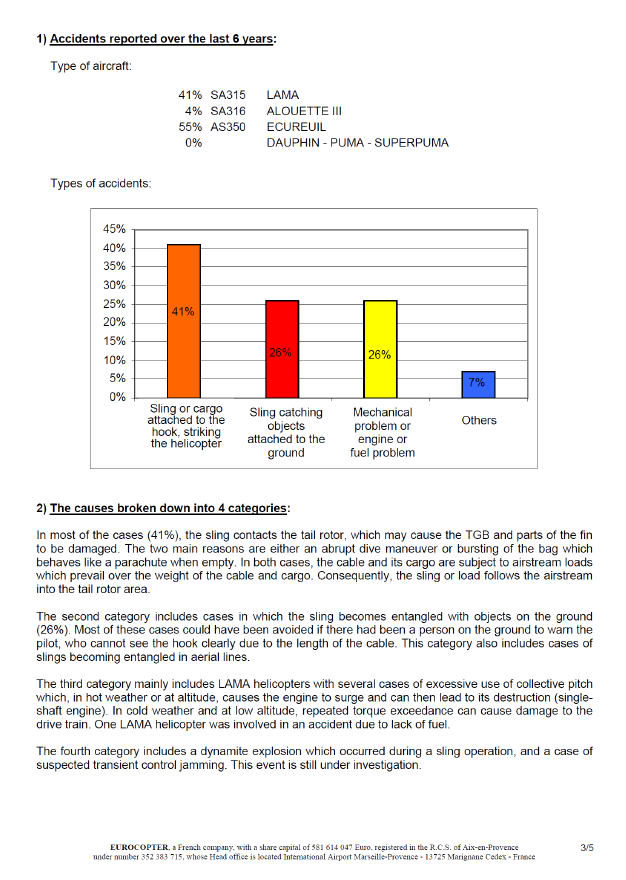
An AS350 helicopter fighting wildfires on the Christchurch Port Hills crashed after up-swinging monsoon bucket cable hit tail rotor assembly. Pilot fatally injured, helicopter destroyed. Key lessons: need for vigilance during turbulence; always fly within aircraft’s limitations; operators should record and investigate all operational incidents; and performance-impairing substances pose a serious risk to aviation safety (NB: very unlikely pilot was impaired at time of accident).
Executive summary Tuhinga whakarāpopoto

-
On the afternoon of 13 February 2017, wildfires broke out on the Port Hills between Lyttelton Harbour and the south-eastern suburbs of Christchurch. A major effort began early the following day to control the fires, using large ground parties assisted by up to 12 helicopters and two aeroplanes. In the early afternoon one of the helicopters, a Eurocopter AS350 BA
‘Squirrel’ registered ZK-HKW, crashed while returning to the dipping pond to refill an underslung monsoon bucket. The pilot was fatally injured and the helicopter was destroyed.
- The suspension line for the monsoon bucket had contacted the tail rotor. The damage to the tail rotor caused the vertical stabiliser to tear off the tail boom, and the helicopter became uncontrollable and crashed.
- A video recording taken from a camera mounted underneath the helicopter showed the monsoon bucket rising towards the tail rotor. The video recording also showed that an object fell from the helicopter shortly beforehand. It is virtually certain that this was the window that had dislodged from the left rear sliding door. The pilot had experienced a similar loss of the left rear window while flying the same helicopter on a firefighting mission in 2015.
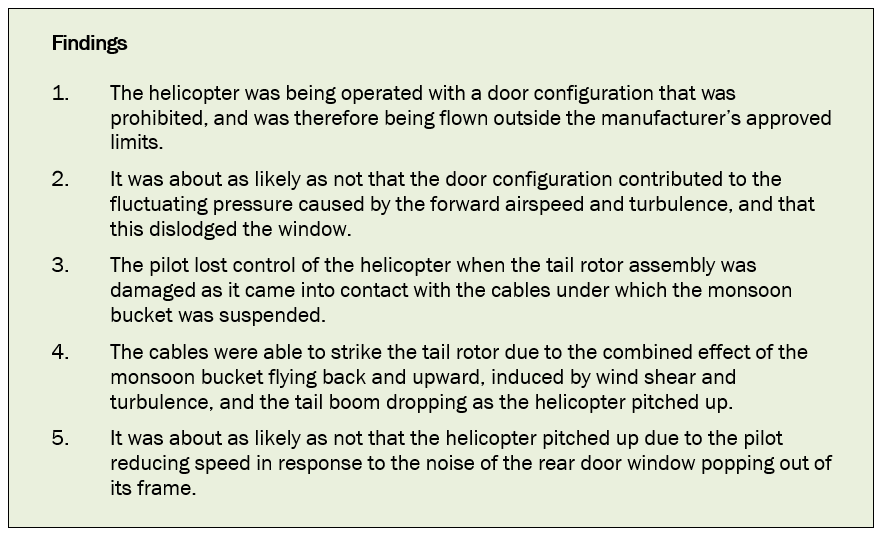
- The Transport Accident Investigation Commission (Commission) found that the door configuration was prohibited in the flight manual, and therefore the helicopter was being flown outside the manufacturer’s approved limits. It was very likely that the monsoon bucket flew up towards the tail rotor due to a combination of forward air speed and turbulence. At the same instant, the pilot’s slowing of the helicopter in response to losing the window resulted in the tail rotor dipping and making contact with the rising suspension line for the monsoon bucket.
-
The hazard of an underslung load striking a tail rotor is a known risk to helicopter operations.
- Although not directly contributing to the accident, the Commission found three deficiencies that indicated the helicopter operator’s quality assurance system should be reviewed.
- The Commission found that it was very unlikely that the pilot was impaired by his recent use of cannabis, but reiterates its view that the use of performance-impairing substances by pilots is a serious risk to aviation safety.
-
Two safety issues were identified in the inquiry:
-
there may not be a good awareness within the helicopter industry of the additional risks involved with underslung load operations, particularly with the use of monsoon buckets during firefighting operations
- the operator did not have adequate systems available for the pilot to determine the actual all-up weight and balance of the helicopter for the firefighting operation, or to ensure that incidents such as the previous loss of a window were recorded, notified to the CAA and investigated.
- The Commission has previously made recommendations to address the issue of substance impairment and to address industry awareness of the risks involved with underslung load operations. It made a new recommendation to address the operator’s procedural safety issues.
- The Commission identified the following key lessons as a result of its inquiry into this accident:
- flight in turbulent conditions requires care in order for the pilot to avoid exceeding an aircraft or equipment speed limitation
- it is important that operators and pilots understand the reasons for and observe the specific limitations applicable to each aircraft that they operate, as variations often exist between different variants of the same aircraft type
- all operational incidents should be recorded and investigated by the operator so that the causes can be identified and corrective or preventive actions taken
- performance-impairing substances such as recreational drugs pose a serious risk to aviation safety. Their short- and long-term effects may be unpredictable and result in pilots being impaired when flying their aircraft.
Factual information Pārongo pono
Narrative
- On the afternoon of 13 February 2017, wildfires broke out on the Port Hills between Lyttelton Harbour and the south-eastern suburbs of Christchurch. The National Rural Fire Authorit (on 1 July 2017 the National Rural Fire Authority merged with urban fire services to form Fire and Emergency New Zealand) was controlling the response. It contracted helicopter companies to survey the extent of the fires and to evacuate a number of people. Way To Go Heliservices Limited (the operator) provided one of the helicopters, a Eurocopter AS350 BA ‘Squirrel’ registered ZK-HKW (the helicopter). The pilot flew back to the operator’s base at Rangiora Airfield at about dusk.
- At about 0540 the next day the same pilot flew the helicopter from Rangiora to re-join the firefighting operation, which now involved more helicopters and occasionally two aeroplanes. At the staging area the fire authority’s ‘air attack supervisor’ (the supervisor) briefed the pilots on the situation and the planned operations for that day. The briefing covered the expected weather, any known hazards and the general procedures to be followed. The supervisor was an experienced park ranger who was familiar with the area and had extensive experience in fighting wildfires and in controlling firefighting aircraft. The supervisor oversaw the aviation effort from an airborne helicopter.
- The supervisor allocated the aircraft to separate sectors of the fire and appointed a lead pilot for each sector. The pilot of the accident helicopter was appointed lead pilot for the three helicopters in his sector.
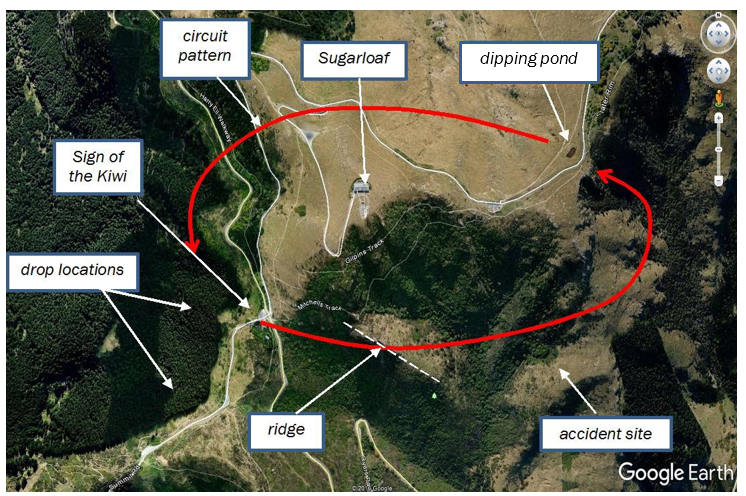
- After receiving further instructions from the supervisor, the pilot briefed the other pilots in his group on the agreed circuit pattern and the radio procedures. The circuit pattern between the dipping ponds and drop points allocated to each group provided separation from other groups, but each pilot remained responsible for their own aircraft’s safe operation.
- The pilot’s group operated at several locations on the Port Hills during the morning. After a lunch and refuelling break, the group was directed to drop water on fires near the ‘Sign of the Kiwi’, a historic building at the junction of Summit Road and Dyers Pass Road. The dipping pond was adjacent to Summit Road, about two kilometres northeast of the fires.
- The pilots flew a left-hand pattern in clear conditions between the dipping pond and the fire, around Sugarloaf peak (Sugarloaf is a Port Hills landmark 494 metres above sea level, with a 121-metre-high mast on the summit) (see Figure 1). On the return leg to the dipping pond, the helicopters flew over prominent ridges south of Sugarloaf. One ridge was a 50-metre-high rocky outcrop with a cliff face on the west side. The time taken to complete one circuit, from dipping to returning to the pond after dropping the water on the fire, was approximately four minutes.
- At about 1405 an abbreviated ‘Mayday’ call was heard by several pilots, but it was not clear on which radio frequency the call had been made. The supervisor asked for a roll call of all aircraft, to which the pilot did not respond. Another pilot soon found the wreckage of the helicopter near the head of a gully east of Sugarloaf. The pilot had been fatally injured.
- A witness located at Governors Bay, two kilometres south of Sugarloaf, later reported having seen an object fall from the helicopter and the helicopter pitch up before it disappeared behind a ridge.
- The supervisor instructed all pilots to return to the staging area and to shut down. Firefighting flights did not resume until the pilots had been debriefed and had a mandatory rest, and each had decided whether to continue firefighting that day.
Personnel information
- The pilot had begun his training to fly helicopters in August 1998 and gained his commercial pilot licence in 2002. His total helicopter flying experience was about 2,350 flight hours, of which about 500 hours had been on the AS350 helicopter type.
- In January 2008 he had joined the operator, initially as a contract pilot and ground crew member. He had left the operator in August 2009, but returned in January 2013 as a full-time pilot.
- The pilot had commenced underslung-load training in March 2013, and at the time of the accident had accrued about 80 hours of such work. He held a ‘B category’ instructor rating, issued in September 2015, and a Grade 2 agricultural rating that had been issued in December 2016.
- The pilot held the ‘Senior Person’ roles (Senior Persons are mandated management positions for certificated operators. Holders are approved by the Civil Aviation Authority) of quality assurance manager and training manager for the operator. He also trained fire service personnel in working with helicopters in a firefighting role.
Medical
- The pilot held a class 1 medical certificate with no restrictions, valid until 26 February 2017. He was said to have been healthy and in good spirits on the day of the accident.
- The post-mortem examination of the pilot determined that he died as a result of multiple high-energy-impact injuries. The examination found no sign of any pre-existing neurological or cardiovascular disease.
- Through interviews with people closely associated with the pilot, it was established that he was an occasional user of cannabis, and had smoked cannabis when he was off duty two days before the accident.
- A screening test detected cannabis metabolites in samples of the pilot’s blood and urine. The tetrahydrocannabinol (THC) (the principal psychoactive constituent of cannabis) concentration in the blood was 0.6 micrograms per litre, and THC-acid was confirmed in the urine sample.
- Additional testing was undertaken in order to establish the relationship between the screening results and the pilot’s recent use of cannabis. An expert forensic toxicologist reviewed the test evidence and concluded that the pilot was “unlikely to have been under the influence of cannabis at the time of the accident”.
- Pilots must complete a questionnaire when applying to the Civil Aviation Authority (CAA) for a medical certificate. One of the questions is, “Have you ever had any experience with the following: use of legal or illegal recreational drugs or substances?” The pilot had answered “No” on his most recent medical certificate application form, dated 24 February 2016.
Aircraft information

- The helicopter had been manufactured in France in 1980 and imported into New Zealand in January 2015. It had flown for a total of 9,127 hours.
- An annual review of airworthiness had been completed on 1 February 2017. The most recent scheduled maintenance had been a 150-hour/annual airframe inspection performed on 8 February 2017.
- Pilots flew the helicopter from the right seat. They were assisted in performing underslung-load tasks, such as firefighting, by various modifications to the helicopter. The pilot’s seat could be locked in a position offset to the right of the normal position, which allowed a pilot a better view downwards on that side. The floor contained a window, outboard of the pilot’s seat, to observe an underslung load. The collective lever had an extension to ensure that the pilot had full control when their seat was in the offset position.
- A rear-facing mirror was installed under the nose of the helicopter on the right side. This enabled a pilot to see an underslung load during normal flight.
- The front seats were equipped with four-point harnesses. The shoulder straps for each seat had a common, lockable inertia reel mounted on the rear of the seat. The front-seat lap belt buckles had non-rotating, lifting catches. The adjustable lap belts were anchored to the floor.
- The helicopter was fitted with sliding doors on the left side of the cabin and standard doors on the right side. To further improve the pilot’s view of the underslung bucket while firefighting, all the doors on the right side had been removed and the doors on the left side were closed. A supplement to the AS 350 BA flight manual stated that this particular door configuration was prohibited for the helicopter (AS 350 BA flight manual supplement number 13). The operator said that it considered that the supplement was ambiguous and was not aware that the configuration was prohibited.
- Some later variants of the AS350 helicopter were approved to operate with the above door configuration up to an airspeed limit of 110 knots (the absolute ‘never exceed’ speed at sea level with all doors fitted and closed was 155 knots). Airbus Helicopters advised that one reason for this lower speed limit for variants approved to fly with the above configuration was to prevent air pressure differences applying excessive force to parts of the cabin. The pilot had removed the rear seat cushions from the cabin to eliminate the risk of their being blown out of the cabin and striking the main or tail rotor.
- The monsoon bucket was a ‘Cloudburst 1000’ model, a collapsible type with a capacity of 1,000 litres (1,000 litres of fresh water weigh 1,000 kilograms). It was attached to a strop approximately six metres in length, making a total underslung load length of approximately 10 metres below the helicopter hook. The bucket manufacturer advised that the complete bucket assembly weighed approximately 62 kilograms. The manufacturer did not state any airspeed limitations, but said feedback from operators was that an empty bucket flew well at speeds up to 100 knots. The maximum load permitted on the hook was 750 kilograms (AS 350 BA flight manual supplement number 12). The flight manual supplement for the hook gave an absolute airspeed limit of 80 knots when loaded, and contained a note stating: “The pilot is responsible for determining the limit speed according to the load and sling length”.
- The bucket was filled by lowering it into a dipping pond, or it could be landed and filled from hoses. The water drop valve was electrically commanded by a button on the pilot’s cyclic stick (the flight control that alters the tilt angle of the main rotor disc and thus the direction in which the helicopter flies). The valve was pneumatically (operated using air pressure) actuated by helicopter engine bleed air supplied through a detachable, flexible hose.
- The flight manual carried in the helicopter did not contain information on the Cloudburst bucket, and the operator was unable to provide its specifications. Therefore, the operator’s pilots did not have ready access to information necessary for calculating the operating weight when firefighting.
Meteorological information
- An automatic weather station was located on Sugarloaf, approximately 500 metres from the scene of the accident. The wind at the estimated time of the accident was from 273 degrees true (with reference to true north) (˚T), varying between 264˚T and 279˚T, with the speed between 20 and 29 knots.
- The other pilots operating in the circuit around Sugarloaf before the accident had noted a moderate to strong west to northwest flow with light turbulence, but it had not been a concern to them. However, the pilot of one of the first helicopters to respond to the accident said, “It was windy and a bit of a struggle in [a Kawasaki BK117]”.
- Approximately 85 minutes after the accident, the supervisor stopped helicopter operations in a fire sector three kilometres southwest of Sugarloaf because of reported wind shear (a change in wind speed and/or direction over a relatively short distance).


Survival aspects
- The helicopter was fitted with a 406-megahertz emergency locator transmitter (ELT). The ELT activated as a result of the impact, but it was not until 1533 (approximately one and a half hours after the accident) that the ELT signal was reported to Rescue Coordination Centre New Zealand. The rescue coordination centre advised that the detection was by a low-earth-orbit satellite only.
- The roof-mounted antenna had separated from the coaxial cable that connected it to the ELT. As a result, a very weak signal was being transmitted. Consequently, a satellite had to be in a low orbit and nearly overhead in order to detect such a weak signal.
- The Commission has noted in previous reports the poor reliability of ELTs and has made recommendations to the Director of Civil Aviation concerning the issue (for example, inquiry report 2011-003, in-flight break-up, ZK-HMU, Robinson R22, near Mount Aspiring, 27 April 2011). The Commission has also included the issue as a transport-related concern in its Watchlist (see https://taic.org.nz/watchlist/technologies-track-and-locate).
- The floor attachments for the pilot’s seat had failed in the heavy impact with the ground. The inboard lap belt had been forcibly pulled through its floor-mounted adjusting mechanism, leaving the pilot unrestrained. Although the other three points of the harness had remained firmly connected to the seat belt buckle, the disconnected lap belt resulted in the pilot being thrown from the cabin.
- The pilot had been wearing a helmet, but the impact forces were not survivable.

On-board video recording
- A digital video camera was mounted under the forward fuselage, on the helicopter centreline, aimed down and rearwards toward the monsoon bucket. It was attached to the bracket that supported the helicopter’s rear-facing mirror. The camera also recorded sound.
- The on-board video camera recorded all the flights on the day of the accident and the previous day. The camera had a clear view of the monsoon bucket in flight and when filling at the dipping pond, the front parts of the landing gear and the ground underneath the helicopter. The video recording enabled the normal in-flight behaviour of the bucket to be compared with its behaviour on the accident flight (see Figure 6).
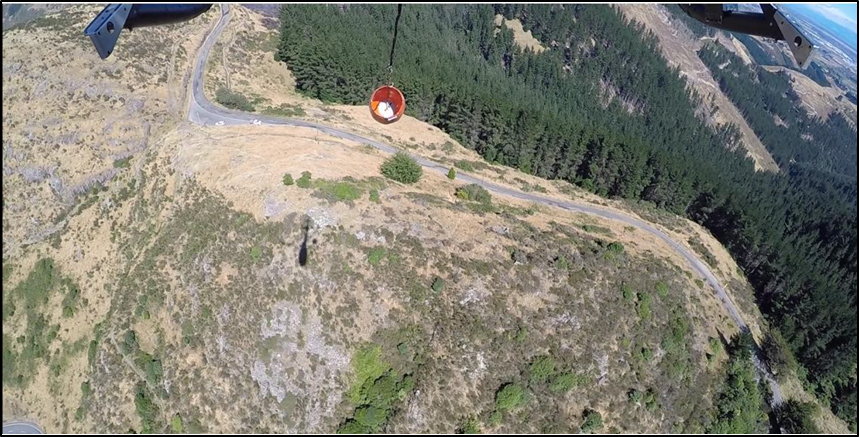
- The track flown, the height above ground, the groundspeed and the relative movement of the helicopter were estimated from the video (speed and direction were calculated using the time and distance between two clearly identified features).
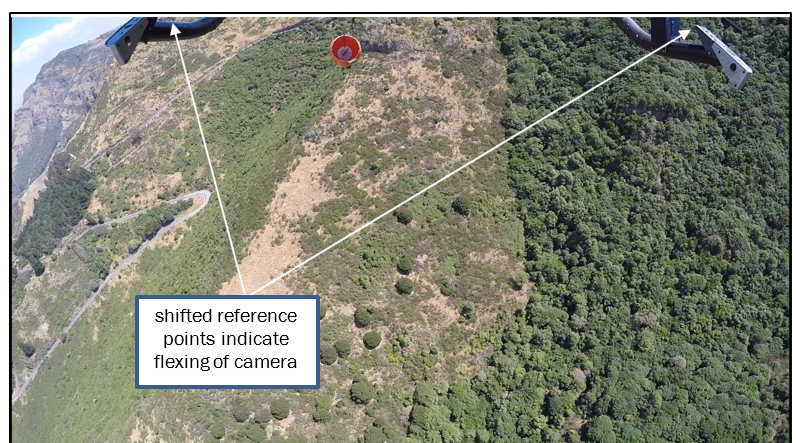
- Changes in the position of the video frame with reference to the landing gear indicated the relative movement of the camera as it flexed on its mount (compare Figure 5 and Figure 6).
- The on-board video data was sent to the BEA for further analysis of the images and sounds.
Organisational and management information
The operator
- The operator was certified under Civil Aviation Rules Part 119 to conduct commercial and charter operations. It had been performing commercial work in the Canterbury region since 2009, and operated multiple helicopter types.
- The chief executive was the operator’s chief pilot.
- Civil Aviation Rules Part 119 did not require helicopter operators to have drug and alcohol management systems, although the operator did have reference to such policies in its safety manual.
Firefighting operations
- Firefighting air operations are regulated by Civil Aviation Rules Part 91, General Operating and Flight Rules, and Part 133, External Load Operations. At the time of the accident the interaction of air operations with the rural fire authorities was covered by a New Zealand Standard – National Rural Fire Authority: Standard for use of aircraft at wildfires, RF300, first issued in August 2015.
- The standard required an air operator to apply to the National Rural Fire Authority for a certificate of compliance (with the standard) before the operator could be considered for tasking on a firefighting mission controlled by a rural fire authority. The application required a declaration by the operator of its compliance with the requirements of the standard (the general contractual provisions [see https://fireandemergency.nz/about-us/general-contractual-provisions] of Fire and Emergency New Zealand include requirements for contractors to: operate in compliance with applicable user requirements, specifications and standards; and perform the service using due diligence, care and skill, and with sufficient appropriately trained, qualified, experienced and supervised persons. Contractors are required to ensure that each service, prior to acceptance, complies with all New Zealand laws, codes and standards), and verification by a rural fire authority that the operator was experienced in aerial firefighting.
- On 30 September 2016 the operator had been issued with a National Rural Fire Authority Interim Certificate of Compliance for an Aircraft Operator. The interim status was for a period of 36 months from the date of issue, or until the operator had passed a formal audit by the National Rural Fire Authority, whichever was sooner. The audit had not yet been conducted at the time of the accident.
Previous incident
- In January 2015 a wildfire had occurred at Flock Hill Station near Craigieburn Forest Park in Canterbury. The fire had been on Department of Conservation land therefore the department had been responsible for fighting the fire.
- The pilot had assisted in the fighting of that fire over a number of days, flying a monsoon bucket with the same helicopter. During that task the window panel from the left rear sliding door had fallen from the helicopter.
-
The Department of Conservation rural fire officer in charge of the firefighting effort recalled that he had noted the missing window by chance, and that the pilot had told him that it had happened because he had been flying too fast. The rural fire officer had recorded the event on an incident reporting card, but no further investigation had been undertaken.
- At the briefing for all personnel the next day, the rural fire officer had referred to the loss of the window as “flying too fast” and reiterated to the pilots that their flying had to be ‘SEEL’ (safe, effective, efficient and bound by logistical limitations). The rural fire officer said that the incident had been included in the operational debrief held after firefighting activities were complete.
- The operator’s chief pilot/chief executive had been aware of this incident, but it had not been recorded in the internal quality assurance system and no internal investigation had been conducted. The operator had not notified the incident to the CAA, as required by Civil Aviation Rules Part 12: Accidents, Incidents, and Statistics. However, the maintenance logbook recorded that a new window had been installed on 30 January 2015.
- The pilot had logged approximately 75.5 hours of underslung-load operations, including firefighting, in the helicopter since the Flock Hill Station incident.
Analysis Tātaritanga
Introduction
- The accident occurred during a complex, large-scale, airborne firefighting operation. The firefighting command and control system was functioning as planned, with no significant issues reported. The other pilots in the Sugarloaf circuit reported that the winds, although gusty at times, had not compromised the safe operation of their helicopters.
- There had been no concern for the pilot’s performance during the day of the accident. No prior abnormalities were reported with the helicopter that day, and the on-board video recording appeared to show normal flight operations.
- The wreckage showed that the bucket suspension lines cluster had made contact with the tail rotor. The damage to the tail rotor blades and the subsequent separation of the vertical stabiliser caused the loss of control. The on-board video recording provided evidence that supported this conclusion.
What happened
Safety issue – There may not be a good awareness within the helicopter industry of the additional risks involved with underslung load operations, particularly with the use of monsoon buckets during firefighting operations.
- On the final circuit the pilot was returning to the dipping pond to refill the monsoon bucket. The on-board video recording confirmed that at all times while in cruise flight the helicopter height provided clearance between the monsoon bucket and the ground.
- The groundspeed of the helicopter when it crossed the rocky ridge south of Sugarloaf was estimated on the accident circuit, and several circuits beforehand, to have been between 80 and 90 knots. The door configuration in use at the time of the accident (two right-hand standard doors removed and the left-hand front and left rear sliding door closed) had not been tested by Airbus Helicopters for the AS350 BA variant, and for that reason the configuration was prohibited. Although other variants of the AS350 could operate safely with this door configuration, it was not possible without flight test data for the AS350 BA to determine the extent to which the airspeed was a factor in the loss of the window. The combined effect of air speed and turbulence is discussed in the following section.
- Shortly after the helicopter passed over the rocky ridge, the video recording showed slight transient movements in pitch and roll. A vibration went through the monsoon bucket and the strop, as had happened on previous passes over the ridge, and the tension in the suspension line relaxed. This time the bucket rose quickly until it went out of view of the camera. The bucket had also risen out of camera view at a similar place on some earlier circuits, but for less time.
- When the bucket moved out of camera view, the frame of the video recording in relation to the landing gear reference points changed (refer to paragraph 3.7.8). This was most likely the result of rearward pressure on the camera because of an increase in airspeed.
- The transient pitch and roll changes could have been made by the pilot. However, when considered with the apparent airspeed increase and the vibration of the suspension lines and strop, it was very likely that these were all signs of turbulence and wind shear.
- Although this had occurred at most other times during the numerous circuits when the helicopter had crossed the ridge, it was significantly more pronounced on the last circuit.
- The BEA analysis of the video recording identified a loud sound at this time. An abrupt increase in pitch attitude of the helicopter occurred shortly after the loud sound. Shortly afterwards, a second loud sound was heard, accompanied by a sudden and short-duration, high-frequency airframe vibration. The background sound, corresponding to the frequency of the tail rotor, then ceased.
- It is virtually certain that the second loud sound and the high-frequency airframe vibration occurred when the monsoon bucket and the tail rotor made contact. The tail rotor blades were largely destroyed by this contact.
- The source of the first loud sound and the relevance of the abrupt pitch change are discussed below.
Other objects seen in the video
- After the airframe vibration occurred, two airborne objects appeared below the helicopter very briefly (see Figure 8).

- Approximately four seconds later the vertical stabiliser assembly could be seen falling to the ground (see Figure 9).

- A close examination of the images of the left object (viewed in the camera direction) determined that the object appeared to be light weight, of rectangular form, and highly reflective (see Figure 10). The object’s brightness varied frequently because it was tumbling.

- It is virtually certain that this object was the missing window panel. Although the window was transparent, it was tumbling and appeared bright when it reflected the sun and was invisible when edge on.
- The door configuration meant that the window was likely subjected to fluctuating pressure as the helicopter encountered turbulence and wind shear while flying at the estimated 80-90 knots. It is very likely that the window panel was dislodged from the door by a sudden increase in air loading due to turbulence or a change in airspeed. The first loud noise in the video sound analysis was very likely the window being dislodged.
- The dislodging of the window would have caused a sudden change in airflow through the cabin and an increase in noise and a sharp sound. This would have been of immediate concern to a pilot. It would be typical for a pilot to instinctively reduce speed under such circumstances. In a helicopter the speed is reduced by moving the cyclic aft, called a ‘flare’ manoeuvre, which pitches the nose up (and the tail down). This pitch change was discernible in the video recording after the first loud sound, and corresponded with what the witness at Governors Bay (refer to paragraph 3.1.8) reported seeing just before the helicopter crashed.
- At the same time that the tail was lowering, the monsoon bucket was rapidly rising from the transient airspeed increase. The convergence resulted in cables from the strop entering the tail rotor disc, causing the damage that resulted in the pilot losing control of the helicopter.
- The need to abruptly flare a helicopter with an underslung load is unusual. The Commission considered other reasons for the pilot making an abrupt pitch-up.
- One reason could have been a ‘startle effect’ following the window suddenly dislodging. The level of surprise or startle that a pilot might experience when something unexpected occurs could be significant. Startle can be detrimental to their handling of the event. Simons (1996) suggests that when people are subjected to some sort of startling stimulus when a real threat exists, the intensity of that startle is increased (the Effects of Startle on Pilots During Critical Events: A Case Study Analysis. Wayne L Martin, Patrick S Murray, Paul R Bates, Griffith University, Brisbane, Australia 2012). The pilot’s experience in firefighting environments would likely have made him less susceptible to this reaction. It was not possible to determine whether the ‘startle effect’ was a factor in this accident.
- Another reason could be that the pilot made an avoiding manoeuvre for some reason, such as to avoid a bird.
- The object seen to the right in the video recording appeared to be small and animated, with an irregular shape (see Figure 11). This object went out of view for a few frames then reappeared briefly.

-
It is very unlikely that this object was a section of tail rotor blade, because it came from ahead of the helicopter. The object was more likely to have been a bird, as the motion resembled the flapping of a bird’s wings.
- Although the normal response of a pilot to avoid a head-on collision with a bird would be to pitch up, the bird did not come into view until after the pitch-up. The time interval, and the distance below the helicopter when the object passed, suggests that the pitch-up was not a collision-avoidance manoeuvre. However, the possibility that the pilot was manoeuvring to avoid something could not be excluded.
Window installation
- The maintenance instructions for the helicopter specified that the window panel was to be held in the door aperture by a ‘Z’-shaped rubber seal around its edge. A line of sealant placed around the seal lip prevented moisture ingress and helped to keep the window centred. The manufacturer said that the sealant helped to maintain the window in place under flight loads, although its tests and analyses were performed without the sealant.
- The installation instructions specified that the rubber seal was to be fitted to the door so that the window panel was located on the inside of the door profile, and the edge of the window panel overlapped the edge of the aperture in the door by at least three to six millimetres. This design was to prevent the window panel being accidently dislodged and falling outwards from the door. The design would not have prevented the window falling inwards in the event of it being dislodged.
- However, as the window panel was not found, the overlap dimensions and whether any sealant was on the window panel could not be determined.
- The helicopter manufacturer advised of a similar occurrence in Europe in 2002, when a window panel fell out of a rear door. The main rotor blades were damaged in the incident. That investigation determined that the window had very recently been installed incorrectly, using soapy water to aid installation.
Strop length
- The pilot was flying with a shorter strop than those that most of the other helicopters were using that day. There were advantages or disadvantages to using a short strop, but there was no evidence to show that a short strop was more dangerous than a longer one. Industry advice was that strop length was determined largely by a pilot’s preference. Although a longer strop would have resulted in the bucket suspension cable cluster trailing farther behind the tail rotor, any contact of the strop itself with the tail rotor could have had similar consequences.
Operator procedures
Safety issue – The operator did not have adequate systems available for the pilot to determine the actual all-up weight and balance of the helicopter for the firefighting operation, or to ensure that incidents such as the previous loss of a window were recorded, notified to the CAA and investigated.
Weight and balance
- The on-board video recording showed that the pilot filled the 1,000-litre bucket to capacity each time it was dipped into the pond. He had no reliable means of filling the bucket only to the 750-kilogram load limit for the hook. A line had been painted inside the bucket, but it had faded. The line was not visible on the video recording and it is unlikely that the pilot could see it clearly. Although the pilot had the option of subsequently releasing some water by briefly opening the bucket valve, video evidence showed that it was virtually certain that the initial part of each circuit began with the bucket weight exceeding the hook load limit.
- The capacity of the bucket allowed an opportunity for the hook load limit to be exceeded; this ought to have been recognised as a risk when planning for the task. There are buckets available that have removable bungs in their walls, so that the capacity can be restricted.
- The right doors had been removed for the firefighting mission, but that was a prohibited configuration for the AS350 BA helicopter. It is very likely that the configuration had been considered acceptable because it was permitted on some other AS350 variants. However, operating limitations often differ between similar variants of an aircraft. Operators and pilots must know and adhere to the limitations published in the applicable flight manuals.
- The cabin had been stripped of seats and loose items to eliminate the risk of an object falling through the open doors and hitting the main rotor or the tail rotor. This would have reduced the empty weight of the helicopter. However, the operator had not provided a revised weight and balance sheet for this different empty configuration.
- As there was no flight manual supplement for the Cloudburst bucket, the weight of the bucket and attached lines was not readily available to pilots.
- The helicopter was recovered with an estimated 25% of fuel capacity on board. The maximum all-up weight with an external load was 2,250 kilograms. This weight could be reduced to that at which an out-of-ground-effect (Hovering close to the ground normally results in a positive influence on lift characteristics of the helicopter’s main rotor therefore more power is required to maintain a hover out of ground effect) hover could be maintained. The weight of the helicopter on the accident flight was not ascertained accurately because of the above variables. However, the weight very likely exceeded the flight manual limit whenever the bucket was filled to capacity.
- It could not be determined whether the pilot had calculated the revised weight and balance for the configuration and the actual underslung load.
- In its report on a heli-skiing accident on Mount Alta in 2014 (Commission report AO-2014-005, Eurocopter AS350-B2 (ZK-HYO), collision with terrain during heliski flight, Mount Alta, 16 August 2014), the Commission had raised the safety issue of New Zealand helicopter pilots working in a culture of operating outside the manufacturers’ published and placarded ‘never exceed’ limitations, including the maximum allowable weight limitations. The Commission had recommended that the Director of Civil
- Aviation include the safety issue of helicopter operational culture in its current ‘sector risk profile’ review.
- Although the monsoon bucket was empty at the time of this accident, and therefore overloading was not a factor contributing to the accident, the helicopter was very likely overloaded each time the monsoon bucket was filled at the dipping pond.
Non-reporting of previous incident
- The loss of the window panel during the 2015 Flock Hill Station fire met the criteria of an occurrence that should have been notified to the CAA, in accordance with Civil Aviation Rules Part 12. This is specified in CAA Advisory Circular AC 12-1 Mandatory Occurrence Notification and Information Appendix A – Aircraft Systems Incidents.
- A strike on the tail rotor by the window panel had the potential to cause significant damage to the tail rotor. Therefore, the window panel entering the airflow along the right side of the helicopter in forward speed could present a hazard to the safety of the helicopter.
- In accordance with Civil Aviation Rules Part 12, the operator was required to notify this occurrence to the CAA and provide a report on its investigation of the incident. The non-notification of this event meant that follow-up by the CAA and the wider dissemination of any safety lessons could not occur.
- The Civil Aviation Rules also required that the operator establish an internal quality assurance system that included, in part:
- a safety policy and safety policy procedures, including the procedure for occurrence investigations conducted in accordance with Part 12; and
- a procedure to ensure quality indicators, including defect and incident reports, and personnel and customer feedback, are monitored to identify existing problems or potential causes of problems within the system; and
- a procedure for corrective action to ensure existing problems that have been identified within the system are corrected; and
- a procedure for preventive action to ensure that potential causes of problems that have been identified within the system are remedied.
- The fact that the 2015 Flock Hill Station fire window loss had not been investigated by the operator, or notified to the CAA, was a missed opportunity for the operator to understand the circumstances and take preventive action.
Substance use
- The Commission regards the use of recreational drugs by active pilots as a significant safety concern. Trace evidence of cannabis use was found in the toxicological analysis of samples taken from the pilot. The expert forensic toxicologist was of the opinion that the pilot was ‘unlikely’ to have been under the influence of cannabis at the time of the accident.
- Therefore, substance use is very unlikely to have been a factor contributing to this accident. However, as pilots may not know when they will be next required for duty, and the short- and long-term effects of cannabis use are variable, the use of cannabis at any time poses a serious risk to aviation safety. While not causal, substance use is part of the circumstances of this accident that the Commission believes has significant implications for transport safety.
- The regulatory environment for preventing performance impairment through substance use is currently on the Commission’s published watchlist. The stated problem is that judgement, decision-making, and reaction time can all be affected by the use of drugs or alcohol. The use of performance-impairing substances by persons performing safety critical tasks in a transport environment is a significant risk.
- In its Medical Information Sheet CAA MIS 013, the CAA describes recreational drugs as “having a wide range of effects, and different people can respond / react to them in varying and different ways. In general terms the effects that are of aviation safety concern include:
- Changes to mental function, thinking, and decision making;
- Changes to the sensory functions of the body;
- Reduction in co-ordination and physical performance;
- Potential for incapacitation; and
-
Changes to behaviour.
Some of these effects can occur because of the drug itself, and some can occur afterwards (like a hangover), or because of withdrawal from the drug”.
- In a previous report (Aviation inquiry 12-001, hot-air balloon, collision with power lines and in-flight fire, near Carterton, 7 January 2012), the Commission had recommended that the Secretary for Transport complete, as a matter of priority, all necessary work that will support the introduction of appropriate legislation or rules that will:
- prescribe allowable maximum levels for alcohol
- prohibit persons from operating an aircraft, vessel or rail vehicle if they are impaired by drugs
- require operators to implement drug and alcohol detection and deterrence regimes, including random testing
-
prescribe post-occurrence testing requirements for drugs and alcohol.
This legislation or these rules should apply:
- across the aviation, maritime and rail transport modes
- to persons operating an aircraft or a marine craft for recreational purposes. (012/13)
- In 2015, noting several other cases where performance-impairing substances had been detected in persons in transport safety-critical roles, the Commission had published its Watchlist on substance abuse.
- The Watchlist item ‘Substance use: regulatory environment for preventing substance impairment’ described the Commission’s concern about the lack of effective regulation against substance use by persons performing transport safety-critical tasks in a transport environment.
- The CAA has since advised that air operators will be expected to include drug and alcohol policies in their safety management systems. The policies shall have provisions for random and post-incident testing of persons in safety-critical roles. The CAA specified in Advisory Circular AC100-1, Safety Management, that all operators should have their safety management systems approved by 1 February 2021.
- The operator in this case had yet to establish an approved safety management system but did have a drug and alcohol policy and a policy for random or post-accident and -incident drug and alcohol testing in its safety manual. The chief pilot was not aware of the pilot’s occasional cannabis use and said that the pilot had never presented under the influence at work. Random drug and alcohol testing had not been conducted.
- On his application for a CAA medical certificate (in this case, regarding the use of recreational drugs or substances. See paragraph 3.2.10) the pilot had declared that he had no experience of recreational drugs. The Commission examined the issue of pilots not declaring their use of performance-impairing substances in a 2015 inquiry involving a fatal helicopter crash near Queenstown (Report AO-2015-002R, Mast bump and in-flight break-up, Robinson R44, ZK-IPY, Lochy River, near Queenstown, 19 February 2015), although in that case the use had been for a medical condition.
- As a result of that inquiry the Commission had recommended that the Director of Civil Aviation review the medical certificate application process to ensure that it promoted a positive reporting culture for applicants (recommendation 021/17).
-
The Director had replied:
The CAA accepts… this recommendation and will do what it can to promote a “positive reporting culture” for medical certificate applicants to the degree it can do so while still acting decisively to protect the public interest when it has reasonable cause for concern about matters of potential aeromedical significance. The CAA will review current processes in line with this recommendation by 1 December 2017.
- This recommendation had been directed at improving the full disclosure of medical conditions. The effectiveness of the process remains heavily reliant on an applicant’s full disclosure.
-
However, a limitation of the disclosure system is that pilots are unlikely to disclose that they use recreational drugs if they fear that in doing so they risk losing their medical certificates, and thus the privileges of their licences.
- The CAA had advised before report AO-2015-002R was published that it had completed a review of the medical certificate application process, as recommended by the Commission in that inquiry, and potential policy changes were under consideration.
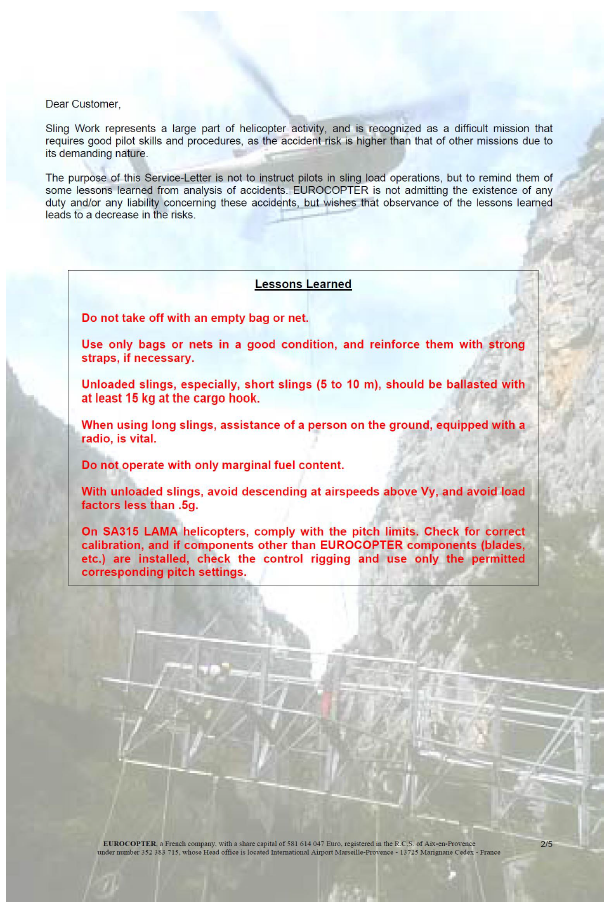
Appendix 1: Eurocopter Service Letter No. 1727-25-05
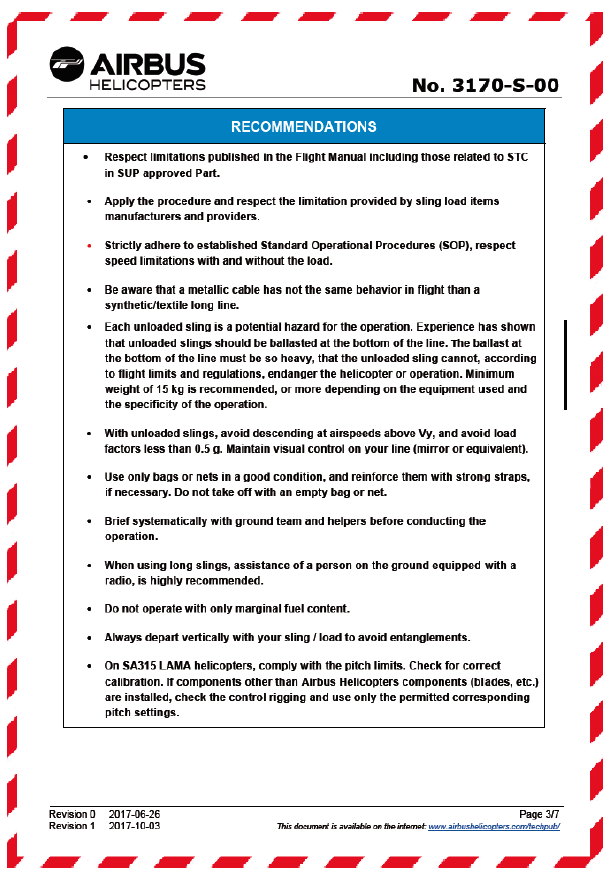
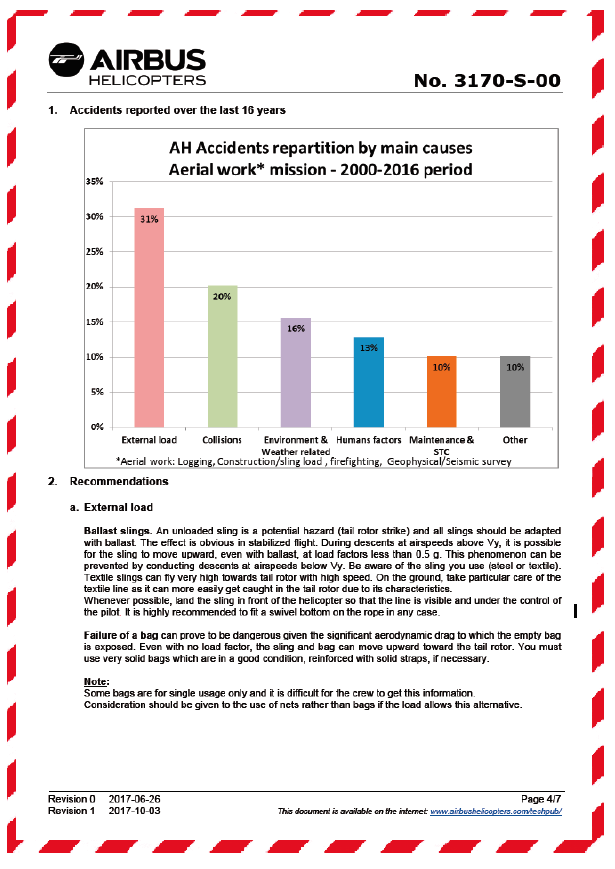
Appendix 2: Airbus Helicopters Safety Information Notice No. 3170-S-00