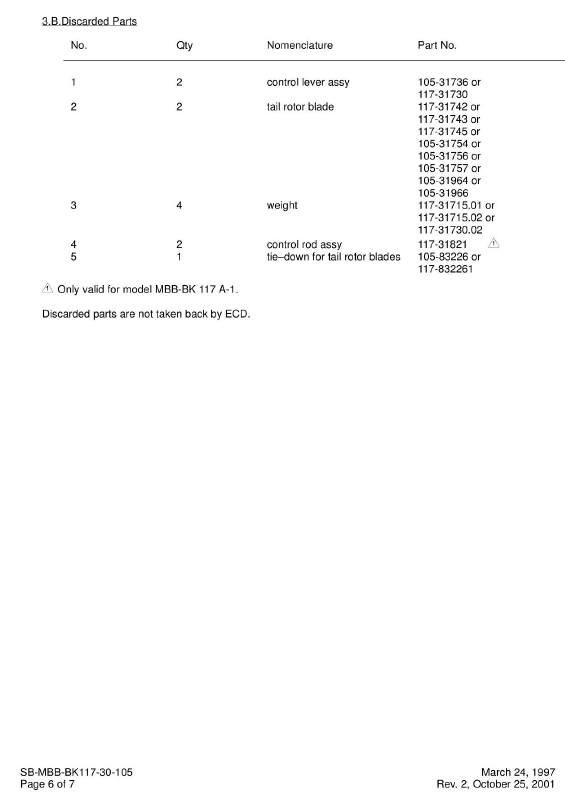
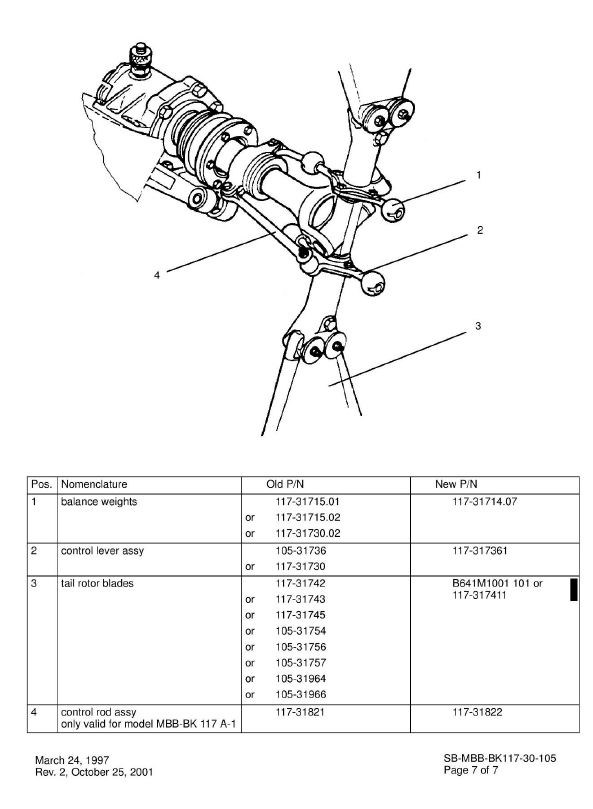
Appendix 4. Eurocopter Service Bulletin SB-MBB-BK 117-30-105
Appendix 5. Continuing Airworthiness Notice (CAN) 05-008
Appendix 6. Advisory Circular AC 21-2, Airworthiness Certification Process