A Pacific Aerospace Limited 750XL aeroplane was being used for tandem skydiving from Taupō aerodrome. During the climb, a turbine blade in the single engine failed. The pilot put the aeroplane into a glide and all on board bailed out and landed without serious injury. With nobody on board, the aeroplane crashed into Lake Taupō and was destroyed.
Executive summary Tuhinga whakarāpopoto


- On 7 January 2015 a Pacific Aerospace Limited 750XL aeroplane was being used for tandem parachuting (or ‘skydiving’) operations at Taupō aerodrome. During the climb on the fourth flight of the day, the Pratt & Whitney Canada PT6A-34 engine failed suddenly. The 12 parachutists and the pilot baled out of the aeroplane and landed without serious injury. The aeroplane crashed into Lake Taupō and was destroyed.
- The engine failure originated from a fatigue crack in a compressor turbine blade. The failed blade was one of a set of overhauled blades that had been installed 1,127 flight hours before the accident flight. The inspection interval for overhauled blades was 3,000 hours.
- The turbine section of the engine had been inspected during scheduled maintenance 87 flight hours before the accident. The recommended procedure was to inspect both sides of the compressor turbine blades for any cracks, but it was very likely that only one side was inspected. It was not determined whether the fatigue crack existed and might have been visible at the time of that inspection.
- It was fortuitous that none of the parachutists or the pilot landed in the lake. Although each tandem rider was wearing a lifejacket, the tandem masters would have had to rely on the buoyancy of their un-deployed main parachutes to stay afloat. The pilot had no flotation device.
- The following safety issues were identified during the inquiry:
- the measurement specifications for overhauled compressor turbine blades that had been through a strip and recoat repair process were not exactly the same as those for new blades. Blades that had been through that repair process, without verification of critical dimensions, might fail before the next 3,000-hour inspection
- when aircraft maintenance staff do not refer to the current Instructions for Continuing Airworthiness for a task, perhaps because they are very familiar with the basic task and do not know that the task documentation has changed, safety might be compromised
- parachute drop pilots were not required to wear lifejackets or flotation devices if their flights were expected to remain within gliding distance of land. That scenario downplayed the possibility of a pilot having to ditch an aeroplane or having to use the emergency parachute when over or near water.
- The failed blade and two others sampled from the set were undersize in some dimensions, compared with new blades. The size discrepancy likely contributed to the fatigue failure. As a result of this occurrence, Pratt & Whitney Canada amended the measurement specifications for the acceptance of blades that had been through a strip and recoat repair process to better reflect the criteria for new blades in the trailing edge area.
- Pratt & Whitney Canada and Pacific Aerospace also reviewed the contemporary operation of the 750XL aeroplane and PT6A-34 engine in the skydiving role against their original design assumptions. They found that, on average, operators were using higher engine power settings more frequently and for longer periods than had been assumed. As a result of these findings, Pratt & Whitney Canada will introduce an additional scheduled inspection for PT6A-34 engines that are used in single-engine installations.
- The aeroplane operator (Skydive Taupo Limited) had maintained the engine in accordance with a maintenance programme that was a recognised alternative to that of Pratt & Whitney Canada. The operator had not completed the registration process with the programme supplier, but neither this oversight nor the alternative maintenance programme was a factor in the engine failure.
- The pilot did not follow the operator’s recommended procedure for baling out, which put himself and others at risk of serious injury. To reduce the likelihood of this hazard, the operator improved the emergency procedures training given to its pilots.
- The Transport Accident Investigation Commission made a recommendation to Skydive Taupo to investigate options for equipping its parachute drop pilots with effective flotation devices.
- The key lessons arising from this inquiry were as follows:
- operators and pilots engaged in skydiving operations should assess carefully the risk of having to use an emergency parachute or landing in water, and ensure that they have the appropriate training and equipment. Pilots must have a thorough understanding of the care and use of emergency parachutes, as their lives depend on them
- aircraft maintenance engineers should not commence any task related to airworthiness without ensuring that they have the current procedure and information necessary for the task
- operators and maintenance providers should ensure that they comply fully with any registration or other requirement of approved supplemental type certificates.
Factual information Pārongo pono
The accident flight
- On Wednesday 7 January 2015 a Pacific Aerospace Limited 750XL aeroplane, registered ZK-SDT (the aeroplane), was being used for commercial skydiving at Taupō aerodrome. The skydiving operator held an air operator’s certificate issued by the CAA under Civil Aviation Rules Part 115, Adventure Aviation.
- The day was fine with light winds. The air temperature was 22OC and the sea level pressure 1,018 hectopascals. At approximately 1215 the aeroplane departed with six tandem pairs and a pilot (the pilot) on board (a tandem pair in a parachute jump comprises the tandem ‘master’, who wears the parachute and has complete control of the jump, and a ‘rider’ whose harness is connected to that of the tandem master by four clips during the actual jump). This was the fourth flight that day, all of them flown by the same pilot. The operator’s records showed that the weight and balance for all of the flights were within the flight manual limits.
- After take-off from runway 17, the aeroplane climbed straight ahead along the shore of Lake Taupō. When the aeroplane was approximately 2,100 feet (ft) above the lake (the Taupō aerodrome is 1,335 ft above mean sea level, approximately 160 ft above the lake elevation of 1,172 ft. Imperial units are still used for vertical distances in civil aviation), a loud bang came from the engine and sparks emitted from the engine exhaust. The propeller stopped quickly. The pilot shut down the engine, put the aeroplane into a glide and broadcast a ‘Mayday’ radio call.
- The tandem master who was seated nearest to the pilot quickly assessed that baling out would be safer for the parachutists than a forced landing, and shouted “Get out!” Each tandem master then had to ensure that they were attached correctly to their rider before they shuffled to the cabin rear door and baled out.
- The pilot looked in the cockpit rear-view mirror that showed the cabin interior. Sure that all the tandem pairs had baled out, he then exited through the cockpit door adjacent to his seat. However, two parachutists were still on board.
- The last tandem pair was about to exit when the tandem master saw parachute lines obstructing the exit. He hesitated, and saw the pilot hit the top of the wing, forward of the cabin door, then fall away. The parachutists then left the aeroplane.
- All of the occupants landed on dry land by the lake shore, with two receiving minor injuries.
- The aeroplane struck the water at high speed, approximately 150 metres offshore and six kilometres from the aerodrome. It broke into four main sections: the engine and propeller, the fuselage with the left wing attached, the right wing, and the tail.
- Other pilots heard the Mayday call and many witnesses saw the accident. As a result, emergency services were notified promptly.
Personnel information
The pilot
- The pilot held a current commercial pilot licence (aeroplane), issued in 2011, and a valid Class 1 medical certificate with no conditions, restrictions or endorsements. He had nearly 600 hours of flying time, including 14 hours on the 750XL.
-
The pilot had had some initial training on the 750XL in November 2014, during which time he had been issued with a parachute drop pilot rating (Civil Aviation Rule 91.705(a) required the pilot in command of an aircraft performing a parachute drop operation to hold a parachute drop pilot rating issued under Civil Aviation Rules Part 61). The drop rating was not specific to an aircraft type.
- The chief pilot of the operator had hired the pilot on 5 January 2015. Over the next two days, the pilot had flown six hours of skydiving flights as pilot-in-command under the supervision of the chief pilot. On 6 January 2015 the pilot had been issued with a 750XL type rating and completed an initial crew competency check with the operator.
-
The engine failure occurred on the fourth flight of the pilot’s first day of flying without direct supervision.
Tandem masters
- The operator employed tandem masters with a minimum of 750 parachute descents. The six tandem masters on the accident flight had individual experience of between 3,800 descents and 10,000 descents.
Aircraft information
- The Pacific Aerospace 750XL aeroplane is manufactured in New Zealand. It was certificated by the CAA in 2003, initially for the skydiving role, carrying up to 17 individual parachutists (refer to 750XL flight manual Supplement 5, Installation of Parachuting Kit). More than 100 of the type have been manufactured in skydiving, utility, agricultural and passenger versions.
- The aeroplane met the United States Federal Aviation Regulations Part 23, Airworthiness Standards for “normal, utility, acrobatic and commuter category airplanes”. There were no requirements in those standards that concerned ditching (to ditch is to make an emergency landing of an aircraft onto water). The aeroplane flight manual warned that “the ditching characteristics of the aeroplane [were] unknown” (Pacific Aerospace Limited, pp. 3-15). The only known ditching of a 750XL had had a fatal outcome (CAA aircraft accident report 03/3794, ZK-UAC, Pacific Ocean, 26 December 2003).
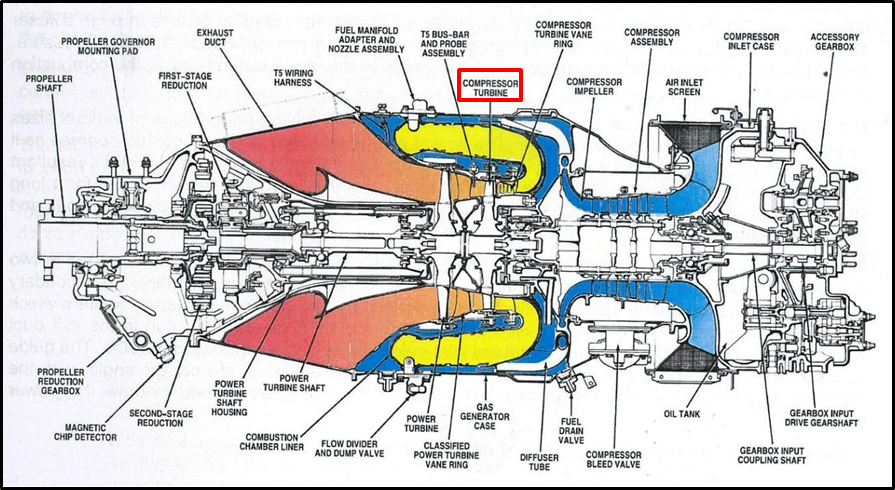
- The standard engine is the P&WC PT6A-34 turboprop (see Figure 1). The airflow through the engine is from back to front. The air passes through a four-stage compressor section, is combined with fuel and burnt in the combustion chamber. The combustion gases pass through two turbines. The first is the compressor turbine, which drives the compressor section and the accessories gearbox at the rear of the engine. The second turbine is the power turbine, which drives the propeller through a reduction gearbox.
- The accident aeroplane had been manufactured in June 2005 in the agricultural version. The operator had acquired it in 2009 and had it converted for skydiving. The operator had replaced the originally installed engine with another PT6A-34 that had an operational and maintenance history known to the operator. This engine had been manufactured in August 2002.
- The previous scheduled maintenance was a 150-hour/400-hour maintenance check carried out between 30 November 2014 and 9 December 2014.
Alternative engine maintenance programme
- The engine had been maintained, initially, in accordance with the P&WC Maintenance Programme, which specified 4,000 hours between engine overhauls. In November 2009 the operator had purchased the right to use a supplemental type certificate (STC) (a supplemental type certificate is a certificate that allows changes to: a type certificate category or type acceptance certificate category; the type design; the flight manual; the operating limitations; and any special conditions prescribed on the type certificate or type acceptance certificate) of MORE® Company Inc (MORE) of the United States as the engine maintenance programme (The Federal Aviation Administration had first approved STC number SE00002EN in 1994. The STC had been re-issued on 6 March 2009).
-
MORE described the benefits of its programme as follows (MORE Company Inc., 2004, p. 9):
The MORE® Instructions for Continued Airworthiness use the P&WC maintenance manual as a foundation and then add several additional inspection methods: periodic borescope inspection of the hot [turbine] section, periodic inspection of the compressor and exhaust duct areas, periodic Power Plant-Adjustment/Test (to monitor engine performance), periodic spectrometric oil analysis, periodic oil filter debris analysis, periodic vibrational analysis, etc.
The purpose of this aggressive inspection system is to find problems in their early stages … Early correction of engine problems will lead to an increase in engine durability, an increase in engine longevity, and an increase in engine safety; which in turn will allow an increase in the engine overhaul interval and long term cost savings to the operator.
- The MORE programme superseded or added to some P&WC requirements for turbine (or ‘hot section’ (a hot section is the turbine section (or ‘module’) of a gas turbine (‘jet’) engine) inspection and overhaul intervals (namely P&WC Service Bulletins 1303, 1403, 1703 and 1803), but did not extend the turbine and compressor service lives, which remained at 8,000 hours (as specified in P&WC Service Bulletins 1002 and 1302). The MORE Instructions for Continued Airworthiness included the following inspections, among others:
- oil filter debris analysis and oil sample analysis every 150 hours
- borescope inspection of the hot section and propeller balancing every 450 hours.
- An operator that wished to maintain an engine under the MORE programme would purchase the right, following which MORE would provide a customised maintenance programme manual. The manual explained the registration process that the operator should complete within 30 days. Part of the process was a detailed ‘initial entry inspection’ of the engine. A registration was not completed and the STC could not be used until MORE sent the operator a certificate.
- The United States considered a change to a maintenance programme to be a major modification. The MORE initial entry inspection checklist included a requirement to submit a Form 337, with details of the modification, to the aviation regulator, the Federal Aviation Administration. The CAA had a similar requirement and used the same form number for advising major modifications.
- When the operator purchased the STC in 2009, it did not complete the registration process within the required 30 days. The initial entry inspection of the engine had been completed on 30 November 2011, but the inspection checklist noted against the Form 337 requirement, “Not yet done. Await owner to get aircraft on maintenance programme with CAA”. The CAA had no record of having received the Form 337. MORE had not been sent the required documents and no certificate had been issued for the engine. No-one at the operator or MORE recognised this until after the engine failure.
- Although the MORE registration had not been completed, the operator complied with all of the programme’s inspection tasks and schedules as if it had been. There had been no revisions to the programme between the assumed registration in 2009 and January 2015. The required inspections and oil analyses had not shown any abnormal engine wear or trend.
- Between the initial entry inspection on 30 November 2011 for the MORE ® programme and 7 January 2015 the aeroplane had flown 2,250 hours.
Compressor turbine overhaul
-
P&WC Service Bulletin 1403 required inspections of compressor turbine disks and blade sets at the following intervals:
(a) Compressor turbine disk with full set of new blades installed at last shop visit, inspect within 5,000 hours.
(b) Compressor turbine disk with full or partial set of previously run compressor turbine blades installed, inspect within 3,000 hours since last compressor turbine blade inspection.
- The turbine inspection process required the replacement of the blades with a set of new or overhauled blades. The overhaul process included cleaning and inspecting the blades using non-destructive methods, checking for blade stretch (usually referred to as creep) and the sacrificial (destructive) testing of two blades from the set. The set would be scrapped if the sacrificial blades failed the test. Otherwise, blades that met the inspection criteria could be re-used without further work (P&WC advised that there was no life limit for compressor turbine blades). If repair were required, the protective thermal coating would be stripped, the repair carried out, and a new coating applied.
- In compliance with the above service bulletin, the compressor turbine module was removed for inspection in May 2013 at 4,974.25 engine hours since new. The module and associated components were sent to an approved engine overhaul facility in Australia, along with a replacement set of 56 overhauled compressor turbine blades to be installed after the inspection (the compressor turbine assembly had 58 blades. Two blades from every set sent for inspection and overhaul were sacrificed for metallurgical analysis as part of the overhaul process. Therefore, two new blades were added to the set when it was returned).
- The replacement blades (part number 3120751-01) had been obtained from an approved New Zealand supplier. That company had obtained them from a company in the United States that was the only facility approved by P&WC to overhaul compressor turbine blades. The blades had the appropriate Authorised Release Certificate from the United States (Federal Aviation Administration Form 8130-3).
- The Australian facility installed the 56 overhauled blades and two new blades into the turbine disk, and issued the appropriate Authorised Release Certificates for the work done.
- The operator’s maintenance provider had reassembled the turbine module and reinstalled the engine into the aeroplane. The aeroplane had returned to service on 22 May 2013.
-
The overhauled turbine blades had operated for 1,127.9 hours before the engine failed on 7 January 2015.
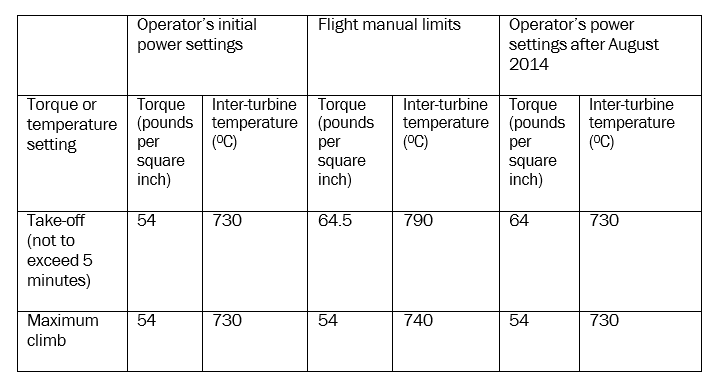
Table 1. Operator’s power settings compared to flight manual limits
Recorded data
- No flight data recorder was fitted to the aeroplane, nor was one required to be fitted.
- A GPS tracking unit was installed in the aeroplane to record the aeroplane’s position, course, speed and altitude. Every 25 seconds the current data was sent as a mobile phone text message to the operator’s base. The retrieved data matched the pilot’s recollection of the flight path on the accident flight.
- An optional data acquisition alarm monitor, which recorded some engine parameters such as torque and turbine temperature, was installed in the aeroplane. A display on the cockpit instrument panel provided visual and aural alerts in the event of a parameter exceedance. The pilot said there was no alarm during the accident flight.
- The memory module of the data acquisition alarm monitor was mounted on the forward face of the engine firewall. The module was found, but the crash had dislodged the memory chip, which was not found.
- The operator had downloaded the recorded engine data periodically to monitor the engine condition and performance trends. A separate investigation by the CAA after the accident found that the operator had not been using the system effectively to enable reliable trend monitoring (CAA Safety Investigation Unit, Aircraft Accident, ZK-SDT Pacific Aerospace 750XL, Taupo, 7 January 2015). As a result, the maintenance provider amended its procedures and training.
- The flight manual noted that the electronic Ng (Ng is the revolutions per minute of the compressor section of the engine) display also stored the peak value of Ng since electrical power was last applied. The engine instruments that were of the same design were sent to their manufacturer in the United States (Electronics International) to recover the stored data. No useful data was obtained. The instrument manufacturer later advised that the instruments took a ‘snapshot’ of data at pre-set time intervals, and a parameter was only recorded as the peak value if its value at that time was greater than the previous peak for three seconds or longer. A peak value was not necessarily an exceedance of a flight manual limit. The instruments did not record parameter values at the time they lost electrical power. Pacific Aerospace was advised of this corrected information.
Medical and pathological information
- The operator had a drug and alcohol policy as required by Civil Aviation Rules Part 115, Adventure Aviation. That policy required the responsible manager to consider the need to test crew members after any incident. In this case the manager decided that the tandem masters could not have contributed to an engine failure, so they were not tested.
- The manager tested the pilot for alcohol immediately after he arrived back at the aerodrome. The test was negative. A person certified for drug screening and collection tested the pilot later that day. That test was negative.
Tests and research
- Between 10 March and 11 March 2015 the engine was examined at the P&WC plant in Canada under the supervision of the accredited representative of Canada. There was no sign of foreign object damage to the engine, or of pre-impact thermal stress in the turbine (‘hot’) section. The damage was consistent with the engine having been not rotating at impact.
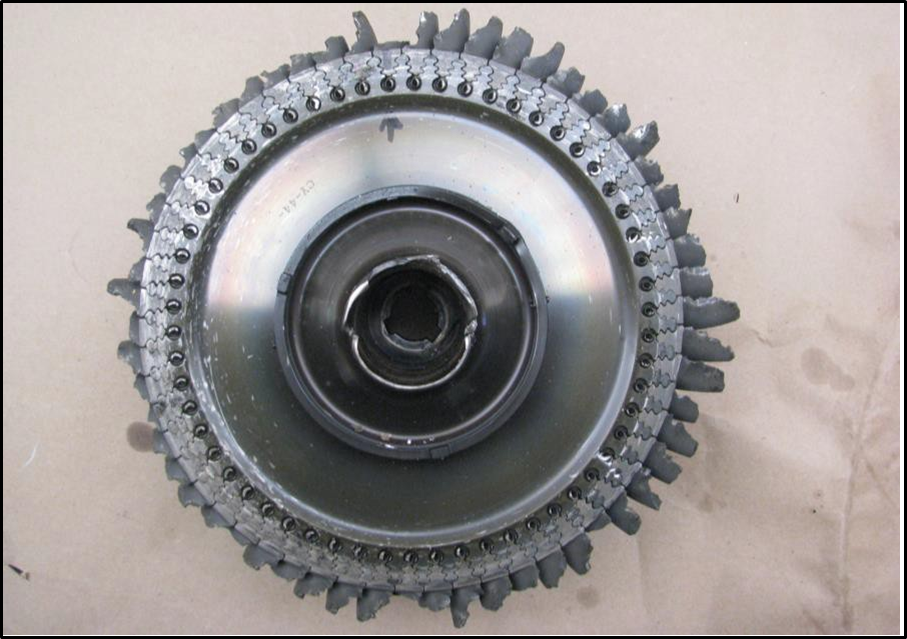
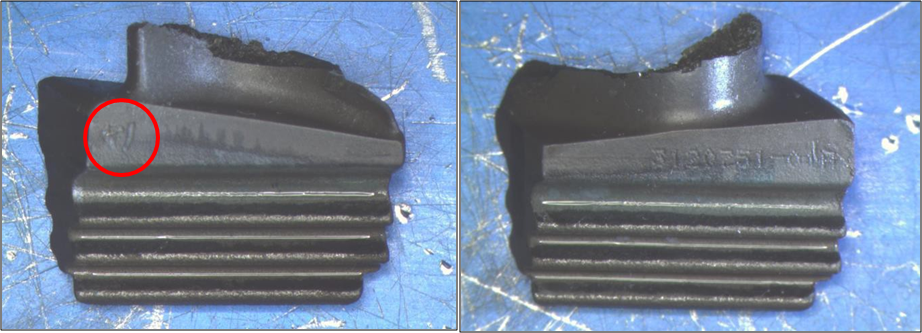
- All of the blades of both turbines were fractured. A visual examination identified one compressor turbine blade that was suspect (the arrowed blade in Figure 2), because it had a relatively flat fracture surface. The mark ‘R1’ (reworked once) on the platform of the blade showed that it had been stripped and recoated previously (see Figure 3). Therefore it was very likely that the blade (and the others in the replacement set) had been in service for at least 6,100 hours (this figure is the nominal 5,000-hours’ inspection interval for new blades plus the 1,128 hours since this blade set had been installed during the May 2013 compressor turbine module overhaul). Turbine blades are not identified individually and can be re-used as long as they meet the inspection/repair acceptance criteria. The total time in service for the blades was not determined.
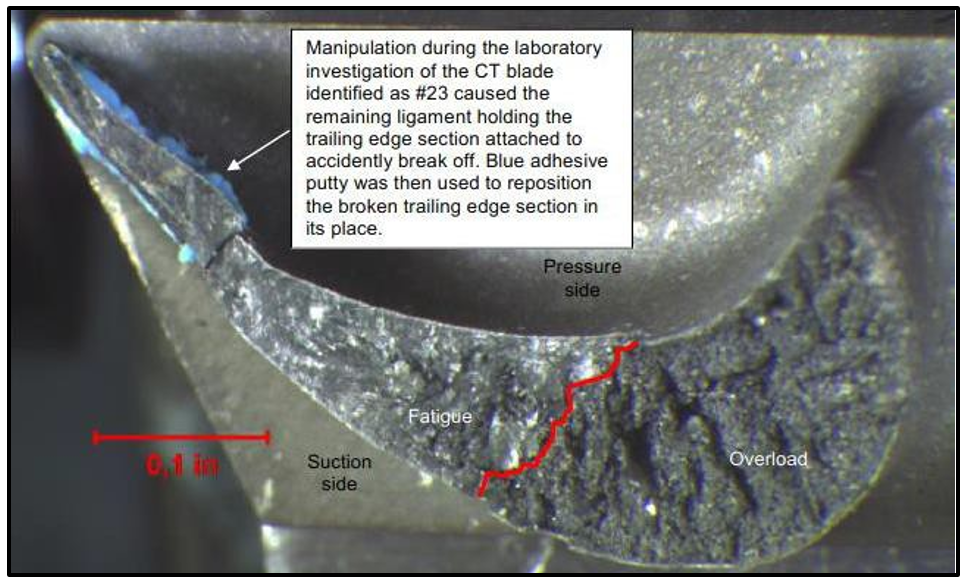
- A microscopic examination found that the fracture surfaces of all of the compressor turbine blades, except the suspect blade, were characteristic of overload. The fracture surface of the suspect blade had two distinct zones: one characteristic of fatigue towards the trailing edge; and one characteristic of overload (see Figure 4). There was no metallurgical anomaly in the trailing edge zone that could have initiated the fracture.
- The trailing edge radius of the suspect blade was less than the dimension specified for a new blade. Measurements of other blades from the set found that “potentially other blades from the overhauled blades had under minimum [trailing edge] thickness and/or [trailing edge] radius” (P&WC, 2015).
-
The examination determined that the engine failure was initiated by the fracture of a compressor turbine blade. The P&WC investigation report said, in part (P&WC, 2015, p. 30):
One compressor turbine blade fractured by fatigue initiating at the trailing edge tip of the [blade], propagating towards the leading edge until final fracture by tensile overload.
The under minimum trailing edge radius may have contributed to the fatigue crack initiation.
- The compressor turbine blades were overhauled at an approved United States facility that was an associated company of P&WC. The strip and recoat process used by the supplier was approved by P&WC and complied with its aftermarket specification.
Mission profile review
- Aircraft and engine manufacturers collaborate in defining the intended use, or ‘mission profile’, of each aircraft-engine combination. The mission profile affects the physical design, the engine power requirements, and the frequency and content of scheduled maintenance.
- P&WC explained that component life and durability are predicated on operators adhering to the design mission profile, which takes into account factors such as flight duration and power demands. Significant long-term operation above standard mission parameters undermines the designers’ assumptions and can lead to reduced lives for components and the aircraft. In practice, operators are unlikely to know the parameters of the design mission profile.
- In 2015 P&WC, in conjunction with Pacific Aerospace, reviewed the engine handling procedures of nine skydiving operators in seven countries, including New Zealand, that used the 750XL with the PT6A-34 engine. The review produced an average mission profile that P&WC compared with the mission profile that was originally specified (Pacific Aerospace advised that this was four jumps per hour from 10,000 ft).
- The review found that skydiving operators typically operated their engines at the flight manual inter-turbine temperature limits for take-off and climb. Exceedances can occur during the climb, especially on hot days, when pilots operate to the torque limits and do not respect the inter-turbine temperature limits. At a given torque setting the inter-turbine temperature increases with altitude and could exceed the temperature limit. The review also found that engines were being operated at the high end of the operating limits for 72% of the average mission duration.
- As a result of the review, P&WC advised that it would revise the maintenance procedures for single-engine applications of the PT6A-34 engine in the skydiving role (P&WC planned to incorporate the revision into the PT6A engine maintenance manual in April 2017).
Other information
Type certificate anomalies
- In its separate investigation of this accident (see paragraph 3.3.26), the CAA identified an anomaly with the aircraft type certificate that it issued for the 750XL. The anomaly arose because of dual certification of the PT6A-34 engine by Canada and the United States. The 750XL is manufactured with a PT6A-34 engine. Although the CAA had accepted only the Canadian certification for all PT6A-series engines, it certificated the 750XL with reference to the United States engine certification. The CAA took internal action to correct this anomaly.
- A further anomaly concerned the CAA’s acceptance of the MORE® maintenance programme STC for the 750XL. The STC is held by a United States company and approved for the PT6A-34 engine certificated by the United States. Canada had not approved the STC for use with PT6A-34 engines certificated by Canada. Further investigation led to the identification of other potential anomalies with approved engine STCs. The CAA took action to correct these.
Analysis Tātaritanga
What happened
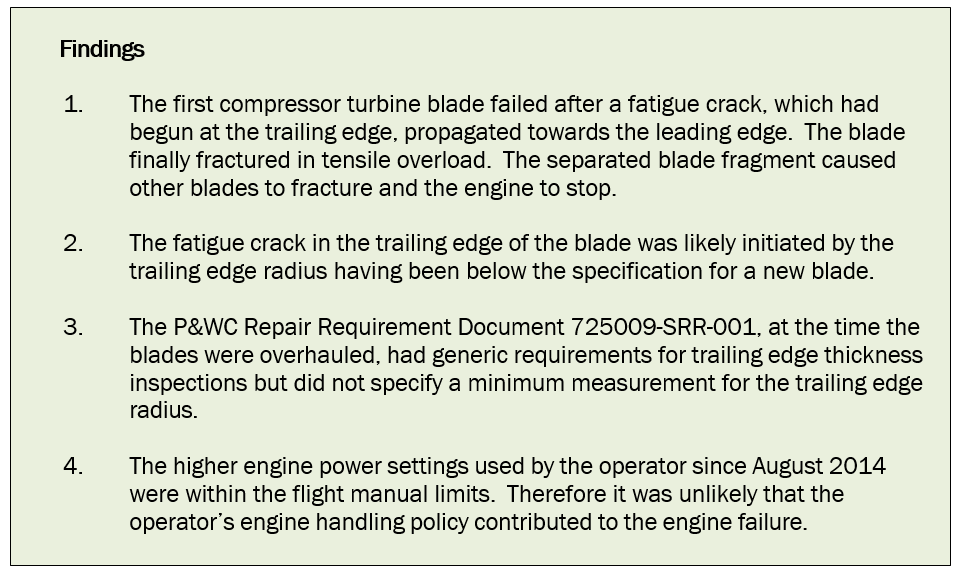
- A fractured compressor turbine blade caused the engine failure. The fracture originated in a fatigue crack in the trailing edge of the blade. The blade, one of a set of overhauled blades, had been operated for less than half the time before the next inspection was due in accordance with Service Bulletin 1403 (see paragraph 3.3.14).
- The engine failure occurred at a low height and over terrain that did not offer favourable options for a forced landing. As all of the occupants were wearing parachutes, baling out was the most appropriate action to take. The experience of the tandem masters contributed to a successful evacuation.
- The pilot unwittingly jeopardised the evacuation by baling out through his cockpit window rather than from the cabin rear door, and by deploying his parachute immediately. His actions were very likely due to natural anxiety and also, in part, to inadequate training in emergency procedures by the operator.
Safety issues
- Turbine engines, in general, are extremely reliable, which has led to their acceptance and approval for an increasing number of commercial single-engine-aircraft operations. However, a turbine blade failure will usually cause other blade failures on that turbine disk. Blade fragments will destroy downstream turbine stages, leading to total engine failure. Therefore turbine reliability is important for aviation safety.
- The following safety issues were identified during this inquiry:
- the measurement specifications for overhauled compressor turbine blades that had been through a strip and recoat repair process were not exactly the same as those for new blades. Blades that had been through that repair process, without verification of critical dimensions, might fail before the next 3,000-hour inspection
- when aircraft maintenance staff do not refer to the current Instructions for Continuing Airworthiness for a task, perhaps because they are very familiar with the basic task and do not know that the task documentation has changed, safety might be compromised
- parachute drop pilots were not required to wear lifejackets or flotation devices if their flights were expected to remain within gliding distance of land. That scenario downplayed the possibility of a pilot having to ditch an aeroplane or having to use the emergency parachute when over or near water.
Premature failure of the compressor turbine blade
Safety issue: The measurement specifications for overhauled compressor turbine blades that had been through a strip and recoat repair process were not exactly the same as those for new blades. Blades that had been through that repair process, without verification of critical dimensions, might fail before the next 3,000-hour inspection.
- The examination of the engine by P&WC identified the compressor turbine blade that had fractured first and caused the engine failure. The blade fracture surface had distinct fatigue and overload zones. Due to the damage, only approximate measurements of the blade dimensions in the fatigue zone could be performed. These showed that the radius of the trailing edge, after allowing for the thermal coating applied to blades, was less than that specified for a new blade.
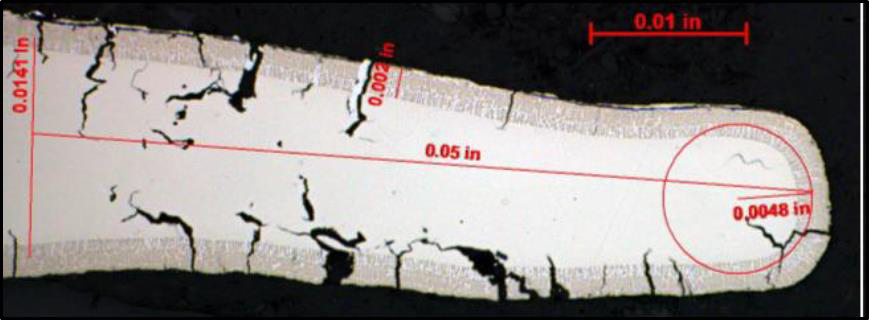
- Measurements were also taken of the remnants of six other overhauled blades and one of the two blades that had been new when installed in May 2013. One of the overhauled blades was under-size in trailing edge thickness and radius (see Figure 5), and two more were at the minimum limit for one or other dimension. The dimensions of the blade that was new when installed in May 2013 met the required specifications.
- During the overhaul, the blade had required repair in accordance with the P&WC-approved supplier process MPP1, based on document 725009-SRR-001. This document did not require the measurement of repaired blades in all of the dimensions specified by P&WC for the acceptance of new blades, although there had always been a verification of the minimum trailing edge thickness for blades that had been through a strip and recoat process.
- Engine turbine blades must endure very high temperatures and centrifugal loads; therefore the blades are manufactured to strict specifications. Under-size blades will erode or stretch, which can lead to their failing before reaching the next inspection. Of the eight compressor turbine blade remnants sampled from this set, two were under-size and another two were at the minimum size for a critical dimension.
- An operator will usually make a commercial decision on whether to install new or overhauled turbine blades. However, the use of overhauled components, or the introduction of an engine overhaul extension programme like this STC, could introduce new risks for an operator. It is a safety issue that the specifications for compressor turbine blades that had been through a strip and recoat process were not as well defined as those for new blades, and that overhauled blades might fail to reach the stated inspection intervals. The issue was of particular importance to operators of single-engine aircraft.
- P&WC noted that dimensional differences could arise for blades that had been repaired during overhaul: that is, had been stripped, repaired and then recoated. It submitted that blade durability after that process had been acceptable, as shown by [past] field experience.
- P&WC subsequently revised Repair Requirement Document 725009-SRR-001, for all of its PT6 engines, so that the trailing edge thickness measurement requirements matched those for new compressor turbine blades.
-
When asked about the implications of this investigation for other engines that were presently in service with overhauled compressor turbine blades, P&WC replied that further intervention would not improve fleet reliability. Its response was, in part:
Pratt & Whitney Canada has assessed the risk of further occurrences of this nature on the basis of the number of events and the time accrued on similarly repaired components over the service history of the affected fleet. Future risk of significant events related to fracture of under-dimensional, recoated blades was determined to be well within acceptable parameters (as defined by available Guidance Material). Additional field intervention would be deemed to be neither effective nor warranted at this point with respect to measurably improving fleet reliability (Email, P&WC, 9 March 2016).
- The flight manual has operating limits for engine speed and temperature, which pilots must observe in order to protect the engine from sudden or cumulative damage that will shorten the lives of turbine components. In general, the higher the power settings, the shorter the turbine life. The mission profile review conducted by P&WC and Pacific Aerospace found that skydiving operators tended to have a higher frequency of operating cycles (an operating cycle is one take-off and landing) than was originally assumed, and that would also affect directly the lives of engine components.
- Approximately 15 months after the overhauled turbine module was installed, the operator raised the take-off torque setting but retained the turbine temperature limit. Both settings remained at or below the flight manual limits. The operator’s engine handling procedure, even allowing for the high frequency of operating cycles in the skydiving role, would not have affected unduly the durability of the compressor turbine blades had all of the blades conformed to the correct specifications for acceptance after repair.
Maintenance practices
Safety issue: When aircraft maintenance staff do not refer to the current Instructions for Continuing Airworthiness for a task, perhaps because they are very familiar with the basic task and do not know that the task documentation has changed, safety might be compromised.
Engine inspections
- In 2003 P&WC had amended an inspection procedure to improve the early detection of cracks in the compressor turbine blades (P&WC Service Information Letter PT6A-116). The original procedure had called for a borescope to be inserted into the fuel nozzle port in the combustion module casing to look for heat distress on the upstream (upstream is in reference to the direction of gas flow through the engine, which, for the PT6 series of engines, is from back to front) side of the compressor turbine disk. The amendment recommended that the borescope be inserted through the exhaust duct also, to inspect the downstream side of the disk and the trailing edge of the turbine blades. The lower, overlapping, part of the compressor turbine blades, where cracks had been found in other engines, could be inspected only by viewing the blades from the exhaust port. The amended procedure had been first added to the engine maintenance manual in 2006. The Service Letter had been revised and reissued in July 2013.
- Since 2004, P&WC had issued further Service Information Letters and Service Bulletins to draw attention to the detrimental effects of engine over-temperature events on the turbine section, and how careful engine handling and proper maintenance procedures could prevent this damage. Appendix 1 has a summary of the information provided by P&WC.
-
The engine failure occurred 87 flight hours after the previous scheduled maintenance, which included a borescope inspection of the compressor turbine blades. However, when engineers of the maintenance provider were inspecting other PT6A-34 engines soon after the accident, the P&WC representative observed that the engineers did not follow fully the borescope requirement to inspect the downstream (forward) side of the compressor turbine disk.
- P&WC did not attempt to estimate the rate of propagation of the fatigue crack in the compressor turbine blade. Therefore it is not known whether the crack could have been present, and potentially detectable, at the time of the scheduled borescope inspection. The P&WC representative suggested that a borescope operator ought to be able to see a crack of five millimetres or more in length. P&WC informed the Commission that the published 300-hour inspection interval remained satisfactory for detecting cracks in compressor turbine blades.
- The Commission has discussed previously the issue of staff relying on their memory or habitual procedures when performing maintenance, and not referring to and following current procedures in a manual (for example, see Report 11-004, Piper PA31-350 Navajo Chieftain, ZK-MYS, landing without nose landing gear extended, Nelson Aerodrome, 11 May 2011). Manufacturers publish many amendments to manuals and Instructions for Continuing Airworthiness, of which some might not reach ‘frontline’ staff. If staff do not check that they are using the current procedures for tasks related to airworthiness, the intent of the procedures can be undermined and safety compromised.
- The maintenance provider has confirmed, since the accident, that it conducts fully the inspection requirements of the engine maintenance manual. It has also chosen not to use overhauled compressor turbine blades in the future.
Skydiving mission profile
-
Following the review of the skydiving mission profile, P&WC gave attention to the continued airworthiness of applicable engines. It advised that its analysis had determined that there was a need to improve some maintenance requirements. It said, in part:
Repetitive short missions with the majority of its length in the high end of the allowed power ratings reinforces the need to introduce better creep resistant compressor turbine blades … for skydiving missions. For engines pre-SB1690 configuration used in skydive operation, a [hot section inspection] requirement will be added to improve compressor turbine blade reliability to reach [stated time between overhaul] (Email, Pacific Aerospace, 10 March 2016. SB1690 is Service Bulletin 1690; see Appendix 1, paragraph 3).
- In this case there had been no changes to the MORE programme for the engine between the operator’s assumed registration in 2009 and the day of the accident. Fortunately, if there had been changes, the maintenance provider would have been aware of them, because it maintained another 750XL engine of the operator under the same STC (the operator had fulfilled the MORE® registration requirements for the other 750XL in June 2010).
- MORE had 12 engines (on nine aeroplanes) in New Zealand registered for this STC. As at June 2015 the register was more than 50% inaccurate as to aeroplane type and registration. One likely reason was that operators did not always advise sales of participating engines to MORE, as required by the STC.
- Compliance with the registration and applicable requirements of an approved STC is a condition for the continuing airworthiness of an aircraft or product.
Survivability aspects
Safety issue: Parachute drop pilots were not required to wear lifejackets or flotation devices if their flights were expected to remain within gliding distance of land. That scenario downplayed the possibility of a pilot having to ditch an aeroplane or having to use the emergency parachute when over or near water.
Tandem pairs
- The last tandem pair to leave the aeroplane estimated that the bale-out took up to 20 seconds. There was some delay after the call to “Get out!”, caused by tandem masters having to ensure that they were attached to their riders correctly and by one pair having to release their aeroplane restraint (Restraint belts were fitted even though Civil Aviation Rule 91.505(b) exempted a person engaged in parachute operations from the requirement to have a seat, berth, safety belt or restraining belt). The last tandem pair had to wait for the pilot and his deployed chute to clear the rear door.
- The tandem masters estimated that they had all left the aeroplane by about 1,500 ft above the lake, deploying their reserve parachutes by 1,000 ft. Parachuting rules required reserve parachutes to be deployed for tandem jumps from less than 5,000 ft above ground, because the reserve parachutes inflated more rapidly than main parachutes.
- Each of the tandem riders was equipped with a lifejacket (as required by Civil Aviation Rule 105.57), but the operator did not require the tandem masters to wear lifejackets because the operator expected that, under normal circumstances, the reserve parachutes would provide sufficient buoyancy. Following the accident the operator provided its tandem masters with flotation devices.
The pilot
- Parachute drop pilots are required to wear emergency parachutes on every skydiving flight (passengers on a skydiving flight who are not engaged in a parachute operation are also required to wear emergency parachutes). The operator had given the pilot ground-based training, but did not require its pilots to complete actual parachute descents. The pilot had not parachuted previously.
- The pilot could not recall having inspected the emergency parachute before putting it on that morning. He later said that he had never performed a pre-flight inspection of the parachute himself. The maintenance record for the parachute was found to be in order (Civil Aviation Rules required maintenance records for parachutes, as they are a type of aircraft).
- The operator did not equip its pilots with lifejackets and was not required to do so, because its flights from Taupō that used the Taupō aerodrome parachute landing area remained within gliding distance of land at all times (as permitted by Civil Aviation Rule 91.525). This was a safety issue, because the scenario downplayed the possibility of a pilot having to make a ditching, or bale out and drift to a water landing. In this case it was fortuitous that none of the parachutists or the pilot landed in the lake. A recommendation was made to the operator to investigate options for providing its drop pilots with flotation devices.
- Pilots are trained to put their aeroplanes into a gliding descent if they have to make a forced landing. The pilot, with minimal experience of the 750XL and parachuting operations, determined that he could not reach a suitable area on land. Although ditching in the lake was an option, he was aware that the flight manual warned that the aeroplane’s ditching characteristics were unknown. Therefore he chose to abandon the aeroplane.
- The operator trained its pilots to bale out of the cabin rear door after others had gone, and to pull the emergency parachute ripcord when clear of the aeroplane. However, it was acknowledged that not all emergency situations were foreseeable, and a pilot might have to bale out in a manner contrary to their training.
- The pilot did not intend to bale out before the last of the parachutists. However, by doing so he left the aeroplane uncontrolled, and it began to roll and dive shortly afterwards. If anyone still on board had had difficulty exiting the aeroplane, their survivability could have been jeopardised by the aeroplane’s rapidly changing attitude. In this case the proximity to people and property also meant that the unoccupied aeroplane was a threat.
- The operator suggested that it was likely that the pilot did not see in the cockpit mirror that there were people in the cabin, because the dark-coloured jumpsuits they were wearing merged with the dark cabin rear bulkhead. The operator took action to improve the colour contrast between the cabin rear bulkhead and the jumpsuits.
- By baling out through the cockpit door before everyone else had left the aeroplane, the pilot risked a collision or entanglement with the last tandem pair who exited from the rear door. He also risked colliding with the tail plane because he did not wait until he was clear of the aeroplane to deploy his parachute. Either mishap could have led to serious or fatal injuries. If he had exited through the cabin rear door he would have been sure that he was the last to leave and would not have put others at risk.
Training of parachute drop pilots for emergencies
- The chief pilot and chief parachute instructor were jointly responsible for training drop pilots in the use of emergency parachutes and in emergency procedures. The pilot’s training record, signed by the instructor and counter-signed by the pilot, indicated that this comprehensive training had been done. However, his hasty exit through the cockpit door before everyone else had baled out, and his immediate deployment of the parachute, were contrary to what he had been instructed.
- The pilot’s reaction was understandable given that the engine failure happened on his first day of solo flying in the role and at a relatively low height. However, his training had been completed so recently that the correct procedures, if they had been thoroughly understood, should have been fresh in his mind.
- Civil Aviation Rule 91.705 made drop pilots responsible for ensuring that each person carried in their aircraft, other than a person intending to make a parachute descent, was trained in the use of their emergency parachute and was briefed on the method to be used for exiting the aircraft (see Appendix 2). Rule 91.707 implied that a pilot was responsible for ensuring that their emergency parachute (and any other emergency parachutes carried) were serviceable, at the least by inspecting the parachute packing card.
- In order to be able to comply with these Rule requirements, parachute drop pilots must have a thorough understanding of the emergency procedures applicable to their aircraft. Training in emergency procedures typically requires rote learning so that one’s response to an emergency is instinctive and correct. The pilot’s response to the engine failure, along with his later comment that he had never personally inspected the emergency parachute, indicated that he had not fully understood the procedures. Therefore it was likely that his emergency training had not been adequate.
- The operator advised that, since the accident, it had added a voluntary tandem jump to the parachute drop pilot training, and include a group training session with tandem masters as part of the annual competency testing for pilots.
Appendix 2. Selected Civil Aviation Rules pertaining to parachute operations